
Changing Trends in the Global Consumption of Treatments Used in Hospitalized Patients for COVID-19: A Time Series Multicentre Study

 , , , , ,
, , , , ,  ,
,  ,
,
Abstract
1. Introduction
2. Results
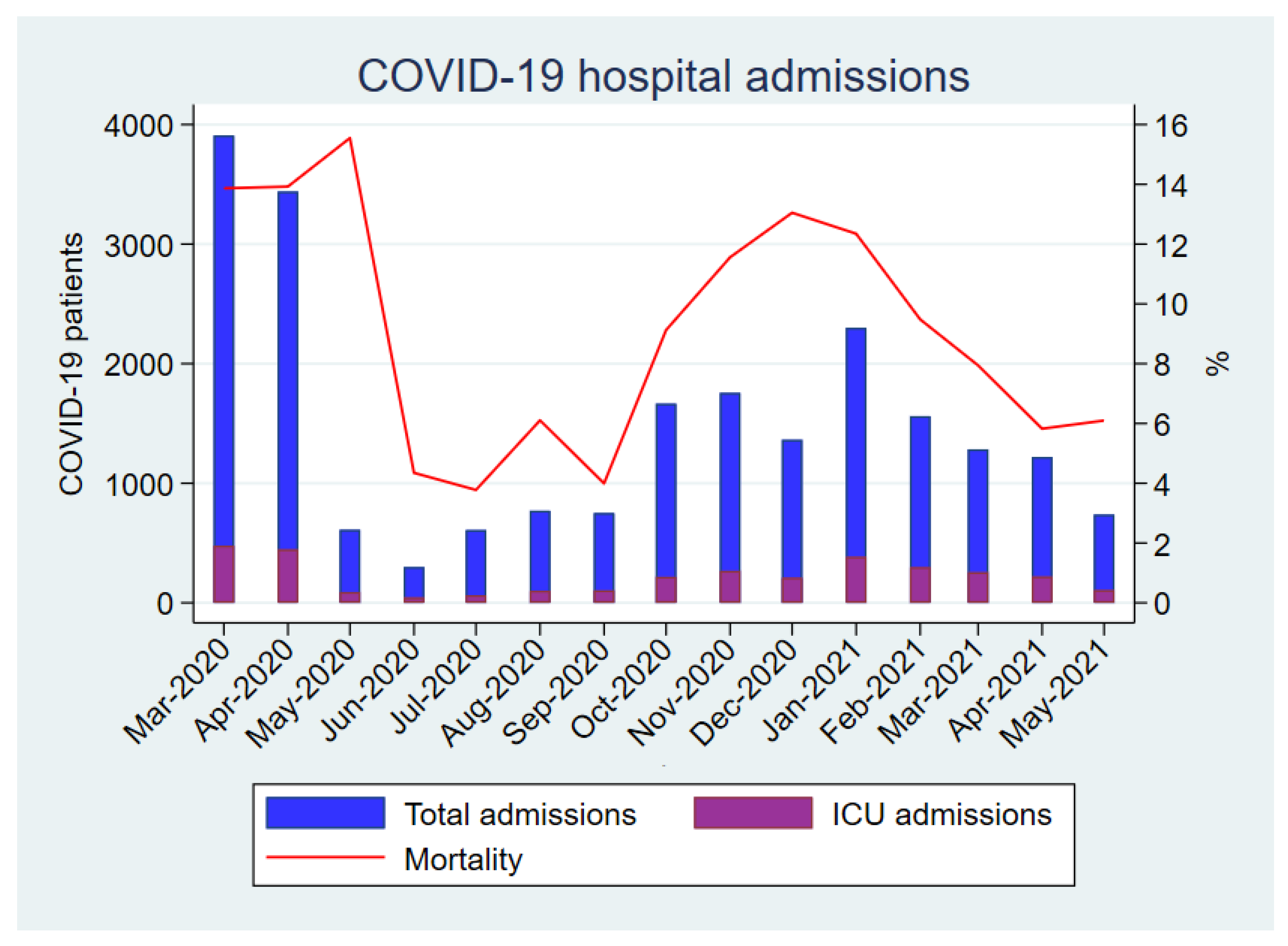
2.1. Demographic and Mortality Data
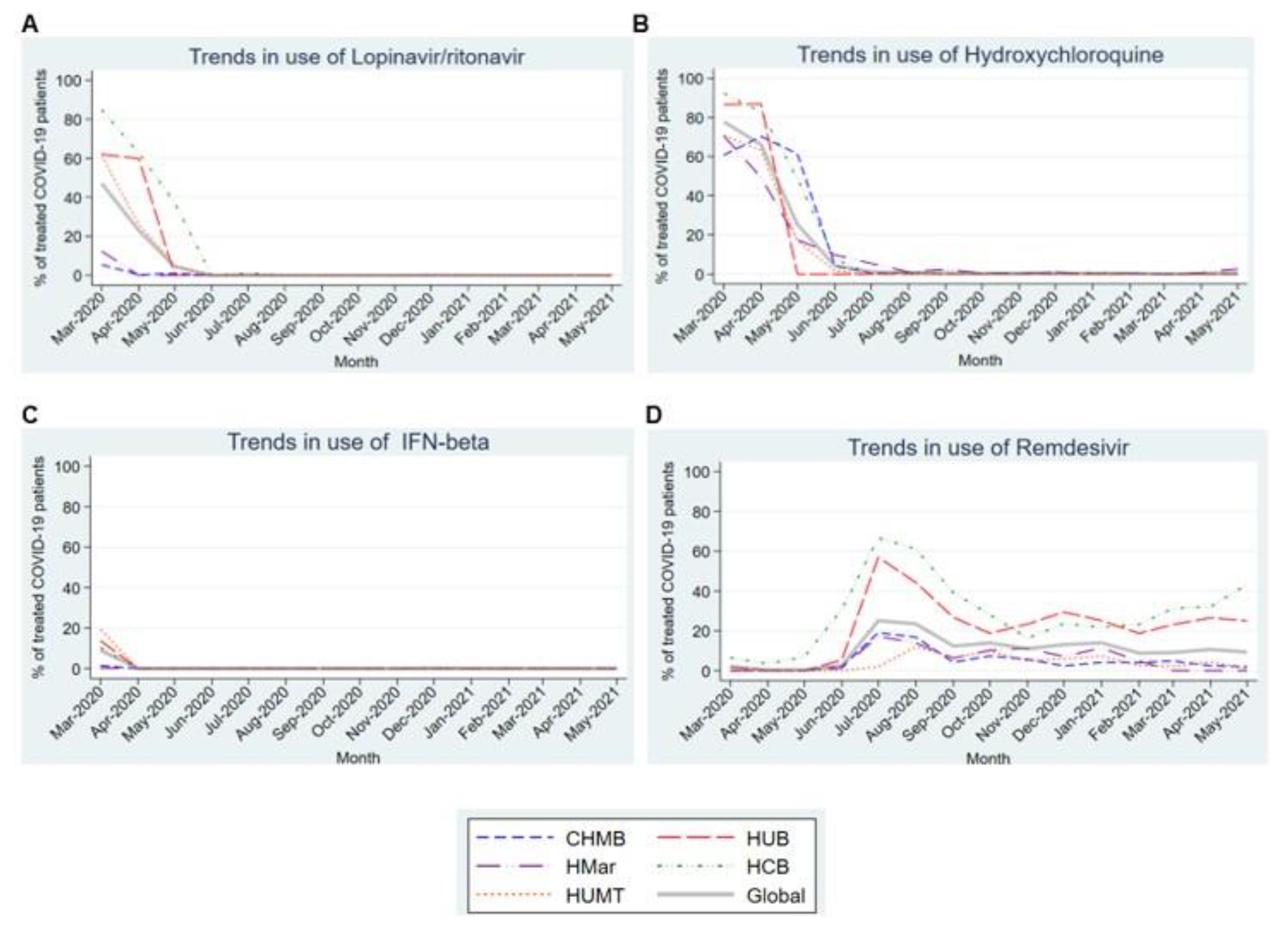
2.2. Antiviral Drugs
2.3. Immunomodulatory and Immunosuppressive Drugs
2.4. Antibiotics
3. Discussion
4. Methods
4.1. Study Design and Population
4.2. Data Collection
4.3. Definitions
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news/item/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 5 December 2022).
- COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 5 December 2022).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Gutiérrez, B.; del Toro, M.D.; Borobia, A.M.; Carcas, A.; Jarrín, I.; Yllescas, M.; Ryan, P.; Pachón, J.; Carratalà, J.; Berenguer, J.; et al. Identification and validation of clinical phenotypes with prognostic implications in patients admitted to hospital with COVID-19: A multicentre cohort study. Lancet Infect. Dis. 2021, 21, 783–792. [Google Scholar] [CrossRef]
- Therapeutics and COVID-19: Living Guideline. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2022 (accessed on 5 December 2022).
- Guidance for COVID-19|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/communication/guidance.html (accessed on 5 December 2022).
- SEIMC—COVID-19—Recomendaciones SEIMC para el Manejo Clínico de Pacientes con COVID-19. Available online: https://covid19.seimc.org/ (accessed on 5 December 2022).
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.P.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate COVID-19. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- Wennberg, J.E. Dealing with medical practice variations: A proposal for action. Health Aff. 1984, 3, 6–32. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair allocation of scarce medical resources in the time of COVID-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Izcovich, A.; Siemieniuk, R.A.; Bartoszko, J.J.; Ge, L.; Zeraatkar, D.; Kum, E.; Qasim, A.; Khamis, A.M.; Rochwerg, B.; Agoritsas, T.; et al. Adverse effects of remdesivir, hydroxychloroquine and lopinavir/ritonavir when used for COVID-19: Systematic review and meta-analysis of randomised trials. BMJ Open 2022, 12, e048502. [Google Scholar] [CrossRef]
- Mohammad Zadeh, N.; Mashinchi Asl, N.S.; Forouharnejad, K.; Ghadimi, K.; Parsa, S.; Mohammadi, S.; Omidi, A. Mechanism and adverse effects of COVID-19 drugs: A basic review. Int. J. Physiol. Pathophysiol. Pharmacol. 2021, 13, 102–109. [Google Scholar]
- De Wilde, A.H.; Jochmans, D.; Posthuma, C.C.; Zevenhoven-Dobbe, J.C.; Van Nieuwkoop, S.; Bestebroer, T.M.; van den Hoogen, B.; Neyts, J.; Snijder, E. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob. Agents Chemother. 2014, 58, 4875–4884. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.M.; Cheng, C.C.; Hung, F.N.; Wong, M.M.L.; Chan, H.; Chan, S.; Kao, R.Y.T.; Poon, L.L.M.; Wong, C.L.P.; Guan, Y.; et al. Role of lopinavir/ritonavir in the treatment of SARS: Initial virological and clinical findings. Thorax 2004, 59, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Y.; Jan, J.T.; Ma, S.H.; Kuo, C.J.; Juan, H.F.; Cheng, Y.S.E.; Hsu, H.-H.; Huang, H.-C.; Wu, D.; Brik, A.; et al. Small molecules targeting severe acute respiratory syndrome human coronavirus. Proc. Natl. Acad. Sci. USA 2004, 101, 10012–10017. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Wu, T.; Zuo, Z.; You, Y.; Yang, X.; Pan, L.; Hu, Y.; Luo, X.; Jiang, L.; Xia, Z.; et al. Evaluation of current medical approaches for COVID-19: A systematic review and meta-analysis. BMJ 2021, 11, 45–52. [Google Scholar] [CrossRef]
- Liu, W.; Zhou, P.; Chen, K.; Ye, Z.; Liu, F.; Li, X.; He, N.; Wu, Z.; Zhang, Q.; Gong, X.; et al. Efficacy and safety of antiviral treatment for COVID-19 from evidence in studies of SARS-CoV-2 and other acute viral infections: A systematic review and meta-analysis. CMAJ 2020, 192, E734–E744. [Google Scholar] [CrossRef]
- First COVID-19 Treatment Recommended for EU Authorisation|European Medicines Agency. Available online: https://www.ema.europa.eu/en/news/first-covid-19-treatment-recommended-eu-authorisation (accessed on 28 June 2022).
- Grundeis, F.; Ansems, K.; Dahms, K.; Mikolajewska, A.; Thieme, V.; Piechotta, V.; Metzendorf, M.-I.; Stegemann, M.; Benstoem, C.; Fichtner, F. Remdesivir for the treatment of COVID-19. Cochrane Database Syst. Rev. 2023, 1, CD014962. [Google Scholar]
- Seethapathy, R.; Zhao, S.; Long, J.D.; Strohbehn, I.A.; Sise, M.E. A Propensity Score-Matched Observational Study of Remdesivir in Patients with COVID-19 and Severe Kidney Disease. Kidney360 2021, 3, 269–278. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 Illness in Native and Immunosuppressed States: A Clinical-Therapeutic Staging Proposal. J. Hear. Lung Transpl. 2020, 39, 405–407. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; TttersaLl, R.S.; Manson, J.J.; on behalf of the HLH Across Speciality Collaboration, UK. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Rosas, I.O.; Bräu, N.; Waters, M.; Go, R.C.; Hunter, B.D.; Bhagani, S.; Skiest, D.; Aziz, M.S.; Cooper, N.; Douglas, I.S.; et al. Tocilizumab in Hospitalized Patients with Severe COVID-19 Pneumonia. N. Engl. J. Med. 2021, 384, 1503–1516. [Google Scholar] [CrossRef] [PubMed]
- Selvaraj, V.; Khan, M.S.; Bavishi, C.; Dapaah-Afriyie, K.; Finn, A.; Lal, A.; Mylonakis, E. Tocilizumab in Hospitalized Patients with COVID-19: A Meta Analysis of Randomized Controlled Trials. Lung 2021, 199, 239–248. [Google Scholar] [CrossRef] [PubMed]
- WHO Prequalifies First Monoclonal Antibody-Tocilizumab-to Treat COVID-19. Available online: https://www.who.int/news/item/11-02-2022-who-prequalifies-first-monoclonal-antibody---tocilizumab-to-treat-covid-19 (accessed on 28 June 2022).
- Annane, D.; Pastores, S.M.; Rochwerg, B.; Arlt, W.; Balk, R.A.; Beishuizen, A.; Briegel, J.; Carcillo, J.; Christ-Crain, M.; Cooper, M.S.; et al. Guidelines for the diagnosis and management of critical illness-related corticosteroid insufficiency (CIRCI) in critically ill patients (Part I): Society of Critical Care Medicine (SCCM) and European Society of Intensive Care Medicine (ESICM) 2017. Intensive Care Med. 2017, 43, 1751–1763. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Russell, C.D.; Millar, J.E.; Baillie, J.K. Clinical evidence does not support corticosteroid treatment for 2019-nCoV lung injury. Lancet 2020, 395, 473–475. [Google Scholar] [CrossRef]
- Rodrigo, C.; Leonardi-Bee, J.; Nguyen-Van-Tam, J.S.; Lim, W.S. Effect of corticosteroid therapy on influenza-related mortality: A systematic review and meta-analysis. J. Infect. Dis. 2015, 212, 183–194. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with COVID-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar]
- Garcia-vidal, C.; Sanjuan, G.; Moreno-garcía, E.; Puerta-alcalde, P.; Garcia-pouton, N.; Chumbita, M.; Fernandez-Pittol, M.; Pitart, C.; Inciarte, A.; Bodro, M.; et al. Incidence of co-infections and superinfections in hospitalized patients with COVID-19: A retrospective cohort study. Clin. Microbiol. Infect. 2021, 27, 83–88. [Google Scholar] [CrossRef]
- Kamel, A.M.; Monem, M.S.A.; Sharaf, N.A.; Magdy, N.; Farid, S.F. Efficacy and safety of azithromycin in COVID-19 patients: A systematic review and meta-analysis of randomized clinical trials. Rev. Med. Virol. 2022, 32, e2258. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Month | Hospital Occupancy Due to COVID-19 N—% (CI 95%) | COVID-19 Patients Admitted to the ICU % (CI 95%) | Male % (CI 95%) | Age Mean (sd) | COVID-19 Deaths % (CI 95%) | LOS Median of Days (IQR) |
|---|---|---|---|---|---|---|
| March 2020 | 3909—36.08% (35.18–36.99) | 12.23 (11.20–13.26) | 54.44 (52.88–56.00) | 61.89 (4.08) | 13.87 (12.78–14.95) | 12.3 (4.79) |
| April 2020 | 3440—51.21% (50.01–52.40) | 12.99 (11.87–13.26) | 54.48 (52.81–56.14) | 63.07 (5.08) | 13.92 (12.77–15.08) | 11.4 (1.23) |
| May 2020 | 611—7.98% (7.37–8.58) | 14.73 (11.92–17.54) | 52.54 (48.58–56.50) | 64.18 (6.96) | 15.55 (12.67–18.42) | 11.5 (5.31) |
| June 2020 | 299—3.26% (2.90–3.62) | 15.05 (11.00–19.10) | 51.17 (45.50–56.84) | 61.32 (2.95) | 4.35 (2.04–6.66) | 11.8 (3.52) |
| July 2020 | 609—6.25% (5.77–6.73) | 10.51 (8.07–12.94) | 54.35 (50.40–58.31) | 57.45 (5.34) | 3.78 (2.26–5.29) | 11.7 (1.14) |
| August 2020 | 770—10.60% (9.89–11.30) | 13.12 (10.73–15.50) | 56.36 (52.86–59.87) | 58.70 (4.17) | 6.10 (4.41–7.79) | 10.6 (3.21) |
| September 2020 | 751—8.55% (7.97–9.14) | 13.85 (11.38–16.32) | 53.93 (50.36–57.49) | 59.06 (5.35) | 3.99 (2.59–5.40) | 13.2 (2.22) |
| October 2020 | 1666—14.23% (13.60–14.86) | 13.03 (11.41–14.64) | 53.66 (51.27–56.06) | 61.84 (5.64) | 9.12 (7.74–10.51) | 12.4 (2.71) |
| November 2020 | 1756—15.18% (14.52–15.83) | 15.21 (13.53–16.88) | 53.82 (51.48–56.06) | 64.40 (5.46) | 11.56 (10.06–13.06) | 12.0 (3.77) |
| December 2020 | 1364—13.59% (12.92–14.26) | 15.40 (13.48–17.31) | 53.30 (50.65–55.95) | 66.35 (6.55) | 13.05 (11.26–14.84) | 14.6 (0.66) |
| January 2021 | 2300—22.36% (21.55–23.16) | 16.74 (15.21–18.26) | 55.39 (53.36–57.42) | 65.94 (3.69) | 12.35 (11.00–13.69) | 12.8 (4.06) |
| February 2021 | 1561—15.05% (14.36–15.74) | 19.09 (17.14–21.04) | 54.64 (52.17–57.11) | 64.69 (3.37) | 9.48 (8.03–10.93) | 12.0 (1.09) |
| March 2021 | 1219—10.90% (10.34–11.47) | 19.94 (17.75–22.12) | 56.00 (53.28–58.71) | 62.78 (2.24) | 7.94 (6.46–9.42) | 11.9 (3.34) |
| April 2021 | 9763—11.10% (10.51–11.69) | 18.05 (15.89–20.21) | 53.40 (50.60–56.20) | 61.08 (2.27) | 5.82 (4.51–7.14) | 13.1 (1.93) |
| May 2021 | 10,683—6.46% (6.01–6.91) | 14.50 (11.96–17.04) | 62.20 (58.70–65.69) | 57.96 (0.53) | 6.10 (4.37–7.82) | 10.1 (1.99) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aranda, J.; Loureiro-Amigo, J.; Murgadella, A.; Vàzquez, N.; Feria, L.; Muñoz, M.; Padulles, A.; Abelenda, G.; Garcia-Vidal, C.; Tuset, M.; et al. Changing Trends in the Global Consumption of Treatments Used in Hospitalized Patients for COVID-19: A Time Series Multicentre Study. Antibiotics 2023, 12, 809. https://doi.org/10.3390/antibiotics12050809
Aranda J, Loureiro-Amigo J, Murgadella A, Vàzquez N, Feria L, Muñoz M, Padulles A, Abelenda G, Garcia-Vidal C, Tuset M, et al. Changing Trends in the Global Consumption of Treatments Used in Hospitalized Patients for COVID-19: A Time Series Multicentre Study. Antibiotics. 2023; 12(5):809. https://doi.org/10.3390/antibiotics12050809
Chicago/Turabian StyleAranda, Judit, Jose Loureiro-Amigo, Anna Murgadella, Núria Vàzquez, Lucía Feria, Miriam Muñoz, Ariadna Padulles, Gabriela Abelenda, Carol Garcia-Vidal, Montse Tuset, and et al. 2023. "Changing Trends in the Global Consumption of Treatments Used in Hospitalized Patients for COVID-19: A Time Series Multicentre Study" Antibiotics 12, no. 5: 809. https://doi.org/10.3390/antibiotics12050809
APA StyleAranda, J., Loureiro-Amigo, J., Murgadella, A., Vàzquez, N., Feria, L., Muñoz, M., Padulles, A., Abelenda, G., Garcia-Vidal, C., Tuset, M., Albanell, M., Boix-Palop, L., Sanmartí-Martínez, N., Gómez-Zorrilla, S., Echeverria-Esnal, D., Rodriguez-Alarcón, A., Borjabad, B., Coloma, A., Carratalà, J., & Oriol, I. (2023). Changing Trends in the Global Consumption of Treatments Used in Hospitalized Patients for COVID-19: A Time Series Multicentre Study. Antibiotics, 12(5), 809. https://doi.org/10.3390/antibiotics12050809