

Risk Factors, Clinical Characteristics, and Antibiotic Susceptibility Patterns of Streptococcal Keratitis: An 18-Year Retrospective Study from a Tertiary Hospital in China
 ,
,
Abstract
1. Introduction
2. Results
2.1. Demographics and Predisposing Factors for Streptococcal Keratitis
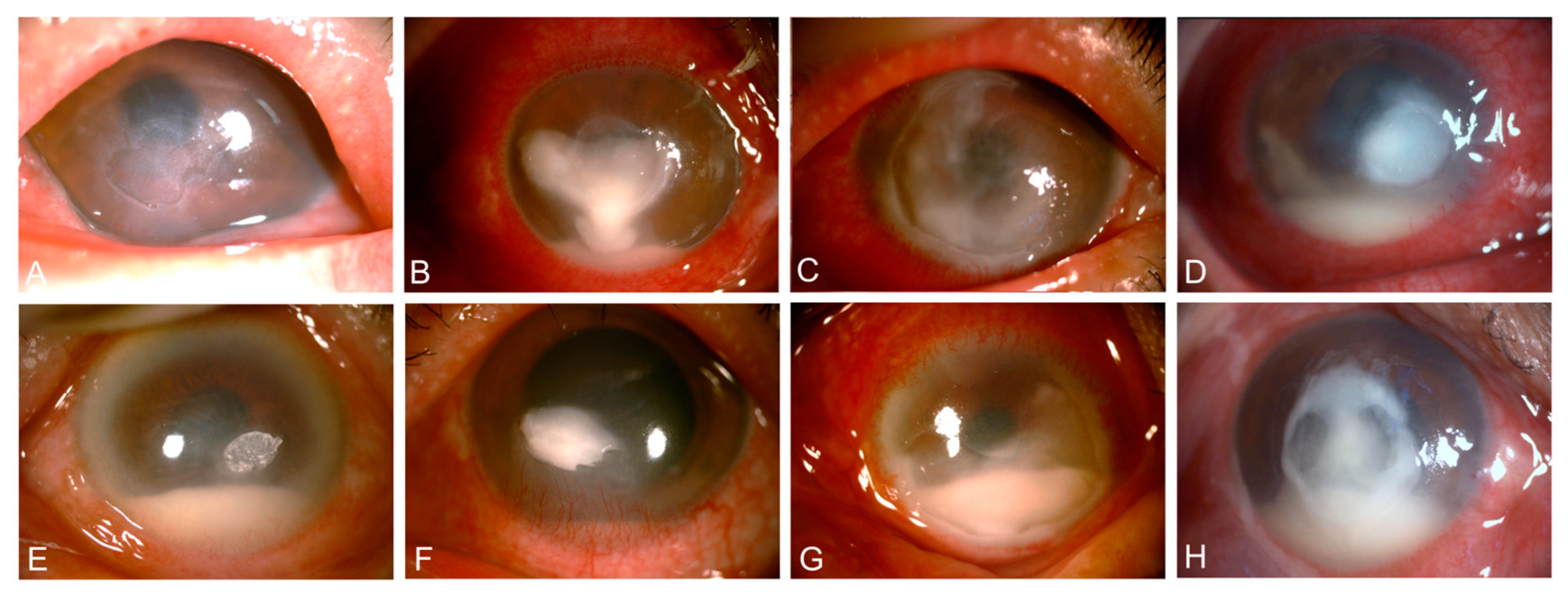
2.2. Clinical Characteristics of Streptococcal Keratitis Subtypes
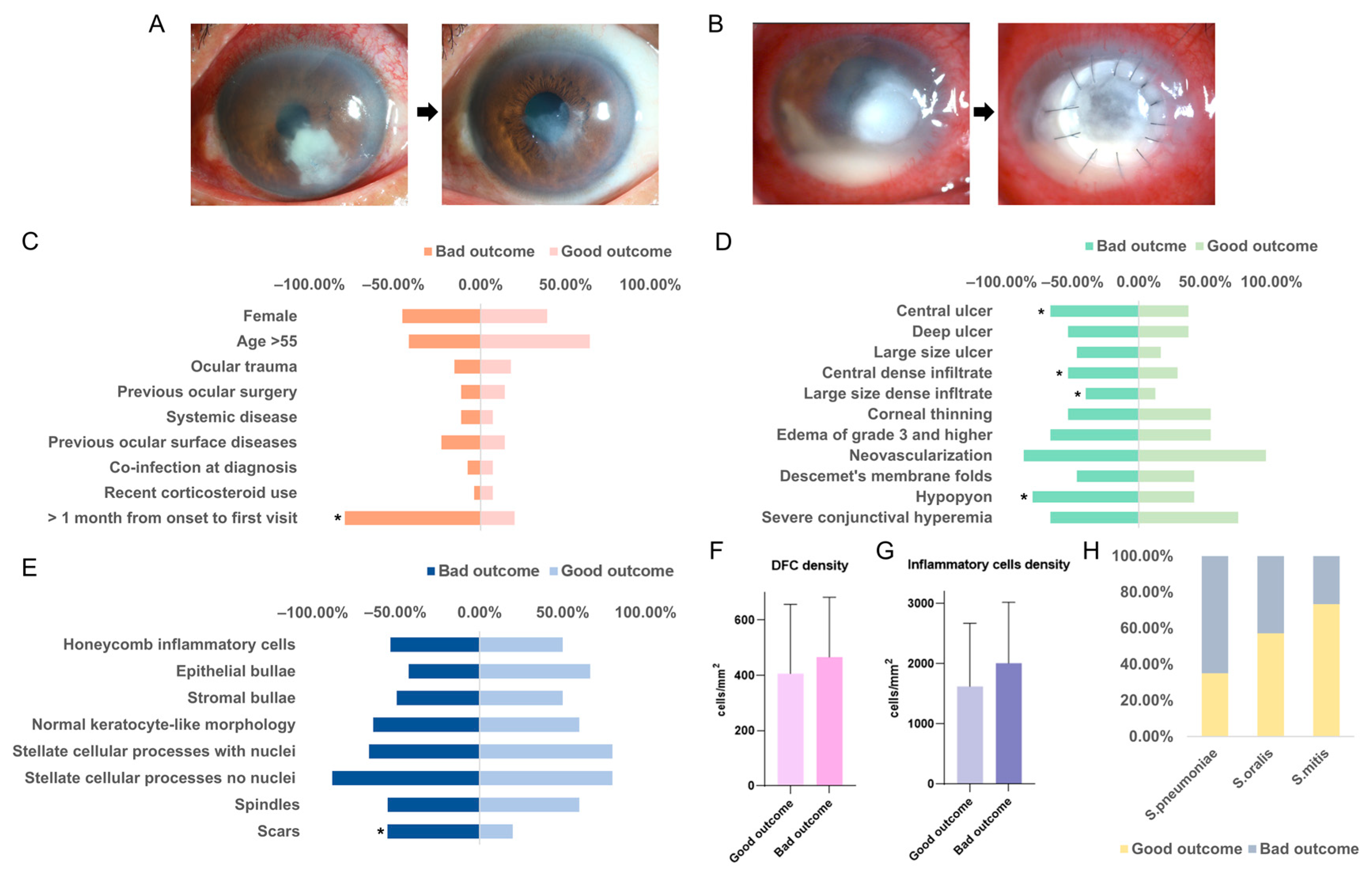
2.3. In Vivo Confocal Microscopy Findings in Streptococcal Keratitis Progression
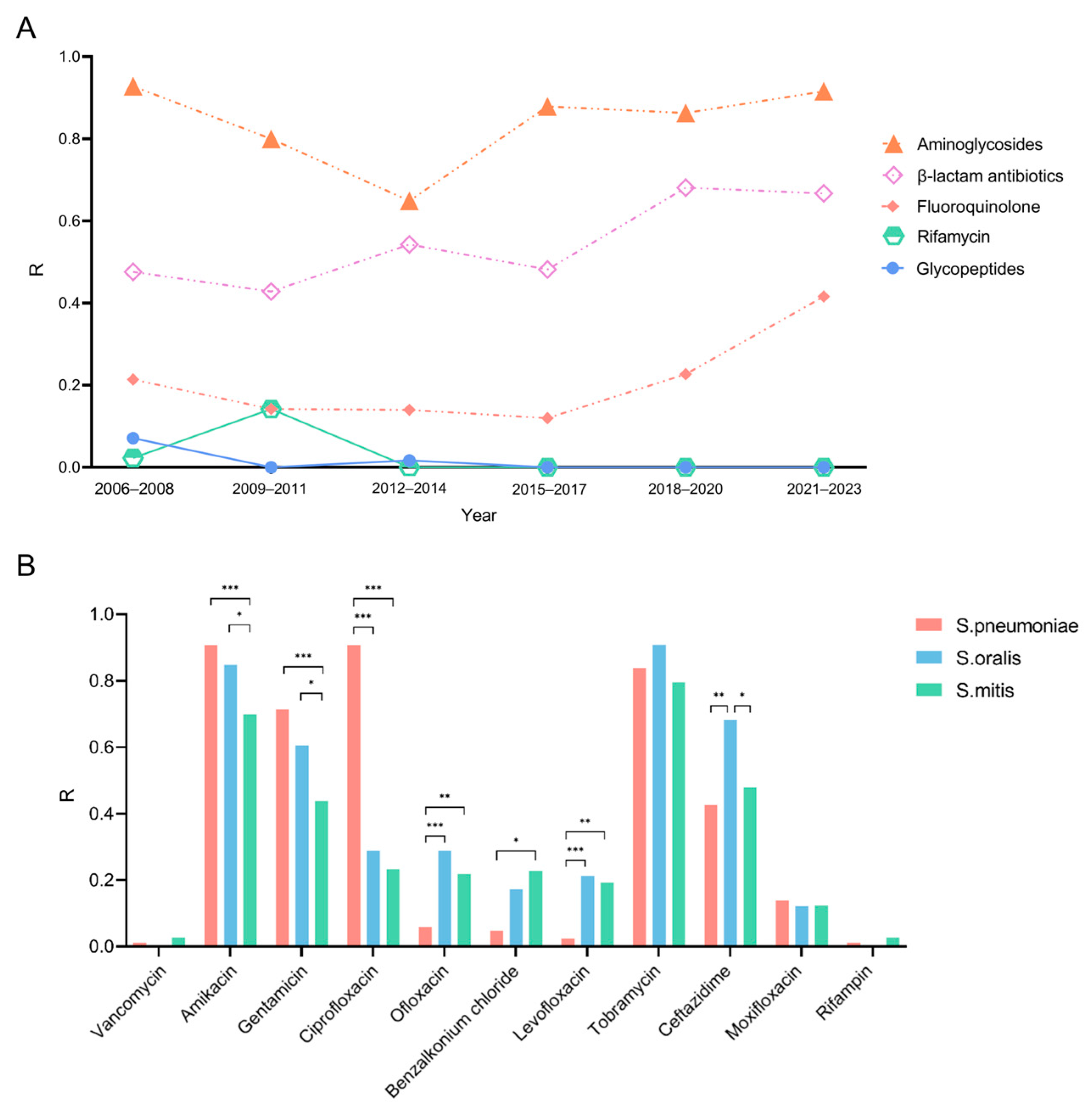
2.4. Antibiotic Resistance Profiles of Streptococcus Species
2.5. Analysis of Prognostic Correlations
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Clinical Diagnosis Procedures
4.3. Antibiotic Susceptibility Testing
4.4. Treatment and Outcome
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Russello, G.; Moramarco, A.; Vizzini, L.; Farina, C.; Fontana, L.; Carretto, E. Diagnostic approach and epidemiology of Microbial Keratitis: Findings from an Italian Tertiary Care center. Diagn. Microbiol. Infect. Dis. 2021, 101, 115470. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Blindness and Vision Impairment Collaborators; Vision Loss Expert Group of the Global Burden of Disease Study. Trends in prevalence of blindness and distance and near vision impairment over 30 years: An analysis for the Global Burden of Disease Study. Lancet Glob. Health 2021, 9, e130–e143. [Google Scholar] [CrossRef] [PubMed]
- Furlanetto, R.L.; Andreo, E.G.; Finotti, I.G.; Arcieri, E.S.; Ferreira, M.A.; Rocha, F.J. Epidemiology and etiologic diagnosis of infectious keratitis in Uberlandia, Brazil. Eur. J. Ophthalmol. 2010, 20, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Oydanich, M.; Dingle, T.C.; Hamula, C.L.; Ghisa, C.; Asbell, P. Retrospective report of antimicrobial susceptibility observed in bacterial pathogens isolated from ocular samples at Mount Sinai Hospital, 2010 to 2015. Antimicrob. Resist. Infect. Control 2017, 6, 29. [Google Scholar] [CrossRef] [PubMed]
- Sirikul, T.; Prabriputaloong, T.; Smathivat, A.; Chuck, R.S.; Vongthongsri, A. Predisposing factors and etiologic diagnosis of ulcerative keratitis. Cornea 2008, 27, 283–287. [Google Scholar] [CrossRef]
- Srinivasan, M.; Mascarenhas, J.; Prashanth, C.N. Distinguishing infective versus noninfective keratitis. Indian J. Ophthalmol. 2008, 56, 203–207. [Google Scholar] [CrossRef]
- Jin, H.; Parker, W.T.; Law, N.W.; Clarke, C.L.; Gisseman, J.D.; Pflugfelder, S.C.; Wang, L.; Al-Mohtaseb, Z.N. Evolving risk factors and antibiotic sensitivity patterns for microbial keratitis at a large county hospital. Br. J. Ophthalmol. 2017, 101, 1483–1487. [Google Scholar] [CrossRef]
- Hardie, J.M.; Whiley, R.A. The genus Streptococcus. In The Genera of Lactic Acid Bacteria; Wood, B.J.B., Holzapfel, W.H., Eds.; Springer: Boston, MA, USA, 1995; pp. 55–124. [Google Scholar]
- Nanayakkara, U.; Khan, M.A.; Hargun, D.K.; Sivagnanam, S.; Samarawickrama, C. Ocular streptococcal infections: A clinical and microbiological review. Surv. Ophthalmol. 2023, 68, 678–696. [Google Scholar] [CrossRef]
- Liesegang, T.J. Bacterial keratitis. Infect. Dis. Clin. N. Am. 1992, 6, 815–829. [Google Scholar] [CrossRef]
- Cabrera-Aguas, M.; Khoo, P.; Watson, S.L. Infectious keratitis: A review. Clin. Exp. Ophthalmol. 2022, 50, 543–562. [Google Scholar] [CrossRef]
- Hong, J.; Chen, J.; Sun, X.; Deng, S.X.; Chen, L.; Gong, L.; Cao, W.; Yu, X.; Xu, J. Paediatric bacterial keratitis cases in Shanghai: Microbiological profile, antibiotic susceptibility and visual outcomes. Eye 2012, 26, 1571–1578. [Google Scholar] [CrossRef]
- Lalitha, P.; Manoharan, G.; Karpagam, R.; Prajna, N.V.; Srinivasan, M.; Mascarenhas, J.; Das, M.; Porco, T.C.; Lietman, T.M.; Cevallos, V.; et al. Trends in antibiotic resistance in bacterial keratitis isolates from South India. Br. J. Ophthalmol. 2017, 101, 108–113. [Google Scholar] [CrossRef]
- Watson, S.L.; Gatus, B.J.; Cabrera-Aguas, M.; Armstrong, B.H.; George, C.R.; Khoo, P.; Lahra, M.M. Bacterial Ocular Surveillance System (BOSS) Sydney, Australia 2017–2018. Commun. Dis. Intell. 2020, 44, 1–14. [Google Scholar] [CrossRef]
- Mascarenhas, J.; Lalitha, P.; Prajna, N.V.; Srinivasan, M.; Das, M.; D’Silva, S.S.; Oldenburg, C.E.; Borkar, D.S.; Esterberg, E.J.; Lietman, T.M.; et al. Acanthamoeba, fungal, and bacterial keratitis: A comparison of risk factors and clinical features. Am. J. Ophthalmol. 2014, 157, 56–62. [Google Scholar] [CrossRef]
- Marquart, M.E.; Benton, A.H.; Galloway, R.C.; Stempak, L.M. Antibiotic susceptibility, cytotoxicity, and protease activity of viridans group streptococci causing endophthalmitis. PLoS ONE 2018, 13, e0209849. [Google Scholar] [CrossRef]
- Whatmore, A.M.; Efstratiou, A.; Pickerill, A.P.; Broughton, K.; Woodard, G.; Sturgeon, D.; George, R.; Dowson, C.G. Genetic relationships between clinical isolates of Streptococcus pneumoniae, Streptococcus oralis, and Streptococcus mitis: Characterization of “Atypical” pneumococci and organisms allied to S. mitis harboring S. pneumoniae virulence factor-encoding genes. Infect. Immun. 2000, 68, 1374–1382. [Google Scholar] [CrossRef]
- Hoffman, J.J.; Dart, J.K.G.; De, S.K.; Carnt, N.; Cleary, G.; Hau, S. Comparison of culture, confocal microscopy and PCR in routine hospital use for microbial keratitis diagnosis. Eye 2022, 36, 2172–2178. [Google Scholar] [CrossRef]
- Hau, S.C.; Dart, J.K.G.; Vesaluoma, M.; Parmar, D.N.; Claerhout, I.; Bibi, K.; Larkin, D.F.P. Diagnostic accuracy of microbial keratitis with in vivo scanning laser confocal microscopy. Br. J. Ophthalmol. 2010, 94, 982–987. [Google Scholar] [CrossRef]
- Termote, K.; Joe, A.W.; Butler, A.L.; McCarthy, M.; Blondeau, J.M.; Iovieno, A.; Holland, S.P.; Yeung, S.N. Epidemiology of bacterial corneal ulcers at tertiary centres in Vancouver, B.C. Can. J. Ophthalmol. 2018, 53, 330–336. [Google Scholar] [CrossRef]
- Chidambaram, J.D.; Prajna, N.V.; Palepu, S.; Lanjewar, S.; Shah, M.; Elakkiya, S.; Macleod, D.; Lalitha, P.; Burton, M.J. In Vivo Confocal Microscopy Cellular Features of Host and Organism in Bacterial, Fungal, and Acanthamoeba Keratitis. Am. J. Ophthalmol. 2018, 190, 24–33. [Google Scholar] [CrossRef]
- Tabatabaei, S.A.; Soleimani, M.; Behrouz, M.J.; Torkashvand, A.; Anvari, P.; Yaseri, M. A randomized clinical trial to evaluate the usefulness of amniotic membrane transplantation in bacterial keratitis healing. Ocul. Surf. 2017, 15, 218–226. [Google Scholar] [CrossRef]
- Williamson, D.A.; Carter, G.P.; Howden, B.P. Current and Emerging Topical Antibacterials and Antiseptics: Agents, Action, and Resistance Patterns. Clin. Microbiol. Rev. 2017, 30, 827–860. [Google Scholar] [CrossRef]
- Saravolatz, L.D.; Pawlak, J.; Saravolatz, S.N.; Johnson, L.B. In Vitro Activity of Retapamulin against Staphylococcus aureus Resistant to Various Antimicrobial Agents. Antimicrob. Agents Chemother. 2013, 57, 4547–4550. [Google Scholar] [CrossRef]
- Peng, M.Y.; Cevallos, V.; McLeod, S.D.; Lietman, T.M.; Rose-Nussbaumer, J. Bacterial Keratitis: Isolated Organisms and Antibiotic Resistance Patterns in San Francisco. Cornea 2018, 37, 84–87. [Google Scholar] [CrossRef]
- Asbell, P.A.; Sanfilippo, C.M.; Sahm, D.F.; DeCory, H.H. Trends in Antibiotic Resistance Among Ocular Microorganisms in the United States from 2009 to 2018. JAMA Ophthalmol. 2020, 138, 439–450. [Google Scholar] [CrossRef]
- Egrilmez, S.; Yildirim-Theveny, Ş. Treatment-Resistant Bacterial Keratitis: Challenges and Solutions. Clin. Ophthalmol. 2020, 14, 287–297. [Google Scholar] [CrossRef]
- Sand, D.; She, R.; Shulman, I.A.; Chen, D.S.; Schur, M.; Hsu, H.Y. Microbial keratitis in los angeles: The doheny eye institute and the los angeles county hospital experience. Ophthalmology 2015, 122, 918–924. [Google Scholar] [CrossRef]
- Mantadakis, E.; Maraki, S.; Michailidis, L.; Gitti, Z.; Pallikaris, I.G.; Samonis, G. Antimicrobial susceptibility of Gram-positive cocci isolated from patients with conjunctivitis and keratitis in Crete, Greece. J. Microbiol. Immunol. Infect. 2013, 46, 41–47. [Google Scholar] [CrossRef]
- Gurnani, B.; Kaur, K. Bacterial Keratitis; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2024. [Google Scholar]
- Fernandes, M.; Vira, D.; Dey, M.; Tanzin, T.; Kumar, N.; Sharma, S. Comparison Between Polymicrobial and Fungal Keratitis: Clinical Features, Risk Factors, and Outcome. Am. J. Ophthalmol. 2015, 160, 873–881.e872. [Google Scholar] [CrossRef]
- Rohatgi, J.N. Bacteriology of corneal ulcer with special reference to hypopyon corneal ulcer. Indian J. Ophthalmol. 1967, 15, 54–57. [Google Scholar]
- Acharya, M.; Farooqui, J.H.; Jain, S.; Mathur, U. Pearls and paradigms in Infective Keratitis. Rom. J. Ophthalmol. 2019, 63, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Blautain, B.; Rabut, G.; Dupas, B.; Riancho, L.; Liang, H.; Luzu, J.; Labbé, A.; Garrigue, J.S.; Brignole-Baudouin, F.; Baudouin, C.; et al. Multimodal Approach in Dry Eye Disease Combining In Vivo Confocal Microscopy and HLA-DR Expression. Transl. Vis. Sci. Technol. 2024, 13, 39. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; Rhee, M.K.; Akpek, E.K.; Amescua, G.; Farid, M.; Garcia-Ferrer, F.J.; Varu, D.M.; Musch, D.C.; Dunn, S.P.; Mah, F.S. Bacterial Keratitis Preferred Practice Pattern®. Ophthalmology 2019, 126, P1–P55. [Google Scholar] [CrossRef] [PubMed]
- Ung, L.; Chodosh, J. Foundational concepts in the biology of bacterial keratitis. Exp. Eye Res. 2021, 209, 108647. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameters | Patient (n = 350) |
|---|---|
| Demographics | |
| Age (mean ± SD) | 49.1 ± 23.1 |
| Female, n (%) | 165 (47.1%) |
| Laterality | |
| Left eye, n (%) | 151 (43.1%) |
| Right eye, n (%) | 193 (55.1%) |
| Both eyes, n (%) | 6 (1.7%) |
| Predisposing factors, n (%) | |
| Ocular trauma | 57 (16.3%) |
| Previous ocular surgery | 75 (21.4%) |
| Corneal surgery | 22 (6.3%) |
| PK | 5 (1.4%) |
| DSAEK | 10 (2.9%) |
| AMT | 5 (1.4%) |
| Gunderson flap | 2(0.6%) |
| Other surgery | 53 (15.1%) |
| Cataract Surgery | 17 (4.9%) |
| Eyelid plastic and reconstructive surgery | 8 (2.3%) |
| Ahmed glaucoma valve implantation | 7 (1.9%) |
| Excision of eyelid and conjunctival tumors | 6 (1.7%) |
| Vitrectomy | 4 (1.1%) |
| Other surgeries | 11 (3.1%) |
| Systemic disease | 32 (9.1%) |
| Diabetes mellitus | 14 (4.0%) |
| Ankylosing Spondylitis | 5 (1.4%) |
| Sjögren’s Syndrome | 3 (0.8%) |
| Ankylosing Spondylitis | 3 (0.8%) |
| Other diseases | 8 (2.3%) |
| Previous ocular diseases | 86 (24.6%) |
| Glaucoma | 21 (6.0%) |
| Uveitis | 18 (5.1%) |
| Blepharitis | 11 (3.1%) |
| Scleritis | 7 (1.9%) |
| Other diseases | 29 (8.3%) |
| Co-infection at diagnosis | 29(8.3%) |
| Other bacteria | 16(4.6%) |
| Fungi | 11(3.1%) |
| Amoeba | 2(0.6%) |
| Recent corticosteroid use | 14 (4.0%) |
| Onset time, n (%) | |
| <2 weeks | 151 (43.1%) |
| 2 weeks to 1 month | 104 (29.7%) |
| >1 month | 95 (27.1%) |
| Species of Streptococcus isolated, n (%) | |
| S. pneumoniae | 108 (29.8%) |
| S. mitis | 90 (24.9%) |
| S. oralis | 85 (23.5%) |
| S. sanguis | 23 (6.4%) |
| S. constellatus | 7 (1.9%) |
| S. salivarius | 6 (1.7%) |
| S. agalactiae | 6 (1.7%) |
| S. dysgalactie | 6 (1.7%) |
| S. goronii | 5 (1.4%) |
| S. anginosus | 4 (1.1%) |
| S. pyogenes | 3 (0.8%) |
| Others | 7 (1.9%) |
| Treatment, n(%) | |
| Antibiotic medications | 307 (87.7%) |
| Antibiotic medications and surgery | 43 (12.3%) |
| Clinical Signs | S. pneumoniae (n = 39) | S. oralis (n = 30) | S. mitis (n = 31) | p-Value |
|---|---|---|---|---|
| Location of ulcer | 0.358 | |||
| Central | 25 | 15 | 14 | |
| Paracentral | 11 | 12 | 15 | |
| Peripheral | 3 | 1 | 1 | |
| None | 0 | 0 | 1 | |
| Size of ulcer | 0.555 | |||
| <3 mm | 5 | 4 | 7 | |
| 3–6 mm | 27 | 19 | 21 | |
| >6 mm | 7 | 7 | 3 | |
| Location of dense infiltrate | 0.038 * | |||
| Central | 23 | 8 | 11 | |
| Paracentral | 14 | 12 | 15 | |
| Peripheral | 2 | 4 | 3 | |
| Complete cornea | 0 | 1 | 1 | |
| None | 0 | 5 | 1 | |
| Size of dense infiltrate | 0.037 * | |||
| <3 mm | 7 | 6 | 11 | |
| 3–6 mm | 28 | 19 | 13 | |
| >6 mm | 4 | 5 | 7 | |
| Corneal thinning | 0.798 | |||
| Yes | 22 | 15 | 18 | |
| No | 17 | 15 | 13 | |
| Neovascularization | 0.300 | |||
| Yes | 36 | 28 | 31 | |
| No | 3 | 2 | 0 | |
| Descemet’s membrane folds | 0.337 | |||
| Yes | 13 | 12 | 7 | |
| No | 26 | 18 | 24 | |
| Hypopyon | 0.006 * | |||
| Yes | 32 | 14 | 17 | |
| No | 7 | 16 | 14 | |
| Conjunctival hyperemia | 0.370 | |||
| 1 | 0 | 3 | 2 | |
| 2 | 6 | 6 | 5 | |
| 3 | 33 | 21 | 24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, Z.; Shi, Q.; Peng, B.; Zhang, Z.; Wei, Z.; Wang, Z.; Zhang, Y.; Chen, K.; Xu, X.; Lu, X.; et al. Risk Factors, Clinical Characteristics, and Antibiotic Susceptibility Patterns of Streptococcal Keratitis: An 18-Year Retrospective Study from a Tertiary Hospital in China. Antibiotics 2024, 13, 1190. https://doi.org/10.3390/antibiotics13121190
Cheng Z, Shi Q, Peng B, Zhang Z, Wei Z, Wang Z, Zhang Y, Chen K, Xu X, Lu X, et al. Risk Factors, Clinical Characteristics, and Antibiotic Susceptibility Patterns of Streptococcal Keratitis: An 18-Year Retrospective Study from a Tertiary Hospital in China. Antibiotics. 2024; 13(12):1190. https://doi.org/10.3390/antibiotics13121190
Chicago/Turabian StyleCheng, Zhen, Qingquan Shi, Bo Peng, Zijun Zhang, Zhenyu Wei, Zhiqun Wang, Yang Zhang, Kexin Chen, Xizhan Xu, Xinxin Lu, and et al. 2024. "Risk Factors, Clinical Characteristics, and Antibiotic Susceptibility Patterns of Streptococcal Keratitis: An 18-Year Retrospective Study from a Tertiary Hospital in China" Antibiotics 13, no. 12: 1190. https://doi.org/10.3390/antibiotics13121190
APA StyleCheng, Z., Shi, Q., Peng, B., Zhang, Z., Wei, Z., Wang, Z., Zhang, Y., Chen, K., Xu, X., Lu, X., & Liang, Q. (2024). Risk Factors, Clinical Characteristics, and Antibiotic Susceptibility Patterns of Streptococcal Keratitis: An 18-Year Retrospective Study from a Tertiary Hospital in China. Antibiotics, 13(12), 1190. https://doi.org/10.3390/antibiotics13121190