
A Systematic Review on Antimicrobial Pharmacokinetic Differences between Asian and Non-Asian Adult Populations

Abstract
1. Introduction
2. Results
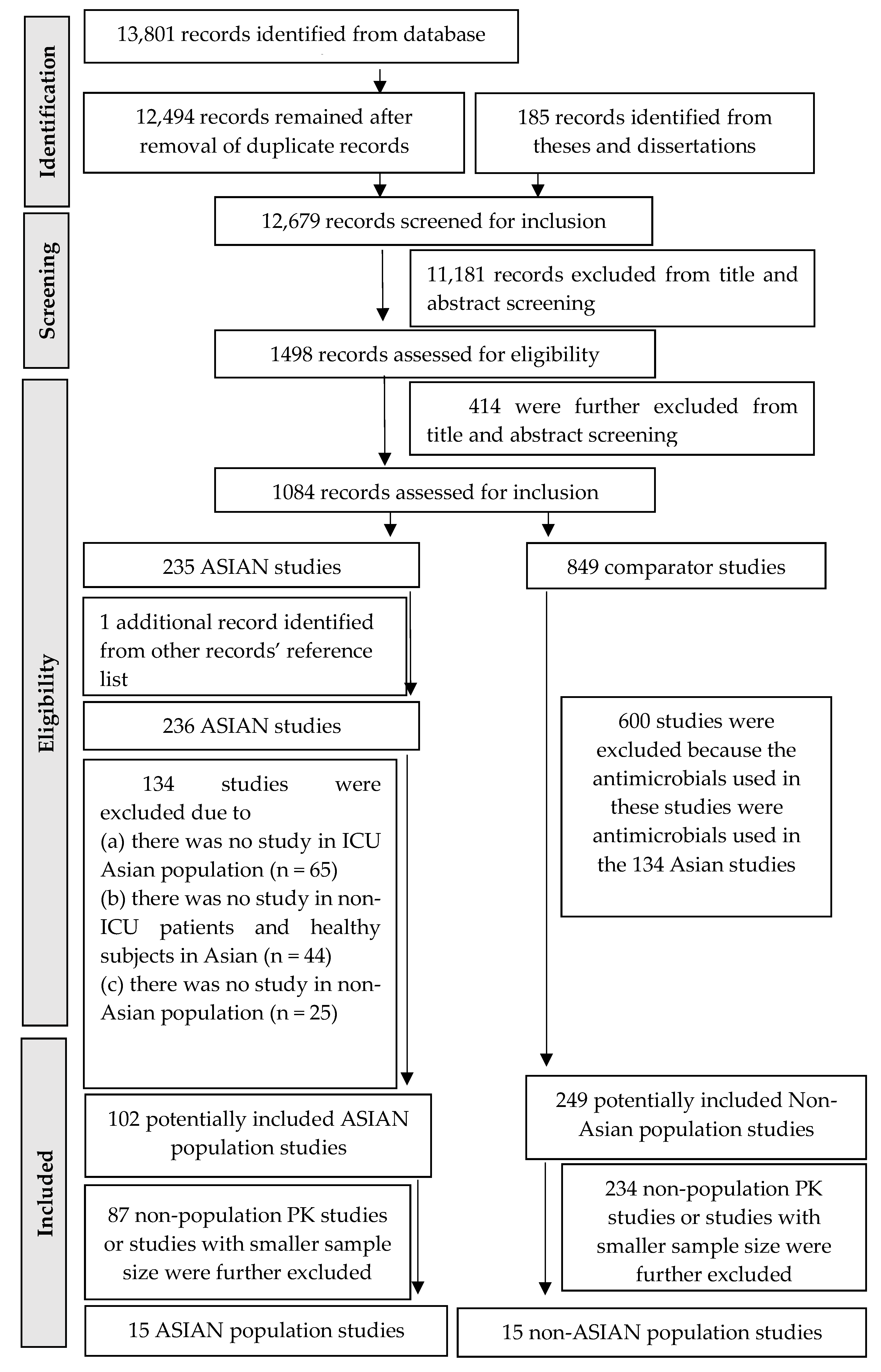
2.1. Study Selection
2.2. Pharmacokinetic Differences between Asian and Non-Asian Population Groups
2.2.1. Carbapenems
Meropenem
Imipenem
Doripenem
2.2.2. Oxazolidinones
Linezolid
2.2.3. Glycopeptide
Vancomycin
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Study Selection
4.3. Data Extraction and Quality Assessment of Pharmacokinetic Studies
4.4. Pharmacokinetic Comparison Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CL | clearance |
| CLCr | creatinine clearance |
| CLnon-ren | non-renal clearance |
| CLren | clearance renal |
| Cmax | maximum concentration in a dosing interval |
| Cmax,ss | maximum concentration at pharmacokinetic steady state |
| Cmin | minimum concentration in a dosing interval |
| CYP450 | cytochrome P450 |
| ECMO | extracorporeal membrane oxygenation |
| ICU | intensive care unit |
| IIV | interindividual variability |
| IV | intravenous |
| KCP | the rate constant from the central compartment to the peripheral compartment |
| Ke | elimination rate constant |
| KPC | the rate constant from the peripheral compartment to the central compartment |
| L | litre |
| L/h | litre per hour |
| L/kg | litre per kilogram body weight |
| L/h/kg | litre per hour per kilogram body weight |
| MIC | minimum inhibitory concentration |
| PK/PD | pharmacokinetic/pharmacodynamic |
| PK | pharmacokinetic |
| Q | intercompartmental clearance |
| RRT | renal replacement therapy |
| SeCr | serum creatinine |
| t1/2 | half-life |
| TDM | therapeutic drug monitoring |
| Vc | volume of distribution in central compartment |
| Vd | volume of distribution |
| Vdss | volume of distribution at steady state |
| Vd-tot | volume of distribution total |
| Vp | volume of distribution in peripheral compartment |
References
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U.; et al. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645–1658. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Lepore, C.; Silver, L.; Theuretzbacher, U.; Thomas, J.; Visi, D. The Small-Molecule Antibiotics Pipeline: 2014–2018. Nat. Rev. Drug Discov. 2019, 18, 739. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Dynamics, Economics & Policy. Access Barriers to Antibiotics; Center for Disease Dynamics, Economics & Policy: Washington, DC, USA, 2019. [Google Scholar]
- Tam, V.H.; Chang, K.T.; Zhou, J.; Ledesma, K.R.; Phe, K.; Gao, S.; Van Bambeke, F.; Sánchez-Díaz, A.M.; Zamorano, L.; Oliver, A.; et al. Determining β-lactam exposure threshold to suppress resistance development in Gram-negative bacteria. J. Antimicrob. Chemother. 2017, 72, 1421–1428. [Google Scholar] [CrossRef]
- Bowker, K.E.; Noel, A.R.; Tomaselli, S.G.; Elliott, H.; MacGowan, A.P. Pharmacodynamics of the antibacterial effect and emergence of resistance to doripenem in Pseudomonas aeruginosa and Acinetobacter baumannii in an in vitro pharmacodynamic model. Antimicrob. Agents Chemother. 2012, 56, 5009–5015. [Google Scholar] [CrossRef]
- MacVane, S.H.; Kuti, J.L.; Nicolau, D.P. Clinical pharmacodynamics of antipseudomonal cephalosporins in patients with ventilator-associated pneumonia. Antimicrob. Agents Chemother. 2014, 58, 1359–1364. [Google Scholar] [CrossRef] [PubMed]
- Muller, A.E.; Punt, N.; Mouton, J.W. Exposure to ceftobiprole is associated with microbiological eradication and clinical cure in patients with nosocomial pneumonia. Antimicrob. Agents Chemother. 2014, 58, 2512–2519. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [PubMed]
- Slaviero, K.A.; Clarke, S.J.; Rivory, L.P. Inflammatory response: An unrecognised source of variability in the pharmacokinetics and pharmacodynamics of cancer chemotherapy. Lancet Oncol. 2003, 4, 224–232. [Google Scholar] [CrossRef] [PubMed]
- Hochepied, T.; Berger, F.G.; Baumann, H.; Libert, C. Alpha(1)-acid glycoprotein: An acute phase protein with inflammatory and immunomodulating properties. Cytokine Growth Factor Rev. 2003, 14, 25–34. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Roberts, J.A.; Lipman, J.; Rello, J. Antibiotic dosing in multiple organ dysfunction syndrome. Chest 2011, 139, 1210–1220. [Google Scholar] [CrossRef]
- Udy, A.A.; Baptista, J.P.; Lim, N.L.; Joynt, G.M.; Jarrett, P.; Wockner, L.; Boots, R.J.; Lipman, J. Augmented renal clearance in the ICU: Results of a multicenter observational study of renal function in critically ill patients with normal plasma creatinine concentrations. Crit. Care Med. 2014, 42, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Inoue, S.; Howgate, E.M.; Rowland-Yeo, K.; Shimada, T.; Yamazaki, H.; Tucker, G.T.; Rostami-Hodjegan, A. Prediction of in vivo drug clearance from in vitro data. II: Potential inter-ethnic differences. Xenobiotica 2006, 36, 499–513. [Google Scholar] [CrossRef] [PubMed]
- Bart, G.; Lenz, S.; Straka, R.J.; Brundage, R.C. Ethnic and genetic factors in methadone pharmacokinetics: A population pharmacokinetic study. Drug Alcohol Depend. 2014, 145, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Ngaimisi, E.; Habtewold, A.; Minzi, O.; Makonnen, E.; Mugusi, S.; Amogne, W.; Yimer, G.; Riedel, K.D.; Janabi, M.; Aderaye, G.; et al. Importance of ethnicity, CYP2B6 and ABCB1 genotype for efavirenz pharmaco-kinetics and treatment outcomes: A parallel-group prospective cohort study in two sub-saharan Africa populations. PLoS ONE 2013, 8, e67946. [Google Scholar] [CrossRef] [PubMed]
- Andrews, L.M.; De Winter, B.C.; Van Gelder, T.; Hesselink, D.A. Consideration of the ethnic prevalence of genotypes in the clinical use of tacrolimus. Pharmacogenomics 2016, 17, 1737–1740. [Google Scholar] [CrossRef] [PubMed]
- Ye, C.; Jin, H.; Zhang, R.; Sun, Y.; Wang, Z.; Sun, W.; Sun, W.; Peng, Q.; Liu, R.; Huang, Y. Variability of warfarin dose response associated with CYP2C9 and VKORC1 gene polymorphisms in Chinese patients. J. Int. Med. Res. 2014, 42, 67–76. [Google Scholar] [CrossRef]
- Ahsan, C.H.; Renwick, A.G.; Macklin, B.; Challenor, V.F.; Waller, D.G.; George, C.F. Ethnic differences in the pharmacokinetics of oral nifedipine. Br. J. Clin. Pharmacol. 1991, 31, 399–403. [Google Scholar] [CrossRef]
- Guo, T.; Mao, G.F.; Xia, D.Y.; Su, X.Y.; Zhao, L.S. Pharmacokinetics of midazolam tablet in different Chinese ethnic groups. J. Clin. Pharm. Ther. 2011, 36, 406–411. [Google Scholar] [CrossRef]
- Tornatore, K.M.; Meaney, C.J.; Wilding, G.E.; Chang, S.S.; Gundroo, A.; Cooper, L.M.; Gray, V.; Shin, K.; Fetterly, G.J.; Prey, J.; et al. Influence of sex and race on mycophenolic acid pharmacokinetics in stable African American and Caucasian renal transplant recipients. Clin. Pharmacokinet. 2015, 54, 423–434. [Google Scholar] [CrossRef]
- Staiano, A.E.; Broyles, S.T.; Gupta, A.K.; Katzmarzyk, P.T. Ethnic and sex differences in visceral, subcutaneous, and total body fat in children and adolescents. Obesity 2013, 21, 1251–1255. [Google Scholar] [CrossRef]
- Liu, A.; Byrne, N.M.; Kagawa, M.; Ma, G.; Kijboonchoo, K.; Nasreddine, L.; Koon Poh, B.; Ismail, M.N.; Hills, A.P. Ethnic differences in body fat distribution among Asian pre-pubertal children: A cross-sectional multicentre study. BMC Public Health 2011, 11, 500. [Google Scholar] [CrossRef] [PubMed]
- Deurenberg, P.; Tagliabue, A.; Wang, J.; Wolde-Gebriel, Z. Multi-frequency bioelectrical impedence for the prediction of body water compartments: Validation in different ethnic groups. Asia Pac. J. Clin. Nutr. 1996, 5, 217–221. [Google Scholar] [PubMed]
- Johnson, J.A.; Livingston, T.N. Differences between blacks and whites in plasma protein binding of drugs. Eur. J. Clin. Pharmacol. 1997, 51, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.; Wang, J.; Pierson, R.N., Jr.; Wang, Z.M.; Heymsfield, S.B.; Sardinha, L.B.; Heshka, S. Extracellular water: Greater expansion with age in African Americans. J. Appl. Physiol. 2005, 99, 261–267. [Google Scholar] [CrossRef]
- Kitada, M. Genetic polymorphism of cytochrome P450 enzymes in Asian populations: Focus on CYP2D6. Int. J. Clin. Pharmacol. Res. 2003, 23, 31–35. [Google Scholar]
- Daniel, L.H. Polymorphisms of cytochrome P450 are potential candidates that could potentially help clinicians on the treatment of cardiovascular diseases among Asian populations. Indian Heart J. 2017, 69, 655–656. [Google Scholar] [CrossRef]
- Cropp, C.D.; Yee, S.W.; Giacomini, K.M. Genetic variation in drug transporters in ethnic populations. Clin. Pharmacol. Ther. 2008, 84, 412–416. [Google Scholar] [CrossRef]
- Tanaka, Y.; Manabe, A.; Fukushima, H.; Suzuki, H.; Nakadate, H.; Kondoh, K.; Nakamura, K.; Koh, K.; Fukushima, T.; Tsuchida, M.; et al. Multidrug resistance protein 4 (MRP4) polymorphisms impact the 6-mercaptopurine dose tolerance during maintenance therapy in Japanese childhood acute lymphoblastic leukemia. Pharm. J. 2015, 15, 380–384. [Google Scholar] [CrossRef]
- Abla, N.; Chinn, L.W.; Nakamura, T.; Liu, L.; Huang, C.C.; Johns, S.J.; Kawamoto, M.; Stryke, D.; Taylor, T.R.; Ferrin, T.E.; et al. The human multidrug resistance protein (MRP4, ABCC4): Functional analysis of a highly polymorphic gene. J. Pharmacol. Exp. Ther. 2008, 325, 859–868. [Google Scholar] [CrossRef]
- Tsai, D.; Jamal, J.A.; Davis, J.S.; Lipman, J.; Roberts, J.A. Interethnic differences in pharmacokinetics of antibacterials. Clin. Pharmacokinet. 2015, 54, 243–260. [Google Scholar] [CrossRef]
- Walton, J.; Harris, A.; Iwabuchi, K. Introduction: Everyday multiculturalism in/across Asia. Ethn. Racial Stud. 2020, 43, 807–815. [Google Scholar] [CrossRef]
- Ishihara, N.; Nishimura, N.; Ikawa, K.; Karino, F.; Miura, K.; Tamaki, H.; Yano, T.; Isobe, T.; Morikawa, N.; Naora, K. Population pharmacokinetic modeling and pharmacodynamic target attainment simulation of piperacillin/tazobactam for dosing optimization in late elderly patients with pneumonia. Antibiotics 2020, 9, 113. [Google Scholar] [CrossRef] [PubMed]
- Cao, G.; Zhang, J.; Wu, X.; Yu, J.; Chen, Y.; Ye, X.; Zhu, D.; Zhang, Y.; Guo, B.; Shi, Y. Pharmacokinetics and pharmacodynamics of levofloxacin injection in healthy Chinese volunteers and dosing regimen optimization. J. Clin. Pharm. Ther. 2013, 38, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Ikawa, K.; Nomura, K.; Morikawa, N.; Ikeda, K.; Ohge, H.; Sueda, T.; Taniwaki, M. Pharmacokinetic-pharmacodynamic target attainment analysis of cefozopran in Japanese adult patients. J. Infect. Chemother. 2008, 14, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Zhou, Y.; Khan, M.S.; Sy, R.N.; Khosa, F. Representation of sex, race, and ethnicity in pivotal clinical trials for dermatological drugs. Int. J. Womens Dermatol. 2021, 7, 428–434. [Google Scholar] [CrossRef]
- Cwalina, T.B.; Jella, T.K.; Manyak, G.A.; Kuo, A.; Kamath, A.F. Is our science representative? A systematic review of racial and ethnic diversity in orthopaedic clinical trials from 2000 to 2020. Clin. Orthop. Relat. Res. 2022, 480, 848–858. [Google Scholar] [CrossRef]
- Jaruratanasirikul, S.; Sriwiriyajan, S. Comparison of the pharmacodynamics of meropenem in healthy volunteers following administration by intermittent infusion or bolus injection. J. Antimicrob. Chemother. 2003, 52, 518–521. [Google Scholar] [CrossRef]
- Krueger, W.A.; Bulitta, J.; Kinzig-Schippers, M.; Landersdorfer, C.; Holzgrabe, U.; Naber, K.G.; Drusano, G.L.; Sörgel, F. Evaluation by monte carlo simulation of the pharmacokinetics of two doses of meropenem administered intermittently or as a continuous infusion in healthy volunteers. Antimicrob. Agents Chemother. 2005, 49, 1881–1889. [Google Scholar] [CrossRef]
- Muro, T.; Sasaki, T.; Hosaka, N.; Umeda, Y.; Takemoto, S.; Yamamoto, H.; Kamimura, H.; Higuchi, S.; Karube, Y. Population pharmacokinetic analysis of meropenem in Japanese adult patients. J. Clin. Pharm. Ther. 2011, 36, 230–236. [Google Scholar] [CrossRef]
- Li, C.; Kuti, J.L.; Nightingale, C.H.; Nicolau, D.P. Population pharmacokinetic analysis and dosing regimen optimization of meropenem in adult patients. J. Clin. Pharmacol. 2006, 46, 1171–1178. [Google Scholar] [CrossRef]
- Mathew, S.K.; Mathew, B.S.; Neely, M.N.; Naik, G.S.; Prabha, R.; Jacob, G.G.; Fleming, D.H. A nonparametric pharmacokinetic approach to determine the optimal dosing regimen for 30-minute and 3-hour meropenem infusions in critically ill patients. Ther. Drug Monit. 2016, 38, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Idoate Grijalba, A.I.; Aldaz Pastor, A.; Marquet, P.; Woillard, J.B. Evaluation of a non-parametric modelling for meropenem in critically ill patients using Monte Carlo simulation. Eur. J. Clin. Pharmacol. 2019, 75, 1405–1414. [Google Scholar] [CrossRef]
- Jaruratanasirikul, S.; Raungsri, N.; Punyo, J.; Sriwiriyajan, S. Pharmacokinetics of imipenem in healthy volunteers following administration by 2 h or 0.5 h infusion. J. Antimicrob. Chemother. 2005, 56, 1163–1165. [Google Scholar] [CrossRef] [PubMed]
- Norrby, S.R.; Björnegård, B.; Ferber, F.; Jones, K.H. Pharmacokinetics of imipenem in healthy volunteers. J. Antimicrob. Chemother. 1983, 12 (Suppl. D), 109–124. [Google Scholar] [CrossRef] [PubMed]
- Yoshizawa, K.; Ikawa, K.; Ikeda, K.; Kumon, H.; Ohge, H.; Morikawa, N. Optimisation of imipenem regimens in patients with impaired renal function by pharmacokinetic-pharmacodynamic target attainment analysis of plasma and urinary concentration data. Int. J. Antimicrob. Agents 2012, 40, 427–433. [Google Scholar] [CrossRef]
- Finch, R.G.; Craddock, C.; Kelly, J.; Deaney, N.B. Pharmacokinetic studies of imipenem/cilastatin in elderly patients. J. Antimicrob. Chemother. 1986, 18 (Suppl. E), 103–107. [Google Scholar] [CrossRef]
- Abhilash, B.; Tripathi, C.D.; Gogia, A.R.; Meshram, G.G.; Kumar, M.; Suraj, B. Pharmaco-kinetic/pharmacodynamic profiling of imipenem in patients admitted to an intensive care unit in India: A nonrandomized, cross-sectional, analytical, open-labeled study. Indian J. Crit. Care Med. 2015, 19, 587–592. [Google Scholar] [CrossRef]
- Couffignal, C.; Pajot, O.; Laouénan, C.; Burdet, C.; Foucrier, A.; Wolff, M.; Armand-Lefevre, L.; Mentré, F.; Massias, L. Population pharmacokinetics of imipenem in critically ill patients with suspected ventilator-associated pneumonia and evaluation of dosage regimens. Br. J. Clin. Pharmacol. 2014, 78, 1022–1034. [Google Scholar] [CrossRef]
- Kim, S.W.; Choe, S.; Kim, D.J.; Zang, D.Y.; Lee, D.H. Pharmacokinetics of doripenem in healthy Koreans and Monte Carlo simulations to explore optimal dosage regimens in patients with normal and enhanced renal function. Ther. Drug Monit. 2018, 40, 425–434. [Google Scholar] [CrossRef]
- Bhavnani, S.M.; Hammel, J.P.; Cirincione, B.B.; Wikler, M.A.; Ambrose, P.G. Use of pharmacokinetic-pharmacodynamic target attainment analyses to support phase 2 and 3 dosing strategies for doripenem. Antimicrob. Agents Chemother. 2005, 49, 3944–3947. [Google Scholar] [CrossRef]
- Lee, D.H.; Kim, Y.K.; Jin, K.; Kang, M.J.; Joo, Y.D.; Kim, Y.W.; Moon, Y.S.; Shin, J.G.; Kiem, S. Population pharmacokinetic analysis of doripenem after intravenous infusion in Korean patients with acute infections. Antimicrob. Agents Chemother. 2017, 61, e02185–e021816. [Google Scholar] [CrossRef] [PubMed]
- Bhalodi, A.A.; Keel, R.A.; Quintiliani, R.; Lodise, T.P.; Nicolau, D.P.; Kuti, J.L. Pharmacokinetics of doripenem in infected patients treated within and outside the intensive care unit. Ann. Pharmacother. 2013, 47, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Aziz, M.H.; Abd Rahman, A.N.; Mat-Nor, M.B.; Sulaiman, H.; Wallis, S.C.; Lipman, J.; Roberts, J.A.; Staatz, C.E. Population pharmacokinetics of doripenem in critically ill patients with sepsis in a Malaysian intensive care unit. Antimicrob. Agents Chemother. 2015, 60, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Lipman, J. Optimal doripenem dosing simulations in critically ill nosocomial pneumonia patients with obesity, augmented renal clearance, and decreased bacterial susceptibility. Crit. Care Med. 2013, 41, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zhang, J.; Chen, Y.; Liang, X.; Guo, Y.; Yu, J.; Zhu, D.; Zhang, Y. Optimization of linezolid treatment regimens for Gram-positive bacterial infections based on pharmacokinetic/pharmacodynamic analysis. Future Microbiol. 2017, 12, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Stalker, D.J.; Jungbluth, G.L.; Hopkins, N.K.; Batts, D.H. Pharmacokinetics and tolerance of single- and multiple-dose oral or intravenous linezolid, an oxazolidinone antibiotic, in healthy volunteers. J. Antimicrob. Chemother. 2003, 51, 1239–1246. [Google Scholar] [CrossRef]
- Sasaki, T.; Takane, H.; Ogawa, K.; Isagawa, S.; Hirota, T.; Higuchi, S.; Horii, T.; Otsubo, K.; Ieiri, I. Population pharmacokinetic and pharmacodynamic analysis of linezolid and a hematologic side effect, thrombocytopenia, in Japanese patients. Antimicrob. Agents Chemother. 2011, 55, 1867–1873. [Google Scholar] [CrossRef]
- Crass, R.L.; Cojutti, P.G.; Pai, M.P.; Pea, F. Reappraisal of linezolid dosing in renal impairment to improve safety. Antimicrob. Agents Chemother. 2019, 63, e00605–e00619. [Google Scholar] [CrossRef]
- Ide, T.; Takesue, Y.; Ikawa, K.; Morikawa, N.; Ueda, T.; Takahashi, Y.; Nakajima, K.; Takeda, K.; Nishi, S. Population pharmacokinetics/pharmacodynamics of linezolid in sepsis patients with and without continuous renal replacement therapy. Int. J. Antimicrob. Agents 2018, 51, 745–751. [Google Scholar] [CrossRef]
- Taubert, M.; Zoller, M.; Maier, B.; Frechen, S.; Scharf, C.; Holdt, L.M.; Frey, L.; Vogeser, M.; Fuhr, U.; Zander, J. Predictors of inadequate linezolid concentrations after standard dosing in critically ill patients. Antimicrob. Agents Chemother. 2016, 60, 5254–5261. [Google Scholar] [CrossRef]
- Yamamoto, M.; Kuzuya, T.; Baba, H.; Yamada, K.; Nabeshima, T. Population pharmacokinetic analysis of vancomycin in patients with gram-positive infections and the influence of infectious disease type. J. Clin. Pharm. Ther. 2009, 34, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Healy, D.P.; Polk, R.E.; Garson, M.L.; Rock, D.T.; Comstock, T.J. Comparison of steady-state pharmacokinetics of two dosage regimens of vancomycin in normal volunteers. Antimicrob. Agents Chemother. 1987, 31, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Shen, K.; Yang, M.; Fan, Y.; Liang, X.; Chen, Y.; Wu, J.; Yu, J.; Zhang, H.; Wang, R.; Zhang, F.; et al. Model-based evaluation of the clinical and microbiological efficacy of vancomycin: A prospective study of Chinese adult in-house patients. Clin. Infect. Dis. 2018, 67 (Suppl. 2), S256–S262. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, J.L.; Dominguez, A.R.; Lane, J.R.; Anderson, P.O.; Capparelli, E.V.; Cornejo-Bravo, J.M. Population pharmacokinetics of vancomycin in adult and geriatric patients: Comparison of eleven approaches. Int. J. Clin. Pharmacol. Ther. 2010, 48, 525–533. [Google Scholar] [CrossRef]
- Dedkaew, T.; Cressey, T.R.; Punyawudho, B.; Lucksiri, A. Pharmacokinetics of vancomycin in critically ill patients in Thailand. Int. J. Pharm. Pharm. Sci. 2015, 9, 232–237. [Google Scholar]
- Roberts, J.A.; Taccone, F.S.; Udy, A.A.; Vincent, J.L.; Jacobs, F.; Lipman, J. Vancomycin dosing in critically ill patients: Robust methods for improved continuous-infusion regimens. Antimicrob. Agents Chemother. 2011, 55, 2704–2709. [Google Scholar] [CrossRef]
- Mattioli, F.; Fucile, C.; Del Bono, V.; Marini, V.; Parisini, A.; Molin, A.; Zuccoli, M.L.; Milano, G.; Danesi, R.; Marchese, A.; et al. Population pharmacokinetics and probability of target attainment of meropenem in critically ill patients. Eur. J. Clin. Pharmacol. 2016, 72, 839–848. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Roberts, J.A.; Rello, J.; Paterson, D.L.; Lipman, J. The effects of hypoalbuminaemia on optimizing antibacterial dosing in critically ill patients. Clin. Pharmacokinet. 2011, 50, 99–110. [Google Scholar] [CrossRef]
- Craig, W.A. The pharmacology of meropenem, a new carbapenem antibiotic. Clin. Infect. Dis. 1997, 24 (Suppl. 2), S266–S275. [Google Scholar] [CrossRef]
- Zhanel, G.G.; Wiebe, R.; Dilay, L.; Thomson, K.; Rubinstein, E.; Hoban, D.J.; Noreddin, A.M.; Karlowsky, J.A. Comparative review of the carbapenems. Drugs 2007, 67, 1027–1052. [Google Scholar] [CrossRef]
- Finfer, S.; Bellomo, R.; McEvoy, S.; Lo, S.K.; Myburgh, J.; Neal, B.; Norton, R. Effect of baseline serum albumin concentration on outcome of resuscitation with albumin or saline in patients in intensive care units: Analysis of data from the saline versus albumin fluid evaluation (SAFE) study. BMJ 2006, 333, 1044. [Google Scholar] [PubMed]
- Udy, A.A.; Roberts, J.A.; Lipman, J. Clinical implications of antibiotic pharmacokinetic principles in the critically ill. Intensive Care Med. 2013, 39, 2070–2082. [Google Scholar] [CrossRef] [PubMed]
- Pea, F.; Viale, P. Bench-to-bedside review: Appropriate antibiotic therapy in severe sepsis and septic shock—Does the dose matter? Crit. Care 2009, 13, 214. [Google Scholar] [CrossRef] [PubMed]
- Price, D.A.; Fisher, N.D.L.; Osei, S.Y.; Lansang, M.C.; Hollenberg, N.K. Renal perfusion and function in healthy African Americans. Kidney Int. 2001, 59, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; Inker, L.A.; Coresh, J. GFR estimation: From physiology to public health. Am. J. Kidney Dis. 2014, 63, 820–834. [Google Scholar] [CrossRef]
- Hollenberg, N.K.; Rivera, A.; Meinking, T.; Martinez, G.; McCullough, M.; Passan, D.; Preston, M.; Taplin, D.; Vicaria-Clement, M. Age, renal perfusion and function in island-dwelling indigenous Kuna Amerinds of Panama. Nephron 1999, 82, 131–138. [Google Scholar] [CrossRef]
- Hoang, K.; Tan, J.C.; Derby, G.; Blouch, K.L.; Masek, M.; Ma, I.; Lemley, K.V.; Myers, B.D. Determinants of glomerular hypofiltration in aging humans. Kidney Int. 2003, 64, 1417–1424. [Google Scholar] [CrossRef]
- Fuiano, G.; Sund, S.; Mazza, G.; Rosa, M.; Caglioti, A.; Gallo, G.; Natale, G.; Andreucci, M.; Memoli, B.; De Nicola, L.; et al. Renal hemodynamic response to maximal vasodilating stimulus in healthy older subjects. Kidney Int. 2001, 59, 1052–1058. [Google Scholar] [CrossRef]
- Roberts, J.A.; Lipman, J. Pharmacokinetic issues for antibiotics in the critically ill patient. Crit. Care Med. 2009, 37, 840–851. [Google Scholar] [CrossRef]
- Morata, L.; Cuesta, M.; Rojas, J.F.; Rodriguez, S.; Brunet, M.; Casals, G.; Cobos, N.; Hernandez, C.; Martínez, J.A.; Mensa, J.; et al. Risk factors for a low linezolid trough plasma concentration in acute infections. Antimicrob. Agents Chemother. 2013, 57, 1913–1917. [Google Scholar] [CrossRef]
- Pea, F.; Furlanut, M.; Cojutti, P.; Cristini, F.; Zamparini, E.; Franceschi, L.; Viale, P. Therapeutic drug monitoring of linezolid: A retrospective monocentric analysis. Antimicrob. Agents Chemother. 2010, 54, 4605–4610. [Google Scholar] [CrossRef] [PubMed]
- Katip, W.; Jaruratanasirikul, S.; Pattharachayakul, S.; Wongpoowarak, W.; Jitsurong, A.; Lucksiri, A. The pharmacokinetics of vancomycin during the initial loading dose in patients with septic shock. Infect. Drug Resist. 2016, 9, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Duffull, S.B.; Wright, D.F.; Winter, H.R. Interpreting population pharmacokinetic-pharmacodynamic analyses—A clinical viewpoint. Br. J. Clin. Pharmacol. 2011, 71, 807–814. [Google Scholar] [CrossRef]
- Wright, D.F.; Winter, H.R.; Duffull, S.B. Understanding the time course of pharmacological effect: A PKPD approach. Br. J. Clin. Pharmacol. 2011, 71, 815–823. [Google Scholar] [CrossRef]
- Mould, D.R.; Upton, R.N. Basic concepts in population modeling, simulation, and model-based drug development-part 2: Introduction to pharmacokinetic modeling methods. CPT Pharmacomet. Syst. Pharmacol. 2013, 2, e38. [Google Scholar] [CrossRef]
- Kanji, S.; Hayes, M.; Ling, A.; Shamseer, L.; Chant, C.; Edwards, D.J.; Edwards, S.; Ensom, M.H.; Foster, D.R.; Hardy, B.; et al. Reporting guidelines for clinical pharmacokinetic studies: The ClinPK Statement. Clin. Pharmacokinet. 2015, 54, 783–795. [Google Scholar] [CrossRef]
- Luo, D.; Wan, X.; Liu, J.; Tong, T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat. Methods Med. Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Botev, R.; Mallié, J.P.; Couchoud, C.; Schück, O.; Fauvel, J.P.; Wetzels, J.F.; Lee, N.; De Santo, N.G.; Cirillo, M. Estimating glomerular filtration rate: Cockcroft-Gault and Modification of Diet in Renal Disease formulas compared to renal inulin clearance. Clin. J. Am. Soc. Nephrol. 2009, 4, 899–906. [Google Scholar] [CrossRef]
- Walpole, S.C.; Prieto-Merino, D.; Edwards, P.; Cleland, J.; Stevens, G.; Roberts, I. The weight of nations: An estimation of adult human biomass. BMC Public Health 2012, 12, 439. [Google Scholar] [CrossRef]
- Katherina, K.; Sudiarti, T. Body weight prediction model using mid upper arm circumferences and knee height in adult. Indones. J. Public Health Nutr. 2020, 1, 24–32. [Google Scholar] [CrossRef]
- Hayes, D.J.; van Buuren, S.; ter Kuile, F.O.; Stasinopoulos, D.M.; Rigby, R.A.; Terlouw, D.J. Developing regional weight-for-age growth references for malaria-endemic countries to optimize age-based dosing of antimalarials. Bull. World Health Organ. 2015, 93, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Heymsfield, S.B.; Peterson, C.M.; Thomas, D.M.; Heo, M.; Schuna, J.M. Why are there race/ethnic differences in adult body mass indexadiposity relationships? A quantitative critical review. Obes. Rev. 2016, 17, 262–275. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Type of Study (POP PK Software) | Population Included in the Study (n) | Dosage Regimen; Route of Administration; Timing of Blood Sampling | Age (Years) | Weight (Kg) | Clearance Creatinine (CLCr; mL/min) | PK Parameters * |
|---|---|---|---|---|---|---|---|
| Meropenem | |||||||
| Jaruratanasirikul et al. (2003) [39] | Non-POP PK (NA) | Healthy subjects (12) | 500–1000 mg Bolus (10 min) and 3 h infusion Single dose | 32.58 ± 8.94 (18–48) | 59.69 ± 7.83 (45–72) | NI | Vd, CL, t1/2 |
| Krueger et al. (2005) [40] | POP PK (NPAG) | Healthy subjects (16) | Low dose group: 0.5 g 0.5 h infusion Q8 h or three doses of 0.5 g as CoI after LD of 0.25 g High dose group: double dose of low dose group Multiple doses | 22.5 c | 66.6 c | NI | Vc, CL, KCP, KPC |
| Muro et al. (2011) [41] | POP PK (NONMEM) | Japanese Patients a (68) | NI about dose and route administration Multiple doses | 71.5 ± 13.5 (25–91) | 52.1 ± 13.9 (30.7–107) | 65.5 ± 55.8 (8.8–406) | Vd, CL |
| Li et al. (2006) [42] | POP PK (NONMEM) | Patients with IAI, CAP, VAP (79) | 05–2 g 0.5 to 3 h infusion Multiple doses | 39.6 ± 18.2 (18–93) | 73.0 ± 16.1 (40.6–127) | 93 | Vd, CL, t1/2 |
| Mathew et al. (2016) [43] | POP PK(Pmetrics) | ICU patients with sepsis, polytrauma (35) | 500–1000 mg bid or tid 0.5 to 3 h infusion Multiple doses | NI | NI | 65.08 ± NI (10–134.8) | Vc, Ke, KCP, KPC |
| Idoate grijalba et al., (2019) [44] | POP PK(Pmetrics) | ICU Patients (80) | Multiple doses | 63.26 ± 15.07 | 72.76 ± 19.17 | b | Vd, Ke |
| Imipenem | |||||||
| Jaruratanasirikul et al. (2005) [45] | Non-POP PK (NA) | Healthy subjects (8) | 500 mg or 1000 mg 0.5 to 2 h infusion Q6 h Multiple doses | 28.25 ± 4.98 (24–39) | 58.75 ± 8.61 (51–75) | NI | Vd, CL, t1/2 |
| Norrby et al. (1983) [46] | Non-POP PK (NA) | Healthy subjects (16) | 500–1000 mg with or without cilastatin Q8 h 20 min infusion Multiple doses | 25 ± NI (18–40) | 75 ± NI (60–89) | NI | Vc, CL, t1/2, KCP, KPC |
| Yoshizawa et al. (2012) [47] | POP PK (NONMEM) | Patients with renal impairment (27) | 500 mg with 500 mg cilastatin (NI) 0.5 to 1 h infusion Single dose | 59.12 b | 58.76 b | 57.95 b | Vc, Vp, CLren, CLnon-ren, Q |
| Finch (1986) [48] | Non-POP PK (NA) | Elderly Patients with acute LRTIs (6) | 500 mg with 500 mg cilastatin Q6 h Over 0.5 h infusion Multiple doses | 76.7 (68–83) | 63.3 (49.8–76) | 50.6 (31–80) | Vd, CL, t1/2 |
| Abhilash et al. (2015) [49] | Non-POP PK (NA) | ICU patients with renal, pulmonary, gastrointestinal, and skin infections (30) | 1 g Q8 h Over 40 min infusion Multiple doses | 43 ± NI (23–81) | 64.1 ± 10.74 (38–83) | NI (30–181) | Vd, t1/2 |
| Couffignal et al. (2014) [50] | POP PK (Monolix) | ICU patients with pneumonia (51) | 500–1000 mg Q8 h 0.5 h infusion Multiple doses | 59.31 b | 78.47 b | 121.72 b,d | Vc, Vp, CL, Q |
| Doripenem | |||||||
| Kim et al. (2018) [51] | POP PK (NONMEM) | Healthy subjects (11) | 250 mg 1 h infusion Single dose | 25 Range (22–30) | 60.9 Range (50–80) | 122 Range (101–139) | Vc, Vp, CL, Q |
| Bhavnani et al. (2005) [52] | POP PK (NONMEM) | Healthy subjects (24) | 500–1000 mg Q8–12 h IV Multiple doses | NI (18–65) | NI | NI | Vc, Vp, CL, Q |
| Lee et al. (2017) [53] | POP PK (NONMEM) | Patients with pyelonephritis, IAI, neutropenic fever, sepsis (37) | 250 mg or 500 mg Q8 h 1 h infusion Multiple doses | 61.7 ± 17.9 (NI) | 59.8 ± 12.4 (NI) | 66.7 ± 34.4 (NI) | Vd, CL |
| Bhalodi et al. (2013) [54] | POP PK (big NPAG) | Non-ICU patients a (12) | 250–2000 mg Q8–12 h 1 to 4 h infusion Multiple doses | 59.7 ± 18.7 (NI) | 96.2 ± 40.8 (NI) | 98.8 ± 55.3 (15–221) | Vc, Vd, CL, KCP, KPC |
| Abdul-Aziz et al. (2016) [55] | POP PK (NONMEM) | ICU patients with IAI, sepsis, VAP (12) | 500 mg Q8 h 1 h infusion Mixed single and multiple doses | 47.97 b | NI | 83.9 b | Vc, Vp, CL, Q |
| Roberts et al., (2013) [56] | POP PK (NONMEM) | ICU patient with nosocomial pneumonia (31) | 250 or 500 mg 0.5 to 4 h infusion Multiple doses | 57.8 ± 14.9 (NI) | 83.0 ± 19.0 (NI) | 137 ± 71 (NI) | Vc, Vp, CL, Q |
| Linezolid | |||||||
| Yang et al. (2017) [57] | Non-POP PK (NA) | Healthy subjects (22) | 600 mg Oral or 1 h infusion Single dose | 28.27 ± 2.21 (NI) | 66.73 ± 4.15 (NI) | NI | Vd, CL, t1/2 |
| Stalker et al. (2003) [58] | Non-POP PK (NA) | Healthy subjects (30) | 375–625 mg Q12 h Oral and IV Single and multiple doses | 625 mg = 33.0 (21.7–48.0) IV 625 mg = 24.8 (19.0–33.0) | 625 mg = 73.3 (54.2–80.7) IV 625 mg = 79.4 (67.6–94.6) | NI | Vd, CL, CLren, Clnon-ren, t1/2 |
| Sasaki et al. (2011) [59] | POP PK (NONMEM) | Patients with infectious diseases a (50) | 300–600 mg bid 1 to 2 h infusion Multiple doses | 69.1 ± 12.8 (32–92) | 57.3 ± 12.1 (38.4–100) | 74.0 ± 54.5 (9.43–330) | Vd, CL |
| Crass et al. (2019) [60] | POP PK (NONMEM) | Adult patients with oral and/or intravenous linezolid (603) | 600 mg Q12 h Oral or IV Number of doses: NI. | 62 ± 15 | 76 ± 19 | 81 ± 39 | Vd, Clnon-ren, Clren, Ka |
| Ide et al. (2018) [61] | POP PK (NONMEM) | ICU patients with sepsis or septic shock (17 divided into two groups #) | 600 mg Q12 h 1 h infusion Multiple doses | Group 1: 65.1 ± 14.5 Group 2: 74.3 ± 11.3 | Group 1: 57.8 ± 7.54 Group 2: 53.4 ± 10.2 | Group 1: 98.1 b Group 2: 20.59 b | Vc, Vp, CL, Q |
| Taubert et al. (2016) [62] | POP PK (NONMEM) | ICU patients with ARDS, peritonitis, pneumonia (52) | 600 mg bid Short duration IV (10 min to 2 h infusion) or oral Multiple doses | 57.66 b | 77.03 b | 92.64 b | Vc, Vp, CL, Q |
| Vancomycin | |||||||
| Yamamoto et al. (2009) [63] | POP PK (NONMEM) | Healthy subjects (6) | 500–1000 mg Over 1 h infusion Multiple doses | 21.7 ± 2.0 (20–25) | 60.3 ± 3.7 (55.2–64.2) | 89.3 ± 10.4 (76.7–106.5) | Vc, Vp, CL, Q |
| Healy et al. (1987) [64] | Non-POP PK (NA) | Healthy subjects (11) | 500 mg Q6 h or 1 g q12 h 1 h infusion Multiple doses | 24.7 ± 2.1 (NI) | 66.5 ± 11.2 (NI) | 110 ± 19.3 (NI) | Vc, Vss, CL |
| Shen et al. (2018) [65] | POP PK (NONMEM) | Adult patients (380) | No more than 2 g/day Duration of infusion: NI Multiple doses | 61.35 b | 61.75 b | 86.91 b | Vd, CL |
| Sanchez et al. (2010) [66] | POP PK (NONMEM) | Hospitalised patients a (141) | 1628 g/day Q6–48 h Duration of infusion: NI Multiple doses | 55 ± 14.58 (NI) | 73.2 ± 17.48 (NI) | 76.13 e | Vc, Vp, CL, Q |
| Dedkaew et al. (2015) [67] | POP PK (NLME) | ICU patients with bacteraemia, pneumonia, SSTI, meningitis, others (138) | 1 g Q12 h or Q24 h 1 to 2 h infusion Multiple doses | 65.7 ± 17.6 (18–97) | 62.1 ± 13.7 (31.7–105) | 54.5 ± 29.1 (10.03–105) | Vc, Vp, CL, Cmin |
| Roberts et al. (2011) [68] | POP PK (NONMEM) | ICU patients with sepsis (206) | LD = 750–1000 mg 0.5 h infusion MD = 2000–3000 mg 24 h infusion | 58.1 ± 14.8 (NI) | 74.8 ± 15.8 (NI) | 90.7 ± 60.4 | Vd, CL |
| Antibiotics | PK Parameters | |||||
|---|---|---|---|---|---|---|
| Vd | CL | |||||
| Patient Characteristics | Clinical Condition | Clinical Parameters | Patient Characteristics | Clinical Condition | Clinical Parameters | |
| Meropenem | - | - | - | Age [42] | - | - |
| Imipenem | - | - | Serum albumin [50] | - | - | - |
| Doripenem | - | - | - | Weight [51] | - | - |
| Linezolid | Body surface area [60] | Peritonitis (469) | - | Age [60]; body surface area [60] | Severe liver cirrhosis [59]; acute respiratory distress syndrome [62] | Fibrinogen and lactate [62] |
| Vancomycin | Age [65,66]; Body weight [68] | Patients’ status (healthy or patients) [63]; type of infectious diseases [63] | - | - | - | - |
| Antimicrobials | Population | Comp (n) | Vc (L/kg) | Vp (L/kg) | CL (L/h/kg) | t1/2 (h) | Q (L/h) | KCP (/h) | KPC (/h) |
|---|---|---|---|---|---|---|---|---|---|
| Meropenem | Asian healthy subjects [39] | One (14) | Dose 1 g = 0.20 Dose 0.5 g = 0.16 | NI | Dose 1 g = 0.22 Dose 0.5 g = 0.21 | Dose 1 g = 0.64 Dose 0.5 g = 0.54 | NI | NI | NI |
| Comparator healthy subjects [40] | Two (6–18) | Dose 1 g = 0.19 Ϯ Dose 0.5 g = 0.18 Ϯ | Dose 1 g = 0.06 ** Dose 0.5 g = 0.06 ** | Dose 1 g = 0.25 Ϯ Dose 0.5 g = 0.24 Ϯ | NI | NI | 1.21 | 4.03 | |
| Asian non-ICU patients [41] | One (1) | 0.64 Ϯ | NI | 0.21 (IIV = 52.1%) | NI | NI | NI | NI | |
| Comparator non-ICU patients [42] | Two (1–12) | 0.15 (IIV = 14.3%) Vd-tot = 0.32 | 0.17 (IIV = 10.2%) | 0.2 (IIV = 11.8%) | NI | 18.6 (IIV = 29.3%) | NI | NI | |
| Asian ICU patients [43] | Two (10) | 0.16 a,Ϯ | 0.19 ** | 0.08 a,b,Ϯ | NI | NI | 1.85 Ϯ | 1.53 Ϯ | |
| Comparator ICU patients [44] | One (1–2) | 0.34 (IIV) = 71.2%) | NI | 0.04 (IIV = 59.3%) | NI | NI | NI | NI | |
| Imipenem | Asian healthy subjects [45] | Non-comp (10) | 0.5 h infusion = 0.16 2 h infusion with dose 0.5 g = 0.16 2 h infusion with dose 1 g = 0.19 | NI | 0.5 h infusion = 0.14 2 h infusion with dose 0.5 g = 0.15 2 h infusion with dose 1 g = 0.14 | 0.5 h infusion = 1.32 2 h infusion with dose 0.5 g = 1.02 2 h infusion with dose 1 g = 2.42 | NI | NI | NI |
| Comparator healthy subjects [46] | Two (8–12) | Dose 0.5 g = 0.14 Vd-tot = 0.15 Dose 1 g = 0.13 Vd-tot = 0.14 | Dose 0.5 g = 0.05 ** Dose 1 g = 0.06 ** | Dose 0.5 g = 0.16 Dose 1 g = 0.15 | Both dosing regimens = 1.0 | NI | Dose 0.5 g = 0.8 Dose 1 g = 1.0 | Dose 0.5 g = 2.2 Dose 1 g = 2.3 | |
| Asian non-ICU patients [47] | Two (6–7) | 0.19 (IIV = 18.9%) Vd-tot = 0.25 | 0.06 Ϯ | 0.14/0.07/0.06 c (IIV for CL renal = 34.1%; for CL non-renal = 29.4%) | NI | 3.18 Ϯ | NI | NI | |
| Comparator non-ICU patients [48] | Non-comp (6) | 0.33 | NI | 0.17 | 1.6 | NI | NI | NI | |
| Asian ICU patients [49] | Non-comp (4) | 0.51/0.54 d | NI | 0.36/0.39 d | 0.98/0.97 d | NI | NI | NI | |
| Comparator ICU patients [50] | Two (3–6) | 0.26 (IIV = 48%) Vd-tot = 0.38 | 0.12 Ϯ | 0.16 (IIV = 48%) | NI | 12.2 Ϯ | NI | NI | |
| Doripenem | Asian healthy subjects [51] | Two (12) | 0.26 Vd-tot = 0.31 (IIV = 35.3%) | 0.05 | 0.36 (IIV = 31.6%) | 1.01 Ϯ | 1.83 Ϯ | NI | NI |
| Comparator healthy subjects [52] | Two (1–2) | 0.13 (IIV = 14.4%) Vd-tot = 0.21 | 0.08 (IIV = 10.4%) | 0.21 (IIV = 13.2%) | 0.95 Ϯ | 9.69 Ϯ | NI | NI | |
| Asian non-ICU patients [53] | One (4) | 0.28 (IIV = 47.3%) | NA | 0.11 (IIV = 55%) | NI | NI | NI | NI | |
| Comparator non-ICU patients [54] | Two (3–4) | 0.19 Ϯ | 0.16 ** | 0.16 Ϯ | NI | NI | 4.7 | 5.7 | |
| Asian ICU patients [55] | Two (6–8) | 0.22 (IIV = 62%) Vd-tot = 0.47 | 0.25 (IIV = 73.3%) | 0.14 (IIV = 56.7%) | NI | 36.3 Ϯ | NI | NI | |
| Comparator ICU patients [56] | Two (4–5) | 0.29 (IIV = 93.7%) Vd-tot = 0.55 | 0.25 (IIV = 62.6%) | 0.25 (IIV = 52.8%) | NI | 23.3 Ϯ | NI | NI | |
| Linezolid | Asian healthy subjects [57] | Non-comp Single dose (13) | IV = 0.67 Oral = 0.65 | NA | IV = 0.10 Oral = 0.11 | IV = 4.37 Oral = 4.33 | NI | NI | NI |
| Comparator healthy subjects [58] | Non-comp Single dose e (36 over 11–16 days) | IV 625 mg = 0.58 Oral 625 mg = 0.61 | NI | IV 625 mg c = 0.10/0.03/0.07 Oral 625 mg c = 0.09/0.03/0.06 | IV 625 mg = 4.40 Oral 625 mg = 4.87 | NI | NI | NI | |
| Asian non-ICU patients [59] | One (1–5) | 0.59 (IIV = 35.8%) | NA | 0.05 (IIV = 30.6%) | NI | NI | NI | NI | |
| Comparator non-ICU patients [60] | One (2–3) | 0.58 (IIV = 17.8%) | NA | 0.07 (IIV = 49.9%) | NI | NI | NI | NI | |
| Asian ICU patients [61] | Two (6) | Group 1 # = 0.34 Group 2 # = 0.37 (IIV = 32.3%) Vd-tot for: Group 1 # = 0.73 Group 2 # = 0.79 | Group 1 # = 0.39 Group 2 # = 0.42 (IIV = 12.3%) | Group 1 # = 0.11 Group 2 # = 0.04 (IIV = 44.8%) | NI | 26.4 | NI | NI | |
| Comparator ICU patients [62] | Two (32 over 4 days) | 0.19 f (IIV = 37%) Vd-tot = 0.54 | 0.35 f,Ϯ | 0.10 f (IIV = 58%) | NI | 67.7 f | NI | NI | |
| Vancomycin | Asian healthy subjects [63] | Two (7–8) | 0.21 (IIV = 18.2%) | 0.65 (IIV = 72.8%) | 0.06 (IIV = 37.5%) | NI | 8.81 (IIV = 19.2%) | NI | NI |
| Comparator healthy subjects [64] | Three (11–17) | Dose 0.5 g = 0.14 Dose 1 g = 0.11 | NI | Dose 0.5 g = 0.08 Dose 1 g = 0.08 | Dose 0.5 g = 8.1 Dose 1 g = 7.7 | NI | NI | NI | |
| Asian non-ICU patients [65] | One (2) | 0.73 (IIV = 24.8%) | NI | 0.06 (IIV = 12.5%) | NI | NI | NI | NI | |
| Comparator non-ICU patients [66] | Two (1–2) | 0.28 Ϯ Vd-tot = 0.72 | 0.44 (IIV = 6.8%) | 0.03/0.04 g (IIV = 24.5%) | NI | 8.13 | NI | NI | |
| Asian ICU patients [67] | Two (2–8) | 0.40 (IIV = 46%) Vd-tot = 0.79 | 0.39 Ϯ (IIV = 36.5%) | 0.05 (IIV = 14%) | NI | NI | NI | NI | |
| Comparator ICU patients [68] | One (2–3) | 1.53 (IIV = 37.4%) | NA | 0.06 (IIV = 38.9%) | NI | NI | NI | NI |
| Antimicrobials | PK Parameters | |
|---|---|---|
| Vd | CL | |
| Meropenem [39,40,41,42,43,44] | Were not observed | Were not observed |
| Imipenem [45,46,47,48,49,50] | Were not observed | Were not observed |
| Doripenem [51,52,53,54,55,56] | Were observed Indicating: Asians > non-Asians [62,63] | Were not observed |
| Linezolid [57,58,59,60,61,62] | Were not observed | Were not observed |
| Vancomycin [63,64,65,66,67,68] | Were not observed | Were not observed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Setiawan, E.; Cotta, M.O.; Roberts, J.A.; Abdul-Aziz, M.H. A Systematic Review on Antimicrobial Pharmacokinetic Differences between Asian and Non-Asian Adult Populations. Antibiotics 2023, 12, 803. https://doi.org/10.3390/antibiotics12050803
Setiawan E, Cotta MO, Roberts JA, Abdul-Aziz MH. A Systematic Review on Antimicrobial Pharmacokinetic Differences between Asian and Non-Asian Adult Populations. Antibiotics. 2023; 12(5):803. https://doi.org/10.3390/antibiotics12050803
Chicago/Turabian StyleSetiawan, Eko, Menino Osbert Cotta, Jason A. Roberts, and Mohd Hafiz Abdul-Aziz. 2023. "A Systematic Review on Antimicrobial Pharmacokinetic Differences between Asian and Non-Asian Adult Populations" Antibiotics 12, no. 5: 803. https://doi.org/10.3390/antibiotics12050803
APA StyleSetiawan, E., Cotta, M. O., Roberts, J. A., & Abdul-Aziz, M. H. (2023). A Systematic Review on Antimicrobial Pharmacokinetic Differences between Asian and Non-Asian Adult Populations. Antibiotics, 12(5), 803. https://doi.org/10.3390/antibiotics12050803