
The African Wastewater Resistome: Identifying Knowledge Gaps to Inform Future Research Directions



Abstract
1. Introduction
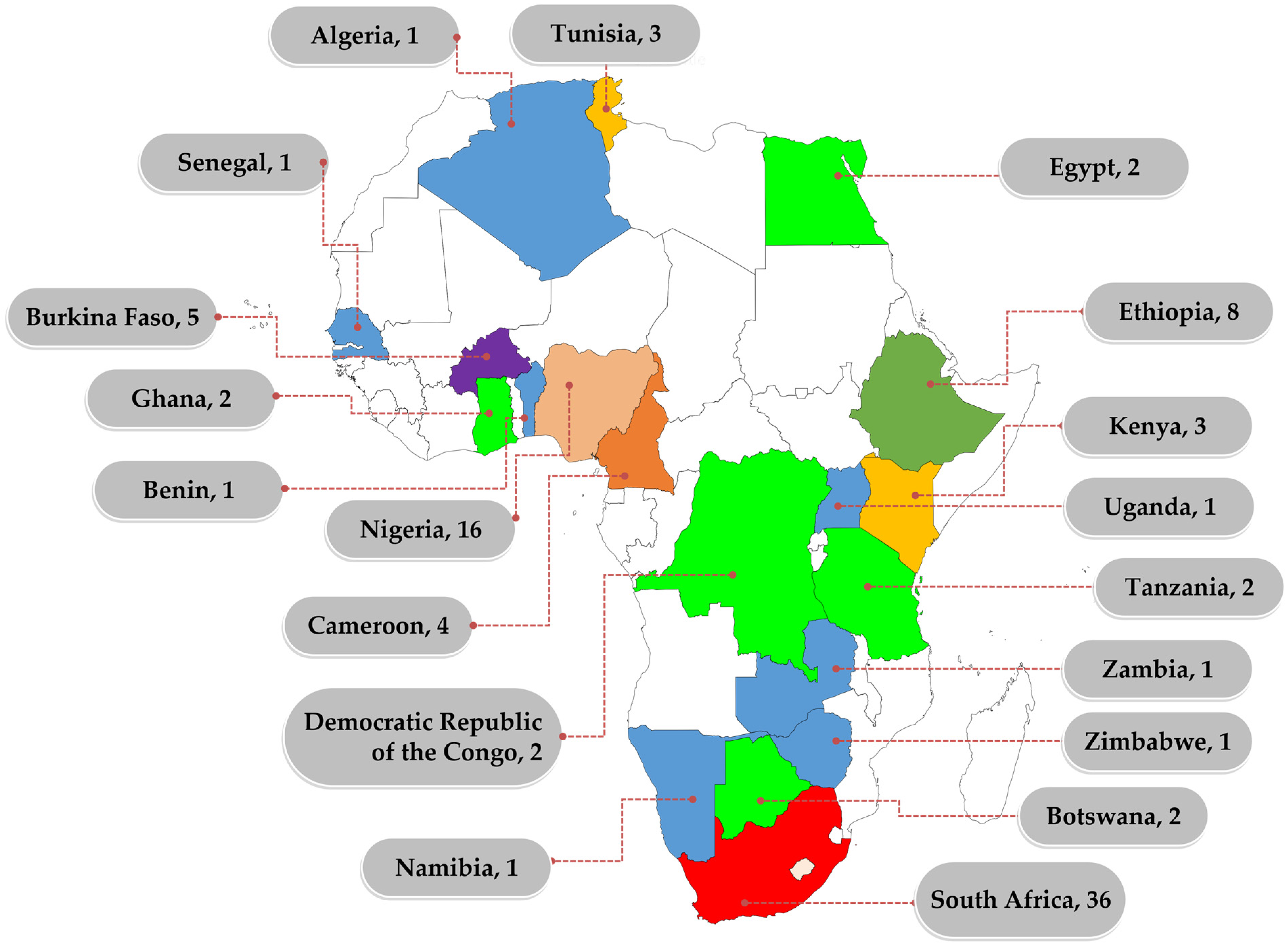
2. Overview of African Studies between 2012 and 2022
3. Case Study: South Africa
3.1. The South African Wastewater Resistome
3.2. Distribution of Studies by Province
3.3. Micro-organisms Targeted
3.4. AMR Determination Methods
3.5. Water Research Funding
4. Identifying Knowledge Gaps
4.1. Spatial (Geographical) Gaps
4.2. Methodological Gaps and Associated Challenges
4.3. Micro-organisms Gap
4.4. Reporting Gap
5. Proposed Future Perspective
- (i).
- There is a need to standardise protocols for assessing the WWTP resistome. This should consider the sampling regime, the sampling frequency, the organisms targeted, which antibiotics need to be tested and which methods should be used.
- (ii).
- There is a need to build capacity in sequencing technologies and bioinformatics, given the recent drift of the science to big data analysis.
- (iii).
- Funding must be made available to researchers as sequencing technologies are not yet widespread in the country, and the cost of using these facilities is still considerably high.
- (iv).
- Reporting of works on AMR in WWTPs needs to be improved, and there is a need to create a repository that would serve as a referral point for future studies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UN United Nations Meeting on Antimicrobial Resistance. Bull. World Health Organ. 2016, 94, 638–639. [CrossRef]
- World Health Organization United Nations High-Level Meeting on Antimicrobial Resistance. Available online: https://apps.who.int/mediacentre/events/2016/antimicrobial-resistance/en/index.html (accessed on 14 April 2023).
- WHO. Antimicrobial Resistance and the United Nations Sustainable Development Cooperation Framework. Guidance for United Nations Country Teams; WHO Press: Geneva, Switzerlan, 2021; pp. 1–24.
- Stanton, I.C.; Bethel, A.; Frances, A.; Leonard, C.; Gaze, W.H.; Garside, R. Existing Evidence on Antibiotic Resistance Exposure and Transmission to Humans from the Environment: A Systematic Map. Environ. Evid. 2022, 11, 8. [Google Scholar] [CrossRef]
- Essack, S.Y.; Sartorius, B. Global Antibiotic Resistance: Of Contagion, Confounders, and the COM-B Model. Lancet Planet. Health 2018, 2, e376–e377. [Google Scholar] [CrossRef]
- De Sosa, J.A.; Byarugaba, D.K.; Amabile-Cuevas, C.F.; Hsueh, P.R.; Kariuki, S.; Okeke, I.N. Antimicrobial Resistance in Developing Countries; Springer: New York, NY, USA, 2010; ISBN 9780387893709. [Google Scholar]
- Tiseo, K.; Huber, L.; Gilbert, M.; Robinson, T.P.; Van Boeckel, T.P. Global Trends in Antimicrobial Use in Food Animals from 2017 to 2030. Antibiotics 2020, 9, 918. [Google Scholar] [CrossRef]
- Kubone, P.Z.; Mlisana, K.P.; Govinden, U.; Abia, A.L.K.; Essack, S.Y. Antibiotic Susceptibility and Molecular Characterization of Uropathogenic Escherichia coli Associated with Community-Acquired Urinary Tract Infections in Urban and Rural Settings in South Africa. Trop. Med. Infect. Dis. 2020, 5, 176. [Google Scholar] [CrossRef]
- WHO Global Action Plan on Antimicrobial Resistance; WHO Document Production Services; WHO: Geneva, Switzerland, 2015.
- Chereau, F.; Opatowski, L.; Tourdjman, M.; Vong, S. Risk Assessment for Antibiotic Resistance in South East Asia. BMJ 2017, 358, j3393. [Google Scholar] [CrossRef]
- O’Neill, J. The Review on Antimicrobial Resistance Chaired by Jim O’Neill. 2015. Available online: https://amr-review.org/sites/default/files/Report-52.15.pdf (accessed on 3 February 2023).
- Proia, L.; Anzil, A.; Borrego, C.; Farrè, M.; Llorca, M.; Sanchis, J.; Bogaerts, P.; Balcázar, J.L.; Servais, P. Occurrence and Persistence of Carbapenemases Genes in Hospital and Wastewater Treatment Plants and Propagation in the Receiving River. J. Hazard. Mater. 2018, 358, 33–43. [Google Scholar] [CrossRef]
- Moslah, B.; Hapeshi, E.; Jrad, A.; Fatta-Kassinos, D.; Hedhili, A. Pharmaceuticals and Illicit Drugs in Wastewater Samples in North-Eastern Tunisia. Environ. Sci. Pollut. Res. 2018, 25, 18226–18241. [Google Scholar] [CrossRef]
- Sinthuchai, D.; Boontanon, S.K.; Boontanon, N.; Polprasert, C. Evaluation of Removal Efficiency of Human Antibiotics in Wastewater Treatment Plants in Bangkok, Thailand. Water Sci. Technol. 2016, 73, 182–191. [Google Scholar] [CrossRef]
- Li, X.; Shi, H.; Li, K.; Zhang, L.; Gan, Y. Occurrence and Fate of Antibiotics in Advanced Wastewater Treatment Facilities and Receiving Rivers in Beijing, China. Front. Environ. Sci. Eng. 2014, 8, 888–894. [Google Scholar] [CrossRef]
- Zhang, Y.; Marrs, C.F.; Simon, C.; Xi, C. Wastewater Treatment Contributes to Selective Increase of Antibiotic Resistance among Acinetobacter spp. Sci. Total Environ. 2009, 407, 3702–3706. [Google Scholar] [CrossRef]
- Omuferen, L.O.; Maseko, B.; Olowoyo, J.O. Occurrence of Antibiotics in Wastewater from Hospital and Convectional Wastewater Treatment Plants and Their Impact on the Effluent Receiving Rivers: Current Knowledge between 2010 and 2019. Environ. Monit. Assess. 2022, 194, 306. [Google Scholar] [CrossRef]
- Nkengasong, J.N.; Tessema, S.K. Africa Needs a New Public Health Order to Tackle Infectious Disease Threats. Cell 2020, 183, 296–300. [Google Scholar] [CrossRef]
- Sriram, A.; Kalanxhi, E.; Kapoor, G.; Craig, J.; Ruchita Balasubramanian, S.B.; Criscuolo, N.; Hamilton, A.; Klein, E.; Tseng, K.; Van Boeckel, T.; et al. The State of the World’s Antibiotics in 2021: A Global Analysis of Antimicrobial Resistance and Its Drivers; 2021. Available online: https://onehealthtrust.org/publications/reports/the-state-of-the-worlds-antibiotic-in-2021/ (accessed on 3 February 2023).
- Delgado-Blas, J.F.; Valenzuela Agüi, C.; Marin Rodriguez, E.; Serna, C.; Montero, N.; Saba, C.K.S.; Gonzalez-Zorn, B. Dissemination Routes of Carbapenem and Pan-Aminoglycoside Resistance Mechanisms in Hospital and Urban Wastewater Canalizations of Ghana. mSystems 2022, 7, e01019–e01021. [Google Scholar] [CrossRef]
- Akpan, S.N.; Odeniyi, O.A.; Adebowale, O.O.; Alarape, S.A.; Adeyemo, O.K. Antibiotic Resistance Profile of Gram-Negative Bacteria Isolated from Lafenwa Abattoir Effluent and Its Receiving Water (Ogun River) in Abeokuta, Ogun State, Nigeria. Onderstepoort J. Vet. Res. 2020, 87, 1–6. [Google Scholar] [CrossRef]
- Tesfaye, H.; Alemayehu, H.; Desta, A.F.; Eguale, T. Antimicrobial Susceptibility Profile of Selected Enterobacteriaceae in Wastewater Samples from Health Facilities, Abattoir, Downstream Rivers and a WWTP in Addis Ababa, Ethiopia. Antimicrob. Resist. Infect. Control 2019, 8, 134. [Google Scholar] [CrossRef]
- Marano, R.B.M.; Fernandes, T.; Manaia, C.M.; Nunes, O.; Morrison, D.; Berendonk, T.U.; Kreuzinger, N.; Telson, T.; Corno, G.; Fatta-Kassinos, D.; et al. A Global Multinational Survey of Cefotaxime-Resistant Coliforms in Urban Wastewater Treatment Plants. Environ. Int. 2020, 144, 106035. [Google Scholar] [CrossRef]
- Alouache, S.; Estepa, V.; Messai, Y.; Ruiz, E.; Torres, C.; Bakour, R. Characterization of ESBLs and Associated Quinolone Resistance in Escherichia coli and Klebsiella pneumoniae Isolates from an Urban Wastewater Treatment Plant in Algeria. Microb. Drug Resist. 2014, 20, 30–38. [Google Scholar] [CrossRef]
- Onalenna, O.; Rahube, T.O. Assessing Bacterial Diversity and Antibiotic Resistance Dynamics in Wastewater Effluent-Irrigated Soil and Vegetables in a Microcosm Setting. Heliyon 2022, 8, e09089. [Google Scholar] [CrossRef]
- Tapela, K.; Rahube, T. Isolation and Antibiotic Resistance Profiles of Bacteria from Influent, Effluent and Downstream: A Study in Botswana. Afr. J. Microbiol. Res. 2019, 13, 279–289. [Google Scholar] [CrossRef]
- Soré, S.; Sawadogo, Y.; Bonkoungou, J.I.; Kaboré, S.P.; Béogo, S.; Sawadogo, C.; Bationo, B.G.; Ky, H.; Madingar, P.D.-M.; Ouédraogo, A.S.; et al. Detection, Identification and Characterization of Extended-Spectrum Beta-Lactamases Producing Enterobacteriaceae in Wastewater and Salads Marketed in Ouagadougou, Burkina Faso. Int. J. Biol. Chem. Sci. 2020, 14, 2746–2757. [Google Scholar] [CrossRef]
- Abasse, O.; Boukaré, K.; Sampo, E.; Bouda, R.; CISSE, H.; Stéphane, K.; Odetokun, I.; Sawadogo, A.; Henri Nestor, B.; Savadogo, A. Spread and Antibiotic Resistance Profile of Pathogens Isolated from Human and Hospital Wastewater in Ouagadougou. Microbes Infect. Dis. 2022, 3, 318–331. [Google Scholar] [CrossRef]
- Bougnom, B.P.; McNally, A.; Etoa, F.X.; Piddock, L.J. Antibiotic Resistance Genes Are Abundant and Diverse in Raw Sewage Used for Urban Agriculture in Africa and Associated with Urban Population Density. Environ. Pollut. 2019, 251, 146–154. [Google Scholar] [CrossRef]
- Mekengo, B.M.; Hussein, S.; Ali, M.M. Distribution and Antimicrobial Resistance Profile of Bacteria Recovered from Sewage System of Health Institutions Found in Hawassa, Sidama Regional State, Ethiopia: A Descriptive Study. SAGE Open Med. 2021, 9, 205031212110390. [Google Scholar] [CrossRef]
- Asfaw, T.; Negash, L.; Kahsay, A.; Weldu, Y. Antibiotic Resistant Bacteria from Treated and Untreated Hospital Wastewater at Ayder Referral Hospital, Mekelle, North Ethiopia. Adv. Microbiol. 2017, 7, 871–886. [Google Scholar] [CrossRef]
- Adomako, L.A.B.; Yirenya-Tawiah, D.; Nukpezah, D.; Abrahamya, A.; Labi, A.K.; Grigoryan, R.; Ahmed, H.; Owusu-Danquah, J.; Annang, T.Y.; Banu, R.A.; et al. Reduced Bacterial Counts from a Sewage Treatment Plant but Increased Counts and Antibiotic Resistance in the Recipient Stream in Accra, Ghana—A Cross-Sectional Study. Trop. Med. Infect. Dis. 2021, 6, 79. [Google Scholar] [CrossRef]
- Wawire, S.A.; Reva, O.N.; O’Brien, T.J.; Figueroa, W.; Dinda, V.; Shivoga, W.A.; Welch, M. Virulence and Antimicrobial Resistance Genes Are Enriched in the Plasmidome of Clinical Escherichia coli Isolates Compared with Wastewater Isolates from Western Kenya. Infect. Genet. Evol. 2021, 91, 104784. [Google Scholar] [CrossRef]
- Mutuku, C. Antibiotic Resistance Profiles among Enteric Bacteria Isolated from Wastewater in Septic Tanks 2017. Am. Sci. Res. J. Eng. Technol. Sci. 2017, 27, 99–107. [Google Scholar]
- Song’oro, E.; Nyerere, A.; Magoma, G.; Gunturu, R. Occurrence of Highly Resistant Microorganisms in Ruai Wastewater Treatment Plant and Dandora Dumpsite in Nairobi County, Kenya. Adv. Microbiol. 2019, 9, 479–494. [Google Scholar] [CrossRef]
- Alpha, A.D.; Delphine, B.; Fatou, T.L.; Mbaye, M.; Mohamed, M.S.; Moussa, D.; Yacine, S.; Monique, K.; Rianatou, A.; Yaya, T.; et al. Prevalence of Pathogenic and Antibiotics Resistant Escherichia coli from Effluents of a Slaughterhouse and a Municipal Wastewater Treatment Plant in Dakar. African J. Microbiol. Res. 2017, 11, 1035–1042. [Google Scholar] [CrossRef]
- Mbanga, J.; Amoako, D.G.; Abia, A.L.K.; Allam, M.; Ismail, A.; Essack, S.Y. Genomic Analysis of Enterococcus spp. Isolated from a Wastewater Treatment Plant and Its Associated Waters in Umgungundlovu District, South Africa. Front. Microbiol. 2021, 12, 648454. [Google Scholar] [CrossRef]
- Mhongole, O.J.; Mdegela, R.H.; Kusiluka, L.J.M.; Forslund, A.; Dalsgaard, A. Characterization of Salmonella spp. from Wastewater Used for Food Production in Morogoro, Tanzania. World J. Microbiol. Biotechnol. 2017, 33, 42. [Google Scholar] [CrossRef]
- Rafraf, I.D.; Lekunberri, I.; Sànchez-Melsió, A.; Aouni, M.; Borrego, C.M.; Balcázar, J.L. Abundance of Antibiotic Resistance Genes in Five Municipal Wastewater Treatment Plants in the Monastir Governorate, Tunisia. Environ. Pollut. 2016, 219, 353–358. [Google Scholar] [CrossRef]
- Afema, J.A.; Byarugaba, D.K.; Shah, D.H.; Atukwase, E.; Nambi, M.; Sischo, W.M. Potential Sources and Transmission of Salmonella and Antimicrobial Resistance in Kampala, Uganda. PLoS ONE 2016, 11, e0152130. [Google Scholar] [CrossRef]
- Mubbunu, L.; Siyumbi, S.; Katongo, C.; Mwambungu, A. Waste Water as Reservoir of Antibiotic Resistant Micro-Organisms: A Case of Luanshya Waste Water Ponds. Int. J. Res. Med. Health Sci. 2014, 4, 9. [Google Scholar]
- Gufe, C.; Ndlovu, M.N.; Sibanda, Z.; Makuvara, Z.; Marumure, J. Prevalence and Antimicrobial Profile of Potentially Pathogenic Bacteria Isolated from Abattoir Effluents in Bulawayo, Zimbabwe. Sci. African 2021, 14, e01059. [Google Scholar] [CrossRef]
- Gasson, J.; Blockman, M.; Willems, B. Antibiotic Prescribing Practice and Adherence to Guidelines in Primary Care in the Cape Town Metro District, South Africa. S. Afr. Med. J. 2018, 108, 304–310. [Google Scholar] [CrossRef]
- DWS—South African Department of Water and Sanitation. Green Drop National Report 2022; Department of Water Affairs: Pretoria, South Africa, 2022.
- Devane, M.L.; Moriarty, E.; Weaver, L.; Cookson, A.; Gilpin, B. Fecal Indicator Bacteria from Environmental Sources; Strategies for Identification to Improve Water Quality Monitoring. Water Res. 2020, 185, 116204. [Google Scholar] [CrossRef]
- Liang, L.; Goh, S.G.; Vergara, G.G.R.V.; Fang, H.M.; Rezaeinejad, S.; Chang, S.Y.; Bayen, S.; Lee, W.A.; Sobsey, M.D.; Rose, J.B.; et al. Alternative Fecal Indicators and Their Empirical Relationships with Enteric Viruses, Salmonella enterica, and Pseudomonas aeruginosa in Surface Waters of a Tropical Urban Catchment. Appl. Environ. Microbiol. 2015, 81, 850–860. [Google Scholar] [CrossRef]
- Field, K.G.; Samadpour, M. Fecal Source Tracking, the Indicator Paradigm, and Managing Water Quality. Water Res. 2007, 41, 3517–3538. [Google Scholar] [CrossRef]
- Saxena, G.; Bharagava, R.N.; Kaithwas, G.; Raj, A. Microbial Indicators, Pathogens and Methods for Their Monitoring in Water Environment. J. Water Health 2015, 13, 319–339. [Google Scholar] [CrossRef]
- Harwood, V.; Shanks, O.; Koraijkic, A.; Verbyla, M.; Ahmed, W.; Iriate, M. General and Host- Associated Bacterial Indicators of Faecal Pollution. 2017. Available online: https://www.waterpathogens.org/book/bacterial-indicators (accessed on 3 February 2023).
- Anjum, M.F.; Schmitt, H.; Börjesson, S.; Berendonk, T.U.; Donner, E.; Stehling, E.G.; Boerlin, P.; Topp, E.; Jardine, C.; Li, X.; et al. The Potential of Using E. coli as an Indicator for the Surveillance of Antimicrobial Resistance (AMR) in the Environment. Curr. Opin. Microbiol. 2021, 64, 152–158. [Google Scholar] [CrossRef]
- Coetzee, I.; Bezuidenhout, C.C.; Bezuidenhout, J.J. Triclosan Resistant Bacteria in Sewage Effluent and Cross-Resistance to Antibiotics. Water Sci. Technol. 2017, 76, 1500–1509. [Google Scholar] [CrossRef]
- Eze, E.C.; El Zowalaty, M.E.; Pillay, M. Antibiotic Resistance and Biofilm Formation of Acinetobacter baumannii Isolated from High-Risk Effluent Water in Tertiary Hospitals in South Africa. J. Glob. Antimicrob. Resist. 2021, 27, 82–90. [Google Scholar] [CrossRef]
- Mapipa, Q.; Digban, T.O.; Nnolim, N.E.; Nontongana, N.; Okoh, A.I.; Nwodo, U.U. Molecular Characterization and Antibiotic Susceptibility Profile of Acinetobacter baumannii Recovered from Hospital Wastewater Effluents. Curr. Microbiol. 2022, 79, 123. [Google Scholar] [CrossRef]
- Govender, R.; Amoah, I.D.; Kumari, S.; Bux, F.; Stenström, T.A. Detection of Multidrug Resistant Environmental Isolates of Acinetobacter and Stenotrophomonas maltophilia: A Possible Threat for Community Acquired Infections? J. Environ. Sci. Heal. Part A Toxic/Hazardous Subst. Environ. Eng. 2020, 56, 213–225. [Google Scholar] [CrossRef]
- Mann, B.C.; Bezuidenhout, J.J.; Bezuidenhout, C.C. Biocide Resistant and Antibiotic Cross-Resistant Potential Pathogens from Sewage and River Water from a Wastewater Treatment Facility in the North-West, Potchefstroom, South Africa. Water Sci. Technol. 2019, 80, 551–562. [Google Scholar] [CrossRef]
- Igbinosa, I.H.; Okoh, A.I. Antibiotic Susceptibility Profile of Aeromonas Species Isolated from Wastewater Treatment Plant. Sci. World J. 2012, 2012, 764563. [Google Scholar] [CrossRef]
- Olaniran, A.O.; Nzimande, S.B.T.; Mkize, N.G. Antimicrobial Resistance and Virulence Signatures of Listeria and Aeromonas Species Recovered from Treated Wastewater Effluent and Receiving Surface Water in Durban, South Africa. BMC Microbiol. 2015, 15, 234. [Google Scholar] [CrossRef]
- Govender, R.; Amoah, I.D.; Adegoke, A.A.; Singh, G.; Kumari, S.; Swalaha, F.M.; Bux, F.; Stenström, T.A. Identification, Antibiotic Resistance, and Virulence Profiling of Aeromonas and Pseudomonas Species from Wastewater and Surface Water. Environ. Monit. Assess. 2021, 193, 294. [Google Scholar] [CrossRef]
- Ndlovu, T.; Rautenbach, M.; Vosloo, J.A.; Khan, S.; Khan, W. Characterisation and Antimicrobial Activity of Biosurfactant Extracts Produced by Bacillus amyloliquefaciens and Pseudomonas aeruginosa Isolated from a Wastewater Treatment Plant. AMB Express 2017, 7, 108. [Google Scholar] [CrossRef]
- Gumede, S.N.; Abia, A.L.K.; Amoako, D.G.; Essack, S.Y. Analysis of Wastewater Reveals the Spread of Diverse Extended-Spectrum β-Lactamase-Producing E. coli Strains in Umgungundlovu District, South Africa. Antibiotics 2021, 10, 860. [Google Scholar] [CrossRef]
- Adegoke, A.A.; Madu, C.E.; Aiyegoro, O.A.; Stenström, T.A.; Okoh, A.I. Antibiogram and Beta-Lactamase Genes among Cefotaxime Resistant E. coli from Wastewater Treatment Plant. Antimicrob. Resist. Infect. Control 2020, 9, 46. [Google Scholar] [CrossRef]
- Pillay, L.; Olaniran, A.O. Assessment of Physicochemical Parameters and Prevalence of Virulent and Multiple-Antibiotic-Resistant Escherichia coli in Treated Effluent of Two Wastewater Treatment Plants and Receiving Aquatic Milieu in Durban, South Africa. Environ. Monit. Assess. 2016, 188, 260. [Google Scholar] [CrossRef]
- Adefisoye, M.A.; Okoh, A.I.; Africa, S.; Adefisoye, M.A.; Okoh, A.I. Ecological and Public Health Implications of the Discharge of Multidrug-Resistant Bacteria and Physicochemical Contaminants from Treated Wastewater Effluents in the Eastern Cape, South Africa. Water 2017, 9, 562. [Google Scholar] [CrossRef]
- Adefisoye, M.A.; Okoh, A.I. Identification and Antimicrobial Resistance Prevalence of Pathogenic Escherichia coli Strains from Treated Wastewater Effluents in Eastern Cape, South Africa. Microbiologyopen 2016, 5, 143–151. [Google Scholar] [CrossRef]
- Nzima, B.; Adegoke, A.A.; Ofon, U.A.; Al-Dahmoshi, H.O.M.; Saki, M.; Ndubuisi-Nnaji, U.U.; Inyang, C.U. Resistotyping and Extended-Spectrum Beta-Lactamase Genes among Escherichia coli from Wastewater Treatment Plants and Recipient Surface Water for Reuse in South Africa. New Microbes New Infect. 2020, 38, 100803. [Google Scholar] [CrossRef]
- Osuolale, O.; Okoh, A. Human Enteric Bacteria and Viruses in Five Wastewater Treatment Plants in the Eastern Cape, South Africa. J. Infect. Public Health 2017, 10, 541–547. [Google Scholar] [CrossRef]
- Igwaran, A.; Iweriebor, B.C.; Okoh, A.I. Molecular Characterization and Antimicrobial Resistance Pattern of Escherichia coli Recovered from Wastewater Treatment Plants in Eastern Cape South Africa. Int. J. Environ. Res. Public Health 2018, 15, 1237. [Google Scholar] [CrossRef]
- Mbanga, J.; Abia, A.L.K.; Amoako, D.G.; Essack, S.Y. Longitudinal Surveillance of Antibiotic Resistance in Escherichia coli and Enterococcus spp. From a Wastewater Treatment Plant and Its Associated Waters in KwaZulu-Natal, South Africa. Microb. Drug Resist. 2021, 27, 904–918. [Google Scholar] [CrossRef]
- Fadare, F.T.; Okoh, A.I. Distribution and Molecular Characterization of ESBL, PAmpC β-Lactamases, and Non-β-Lactam Encoding Genes in Enterobacteriaceae Isolated from Hospital Wastewater in Eastern Cape Province, South Africa. PLoS ONE 2021, 16, e0254753. [Google Scholar] [CrossRef]
- Molale-Tom, L.G.; Bezuidenhout, C.C. Prevalence, Antibiotic Resistance and Virulence of Enterococcus spp. From Wastewater Treatment Plant Effluent and Receiving Waters in South Africa. J. Water Health 2020, 18, 753–765. [Google Scholar] [CrossRef] [PubMed]
- Hamiwe, T.; Kock, M.M.; Magwira, C.A.; Antiabong, J.F.; Ehlers, M.M. Occurrence of Enterococci Harbouring Clinically Important Antibiotic Resistance Genes in the Aquatic Environment in Gauteng, South Africa. Environ. Pollut. 2019, 245, 1041–1049. [Google Scholar] [CrossRef] [PubMed]
- Ekwanzala, M.D.; Dewar, J.B.; Kamika, I.; Momba, M.N.B. Comparative Genomics of Vancomycin-Resistant Enterococcus spp. Revealed Common Resistome Determinants from Hospital Wastewater to Aquatic Environments. Sci. Total Environ. 2020, 719, 137275. [Google Scholar] [CrossRef] [PubMed]
- King, T.L.B.; Schmidt, S.; Essack, S.Y. Antibiotic Resistant Klebsiella spp. from a Hospital, Hospital Effluents and Wastewater Treatment Plants in the UMgungundlovu District, KwaZulu-Natal, South Africa. Sci. Total Environ. 2020, 712, 135550. [Google Scholar] [CrossRef]
- Hosu, M.C.; Vasaikar, S.; Okuthe, G.E.; Apalata, T. Molecular Detection of Antibiotic-Resistant Genes in Pseudomonas aeruginosa from Nonclinical Environment: Public Health Implications in Mthatha, Eastern Cape Province, South Africa. Int. J. Microbiol. 2021, 2021, 8861074. [Google Scholar] [CrossRef]
- Odjadjare, E.E.; Igbinosa, E.O.; Mordi, R.; Igere, B.; Igeleke, C.L.; Okoh, A.I. Prevalence of Multiple Antibiotics Resistant (MAR) Pseudomonas Species in the Final Effluents of Three Municipal Wastewater Treatment Facilities in South Africa. Int. J. Environ. Res. Public Health 2012, 9, 2092–2107. [Google Scholar] [CrossRef]
- Odjadjare, E.C.; Olaniran, A.O. Prevalence of Antimicrobial Resistant and Virulent Salmonella spp. in Treated Effluent and Receiving Aquatic Milieu of Wastewater Treatment Plants in Durban, South Africa. Int. J. Environ. Res. Public Health 2015, 12, 9692–9713. [Google Scholar] [CrossRef]
- Ramessar, K.; Olaniran, A.O. Antibiogram and Molecular Characterization of Methicillin-Resistant Staphylococcus aureus Recovered from Treated Wastewater Effluent and Receiving Surface Water in Durban, South Africa. World J. Microbiol. Biotechnol. 2019, 35, 142. [Google Scholar] [CrossRef]
- Okoh, A.I.; Sibanda, T.; Nongogo, V.; Adefisoye, M.; Olayemi, O.O.; Nontongana, N. Prevalence and Characterisation of Non-Cholerae Vibrio Spp. in Final Effluents of Wastewater Treatment Facilities in Two Districts of the Eastern Cape Province of South Africa: Implications for Public Health. Environ. Sci. Pollut. Res. 2015, 22, 2008–2017. [Google Scholar] [CrossRef]
- Olayinka Osuolale, A.O. Isolation and Antibiotic Profile Of Pakistan. J. Nutr. 2018, 10, 982–986. [Google Scholar]
- Jiang, L. Comparison of Disk Diffusion, Agar Dilution, and Broth Microdilution for Antimicrobial Susceptibility Testing of Five Chitosans. Fujian Agric. For. Univ. China 2011, 24–27. [Google Scholar]
- Cartwright, E.J.P.; Paterson, G.K.; Raven, K.E.; Harrison, E.M.; Gouliouris, T.; Kearns, A.; Pichon, B.; Edwards, G.; Skov, R.L.; Larsen, A.R.; et al. Use of Vitek 2 Antimicrobial Susceptibility Profile to Identify MecC in Methicillin-Resistant Staphylococcus aureus. J. Clin. Microbiol. 2013, 51, 2732–2734. [Google Scholar] [CrossRef]
- Kuchibiro, T.; Komatsu, M.; Yamasaki, K.; Nakamura, T.; Niki, M. Evaluation of the VITEK2 AST–XN17 Card for the Detection of Carbapenemase—Producing Enterobacterales in Isolates Primarily Producing Metallo β—Lactamase. Eur. J. Clin. Microbiol. Infect. Dis. 2022, 41, 723–732. [Google Scholar] [CrossRef]
- Vasala, A.; Hytönen, V.P.; Laitinen, O.H. Modern Tools for Rapid Diagnostics of Antimicrobial Resistance. Front. Cell. Infect. Microbiol. 2020, 10, 308. [Google Scholar] [CrossRef]
- Ekwanzala, M.D.; Dewar, J.B.; Momba, M.N.B. Environmental Resistome Risks of Wastewaters and Aquatic Environments Deciphered by Shotgun Metagenomic Assembly. Ecotoxicol. Environ. Saf. 2020, 197, 110612. [Google Scholar] [CrossRef]
- Mbanga, J.; Amoako, D.G.; Abia, A.L.K.; Fatoba, D.; Essack, S. Genomic Analysis of Antibiotic-Resistant Enterobacter Spp. from Wastewater Sources in South Africa: The First Report of the Mobilisable Colistin Resistance Mcr-10 Gene in Africa. Ecol. Genet. Genomics 2021, 21, 100104. [Google Scholar] [CrossRef]
- Coorevits, L.; Boelens, J.; Claeys, G. Direct Susceptibility Testing by Disk Diffusion on Clinical Samples: A Rapid and Accurate Tool for Antibiotic Stewardship. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1207–1212. [Google Scholar] [CrossRef]
- Gajic, I.; Kabic, J.; Kekic, D.; Jovicevic, M.; Milenkovic, M.; Mitic Culafic, D.; Trudic, A.; Ranin, L.; Opavski, N. Antimicrobial Susceptibility Testing: A Comprehensive Review of Currently Used Methods. Antibiotics 2022, 11, 427. [Google Scholar] [CrossRef]
- Hendriksen, R.S.; Bortolaia, V.; Tate, H.; Tyson, G.H.; Aarestrup, F.M.; McDermott, P.F. Using Genomics to Track Global Antimicrobial Resistance. Front. Public Health 2019, 7, 242. [Google Scholar] [CrossRef]
- Igbinosa, I.H.; Nwodo, U.U.; Sosa, A.; Tom, M.; Okoh, A.I. Commensal Pseudomonas Species Isolated from Wastewater and Freshwater Milieus in the Eastern Cape Province, South Africa, as Reservoir of Antibiotic Resistant Determinants. Int. J. Environ. Res. Public Health 2012, 9, 2537–2549. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, L.; Joffre, E.; Rivera, R.; Sjöling, Å.; Svennerholm, A.M.; Iñiguez, V. Prevalence, Seasonality and Severity of Disease Caused by Pathogenic Escherichia coli in Children with Diarrhoea in Bolivia. J. Med. Microbiol. 2013, 62, 1697–1706. [Google Scholar] [CrossRef] [PubMed]
- Munksgaard, D.G.; Young, J.C. Flow and Load Variations at Wastewater Treatment Plants. J. Water Pollut. Control Fed. 1980, 52, 2131–2144. [Google Scholar]
- Alhumaid, S.; Al Mutair, A.; Al Alawi, Z.; Alzahrani, A.J.; Tobaiqy, M.; Alresasi, A.M.; Bu-Shehab, I.; Al-Hadary, I.; Alhmeed, N.; Alismail, M.; et al. Antimicrobial Susceptibility of Gram-Positive and Gram-Negative Bacteria: A 5-Year Retrospective Analysis at a Multi-Hospital Healthcare System in Saudi Arabia. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 43. [Google Scholar] [CrossRef]
- Jubeh, B.; Breijyeh, Z.; Karaman, R. Resistance of Gram-Positive Bacteria to Current Antibacterial Agents and Overcoming Approaches. Molecules 2020, 25, 2888. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.J. Dissemination of Research Results: On the Path to Practice Change. Can. J. Hosp. Pharm. 2015, 68, 465–468. [Google Scholar] [CrossRef]
- Ross-Hellauer, T.; Tennant, J.P.; Banelytė, V.; Gorogh, E.; Luzi, D.; Kraker, P.; Pisacane, L.; Ruggieri, R.; Sifacaki, E.; Vignoli, M. Ten Simple Rules for Innovative Dissemination of Research. PLoS Comput. Biol. 2020, 16, e1007704. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | & Wastewater Type/Source | Duration of Study | Sample Size | Targeted Resistance | Phenotypic (P)/Genotypic (G) Resistance | Method | Reference |
|---|---|---|---|---|---|---|---|
| * South Africa | WWTP | Two campaigns—actual duration not mentioned | # Not indicated | Cefotaxime-resistance | P | Culture | [23] |
| Algeria | WWTP | 3 days in 2 months | Not indicated | ESBLs and associated quinolone resistance | P, G | Culture; PCR | [24] |
| Botswana | WWTP | $ One-off sampling | one | Overall resistome | G | Shotgun metagenomics | [25] |
| Botswana | WWTP | Monthly for 1 year | 72 | General resistance—9 antibiotics tested | P | Culture | [26] |
| Burkina Faso | Urban channel | 6 months | 101 | ESBLs | P | Culture | [27] |
| Burkina Faso | WWTP | Monthly for 5 months | 15 | General resistance—19 antibiotics | P | Culture | [28] |
| Cameroon | Open-air canals | One-off | 6 (composite) samples | Overall resistome | G | Shotgun metagenomics | [29] |
| Ethiopia | Hospital wastewater | 3 months | 27 | General resistance—13 antibiotics | P | Culture | [30] |
| Ethiopia | Hospital wastewater | 4 months | 40 (composite samples) | General resistance—13 antibiotics | P | Culture | [31] |
| Ghana | WWTP | Monthly—6 months | 30 | General resistance | P | Culture | [32] |
| Kenya | University WWTP | 4 months | Not mentioned | Overall resistome | P, G | Culture; whole-genome sequencing | [33] |
| Kenya | Septic tank | 2 months | Not mentioned | General resistance | P | Culture | [34] |
| Kenya | WWTP | 6 months (covering the dry and rainy seasons) | 24 | General resistance | P | Culture | [35] |
| Nigeria | Hospital WWTP | Weekly for 4 months | Not mentioned | ESBLs | P, G | Culture; PCR | Adekanmbi |
| Senegal | Slaughterhouse wastewater and WWTP | Not mentioned | Not mentioned | General resistance—16 antibiotics | P | Culture | [36] |
| South Africa | WWTP | 7 months (Every two weeks) | 81 | Overall resistome | P, G | Culture; whole-genome sequencing | [37] |
| Tanzania | WWTP | 2013/2014 (Not specific) | 52 | General resistance—14 antibiotics | P | Microdilution | [38] |
| Tunisia | WWTP | Not mentioned | Not mentioned | intI1, ARGs blaCTX-M, blaTEM, qnrA, qnrS, sul I, ermB | G | PCR | [39] |
| Uganda | Multiple sources | Not mentioned | Not mentioned | General resistance—15 antibiotics | P | Culture | [40] |
| Zambia | Wastewater ponds | Not mentioned | 5 samples | General resistance—8 antibiotics | P | Culture | [41] |
| Zimbabwe | Abattoir wastewater | 3 months | 600 samples | General resistance—16 antibiotics | P | Culture | [42] |
| Organism | Media | Incubation Temperature (°C) | Duration (Hours) | Reference |
|---|---|---|---|---|
| Brevibacillus spp.; Paenibacillus spp. | R2A media | Not mentioned (NM) | NM | [51] |
| Acinetobacter baumannii | Leeds Acinetobacter Medium | 37 | 24 | [52] |
| Acinetobacter baumannii; Acinetobacter spp. | CHROMagar Acinetobacter | 37 | 18–24 | [53,54] |
| Aeromonas, Exiguobacterium | Nutrient agar, Blood agar | NM | NM | [55] |
| Aeromonas spp. | Glutamate Starch Phenol-red (GSP) agar plates | 37 | 24 | [56] |
| Aeromonas spp. | Rimler-Shotts agar | 37 | 20 | [57] |
| Aeromonas spp. | Aeromonas spp. Isolation agar | 37 | 24 | [58] |
| Bacillus amyloliquefaciens | nutrient agar | 37 | 18–24 | [59] |
| Bacillus spp. | Nutrient agar, Blood agar | NM | NM | [55] |
| Bacillus spp. | R2A media | NM | NM | [51] |
| E. coli | Eosin methylene blue agar | 37 | 24 | [60] |
| E. coli | Membrane Fecal Coliform (mFC) agar supplemented with 4 mg/L or 8 mg/L cefotaxime antibiotic | 37 | 24 | [61] |
| E. coli | Chromocult Coliform Agar (Merck) | 37 | 24 | [62] |
| E. coli | E. coli-Coliforms Chromogenic medium | 37 | 24 | [63,64] |
| E. coli | CHROMagar ECC | 37 | 24 | [65] |
| E. coli | E. coli-coliform selective agar | 37 | 24 | [66] |
| E. coli | Chromogenic agar * | 37 | 24 | [67] |
| E. coli | Colilert-18TM | 37 | 24 | [68] |
| Enterobacteriaceae | Violet Red Bile Glucose (VRBG) agar | 37 | 18 | [69] |
| Enterococcus spp. | R2A media | NM | NM | [51] |
| Enterococcus spp. | KF-Streptococcus agar containing 1 mL of 2,3,5-Triphenyltetrazolium chloride | 37 | 48 | [70] |
| Enterococcus spp. | chromogenic 51,759 HiCrome™ Rapid Enterococci Agar media | 37 | 24–48 | [71] |
| Enterococcus spp. | Tryptic Soy Broth | 37 | 18 | [67] |
| Enterococcus spp. | Bile Aesculin Azide Agar | 37 | 24 | [67] |
| Enterococcus spp. | CHROMagar™ VRE, BBL™ Enterococcosel™ Broth | 37 ± 2 °C | 18 to 24 | [72] |
| Enterococcus spp. | EnterolertTM | 41 | 24–48 | [68] |
| Klebsiella spp. | Nutrient agar, Blood agar | NM | NM | [55] |
| Klebsiella spp. | HiCrome Klebsiella selective agar | 35 | 24 | [73] |
| Listeria spp. | Listeria Chromogenic agar | 35 | 24–48 | [57] |
| Pseudomonas aeruginosa | Mineral salt medium | 30 | 18–24 | [59] |
| Pseudomonas aeruginosa | CHROMagarTM Pseudomonas | 37 | 24–48 | [74] |
| Pseudomonas spp. | Nutrient agar, Blood agar | NM | NM | [55] |
| Pseudomonas spp. | R2A media | NM | NM | [51] |
| Pseudomonas spp. | Pseudomonas Isolation Agar | 35 | 24–48 | [75] |
| Pseudomonas spp. | Cetrimide agar | 37 | 24 | [58] |
| Pseudomonas spp. | Glutamate Starch Phenol-red (GSP) agar | 37 | 24 | [56] |
| Salmonella spp. | Salmonella-Shigella (SS) agar | 37 | 24–48 | [76] |
| Shewanella spp. | Nutrient agar, Blood agar | NM | NM | [55] |
| Staphylococcus aureus | Mannitol Salt Agar supplemented with cefoxitin. | Not mentioned (NM) | NM | [77] |
| Stenotrophomonas maltophilia | Stenotrophomonas selective agar base with Vancomycin Imipenem Amphotericin B (VIA) supplement | 37 | 18 to 24 | [54] |
| Vibrio spp. | thiosulfate-citrate–bile salt-sucrose (TCBS) agar | 37 | 24 | [63,78,79] |
| Organism(s) | Antibiotics Tested (n = Number Tested) | Phenotypic Resistance | Genotypic Resistance | Method | Reference |
|---|---|---|---|---|---|
| E. coli | n = 23: Amoxicillin/clavulanic acid, amoxicillin, amikacin, ampicillin, cefepime, cephalothin, cefotaxime, cefoxitin, cefixime, nalidixic acid, ceftazidime, cephalexin, cefuroxime, chloramphenicol, ciprofloxacin, gentamicin, imipenem, meropenem, nitrofurantoin, piperacillin, tetracycline, tigecycline, trimethoprim/Sulfamethoxazole. | Amoxicillin/clavulanic acid, amoxicillin, amikacin, ampicillin, cefepime, cephalothin, cefotaxime, cefoxitin, cefixime, ceftazidime, cephalexin, cefuroxime, chloramphenicol, ciprofloxacin, gentamicin, imipenem, meropenem, nitrofurantoin, piperacillin, tetracycline, tigecycline, nalidixic acid, trimethoprim/Sulfamethoxazole. | TEM, SHV, CTX-M | DD/PCR-Sanger Sequencing | [60] |
| E. coli | n = 8: Meropenem, colistin, amoxicillin/clavulanic, ciprofloxacin, nitrofurantoin trimethoprim/sulfamethoxazol, gentamicin, tetracycline. | Colistin, amoxicillin-clavulanic, ciprofloxacin, trimethoprimsulphamethoxazole, gentamicin, tetracycline, nitrofurantoin. | TEM, SHV, CTX-M, VIM, OXA-1, KPC-2, NDM-1 | DD/PCR | [61] |
| S. aureus | n = 20: Amikacin, Gentamicin, Amoxicillin/clavulanic acid, Ampicillin, Oxacillin, Penicillin, Imipenem, Cefoxitin, Cefozolin, Ciprofloxacin, Norfloxacin, Vancomycin, Clindamycin, Lincomycin, Azithromycin, Erythromycin, Chloramphenicol, Rifampicin, Tetracycline Sulfamethoxazole/trimethoprim. | Amikacin, Gentamicin, Amoxicillin/clavulanic acid, Ampicillin, Oxacillin, Penicillin, Imipenem, Cefoxitin, Cefozolin, Norfloxacin, Vancomycin, Clindamycin, Lincomycin, Azithromycin, Erythromycin, Chloramphenicol, Rifampicin, Sulfamethoxazole/trimethoprim, Tetracycline. | aac(6′)/aph(2″), blaZ, ermC, msrA and tetK, | DD/PCR | [77] |
| Klebsiella spp. | n = 16: Amoxicillin-clavulanic acid, piperacillin-tazobactam, cefotaxime, ceftazidime, cefalexin, cefoxitin, ertapenem, meropenem, doripenem, imipenem, aztreonam, ciprofloxacin, norfloxacin, moxifloxacin, gentamicin, tobramycin. | Amoxicillin-clavulanic acid, piperacillin-tazobactam, cefotaxime, ceftazidime, cefalexin, cefoxitin, ertapenem, doripenem, aztreonam, ciprofloxacin, norfloxacin, moxifloxacin, gentamicin, tobramycin. | DD | [73] | |
| Aeromonas spp. | n = 20: Ciprofloxacin, Trimethoprim, Ofloxacin, Chloramphenicol, Penicillins, Clindamycin, Ampicillin-sulbactam, Ampicillin, Gentamicin, Nalidixic acid, Cefotaxime, Nitrofurantoin, Oxacillin, Sulphamethoxazole, Cephalothin, Erythromycin, Tetracycline, Minocycline, vancomycin, Rifamycin. | Ciprofloxacin, Trimethoprim, Chloramphenicol, Penicillins, Clindamycin, Ampicillin-sulbactam, Oxacillin, Ampicillin, Gentamicin, Nalidixic acid, Cefotaxime, Nitrofurantoin, Sulphamethoxazole, Cephalothin, Erythromycin, Tetracycline, Minocycline, vancomycin, Rifamycin. | blaP1class A β-lactamase (pse1-PSE-1/CARB-2), blaTEM, TetC, Class 1 integron, Class 2 integron | DD/PCR | [56] |
| Listeria spp. | n = 24: Penicillin, Cephalothin, Gentamicin, Kanamycin, Amikacin, Ertapenem, Meropenem, Cefotaxime, Ceftriaxone, Vancomycin, Clindamycin, Erythromycin, Nitrofurantoin, Ampicillin, Colistin, Nalidixic acid, Mixofloxacin, Fusidic Acid Ciprofloxacin, Trimethoprim, Tetracycline, Streptomycin, Fosfomycin Chloramphenicol. | Penicillin, Cephalothin, Kanamycin, Ertapenem, Cefotaxime, Ceftriaxone, Vancomycin, Clindamycin, Erythromycin, Nitrofurantoin, Ampicillin, Colistin, Nalidixic acid, Mixofloxacin, Trimethoprim, Tetracycline, | DD | [57] | |
| Aeromonas spp. | Penicillin, Cephalothin, Kanamycin, Ertapenem, Meropenem, Cefotaxime, Ceftriaxone, Vancomycin, Clindamycin, Erythromycin, Nitrofurantoin, Ampicillin, Colistin, Nalidixic acid, Mixofloxacin, Trimethoprim, Tetracycline, Streptomycin, Chloramphenicol, Fosfomycin, Fusidic Acid. | ||||
| E. coli | n = 13: Ampicillin, amoxicillin, cephalothin, cefazolin, ceftazidime, tetracycline, doxycycline, chloramphenicol, amikacin, gentamicin, nalidixicacid, norfloxacin, fosfomycin. | Ampicillin, amoxicillin, cephalothin, ceftazidime, tetracycline, doxycycline, chloramphenicol, nalidixic acid, norfloxacin, fosfomycin. | DD | [62] | |
| Klebsiella Bacillus Pseudomonas Aeromonas Exiguobacterium Shewanella spp. | n = 6: Vancomycin, kanamycin, trimethoprim, oxytetracycline, amoxicillin and chloramphenicol. | Vancomycin, kanamycin, trimethoprim, oxytetracycline, amoxicillin and chloramphenicol. | BD | [55] | |
| Enterococcus spp. | n = 1: Vancomycin | erm(B) was, VREfm, vanA (vanA, vanHA, vanRA, vanSA, vanYA and vanZA gene clusters), vanG (vanRG), vanN (vanRN) and vanL (vanSL), vanC (vanC1XY, vanSC, vanRC and vanXYC), isa(A), et(M), aac(6′)-Ii | WGS | [72] | |
| Enterobacteriaceae | n = 18: Doxycycline, tetracycline, ampicillin, gentamicin, meropenem amoxicillin/clavulanic acid, amikacin, nitrofurantoin, cefuroxime, cefotaxime, norfloxacin, ciprofloxacin, chloramphenicol, nalidixic acid, colistin sulphate, polymyxin, trimethoprim-sulfamethoxazole, imipenem. | Gentamycin, neomycin, penicillin G, nitrofurantoin, polymyxin B, cefuroxime. | ESBL (blaCTX-M, blaTEM, blaSHV, blaGES, blaIMP, blaKPC, blaVIM, blaOXA-1-like,blaPER, blaOXA-48-like, and blaVEB), pAmpC (blaACC, blaEBC, blaFOX,blaCIT, blaDHA, and blaMOX), non-β-lactam (aadA, catI,catII, strA, sulI, sulII, tetA, tetB, tetC, tetD, tetK, and tetM) | DD/PCR | [69] |
| E. coli | n = 18: Ampicillin, amikacin, imipenem, meropenem, streptomycin, ciprofloxacin, chloramphenicol, nalidixic, tetracycline, trimethoprim, norfloxacin, Sulfamethoxazole, gentamycin, neomycin, penicillin G, nitrofurantoin, polymyxin B, cefuroxime. | blaTEM, blaSHV, blaZ, blaCTX-M, aadA, strA, tetA, tetB, tetK and tetM, | DD/PCR | [63] | |
| Vibrio spp. | Ampicillin, amikacin, imipenem, meropenem, streptomycin, chloramphenicol, ciprofloxacin, nalidixic, tetracycline, trimethoprim, norfloxacin, Sulfamethoxazole, gentamycin, neomycin, penicillin G, nitrofurantoin, polymyxin B, cefuroxime. | ||||
| Enterococcus spp. | n = 14: Chloramphenicol, tetracycline, ampicillin, nitrofurantoin, ciprofloxacin, levofloxacin, imipenem, linezolid, erythromycin, quinupristin-dalfopristin, tigecycline, trimethoprim-sulfamethoxazole, vancomycin, teicoplanin. | lsa(A), msr(C), msr(D), erm(B), and mef(A), tet(S), tet(M), and tet(L), aac(60)-aph(200), ant(6)-Ia, aph(30)-III, aac(60)-Iid, aac(60)-Iih, dfrG | DD/WGS | [37] | |
| E. coli | n = 17: Ampicillin, amikacin, imipenem, meropenem, streptomycin, cefotaxime, chloramphenicol, cephalexin, ciprofloxacin, nalidixic acid, tetracycline, norfloxacin, gentamicin, cefuroxime, polymyxin B, colistin sulfate, and nitrofurantoin. | Ampicillin, amikacin, streptomycin, chloramphenicol, ciprofloxacin, cephalexin, nalidixic acid, tetracycline, norfloxacin, gentamicin, cefuroxime, cefotaxime, polymyxin B, colistin sulfate, and nitrofurantoin. | strA, aadA, cat I, cat II, cmlA1, ampC, blaZ, blaTEM, tetA, tetB, tetC, tetD, tetK, tetM | DD/PCR | [64] |
| Aeromonas spp. | n = 12: Ampicillin, ceftazidime, cefixime, polymyxin B, colistin, ciprofloxacin, levofloxacin, ofloxacin, minocycline, meropenem, imipenem, trimethoprim-sulphamethoxazole. | Ampicillin, ceftazidime, cefixime, polymyxin B, colistin, ciprofloxacin, levofloxacin, minocycline, meropenem, imipenem, trimethoprim-sulphamethoxazole. | blaTEM, blaAmpC, AmpC/blaOXA, mcr-1, | DD/PCR | [58] |
| Pseudomonas spp. | Ampicillin, ceftazidime, cefixime, polymyxin B, colistin, ciprofloxacin, levofloxacin, ofloxacin, minocycline, meropenem, imipenem, trimethoprim-sulphamethoxazole. | ||||
| Enterococci | ermA,ermB and ermC, tetK, tetM and tetL, vanA, vanB and vanC, aph(3‘)-IIIa, ant(4‘)-Ia,aac(6′)-Ie-aph(2”)-Ia | PCR | [71] | ||
| Vibrio spp. | n = 13: Imipenem, nalidixic acid, erythromycin, gentamicin, Sulfamethoxazole, cefuroxime, penicillin G, chloramphenicol, polymixin B, trimethoprim-sulfamethoxazole, tetracycline, meropenem and trimethoprim. | Nalidixic acid, erythromycin, Sulfamethoxazole, cefuroxime, penicillin G, chloramphenicol, polymixin B, trimethoprim-sulfamethoxazole, tetracycline and trimethoprim. | DD | [78] | |
| Salmonella spp. | n = 20: Cephalothin, Imipenem, Cefoxitin, Cefuroxime, Piperacillin, Ampicillin, Cefixime, Ceftazidime, Aztreonam, Gentamycin, Amikacin, Streptomycin, Chloramphenicol, Tetracycline, Ciprofloxacin, Norfloxacin, Nalidixic acid, Nitrofurantoin, Sulfamethoxazole Trimethoprim/Sulfamethoxazole. | Imipenem, Piperacillin, Ampicillin, Cefixime, Ceftazidime, Streptomycin, Nalidixic acid, Sulfamethoxazole. | DD | [76] | |
| Pseudomonas spp. | n = 19: Ampicillin, cefotaxime, cephalothin, cefepime, chloramphenicol, clindamycin, erythromycin, gentamicin, minocycline, nalidixic acid, nitrofurantoin, ofloxacin, oxacillin, penicillin G, rifampin, sulphamethoxazole, tetracycline, vancomycin, ampicillin-sulbactam. | Ampicillin, cefotaxime, cephalothin, cefepime, chloramphenicol, clindamycin, minocycline, nalidixic acid, nitrofurantoin, oxacillin, penicillin G, rifampin, sulphamethoxazole, tetracycline, vancomycin, ampicillin-sulbactam. | DD | [75] | |
| Enterococcus spp. | n = 11: Ampicillin, amoxicillin, penicillin, neomycin, streptomycin, vancomycin, chloramphenicol, ciprofloxacin, tetracycline, trimethoprim, erythromycin. | Ampicillin, amoxicillin, penicillin, neomycin, streptomycin, vancomycin, chloramphenicol, ciprofloxacin, tetracycline, trimethoprim, erythromycin. | DD | [70] | |
| E. coli | n = 9: Ampicillin, penicillin, ciprofloxacin, tetracycline, trimethoprim, cefotaxime, ceftazidime, imipenem and meropenem. | Ampicillin, penicillin, ciprofloxacin, tetracycline, trimethoprim, cefotaxime, ceftazidime. | Alr, blaTEM, blaSHV and blaCTX-M | DD/PCR | [65] |
| Bacillus, Pseudomonas, Enterococcus, Brevibacillus, Paenibacillus | n = 3 Penicillin G, vancomycin, erythromycin. | Vancomycin Erythromycin Penicillin G | DD | [51] | |
| E. coli | n = 12: Amoxicillin, Cefuroxime, Gentamicin, Doxycycline, Ciprofloxacin, Ofloxacin, Trimithoprime, Menopenem, Colistin sulphate, Erythromycin, Clindamycin, Sulphamethoxazole. | Amoxicillin, Cefuroxime, Gentamicin, Doxycycline, Ciprofloxacin, Ofloxacin, Trimithoprime, Menopenem, Colistin sulphate, Erythromycin, Clindamycin, Sulphamethoxazole. | DD | [67] | |
| Pseudomonas spp. | n = 20: Penicillins, clinamycins, ciprofloxacin, rafamycin, trimethoprim, sulphamethoxazole, gentamicin, chloramphenicol, tetracycline, erythromycin, minocycline, vacomycin, cefotaxime, nalidixic acid, nitrofurantoin, cephalothin, ofloxacin, ampicillin, ampicillin-sulbactam, oxacillin. | Penicillins, clinamycins, rafamycin, trimethoprim, sulphamethoxazole, chloramphenicol, tetracycline, minocycline, vacomycin, cefotaxime, nalidixic acid, nitrofurantoin, cephalothin, ampicillin, ampicillin-sulbactam, oxacillin. | blaTEM, blaOXA, blaAmpC, TetC, | DD/PCR | [89] |
| Escherichia coli Enterococcus spp. | n = 22: Amikacin, ampicillin, azithromycin, amoxicillin-clavulanic acid, cefepime, cefotaxime, cefoxitin, ceftazidime, ceftriaxone, cephalexin, ciprofloxacin, chloramphenicol, gentamicin, imipenem, meropenem, nalidixic acid, piperacillin-tazobactam, tetracycline, tigecycline, trimethoprim-sulfamethoxazole. | [68] | |||
| n = 16: Imipenem, Ampicillin, tetracycline, Nitrofurantoin, quinupristin-dalfopristin, tigecycline, Linezolid, ciprofloxacin, trimethoprim-sulfamethoxazole, Levofloxacin, Teicoplanin, vancomycin, Gentamycin, Streptomycin, Erythromycin, chloramphenicol. |
| SN | Report Number | Project Title | Year | Aim | WWTP | AST |
|---|---|---|---|---|---|---|
| 1 | 1126/1/05 | Enteric pathogens in water sources and stools of residents in the Venda region of the Limpopo Province | 2005 | Identify and characterise enteric pathogens in water sources and stool samples of residents in the Venda region of the Limpopo Province | No | Yes |
| 2 | 1967/1/13 | Investigations into the existence of unique environmental Escherichia coli populations | 2013 | Identify and characterise E. coli from chosen localities and different samples | No | No |
| 3 | 2138/1/16 | An investigation into the presence of free-living amoebae and amoeba-resistant bacteria in drinking water distribution systems of health care institutions in Johannesburg, South Africa | 2016 | To establish the occurrence of free-living amoebae and amoeba resistant bacteria within the drinking water distribution system in health care facilities in Johannesburg and also highlight the potential human health risk implication thereof | Yes | No |
| 4 | 2432/1/18 | Cholera Monitoring and Response Guidelines | 2018 | The development of cholera monitoring and response guidelines for inclusion in the water resource monitoring programme. | Yes | Yes |
| 5 | 2585/1/19 | Antibiotic-resistant bacteria and genes in drinking water. Implications for drinking water production and quality monitoring | 2019 | Identify and characterise microbial parameters in drinking water systems | No | Yes |
| 6 | 2610/1/18 | Microplastics in freshwater water environments | 2018 | Identify and characterise microplastics in freshwater, drinking water and groundwater | No | No |
| 7 | 2706/1/21 | Measurement of water pollution determining the sources and changes of microbial contamination and impact on food safety from farming to retail level for fresh vegetables | 2021 | To determine the link between water pollution and crop contamination and to determine sources of microbial product contamination, and assess the impact on food safety from farming to retail for selected fresh vegetable supply chains | No | Yes |
| 8 | 2733/1/20 | Substances of emerging concern in South African aquatic ecosystems | 2020 | Identify and evaluate different contaminants of emerging concern in different water sources | Yes | No |
| 9 | 1655/1/10 | Identification of Arsenic Resistance Genes in Micro-organisms from Maturing Fly Ash-Acid Mine Drainage Neutralised Solids | 2011 | To isolate micro-organisms resistant to arsenic from matured AMD-FA neutralized solids, to characterize their arsenic resistance systems and to assess whether these organisms pose a potential ‘threat’ to the sustained use of ‘Neutralization Solids’ | No | No |
| 10 | KV 360/16 | A Scoping Study on the Levels of Antimicrobials and Presence of Antibiotic-Resistant Bacteria in Drinking Water | 2016 | To provide an overview of the levels of antimicrobials and the presence of antibiotic-resistant bacteria in selected drinking water treatment systems (drinking water production facilities) | No | Yes |
| 11 | TT 742/1/17 | Emerging contaminants in wastewater treated for direct potable reuse: the human health risk priorities in South Africa | 2018 | Identify and evaluate different contaminants of emerging concern in different water sources | Yes | No |
| 12 | The epidemiology and cost of treating diarrhoea in South Africa | Identify and characterise enteric pathogens in water sources and stool samples of residents in the Venda region of the Limpopo Province | No | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abia, A.L.K.; Baloyi, T.; Traore, A.N.; Potgieter, N. The African Wastewater Resistome: Identifying Knowledge Gaps to Inform Future Research Directions. Antibiotics 2023, 12, 805. https://doi.org/10.3390/antibiotics12050805
Abia ALK, Baloyi T, Traore AN, Potgieter N. The African Wastewater Resistome: Identifying Knowledge Gaps to Inform Future Research Directions. Antibiotics. 2023; 12(5):805. https://doi.org/10.3390/antibiotics12050805
Chicago/Turabian StyleAbia, Akebe Luther King, Themba Baloyi, Afsatou N. Traore, and Natasha Potgieter. 2023. "The African Wastewater Resistome: Identifying Knowledge Gaps to Inform Future Research Directions" Antibiotics 12, no. 5: 805. https://doi.org/10.3390/antibiotics12050805
APA StyleAbia, A. L. K., Baloyi, T., Traore, A. N., & Potgieter, N. (2023). The African Wastewater Resistome: Identifying Knowledge Gaps to Inform Future Research Directions. Antibiotics, 12(5), 805. https://doi.org/10.3390/antibiotics12050805