
Predicted Environmental Risk Assessment of Antimicrobials with Increased Consumption in Portugal during the COVID-19 Pandemic; The Groundwork for the Forthcoming Water Quality Survey

 ,
,
Abstract
1. Introduction
2. Results
2.1. Antimicrobial Consumption—Hospital and Ambulatory Sectors
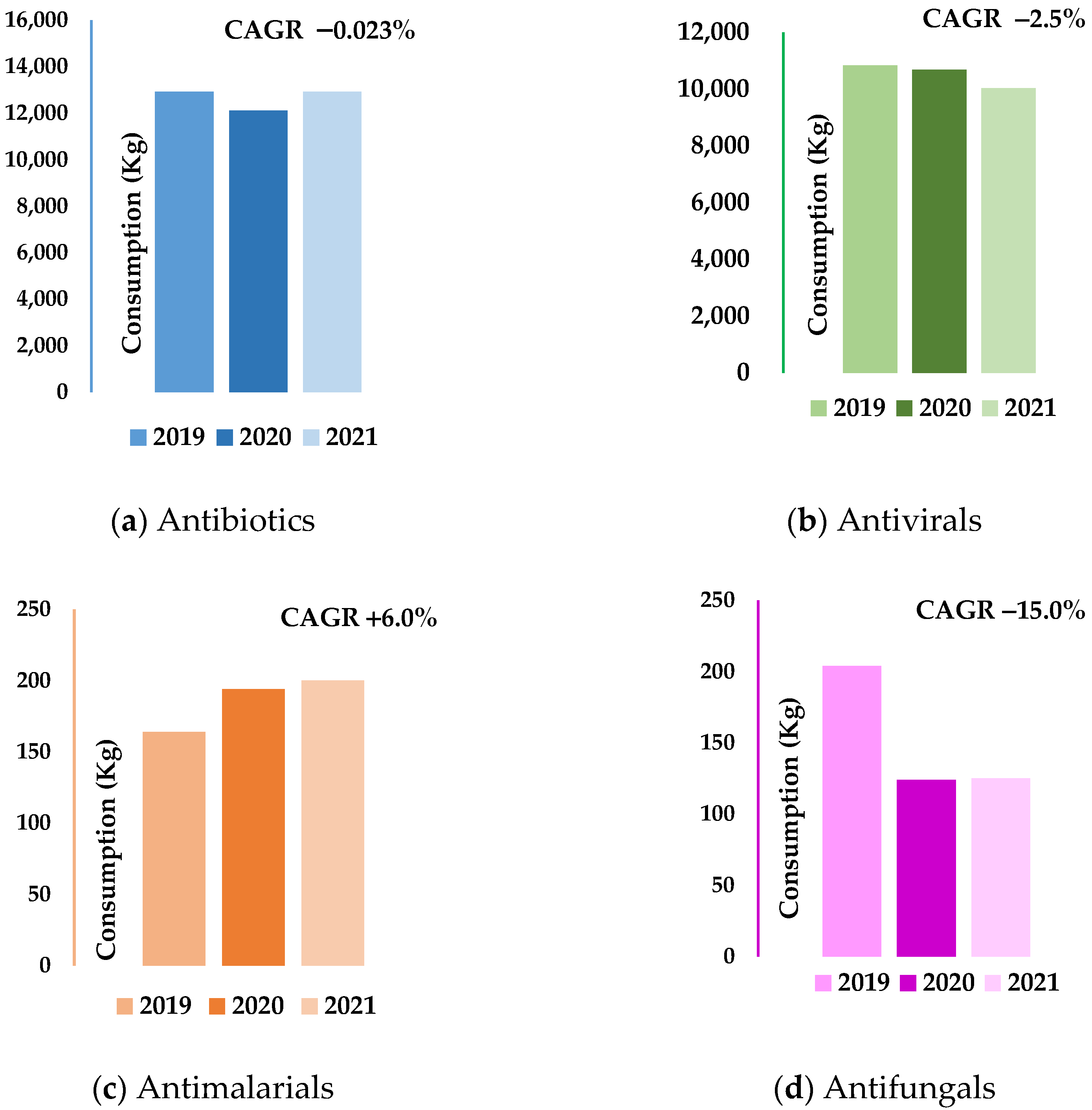
2.2. Consumption Analysis per Therapeutic Class and Its Active Substances
2.3. Consumption Analysis per Region Based on Fpen Assessment
2.4. Predictive Environmental Risk Assessment of Selected Antimicrobials
2.4.1. Excretion Factor Values
2.4.2. Predictive Environmental Concentration (PEC) Assessment for the Selected Substances
2.4.3. Predicted No-Effect Concentration Assessment and Risk Characterisation of Selected Substances
3. Discussion
3.1. Antimicrobial Consumption
3.2. Environmental Risk Assessment
4. Materials and Methods
4.1. Consumption of Antimicrobial Drugs
4.2. Assessment of Market Penetration Factor (Fpen)
4.3. Metabolisation and Excretion Fraction of the Most Representative Antimicrobials
4.4. Predictive Environmental Risk Assessment of Selected Antimicrobials
4.4.1. Calculation of Predicted Environmental Concentrations in Surface Waters (PECs)
4.4.2. Calculation of Predicted No-Effect Concentrations (PNECs)
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antimicrobial Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed on 24 September 2022).
- Purssell, E. Antimicrobials. In Understanding Pharmacology in Nursing Practice; Hood, P., Khan, E., Eds.; Springer: Cham, Switzerland, 2020; pp. 147–165. [Google Scholar]
- Kräusslich, H.-G.; Bartenschlager, R. Antiviral Strategies. In Handbook of Experimental Pharmacology; Kräusslich, H.-G., Bartenschlager, R., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; Volume 189. [Google Scholar]
- De Clercq, E. Strategies in the Design of Antiviral Drugs. Nat. Rev. Drug Discov. 2002, 1, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Nannou, C.; Ofrydopoulou, A.; Evgenidou, E.; Heath, D.; Heath, E.; Lambropoulou, D. Antiviral Drugs in Aquatic Environment and Wastewater Treatment Plants: A Review on Occurrence, Fate, Removal and Ecotoxicity. Sci. Total Environ. 2020, 699, 134322. [Google Scholar] [CrossRef] [PubMed]
- Tompa, D.R.; Immanuel, A.; Srikanth, S.; Kadhirvel, S. Trends and Strategies to Combat Viral Infections: A Review on FDA Approved Antiviral Drugs. Int. J. Biol. Macromol. 2021, 172, 524–541. [Google Scholar] [CrossRef] [PubMed]
- Burns, E.E.; Carter, L.J.; Snape, J.; Thomas-Oates, J.; Boxall, A.B.A. Application of Prioritization Approaches to Optimize Environmental Monitoring and Testing of Pharmaceuticals. J. Toxicol. Environ. Health 2018, 21, 115–141. [Google Scholar] [CrossRef] [PubMed]
- Viana, P.; Meisel, L.; Lopes, A.; de Jesus, R.; Sarmento, G.; Duarte, S.; Sepodes, B.; Fernandes, A.; dos Santos, M.M.C.; Almeida, A.; et al. Identification of Antibiotics in Surface-Groundwater. A Tool towards the Ecopharmacovigilance Approach: A Portuguese Case-Study. Antibiotics 2021, 10, 888. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Mozaz, S.; Vaz-Moreira, I.; Varela Della Giustina, S.; Llorca, M.; Barceló, D.; Schubert, S.; Berendonk, T.U.; Michael-Kordatou, I.; Fatta-Kassinos, D.; Martinez, J.L.; et al. Antibiotic Residues in Final Effluents of European Wastewater Treatment Plants and Their Impact on the Aquatic Environment. Environ. Int. 2020, 140, 105733. [Google Scholar] [CrossRef] [PubMed]
- Gros, M.; Catalán, N.; Mas-Pla, J.; Čelić, M.; Petrović, M.; Farré, M.J. Groundwater Antibiotic Pollution and Its Relationship with Dissolved Organic Matter: Identification and Environmental Implications. Environ. Pollut. 2021, 289, 117927. [Google Scholar] [CrossRef]
- Schwartz, T.; Kohnen, W.; Jansen, B.; Obst, U. Detection of Antibiotic-Resistant Bacteria and Their Resistance Genes in Wastewater, Surface Water, and Drinking Water Biofilms. FEMS Microbiol. Ecol. 2002, 43, 325–335. [Google Scholar] [CrossRef]
- Kummerer, K. Resistance in the Environment. J. Antimicrob. Chemother. 2003, 54, 311–320. [Google Scholar] [CrossRef]
- Silva, T.M.; Estrela, M.; Gomes, E.R.; Piñeiro-Lamas, M.; Figueiras, A.; Roque, F.; Herdeiro, M.T. The Impact of the COVID-19 Pandemic on Antibiotic Prescribing Trends in Outpatient Care: A Nationwide, Quasi-Experimental Approach. Antibiotics 2021, 10, 1040. [Google Scholar] [CrossRef]
- Chen, X.; Lei, L.; Liu, S.; Han, J.; Li, R.; Men, J.; Li, L.; Wei, L.; Sheng, Y.; Yang, L.; et al. Occurrence and Risk Assessment of Pharmaceuticals and Personal Care Products (PPCPs) against COVID-19 in Lakes and WWTP-River-Estuary System in Wuhan, China. Sci. Total Environ. 2021, 792, 148352. [Google Scholar] [CrossRef] [PubMed]
- Saim, S.; Behira, B. Impact of Chloroquine as Treatment of Pandemic COVID-19 on Environment. Mater. Biomater. Sci. 2021, 4, 100–105. [Google Scholar]
- European Centre for Disease Prevention and Control. Antimicrobial Consumption in the EU/EEA (ESAC-Net); Annual Epidemiological Report; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2021. [Google Scholar]
- Khouja, T.; Mitsantisuk, K.; Tadrous, M.; Suda, K.J. Global Consumption of Antimicrobials: Impact of the WHO Global Action Plan on Antimicrobial Resistance and 2019 Coronavirus Pandemic (COVID-19). J. Antimicrob. Chemother. 2022, 77, 1491–1499. [Google Scholar] [CrossRef]
- Da Silva, R.F.; Macedo, M.; Conceição, J. A Pandemia de COVID-19 Em Portugal: Evolução, Vacinação e Farmacovigilância. RevistaMultidisciplinar 2022, 4, 135–154. [Google Scholar] [CrossRef]
- Pais, R.; Taveira, N. Predicting the Evolution and Control of the COVID-19 Pandemic in Portugal. F1000Res 2020, 9, 283. [Google Scholar] [CrossRef]
- Midão, L.; Almada, M.; Carrilho, J.; Sampaio, R.; Costa, E. Pharmacological Adherence Behavior Changes during COVID-19 Outbreak in a Portugal Patient Cohort. Int. J. Environ. Res. Public Health 2022, 19, 1135. [Google Scholar] [CrossRef]
- Romano, S.; Galante, H.; Figueira, D.; Mendes, Z.; Rodrigues, A.T. Time-Trend Analysis of Medicine Sales and Shortages during COVID-19 Outbreak: Data from Community Pharmacies. Res. Soc. Adm. Pharm. 2021, 17, 1876–1881. [Google Scholar] [CrossRef]
- AlBahrani, S.; Almogbel, F.; Alanazi, W.; Almutairi, S.H.; Alanazi, M.; Maximos, S.; Azaiez, F.; Osman, A.; Almuthen, S.; Jebakumar, A.Z.; et al. Carbapenem Use Correlates with Percentage of Patients with COVID-19 in Intensive Care Units. Infection 2022. [Google Scholar] [CrossRef] [PubMed]
- PORDATA. SNS: Consultas, Internamentos e Urgências Nos Hospitais-Continente. Available online: https://www.pordata.pt/Portugal/SNS+consultas++internamentos+e+urg%C3%AAncias+nos+hospitais+++Continente-159 (accessed on 14 October 2022).
- Gironi, L.C.; Damiani, G.; Zavattaro, E.; Pacifico, A.; Santus, P.; Pigatto, P.D.M.; Cremona, O.; Savoia, P. Tetracyclines in COVID-19 Patients Quarantined at Home: Literature Evidence Supporting Real-World Data from a Multicenter Observational Study Targeting Inflammatory and Infectious Dermatoses. Dermatol. Ther. 2021, 34, 14694. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Saúde Doutor Ricardo Jorge. Infeção VIH e SIDA Em Portugal—2020; Instituto Nacional de Saúde Doutor Ricardo Jorge: Lisboa, Portugal, 2020. [Google Scholar]
- Nestler, M.J.; Godbout, E.; Lee, K.; Kim, J.; Noda, A.J.; Taylor, P.; Pryor, R.; Markley, J.D.; Doll, M.; Bearman, G.; et al. Impact of COVID-19 on Pneumonia-Focused Antibiotic Use at an Academic Medical Center. Infect. Control. Hosp. Epidemiol. 2020, 42, 7. [Google Scholar] [CrossRef]
- Pinte, L.; Ceasovschih, A.; Niculae, C.-M.; Stoichitoiu, L.E.; Ionescu, R.A.; Balea, M.I.; Cernat, R.C.; Vlad, N.; Padureanu, V.; Purcarea, A.; et al. Antibiotic Prescription and In-Hospital Mortality in COVID-19: A Prospective Multicentre Cohort Study. J. Pers. Med. 2022, 12, 877. [Google Scholar] [CrossRef] [PubMed]
- Kalhor, H.; Sadeghi, S.; Abolhasani, H.; Kalhor, R.; Rahimi, H. Repurposing of the Approved Small Molecule Drugs in Order to Inhibit SARS-CoV-2 S Protein and Human ACE2 Interaction through Virtual Screening Approaches. J. Biomol. Struct. Dyn. 2020, 40, 1299–1315. [Google Scholar] [CrossRef]
- Morikawa, K.; Oseko, F.; Morikawa, S. Immunomodulatory effect of fosfomycin on human B-lymphocyte function. Antimicrob Agents Chemother. 1993, 2, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Kazempour, M.; Izadi, H.; Chouhdari, A.; Rezaeifard, M. Anti-Inflammatory Effect of Metronidazole in Hospitalized Patients with Pneumonia Due to COVID-19. Iran. J. Pharm. Res. 2021, 20, 532–540. [Google Scholar] [CrossRef] [PubMed]
- Gharebaghi, R.; Heidary, F.; Moradi, M.; Parvizi, M. Metronidazole a Potential Novel Addition to the COVID-19 Treatment Regimen. Arch. Acad. Emerg. Med. 2020, 8, e40. [Google Scholar] [CrossRef] [PubMed]
- Chaves Filho, A.J.M.; Gonçalves, F.; Mottin, M.; Andrade, C.H.; Fonseca, S.N.S.; Macedo, D.S. Repurposing of Tetracyclines for COVID-19 Neurological and Neuropsychiatric Manifestations: A Valid Option to Control SARS-CoV-2-Associated Neuroinflammation? J. Neuroimmune Pharmacol. 2021, 16, 213–218. [Google Scholar] [CrossRef]
- Sodhi, M.; Etminan, M. Therapeutic Potential for Tetracyclines in the Treatment of COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 487–488. [Google Scholar] [CrossRef]
- Schellack, N.; Strydom, M.; Pepper, M.S.; Herd, C.L.; Hendricks, C.L.; Bronkhorst, E.; Meyer, J.C.; Padayachee, N.; Bangalee, V.; Truter, I.; et al. Social Media and COVID-19—Perceptions and Public Deceptions of Ivermectin, Colchicine and Hydroxychloroquine: Lessons for Future Pandemics. Antibiotics 2022, 11, 445. [Google Scholar] [CrossRef]
- Acharya, Y.; Sayed, A. Chloroquine and Hydroxychloroquine as a Repurposed Agent against COVID-19: A Narrative Review. Ther. Adv. Infect. Dis. 2020, 7, 2049936120947517. [Google Scholar] [CrossRef]
- Bienvenu, A.-L.; Bestion, A.; Pradat, P.; Richard, J.-C.; Argaud, L.; Guichon, C.; Roux, S.; Piriou, V.; Paillet, C.; Leboucher, G.; et al. Impact of COVID-19 Pandemic on Antifungal Consumption: A Multicenter Retrospective Analysis. Crit. Care 2022, 26, 384. [Google Scholar] [CrossRef]
- Pomati, F.; Castiglioni, S.; Zuccato, E.; Fanelli, R.; Vigetti, D.; Rossetti, C.; Calamari, D. Effects of a Complex Mixture of Therapeutic Drugs at Environmental Levels on Human Embryonic Cells. Environ. Sci. Technol. 2006, 40, 2442–2447. [Google Scholar] [CrossRef] [PubMed]
- Kümmerer, K.; Henninger, A. Promoting Resistance by the Emission of Antibiotics from Hospitals and Households into Effluent. Clin. Microbiol. Infect. 2003, 9, 1203–1214. [Google Scholar] [CrossRef]
- Sanseverino, I.; Loos, R.; Marinov, D.; Navarro Cuenca, A.; Lettieri, T. State of the Art on the Contribution of Water to Antimicrobial Resistance; EUR 29592 EN; Publications Office of the European Union: Luxembourg, 2018; ISBN 978-92-79-98478-5. [Google Scholar]
- Sandegren, L. Low Sub-Minimal Inhibitory Concentrations of Antibiotics Generate New Types of Resistance. Sustain. Chem. Pharm. 2019, 11, 46–48. [Google Scholar] [CrossRef]
- Varela, A.R.; André, S.; Nunes, O.C.; Manaia, C.M. Insights into the Relationship between Antimicrobial Residues and Bacterial Populations in a Hospital-Urban Wastewater Treatment Plant System. Water Res. 2014, 54, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Rocephalin. Available online: https://www.fass.se/LIF/product?userType=2&nplId=19940902000051 (accessed on 20 November 2022).
- Karungamye, P.; Rugaika, A.; Mtei, K.; Machunda, R. A Review of Methods for Removal of Ceftriaxone from Wastewater. J. Xenobiot. 2022, 12, 223–235. [Google Scholar] [CrossRef]
- Shipingana, L.N.N.; Shivaraju, H.P.; Yashas, S.R. Quantitative Assessment of Pharmaceutical Drugs in a Municipal Wastewater and Overview of Associated Risks. Appl. Water Sci. 2022, 12, 16. [Google Scholar] [CrossRef]
- HPRA. Summary of Product Characteristics-Targaxan. Available online: https://www.hpra.ie/homepage/medicines/medicines-information/find-a-medicine/results/item?pano=PA1336/009/001&t=Targaxan%20550%20mg%20film-coated%20tablets (accessed on 20 November 2022).
- HPRA. Summary of Product Characteristics-Malusone. Available online: https://www.hpra.ie/img/uploaded/swedocuments/LicenseSPC_PA0126-233-001_28082017170036.pdf (accessed on 20 November 2022).
- Nixon, G.L.; Moss, D.M.; Shone, A.E.; Lalloo, D.G.; Fisher, N.; O’Neill, P.M.; Ward, S.A.; Biagini, G.A. Antimalarial Pharmacology and Therapeutics of Atovaquone. J. Antimicrob. Chemother. 2013, 68, 977–985. [Google Scholar] [CrossRef] [PubMed]
- Wellvone. Available online: https://www.fass.se/LIF/product?userType=2&nplId=19970327000107 (accessed on 2 November 2022).
- Ncube, S.; Madikizela, L.M.; Chimuka, L.; Nindi, M.M. Environmental Fate and Ecotoxicological Effects of Antiretrovirals: A Current Global Status and Future Perspectives. Water Res. 2018, 145, 231–247. [Google Scholar] [CrossRef]
- Sanderson, H.; Johnson, D.J.; Reitsma, T.; Brain, R.A.; Wilson, C.J.; Solomon, K.R. Ranking and Prioritization of Environmental Risks of Pharmaceuticals in Surface Waters. Regul. Toxicol. Pharmacol. 2004, 39, 158–183. [Google Scholar] [CrossRef]
- Kümmerer, K. Pharmaceuticals in the Environment: Sources, Fate, Effects and Risks, 3rd ed.; Kümmerer, K., Ed.; Springer: Berlin/Heidelberg, Germany, 2008. [Google Scholar]
- Jain, S.; Kumar, P.; Vyas, R.K.; Pandit, P.; Dalai, A.K. Occurrence and Removal of Antiviral Drugs in Environment: A Review. Water Air Soil Pollut. 2013, 224, 1410. [Google Scholar] [CrossRef]
- Laughlin, C.; Schleif, A.; Heilman, C.A. Addressing Viral Resistance through Vaccines. Future Virol. 2015, 10, 1011–1022. [Google Scholar] [CrossRef]
- Prasse, C.; Schlüsener, M.P.; Schulz, R.; Ternes, T.A. Antiviral Drugs in Wastewater and Surface Waters: A New Pharmaceutical Class of Environmental Relevance? Environ. Sci. Technol. 2010, 44, 1728–1735. [Google Scholar] [CrossRef]
- Funke, J.; Prasse, C.; Ternes, T.A. Identification of Transformation Products of Antiviral Drugs Formed during Biological Wastewater Treatment and Their Occurrence in the Urban Water Cycle. Water Res. 2016, 98, 75–83. [Google Scholar] [CrossRef]
- Boulard, L.; Dierkes, G.; Ternes, T. Utilization of Large Volume Zwitterionic Hydrophilic Interaction Liquid Chromatography for the Analysis of Polar Pharmaceuticals in Aqueous Environmental Samples: Benefits and Limitations. J. Chromatogr. A 2018, 1535, 27–43. [Google Scholar] [CrossRef] [PubMed]
- Abafe, O.A.; Späth, J.; Fick, J.; Jansson, S.; Buckley, C.; Stark, A.; Pietruschka, B.; Martincigh, B.S. LC-MS/MS Determination of Antiretroviral Drugs in Influents and Effluents from Wastewater Treatment Plants in KwaZulu-Natal, South Africa. Chemosphere 2018, 200, 660–670. [Google Scholar] [CrossRef]
- Mosekiemang, T.T.; Stander, M.A.; de Villiers, A. Simultaneous Quantification of Commonly Prescribed Antiretroviral Drugs and Their Selected Metabolites in Aqueous Environmental Samples by Direct Injection and Solid Phase Extraction Liquid Chromatography—Tandem Mass Spectrometry. Chemosphere 2019, 220, 983–992. [Google Scholar] [CrossRef]
- Aminot, Y.; Le Menach, K.; Pardon, P.; Etcheber, H.; Budzinski, H. Inputs and Seasonal Removal of Pharmaceuticals in the Estuarine Garonne River. Mar. Chem. 2016, 185, 3–11. [Google Scholar] [CrossRef]
- K’oreje, K.O.; Vergeynst, L.; Ombaka, D.; De Wispelaere, P.; Okoth, M.; Van Langenhove, H.; Demeestere, K. Occurrence Patterns of Pharmaceutical Residues in Wastewater, Surface Water and Groundwater of Nairobi and Kisumu City, Kenya. Chemosphere 2016, 149, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Ngumba, E.; Kosunen, P.; Gachanja, A.; Tuhkanen, T. A Multiresidue Analytical Method for Trace Level Determination of Antibiotics and Antiretroviral Drugs in Wastewater and Surface Water Using SPE-LC-MS/MS and Matrix-Matched Standards. Anal. Methods 2016, 8, 6720–6729. [Google Scholar] [CrossRef]
- King, D.H. History, Pharmacokinetics, and Pharmacology of Acyclovir. J. Am. Acad. Dermatol. 1988, 18, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Prasse, C.; Wagner, M.; Schulz, R.; Ternes, T.A. Biotransformation of the Antiviral Drugs Acyclovir and Penciclovir in Activated Sludge Treatment. Environ. Sci. Technol. 2011, 45, 2761–2769. [Google Scholar] [CrossRef]
- Schlüter-Vorberg, L.; Prasse, C.; Ternes, T.A.; Mückter, H.; Coors, A. Toxification by Transformation in Conventional and Advanced Wastewater Treatment: The Antiviral Drug Acyclovir. Environ. Sci. Technol. Lett. 2015, 2, 342–346. [Google Scholar] [CrossRef]
- Sherman, E.M.; Worley, M.V.; Unger, N.R.; Gauthier, T.P.; Schafer, J.J. Cobicistat: Review of a Pharmacokinetic Enhancer for HIV Infection. Clin. Ther. 2015, 37, 1876–1893. [Google Scholar] [CrossRef]
- Rezolsta. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20131031000074 (accessed on 26 October 2022).
- Pihlaja, T.L.M.; Niemissalo, S.M.; Sikanen, T.M. Cytochrome P450 Inhibition by Antimicrobials and Their Mixtures in Rainbow Trout Liver Microsomes In Vitro. Environ. Toxicol. Chem. 2022, 41, 663–676. [Google Scholar] [CrossRef]
- INFARMED. Estatística Do Medicamento Produtos Saúde 2017. Lisboa, Portugal. 2018. Available online: https://www.infarmed.pt/documents/15786/1229727/Estat%C3%ADstica+do+Medicamento+2017/c759b946-9dcb-4b0a-b10b-6287bf76c114?version=1.0 (accessed on 2 November 2022).
- Besse, J.-P.; Kausch-Barreto, C.; Garric, J. Exposure Assessment of Pharmaceuticals and Their Metabolites in the Aquatic Environment: Application to the French Situation and Preliminary Prioritization. Hum. Ecol. Risk Assess. Int. J. 2008, 14, 665–695. [Google Scholar] [CrossRef]
- Definition and General Considerations. Available online: https://www.whocc.no/ddd/definition_and_general_considera/ (accessed on 10 May 2022).
- Almeida, A.; Duarte, S.; Nunes, R.; Rocha, H.; Pena, A.; Meisel, L. Human and Veterinary Antibiotics Used in Portugal—A Ranking for Ecosurveillance. Toxics 2014, 2, 188–225. [Google Scholar] [CrossRef]
- Guo, J.; Sinclair, C.J.; Selby, K.; Boxall, A.B.A. Toxicological and Ecotoxicological Risk-based Prioritization of Pharmaceuticals in the Natural Environment. Environ. Toxicol. Chem. 2016, 35, 1550–1559. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, H.; ter Laak, T.; Duis, K. Development and Dissemination of Antibiotic Resistance in the Environment under Environmentally Relevant Concentrations of Antibiotics and Its Risk Assessment; Literature Study; Umweltbundesamt: Dessau-Roßlau, Germany, 2017. [Google Scholar]
- Committee for Medicinal Products for Human Use. Guideline on the Environmental Risk Assessment of Medicinal Products for Human Use; European Medicines Agency: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Pereira, A.M.P.T.; Silva, L.J.G.; Lino, C.M.; Meisel, L.M.; Pena, A. A Critical Evaluation of Different Parameters for Estimating Pharmaceutical Exposure Seeking an Improved Environmental Risk Assessment. Sci. Total Environ. 2017, 603, 226–236. [Google Scholar] [CrossRef]
- Guidance on Information Requirements and Chemical Safety Assessment Chapter R.10: Characterisation of Dose [Concentration]-Response for Environment, 2008. Available online: https://echa.europa.eu/documents/10162/17224/information_requirements_r10_en.pdf/bb902be7-a503-4ab7-9036-d866b8ddce69?t=1322594768638 (accessed on 17 February 2023).
- Bengtsson-Palme, J.; Larsson, D.G.J. Concentrations of Antibiotics Predicted to Select for Resistant Bacteria: Proposed Limits for Environmental Regulation. Environ. Int. 2016, 86, 140–149. [Google Scholar] [CrossRef]
- Cefazoline. Available online: https://go.drugbank.com/drugs/DB01327 (accessed on 23 October 2022).
- EMA. Annex III-Summary of Product Characteristics, Labelling and Package leaflet-Rocephin and Associated Names. Available online: https://www.ema.europa.eu/en/documents/referral/rocephin-article-30-referral-annex-iii_en.pdf (accessed on 26 October 2022).
- Agwuh, K.N.; MacGowan, A. Pharmacokinetics and Pharmacodynamics of the Tetracyclines Including Glycylcyclines. J. Antimicrob. Chemother. 2006, 58, 256–265. [Google Scholar] [CrossRef] [PubMed]
- Flucloxacillin. Available online: https://www.medicines.org.uk/emc/product/545/smpc#gref (accessed on 20 November 2022).
- HPRA. Summary of Product Characteristics-Monuril. 2020. Available online: https://www.hpra.ie/img/uploaded/swedocuments/Licence_PA1441-002-002_24072020094950.pdf (accessed on 20 November 2022).
- Linezolid. Available online: https://go.drugbank.com/drugs/DB00601 (accessed on 21 October 2022).
- EMA. Annex I-Summary of Product Characteristics-Vaborem. 2018. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/vaborem#product-information-section (accessed on 20 November 2022).
- Flagyl. Available online: https://go.drugbank.com/drugs/DB00916 (accessed on 20 October 2022).
- Minocycline. Available online: https://go.drugbank.com/drugs/DB01017 (accessed on 2 October 2022).
- HPRA. Summary of Product Characteristics-Tazocin. Available online: https://www.hpra.ie/img/uploaded/swedocuments/LicenseSPC_PA0822-098-001_22072016100058.pdf (accessed on 20 November 2022).
- Su, C.G.; Aberra, F.; Lichtenstein, G.R. Utility of the Nonabsorbed (<0.4%) Antibiotic Rifaximin in Gastroenterology and Hepatology. Gastroenterol. Hepatol. 2006, 2, 186–197. [Google Scholar]
- Taylor, D.N.; McKenzie, R.; Durbin, A.; Carpenter, C.; Haake, R.; Bourgeois, A.L. Systemic Pharmacokinetics of Rifaximin in Volunteers with Shigellosis. Antimicrob. Agents Chemother. 2008, 52, 1179–1181. [Google Scholar] [CrossRef]
- Trimethoprim. Available online: https://go.drugbank.com/drugs/DB00440 (accessed on 2 November 2022).
- Türk, D.; Hanke, N.; Lehr, T. A Physiologically-Based Pharmacokinetic Model of Trimethoprim for MATE1, OCT1, OCT2, and CYP2C8 Drug–Drug–Gene Interaction Predictions. Pharmaceutics 2020, 12, 1074. [Google Scholar] [CrossRef]
- Vancomycin. Available online: https://go.drugbank.com/drugs/DB00512 (accessed on 12 October 2022).
- Acyclovir. Available online: https://go.drugbank.com/drugs/DB00787 (accessed on 14 October 2022).
- Abdalla, S.; Briand, C.; Oualha, M.; Bendavid, M.; Béranger, A.; Benaboud, S.; Tréluyer, J.-M.; Zheng, Y.; Capito, C.; Demir, Z.; et al. Population Pharmacokinetics of Intravenous and Oral Acyclovir and Oral Valacyclovir in Pediatric Population To Optimize Dosing Regimens. Antimicrob. Agents Chemother. 2020, 64, e01426-20. [Google Scholar] [CrossRef]
- Lamivudine. Available online: https://go.drugbank.com/drugs/DB00709 (accessed on 20 October 2022).
- EMA. Annex I-Summary of Product Characteristics-Epivir. 2022. Available online: https://www.ema.europa.eu/en/documents/product-information/epivir-epar-product-information_en.pdf (accessed on 20 October 2022).
- EMA. Annex I-Summary of Product Characteristics-Emtriva. Available online: https://www.ema.europa.eu/en/documents/product-information/emtriva-epar-product-information_en.pdf (accessed on 22 October 2022).
- Modrzejewski, K.A.; Herman, R.A. Emtricitabine: A Once-Daily Nucleoside Reverse Transcriptase Inhibitor. Ann. Pharmacother. 2004, 38, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- EMA. Annex I-Summary of Product Characteristics-Isentress. 2022. Available online: https://www.ema.europa.eu/en/documents/product-information/isentress-epar-product-information_en.pdf (accessed on 20 October 2022).
- Burger, D.M. Raltegravir: A Review of Its Pharmacokinetics, Pharmacology and Clinical Studies. Expert Opin. Drug Metab. Toxicol. 2010, 6, 1151–1160. [Google Scholar] [CrossRef]
- EMA. Annex I-Summary of Product Characteristics-Tivicay. 2022. Available online: https://www.ema.europa.eu/en/documents/product-information/tivicay-epar-product-information_en.pdf (accessed on 20 October 2022).
- Castellino, S.; Moss, L.; Wagner, D.; Borland, J.; Song, I.; Chen, S.; Lou, Y.; Min, S.S.; Goljer, I.; Culp, A.; et al. Metabolism, Excretion, and Mass Balance of the HIV-1 Integrase Inhibitor Dolutegravir in Humans. Antimicrob. Agents Chemother. 2013, 57, 3536–3546. [Google Scholar] [CrossRef] [PubMed]
- Nicol, M.R.; Joshi, A.; Rizk, M.L.; Sabato, P.E.; Savic, R.M.; Wesche, D.; Zheng, J.H.; Cook, J. Pharmacokinetics and Pharmacological Properties of Chloroquine and Hydroxychloroquine in the Context of COVID-19 Infection. Clin. Pharmacol. Ther. 2020, 108, 1135–1149. [Google Scholar] [CrossRef] [PubMed]
- Hydroxychloroquine. Available online: https://go.drugbank.com/drugs/DB01611 (accessed on 21 October 2022).
- Baggish, A.L.; Hill, D.R. Antiparasitic Agent Atovaquone. Antimicrob. Agents Chemother. 2002, 46, 1163–1173. [Google Scholar] [CrossRef]
- Wess, R.A.; Schmidt, T.; Höger, S. Challenges of Regulatory Environmental Risk Assessment for Human Pharmaceuticals with Focus on Antibiotics. Chimia 2020, 74, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Piperacillin/Tazobactam. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20070720000011 (accessed on 25 October 2022).
- Meropenem. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20090613000065&docType=78&scrollPosition=901.69873046875 (accessed on 21 October 2022).
- Le Page, G.C. Environmental Risk Assessment of Antibiotics: Investigations into Cyanobacteria Interspecies Sensitivities and Establishing Appropriate Protection Limits. Ph.D. Thesis, University of Exeter, Exeter, UK, 2018. [Google Scholar]
- Guo, J.; Selby, K.; Boxall, A.B.A. Comparing the Sensitivity of Chlorophytes, Cyanobacteria, and Diatoms to Major-Use Antibiotics: Algal Sensitivity to Antibiotics. Environ. Toxicol. Chem. 2016, 35, 2587–2596. [Google Scholar] [CrossRef] [PubMed]
- Brain, R.A.; Johnson, D.J.; Richards, S.M.; Sanderson, H.; Sibley, P.K.; Solomon, K.R. Effects Of 25 Pharmaceutical Compounds to Lemna Gibba Using a Seven-Day Static-Renewal Test. Environ. Toxicol. Chem. 2004, 23, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Stoichev, T.; Baptista, M.S.; Basto, M.C.P.; Vasconcelos, V.M.; Vasconcelos, M.T.S.D. Effects of Minocycline and Its Degradation Products on the Growth of Microcystis Aeruginosa. Ecotoxicol. Environ. Saf. 2011, 74, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Xifaxan. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20110923000033 (accessed on 15 November 2022).
- Havelkova, B.; Beklova, M.; Kovacova, V.; Hlavkova, D.; Pikula, J. Ecotoxicity of Selected Antibiotics for Organisms of Aquatic and Terrestrial Ecosystems. Neuroendocrinol. Lett. 2016, 37, 38–44. [Google Scholar] [PubMed]
- Emtricitabine/Tenofovir Disoproxil Sandoz. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20160202000087 (accessed on 27 November 2022).
- Abacavir/Lamivudine Sandoz. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20141230000119 (accessed on 27 November 2022).
- Dovato. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20180914000069 (accessed on 15 November 2022).
- Isentress. Available online: https://www.fass.se/LIF/product?userType=2&nplId=20070602000016 (accessed on 15 November 2022).
- Plaquenil. Available online: https://www.fass.se/LIF/product?userType=2&nplId=19610412000017 (accessed on 21 October 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pharmacotherapeutic Group/Class | Antimicrobial Active Substances | 2019 | 2020 | 2021 | |||
|---|---|---|---|---|---|---|---|
| Control Consumption kg | Consumption kg | AGR % | Consumption kg | AGR % | |||
| Antibiotics | Penicillins | Flucloxacillin | 283 (H) 2792 (A) | 269 (H) 2209 (A) | −4.9 −20.9 | 326 (H) 1974 (A) | +15.2 −29.3 |
| Piperacillin | 6083 (H) | 5787(H) | −4.9 | 6206 (H) | +2.0 | ||
| Enzyme inhibitor | Tazobactam | 765 (H) | 729 (H) | −4.7 | 776 (H) | +1.4 | |
| Carbapenems | Meropenem | 479 (H) | 474 (H) | −1.0 | 518 (H) | +8.1 | |
| Cephalosporins | Cefazolin | 696 (H) | 616 (H) | −11.5 | 716 (H) | +2.9 | |
| Ceftriaxone | 879(H) | 895 (H) | +1.8 | 966 (H) | +9.9 | ||
| Sulfonamides/ Trimethoprim | Trimethoprim | 55 (H) 427 (A) | 51 (H) 403 (A) | −7.2 −5.6 | 52 (H) 447 (A) | −5.4 +4.7 | |
| Tetracyclines | Doxycycline | 225 (A) | 212 (A) | −5.8 | 248 (A) | +10.2 | |
| Minocycline | 165 (A) | 157 (A) | −4.8 | 179 (A) | +8.5 | ||
| Other Antibiotics | Fosfomycin Linezolid Metronidazole | 53 (H) 2726 (A) 81 (H) 63 (H) 975 (A) | 57 (H) 2735 (A) 79 (H) 54 (H) 830 (A) | +7.5 +0.33 −2.5 −14.3 +14.9 | 43 (H) 2866(A) 91 (H) 229 (H) 1049 (A) | −19.0 +5.1 +12.3 +263.0 +7.6 | |
| Rifaximin | 69 (H) 135 (A) | 57 (H) 174 (A) | −17.0 +29.0 | 60 (H) 274 (A) | +13.0 +102.0 | ||
| Vancomycin | 306 (H) | 305 (H) | −0.3 | 327 (H) | +6.9 | ||
| Antivirals | * NRTIs | Emtricitabine | 1217 (H) | 1312 (H) | +7.8 | 1340 (H) | +10.1 |
| Lamivudine | 1378 (H) | 1459 (H) | +5.8 | 1511(H) | +9.7 | ||
| Integrase inhibitors | Dolutegravir | 192 (H) | 229 (H) | +19.3 | 253 (H) | +31.8 | |
| Raltegravir | 1321 (H) | 1406 (H) | +6.4 | 1224 (H) | −7.3 | ||
| ** NA excl. RTIs | Valacyclovir | 1405 (H) | 1392 (H) | −0.9 | 1560 (H) | +11.0 | |
| CYP450 3A | Cobicistat | 242 (H) | 259 (H) | +7.0 | 235 (H) | −2.9 | |
| Antimalarials | Hydroxychloroquine | 4.8 (H) 1578 (A) | 17.0 (H) 1802 (A) | +45.8 +14.2 | 5.2 (H) 1727 (A) | +14.6 +9.4 | |
| Atovaquone | 158 (H) | 176 (H) | +11.4 | 192 (H) | +21.5 | ||
| Active Substances | Environmental Risk Assessment | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alentejo | Algarve | Centre | Lisbon/Tagus Valley | North | |||||||||||
| PEC µg/L 2021 | RISK (PEC/PNEC) | PEC µg/L 2021 | RISK (PEC/PNEC) | PEC µg/L 2021 | RISK (PEC/PNEC) | PEC µg/L 2021 | RISK (PEC/PNEC) | PEC µg/L 2021 | RISK (PEC/PNEC) | ||||||
| ECOtox | MICsub | ECOtox | MICsub | ECOtox | MICsub | ECOtox | MICsub | ECOtox | MICsub | ||||||
| Penicillins | |||||||||||||||
| Flucloxacillin | 0.20 | 0.02 | 0.67 | 0.25 | 0.02 | 0.83 | 0.36 | 0.03 | 1.2 | 0.48 | 0.04 | 1.6 | 0.21 | 0.02 | 0.70 |
| Piperacillin | 0.34 | ND | 5.7 | 0.18 | ND | 3.0 | 0.50 | ND | 8.3 | 0.62 | ND | 10.3 | 0.53 | ND | 8.8 |
| Tazobactam | 0.089 | 0.002 | 0.36 | 0.047 | 0.001 | 0.19 | 0.13 | 0.003 | 0.52 | 0.16 | 0.004 | 0.64 | 0.14 | 0.003 | 0.56 |
| Carbapenems | |||||||||||||||
| Meropenem | 0.065 | 0.22 | 0.81 | 0.094 | 0.31 | 1.2 | 0.23 | 0.77 | 2.9 | 0.22 | 0.73 | 2.8 | 0.12 | 0.4 | 1.5 |
| Cephalosporins | |||||||||||||||
| Cefazolin | 0.95 | 0.40 | 0.10 | 0.090 | 0.38 | 0.09 | 0.17 | 0.71 | 0.17 | 0.15 | 0.63 | 0.15 | 0.17 | 0.71 | 0.17 |
| Ceftriaxone | 0.049 | 0.15 | 1.5 | 0.13 | 0.39 | 4.1 | 0.17 | 0.51 | 5.3 | 0.10 | 0.30 | 3.1 | 0.14 | 0.42 | 4.4 |
| Trimethoprim | |||||||||||||||
| Trimethoprim | 0.020 | 1.5 × 10−4 | 0.04 | 0.036 | 2.7 × 10−4 | 0.07 | 0.065 | 4.9 × 10−4 | 0.13 | 0.06 | 4.6 × 10−4 | 0.12 | 0.046 | 3.5 × 10−4 | 0.092 |
| Tetracyclines | |||||||||||||||
| Doxycycline | 0.040 | 0.074 | 0.020 | 0.096 | 0.18 | 0.05 | 0.11 | 0.20 | 0.06 | 0.13 | 0.24 | 0.07 | 0.10 | 0.19 | 0.05 |
| Minocycline | 0.004 | 0.001 | 0.004 | 0.015 | 0.004 | 0.015 | 0.024 | 0.006 | 0.024 | 0.02 | 0.005 | 0.02 | 0.017 | 0.040 | 0.017 |
| Other Antibiotic | |||||||||||||||
| Fosfomycin | 0.21 | ND | 0.11 | 0.34 | ND | 0.17 | 0.44 | ND | 0.22 | 0.41 | ND | 0.21 | 0.32 | ND | 0.16 |
| Linezolid | 0.0022 | 0.002 | 2.8 × 1−4 | 0.0068 | 0.008 | 8.5 × 10−4 | 0.008 | 0.008 | 9.5 × 10−4 | 0.008 | 0.009 | 0.001 | 0.004 | 0.004 | 5.0 × 10−4 |
| Metronidazole | 0.10 | 0.002 | 0.80 | 0.21 | 0.005 | 1.68 | 0.26 | 0.006 | 2.08 | 0.26 | 0.006 | 2.08 | 0.19 | 0.005 | 1.52 |
| Rifaximin | 0.085 | 1.12 | ND | 0.080 | 1.05 | ND | 0.16 | 2.11 | ND | 0.12 | 1.58 | ND | 0.15 | 1.97 | ND |
| Vancomycin | 0.011 | 3.0 × 10−6 | 0.001 | 0.021 | 4.8 × 10−4 | 0.003 | 0.064 | 0.001 | 0.008 | 0.055 | 0.001 | 0.007 | 0.068 | 0.002 | 0.009 |
| Antivirals | |||||||||||||||
| Acyclovir | 0.20 | 0.008 | ND | 0.56 | 0.022 | ND | 0.74 | 0.030 | ND | 0.70 | 0.028 | ND | 0.49 | 0.020 | ND |
| Emtricitabine | 0.068 | 1.1 × 10−4 | ND | 0.28 | 4.6 × 10−4 | ND | 0.14 | 2.3 × 10−4 | ND | 0.49 | 8.0 × 10−4 | ND | 0.17 | 2.8 × 10−4 | ND |
| Lamivudine | 0.038 | 6.1 × 10−4 | ND | 0.13 | 0.002 | ND | 0.20 | 0.008 | ND | 0.49 | 0.008 | ND | 0.27 | 0.004 | ND |
| Dolutegravir | 0.0042 | 4.4 × 10−4 | ND | 0.024 | 0.003 | ND | 0.030 | 0.007 | ND | 0.071 | 0.007 | ND | 0.036 | 0.004 | ND |
| Raltegravir | 0.040 | 1.1 × 10−4 | ND | 0.13 | 3.4 × 10−4 | ND | 0.19 | 5.0 × 10−4 | ND | 0.27 | 7.1 × 10−4 | ND | 0.21 | 5.5 × 10−4 | ND |
| Cobicistat | 0.0042 | 8.7 × 10−6 | ND | 0.047 | 9.7 × 10−5 | ND | 0.014 | 1.7 × 10−4 | ND | 0.081 | 1.7 × 10−4 | ND | 0.035 | 7.2 × 10−5 | ND |
| Antimalarials | |||||||||||||||
| Hydroxychloroquine | 0.056 | 0.016 | ND | 0.83 | 0.024 | ND | 0.099 | 0.029 | ND | 0.11 | 0.032 | ND | 0.076 | 0.022 | ND |
| Atovaquone | 0.0002 | 0.24 | ND | 0.0055 | 6.63 | ND | 0.018 | 21.7 | ND | 0.054 | 65.1 | ND | 0.038 | 45.8 | ND |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almeida, A.; De Mello-Sampayo, C.; Lopes, A.; Carvalho da Silva, R.; Viana, P.; Meisel, L. Predicted Environmental Risk Assessment of Antimicrobials with Increased Consumption in Portugal during the COVID-19 Pandemic; The Groundwork for the Forthcoming Water Quality Survey. Antibiotics 2023, 12, 652. https://doi.org/10.3390/antibiotics12040652
Almeida A, De Mello-Sampayo C, Lopes A, Carvalho da Silva R, Viana P, Meisel L. Predicted Environmental Risk Assessment of Antimicrobials with Increased Consumption in Portugal during the COVID-19 Pandemic; The Groundwork for the Forthcoming Water Quality Survey. Antibiotics. 2023; 12(4):652. https://doi.org/10.3390/antibiotics12040652
Chicago/Turabian StyleAlmeida, Anabela, Cristina De Mello-Sampayo, Ana Lopes, Rita Carvalho da Silva, Paula Viana, and Leonor Meisel. 2023. "Predicted Environmental Risk Assessment of Antimicrobials with Increased Consumption in Portugal during the COVID-19 Pandemic; The Groundwork for the Forthcoming Water Quality Survey" Antibiotics 12, no. 4: 652. https://doi.org/10.3390/antibiotics12040652
APA StyleAlmeida, A., De Mello-Sampayo, C., Lopes, A., Carvalho da Silva, R., Viana, P., & Meisel, L. (2023). Predicted Environmental Risk Assessment of Antimicrobials with Increased Consumption in Portugal during the COVID-19 Pandemic; The Groundwork for the Forthcoming Water Quality Survey. Antibiotics, 12(4), 652. https://doi.org/10.3390/antibiotics12040652