
Clinical Efficacy of Fidaxomicin and Oral Metronidazole for Treating Clostridioides difficile Infection and the Associated Recurrence Rate: A Retrospective Cohort Study

 , ,
, ,
Abstract
:1. Introduction
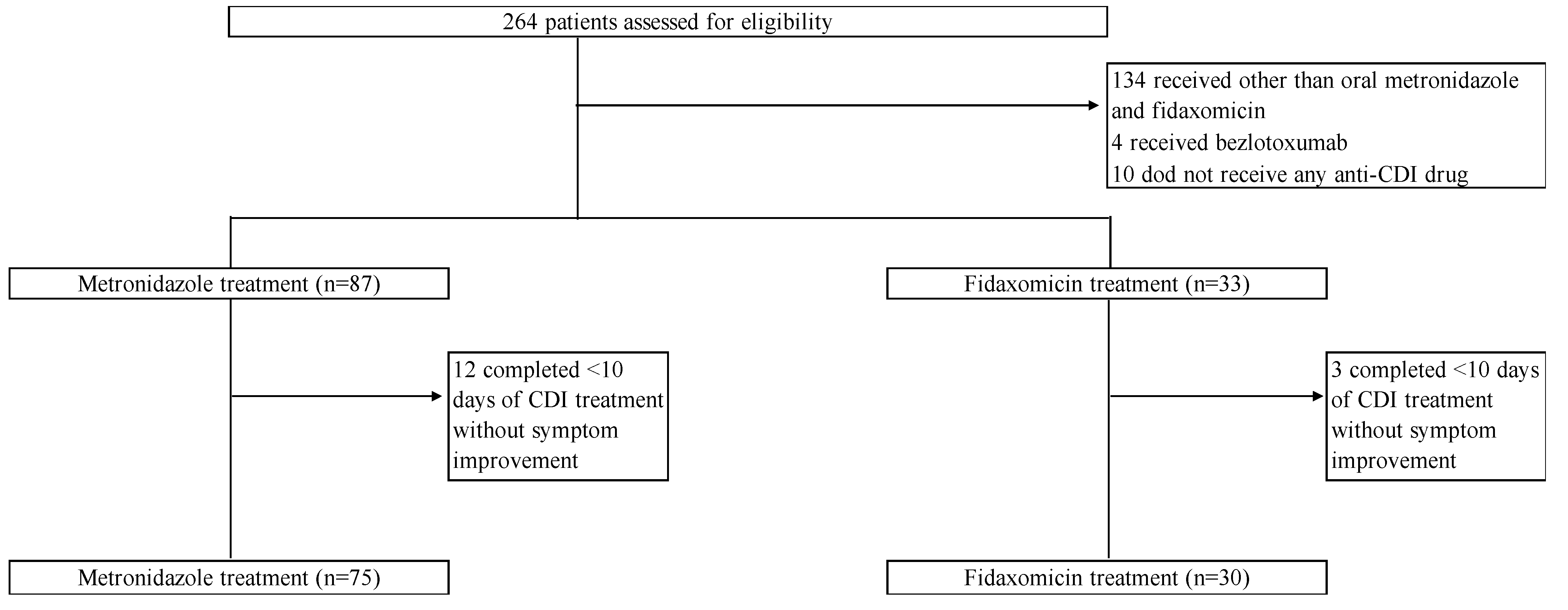
2. Results
3. Discussion
4. Materials and Methods
4.1. Study Design
4.2. Outcomes
4.3. Variable Definition
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, C.; Monaghan, T.; Yadegar, A.; Louie, T.; Kao, D. Insights into the Evolving Epidemiology of Clostridioides difficile Infection and Treatment: A Global Perspective. Antibiotics 2023, 12, 1141. [Google Scholar] [CrossRef] [PubMed]
- Lessa, F.C.; Mu, Y.; Bamberg, W.M.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile Infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef]
- Guh, A.Y.; Mu, Y.; Winston, L.G.; Johnston, H.; Olson, D.; Farley, M.M.; Wilson, L.E.; Holzbauer, S.M.; Phipps, E.C.; Dumyati, G.K.; et al. Trends in U.S. Burden of Clostridioides difficile Infection and Outcomes. N. Engl. J. Med. 2020, 382, 1320–1330. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Prabhu, V.S.; Marcella, S.W. Attributable Healthcare Resource Utilization and Costs for Patients with Primary and Recurrent Clostridium difficile Infection in the United States. Clin. Infect. Dis. 2018, 66, 1326–1332. [Google Scholar] [CrossRef]
- Johnson, S.; Lavergne, V.; Skinner, A.M.; Gonzales-Luna, A.J.; Garey, K.W.; Kelly, C.P.; Wilcox, M.H. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clin. Infect. Dis. 2021, 73, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Louie, T.J.; Miller, M.A.; Mullane, K.M.; Weiss, K.; Lentnek, A.; Golan, Y.; Gorbach, S.; Sears, P.; Shue, Y.-K. Fidaxomicin versus Vancomycin for Clostridium difficile Infection. N. Engl. J. Med. 2011, 364, 422–431. [Google Scholar] [CrossRef]
- Cornely, O.A.; Crook, D.W.; Esposito, R.; Poirier, A.; Somero, M.S.; Weiss, K.; Sears, P.; Gorbach, S.; for the OPT-80-004 Clinical Study Group. Fidaxomicin versus Vancomycin for Infection with Clostridium difficile in Europe, Canada, and the USA: A Double-Blind, Non-Inferiority, Randomised Controlled Trial. Lancet Infect. Dis. 2012, 12, 281–289. [Google Scholar] [CrossRef]
- Kunishima, H.; Ohge, H.; Suzuki, H.; Nakamura, A.; Matsumoto, K.; Mikamo, H.; Mori, N.; Morinaga, Y.; Yanagihara, K.; Yamagishi, Y.; et al. Japanese Clinical Practice Guidelines for Management of Clostridioides (Clostridium) Difficile Infection. J. Infect. Chemother. 2022, 28, 1045–1083. [Google Scholar] [CrossRef]
- Trubiano, J.A.; Cheng, A.C.; Korman, T.M.; Roder, C.; Campbell, A.; May, M.L.A.; Blyth, C.C.; Ferguson, J.K.; Blackmore, T.K.; Riley, T.V.; et al. Australasian Society of Infectious Diseases Updated Guidelines for the Management of Clostridium difficile Infection in Adults and Children in Australia and New Zealand. Intern. Med. J. 2016, 46, 479–493. [Google Scholar] [CrossRef]
- Gentry, C.A.; Campbell, D.L.; Williams, R.J., II. Outcomes Associated with Recent Guideline Recommendations Removing Metronidazole for Treatment of Non-Severe Clostridioides difficile Infection: A Retrospective, Observational, Nationwide Cohort Study. Int. J. Antimicrob. Agents 2021, 66, 106282. [Google Scholar] [CrossRef]
- Otsuka, T.; Sugimoto, M.; Inoue, R.; Ohno, M.; Ban, H.; Nishida, A.; Inatomi, O.; Takahashi, S.; Naito, Y.; Andoh, A. Influence of Potassium-Competitive Acid Blocker on the Gut Microbiome of Helicobacter Pylori-Negative Healthy Individuals. Gut 2017, 66, 1723–1725. [Google Scholar] [CrossRef] [PubMed]
- Okumura, H.; Fukushima, A.; Taieb, V.; Shoji, S.; English, M. Fidaxomicin Compared with Vancomycin and Metronidazole for the Treatment of Clostridioides (Clostridium) Difficile Infection: A Network Meta-Analysis. J. Infect. Chemother. 2020, 26, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Dai, J.; Gong, J.; Guo, R. Real-World Comparison of Fidaxomicin versus Vancomycin or Metronidazole in the Treatment of Clostridium difficile Infection: A Systematic Review and Meta-Analysis. Eur. J. Clin. Pharmacol. 2022, 78, 1727–1737. [Google Scholar] [CrossRef]
- Cornely, O.A.; Nathwani, D.; Ivanescu, C.; Odufowora-Sita, O.; Retsa, P.; Odeyemi, I.A.O. Clinical Efficacy of Fidaxomicin Compared with Vancomycin and Metronidazole in Clostridium difficile Infections: A Meta-Analysis and Indirect Treatment Comparison. J. Antimicrob. Chemother. 2014, 69, 2892–2900. [Google Scholar] [CrossRef]
- Appaneal, H.J.; Caffrey, A.R.; LaPlante, K.L. What Is the Role for Metronidazole in the Treatment of Clostridium difficile Infection? Results From a National Cohort Study of Veterans With Initial Mild Disease. Clin. Infect. Dis. 2019, 69, 1288–1295. [Google Scholar] [CrossRef]
- Jacobson, S.M.; Slain, D. Evaluation of a Bedside Scoring System for Predicting Clinical Cure and Recurrence of Clostridium difficile Infections. Am. J. Health. Syst. Pharm. 2015, 72, 1871–1875. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, H.; Yoshihara, A.; Yamamoto, T.; Sugimoto, K. A Preliminary Study of Bowel Rest Strategy in the Management of Clostridioides difficile Infection. Sci. Rep. 2020, 10, 22061. [Google Scholar] [CrossRef] [PubMed]
- Lamp, K.C.; Freeman, C.D.; Klutman, N.E.; Lacy, M.K. Pharmacokinetics and Pharmacodynamics of the Nitroimidazole Antimicrobials. Clin. Pharmacokinet. 1999, 36, 353–373. [Google Scholar] [CrossRef]
- Sears, P.; Crook, D.W.; Louie, T.J.; Miller, M.A.; Weiss, K. Fidaxomicin Attains High Fecal Concentrations with Minimal Plasma Concentrations Following Oral Administration in Patients with Clostridium difficile Infection. Clin. Infect. Dis. 2012, 55 (Suppl. S2), S116–S120. [Google Scholar] [CrossRef]
- Chilton, C.H.; Crowther, G.S.; Ashwin, H.; Longshaw, C.M.; Wilcox, M.H. Association of Fidaxomicin with C. difficile Spores: Effects of Persistence on Subsequent Spore Recovery, Outgrowth and Toxin Production. PLoS ONE 2016, 11, e0161200. [Google Scholar] [CrossRef]
- Spigaglia, P. Recent Advances in the Understanding of Antibiotic Resistance in Clostridium difficile Infection. Ther. Adv. Infect. Dis. 2016, 3, 23–42. [Google Scholar] [CrossRef]
- Freeman, J.; Vernon, J.; Morris, K.; Nicholson, S.; Todhunter, S.; Longshaw, C.; Wilcox, M.H.; Pan-European Longitudinal Surveillance of Antibiotic Resistance among Prevalent Clostridium difficile Ribotypes’ Study Group. Pan-European Longitudinal Surveillance of Antibiotic Resistance among Prevalent Clostridium difficile Ribotypes. Clin. Microbiol. Infect. 2015, 21, 248.e9–248.e16. [Google Scholar] [CrossRef]
- Aoki, K.; Takeda, S.; Miki, T.; Ishii, Y.; Tateda, K. Antimicrobial Susceptibility and Molecular Characterisation Using Whole-Genome Sequencing of Clostridioides difficile Collected in 82 Hospitals in Japan between 2014 and 2016. Antimicrob. Agents Chemother. 2019, 63, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Kunishima, H.; Chiba, J.; Saito, M.; Honda, Y.; Kaku, M. Antimicrobial Susceptibilities of Clostridium difficile Isolated in Japan. J. Infect. Chemother. 2013, 19, 360–362. [Google Scholar] [CrossRef]
- Kato, H.; Senoh, M.; Honda, H.; Fukuda, T.; Tagashira, Y.; Horiuchi, H.; Chiba, H.; Suzuki, D.; Hosokawa, N.; Kitazono, H.; et al. Clostridioides (Clostridium) Difficile Infection Burden in Japan: A Multicenter Prospective Study. Anaerobe 2019, 60, 102011. [Google Scholar] [CrossRef]
- Freeman, J.; Vernon, J.; Pilling, S.; Morris, K.; Nicolson, S.; Shearman, S.; Clark, E.; Palacios-Fabrega, J.A.; Wilcox, M.; Pan-European Longitudinal Surveillance of Antibiotic Resistance among Prevalent Clostridium difficile Ribotypes’ Study Group. Five-Year Pan-European, Longitudinal Surveillances of Clostridium difficile Ribotype Prevalence and Antimicrobial Resistance: The Extended ClosER Study. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Senoh, M.; Kato, H. Molecular Epidemiology of Endemic Clostridioides difficile Infection in Japan. Anaerobe 2022, 74, 102510. [Google Scholar] [CrossRef] [PubMed]
- van Rossen, T.M.; Ooijevaar, R.E.; Vandenbroucke-Grauls, C.M.J.E.; Dekkers, O.M.; Kuijper, E.J.; Keller, J.J.; van Prehn, J. Prognostic Factors for Severe and Recurrent Clostridioides difficile Infection: A Systematic Review. Clin. Microbiol. Infect. 2022, 28, 321–331. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variables | Total (n = 105) | Metronidazole Group (n = 75) | Fidaxomicin Group (n = 30) | p-Value |
|---|---|---|---|---|
| Age (years), median (IQR) | 76 (68–83) | 76 (70–85) | 76 (57–81) | 0.17 |
| Female sex, no. (%) | 49 (46.7) | 36 (48.0) | 13 (43.3) | 0.83 |
| Body mass index, median (IQR) | 18.4 (16.4–21.3) | 18.3 (16.4–20.5) | 18.5 (16.8–22.0) | 0.26 |
| Temperature at the time of CDI diagnosis, median (IQR) | 37.6 (37.1–38.2) | 37.7 (37.1–38.2) | 37.6 (37.1–38.2) | 0.82 |
| Bowel movements at the time of CDI diagnosis, median (IQR) | 4 (3–7) | 4 (3–7) | 4 (3–6) | 0.93 |
| Bloody stool at the time of CDI diagnosis, median (IQR) | 12 (11.4) | 10 (13.3) | 2 (6.7) | 0.33 |
| Comorbidities, no. (%) | ||||
| Diabetes mellitus | 36 (34.3) | 24 (32.0) | 12 (40.0) | 0.50 |
| Chronic kidney disease | 28 (25.7) | 16 (21.3) | 12 (40.0) | 0.09 |
| Heart failure/ischemic heart disease | 25 (23.8) | 17 (22.7) | 8 (26.7) | 0.80 |
| Chronic liver disease | 2 (1.9) | 1 (1.3) | 1 (3.3) | 0.50 |
| Chronic obstructive pulmonary disease | 7 (6.7) | 5 (6.7) | 2 (6.7) | 1.00 |
| Cerebrovascular disease | 25 (23.8) | 21 (28.0) | 4 (13.3) | 0.13 |
| Inflammatory bowel disease | 4 (3.8) | 3 (4.0) | 1 (3.3) | 1.00 |
| Solid malignancy | 26 (24.8) | 17 (22.7) | 9 (30.0) | 0.46 |
| Hematologic malignancy | 6 (5.7) | 5 (6.7) | 1 (3.3) | 0.67 |
| Enteral feeding, no. (%) | 24 (22.9) | 20 (26.7) | 4 (13.3) | 0.20 |
| Past hospitalization within 1 year, no. (%) | 61 (58.1) | 40 (53.3) | 21 (70.0) | 0.13 |
| History of abdominal surgery, no. (%) | 23 (21.9) | 13 (17.3) | 10 (33.3) | 0.12 |
| ICU admission at the time of CDI diagnosis, no. (%) | 10 (9.5) | 8 (19.7) | 2 (6.7) | 0.72 |
| Non-severe CDI, no. (%) | ||||
| IDSA/SHEA criteria | 71 (67.6) | 53 (70.7) | 18 (60.0) | 0.35 |
| Laboratory data, median (IQR) | ||||
| White blood cell count (/μL) | 9100 (5500–12,700) | 8000 (5000–11,600) | 10,550 (5800–14,500) | 0.05 |
| Albumin (mg/dL) | 2.4 (2.1–2.9) | 2.4 (2.2–2.8) | 2.5 (1.6–3.1) | 0.98 |
| Creatinine (mg/dL) | 0.74 (0.5–1.46) | 0.7 (0.48–1) | 0.8 (0.54–1.61) | 0.30 |
| C-reactive protein (mg/dL) | 4.1 (1.3–7.0) | 4.01 (1.18–7.05) | 4.44 (1.27–6.78) | 0.44 |
| Antibiotics, no. (%) | ||||
| Penicillin | 3 (2.9) | 2 (2.7) | 1 (3.3) | 1.00 |
| Cephalosporin | 52 (49.5) | 33 (44.0) | 19 (63.0) | 0.09 |
| Carbapenem | 24 (22.9) | 17 (22.7) | 7 (23.3) | 1.00 |
| Fluoroquinolone | 13 (12.4) | 8 (10.7) | 5 (16.7) | 0.51 |
| Clindamycin | 1 (0.9) | 1 (1.3) | 0 (0.0) | 1.00 |
| β-Lactam/β-Lactamase inhibitor | 60 (57.1) | 44 (58.7) | 16 (53.3) | 0.67 |
| Antiviral agents | 6 (5.7) | 6 (8.0) | 0 (0.0) | 0.18 |
| Antifungal agents | 5 (4.8) | 5 (6.7) | 0 (0.0) | 0.32 |
| Concomitant medication use, no. (%) | ||||
| PPIs | 49 (46.7) | 35 (46.7) | 14 (46.7) | 1.00 |
| H2RAs | 5 (4.8) | 5 (6.7) | 0 (0.0) | 0.32 |
| P-CABs | 17 (16.2) | 6 (8.0) | 11 (36.7) | 0.001 |
| Immunosuppression therapy | 20 (19.0) | 13 (17.3) | 7 (23.3) | 0.58 |
| Anticancer chemotherapy | 7 (6.7) | 5 (6.7) | 2 (6.7) | 1.00 |
| Probiotics used before CDI diagnosis, no. (%) | 40 (38.1) | 27 (36.0) | 13 (43.3) | 0.51 |
| Variables | Metronidazole Group (n = 75) | Fidaxomicin Group (n = 30) | p-Value |
|---|---|---|---|
| Global cure, no. (%) | 40 (53.3) | 21 (70.0) | 0.13 |
| Clinical cure, no. (%) | 59 (78.7) | 26 (86.7) | 0.42 |
| Recurrence, no. (%) | 19 (25.3) | 5 (16.7) | 0.44 |
| Change in the initial CDI treatment, no. (%) | 14 (18.7) | 0 (0.0) | 0.01 |
| Adverse effect, no. (%) | 2 (2.7) | 0 (0.0) | 1.00 |
| All-cause mortality within 30 days, no. (%) | 1 (1.4) | 1 (3.4) | 0.49 |
| Variables | Global Cure Group (n = 61) | Non-Global Cure Group (n = 44) | p-Value |
|---|---|---|---|
| Age (years), median (IQR) | 77 (70–84) | 76 (66–86) | 0.93 |
| Male sex, no. (%) | 36 (59.0) | 20 (45.5) | 0.23 |
| Body mass index, median (IQR) | 18.3 (16.2–20.4) | 18.6 (16.1–21.2) | 0.76 |
| Temperature at the time of CDI diagnosis, median (IQR) | 37.4 (36.3–38.5) | 37.9 (37.2–38.6) | 0.09 |
| Bowel movements at the time of CDI diagnosis, median (IQR) | 4 (2.5–5.5) | 5 (2.5–7.5) | 0.08 |
| Bloody stool at the time of CDI diagnosis, no. (%) | 8 (13.1) | 4 (9.1) | 0.76 |
| Comorbidities, no. (%) | |||
| Diabetes mellitus | 19 (31.1) | 17 (38.6) | 0.53 |
| Chronic kidney disease | 16 (26.2) | 12 (27.3) | 1.00 |
| Heart failure/ischemic heart disease | 15 (24.6) | 10 (22.7) | 1.00 |
| Chronic liver disease | 2 (3.3) | 0 (0.0) | 0.50 |
| Chronic obstructive pulmonary disease | 3 (4.9) | 4 (9.1) | 0.45 |
| Cerebrovascular disease | 14 (23.0) | 11 (25.0) | 0.82 |
| Inflammatory bowel disease | 3 (4.9) | 1 (2.3) | 0.64 |
| Solid malignancy | 14 (23.0) | 12 (27.3) | 0.65 |
| Hematologic malignancy | 0 (0.0) | 6 (13.6) | 0.004 |
| Enteral feeding, no. (%) | 10 (16.4) | 51 (83.6) | 0.10 |
| Past hospitalization within 1 year, no. (%) | 35 (57.4) | 26 (59.1) | 1.00 |
| History of abdominal surgery, no. (%) | 14 (23.0) | 9 (20.5) | 0.82 |
| ICU admission at the time of CDI diagnosis, no. (%) | 5 (50.0) | 56 (91.8) | 0.74 |
| Severe CDI, no. (%) | 18 (29.5) | 16 (36.4) | 0.53 |
| Antibiotics, no. (%) | |||
| Penicillin | 1 (1.7) | 2 (4.5) | 0.57 |
| Cephalosporin | 31 (59.6) | 30 (56.6) | 0.84 |
| Carbapenem | 10 (41.7) | 51 (63.0) | 0.10 |
| Fluoroquinolone | 7 (11.5) | 6 (13.6) | 0.77 |
| Clindamycin | 0 (0.0) | 1 (2.3) | 0.42 |
| β-Lactam/β-Lactamase inhibitor | 36 (59.0) | 24 (54.5) | 0.69 |
| Antiviral agents | 4 (6.6) | 2 (4.5) | 1.00 |
| Antifungal agents | 2 (3.3) | 3 (6.8) | 0.65 |
| Concomitant medication use, no. (%) | |||
| PPIs | 30 (49.2) | 19 (43.2) | 0.56 |
| H2RAs | 3 (4.9) | 2 (4.5) | 1.00 |
| P-CAB | 12 (19.7) | 5 (11.4) | 0.29 |
| Immunosuppression therapy | 10 (16.4) | 10 (22.7) | 0.46 |
| Anticancer chemotherapy | 3 (4.9) | 4 (9.1) | 0.45 |
| Probiotics, no. (%) | 21 (34.4) | 19 (43.2) | 0.42 |
| FDX treatment, no. (%) | 21 (34.4) | 9 (20.5) | 0.13 |
| Variable | Odds Ratio | 95% CI | p-Value |
|---|---|---|---|
| Fidaxomicin treatment | 1.49 | 0.94–2.37 | 0.09 |
| Age | 1.01 | 0.98–1.04 | 0.66 |
| Severe Clostridioides difficile infection | 0.68 | 0.29–1.58 | 0.37 |
| Use of proton pump inhibitor | 1.24 | 0.56–2.77 | 0.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, N.; Hirai, J.; Ohashi, W.; Asai, N.; Shibata, Y.; Mikamo, H. Clinical Efficacy of Fidaxomicin and Oral Metronidazole for Treating Clostridioides difficile Infection and the Associated Recurrence Rate: A Retrospective Cohort Study. Antibiotics 2023, 12, 1323. https://doi.org/10.3390/antibiotics12081323
Mori N, Hirai J, Ohashi W, Asai N, Shibata Y, Mikamo H. Clinical Efficacy of Fidaxomicin and Oral Metronidazole for Treating Clostridioides difficile Infection and the Associated Recurrence Rate: A Retrospective Cohort Study. Antibiotics. 2023; 12(8):1323. https://doi.org/10.3390/antibiotics12081323
Chicago/Turabian StyleMori, Nobuaki, Jun Hirai, Wataru Ohashi, Nobuhiro Asai, Yuichi Shibata, and Hiroshige Mikamo. 2023. "Clinical Efficacy of Fidaxomicin and Oral Metronidazole for Treating Clostridioides difficile Infection and the Associated Recurrence Rate: A Retrospective Cohort Study" Antibiotics 12, no. 8: 1323. https://doi.org/10.3390/antibiotics12081323
APA StyleMori, N., Hirai, J., Ohashi, W., Asai, N., Shibata, Y., & Mikamo, H. (2023). Clinical Efficacy of Fidaxomicin and Oral Metronidazole for Treating Clostridioides difficile Infection and the Associated Recurrence Rate: A Retrospective Cohort Study. Antibiotics, 12(8), 1323. https://doi.org/10.3390/antibiotics12081323