

Predictive Factors of Piperacillin Exposure and the Impact on Target Attainment after Continuous Infusion Administration to Critically Ill Patients
 ,
,  , , and
, , and
Abstract
1. Introduction
2. Results
2.1. Patients and Datasets
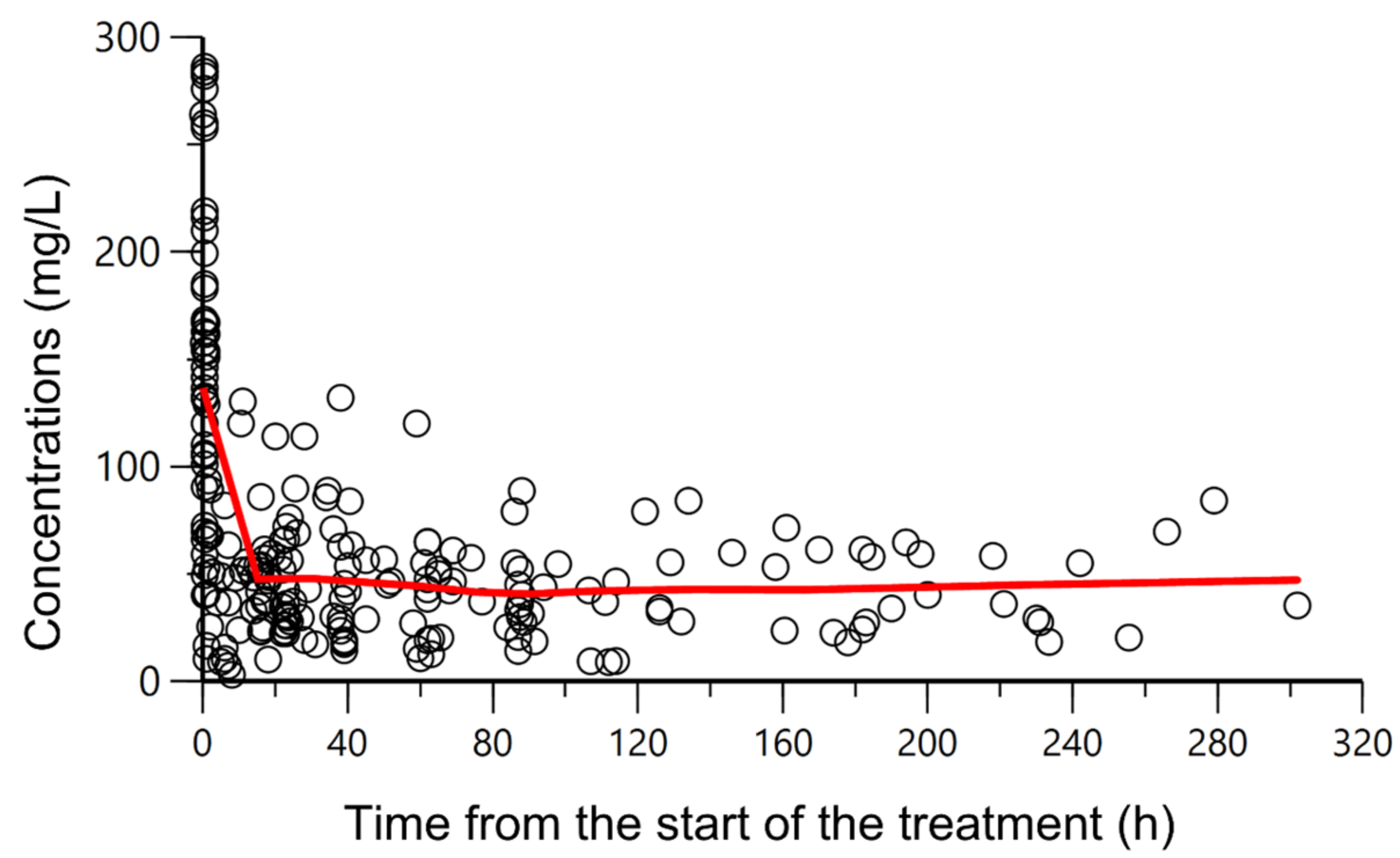
2.2. Population PK Modeling
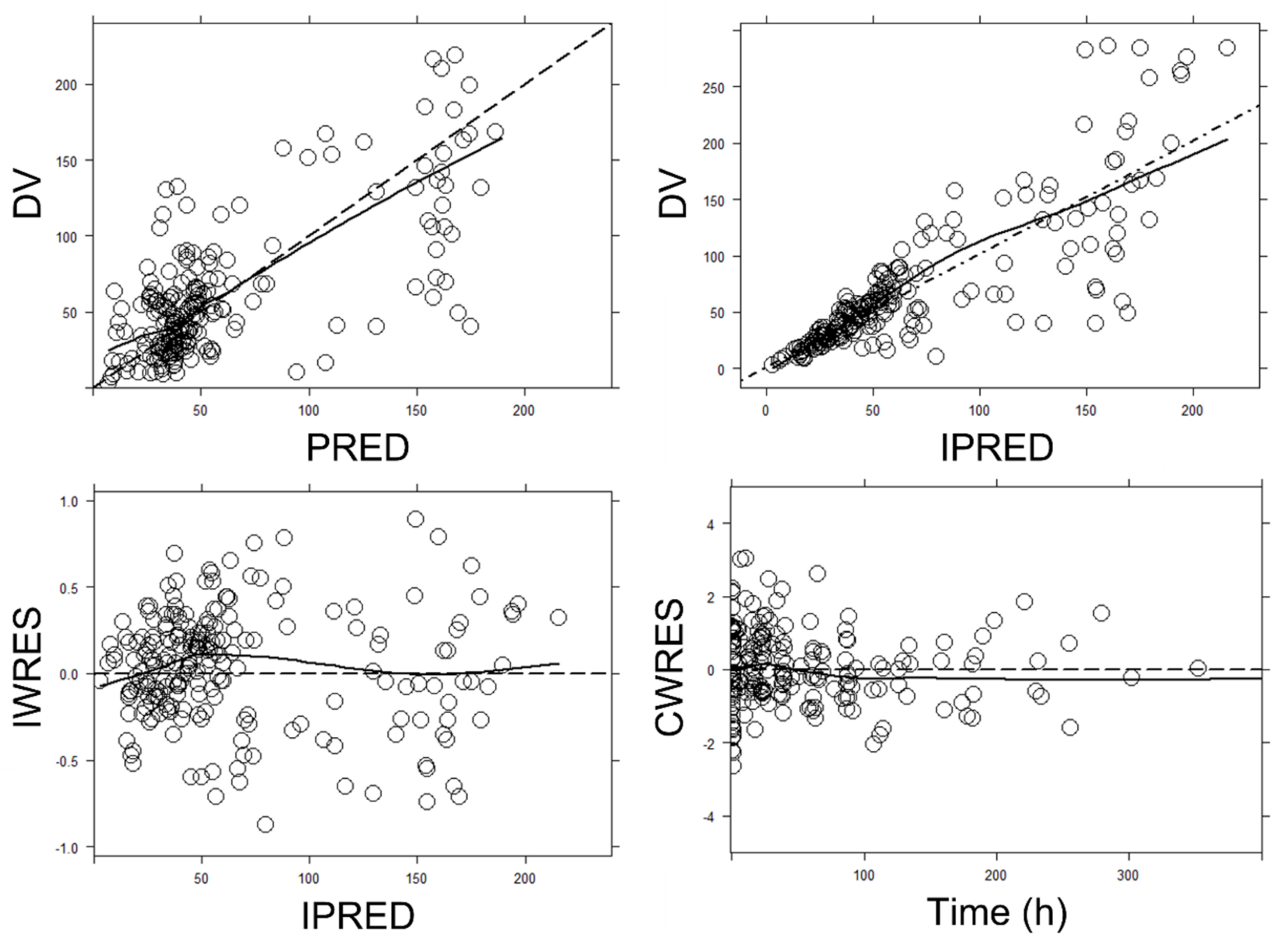
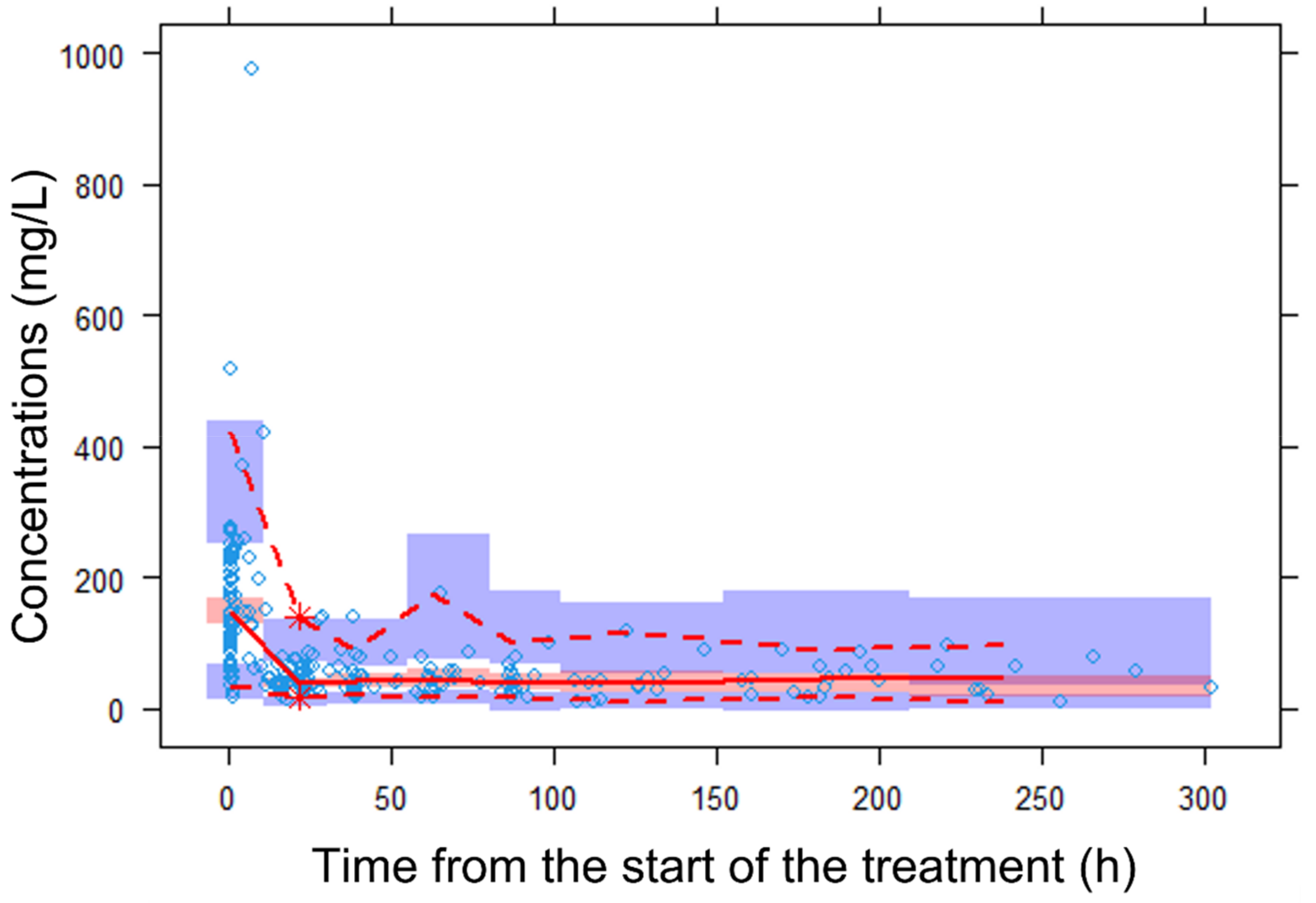
2.3. Model Evaluation
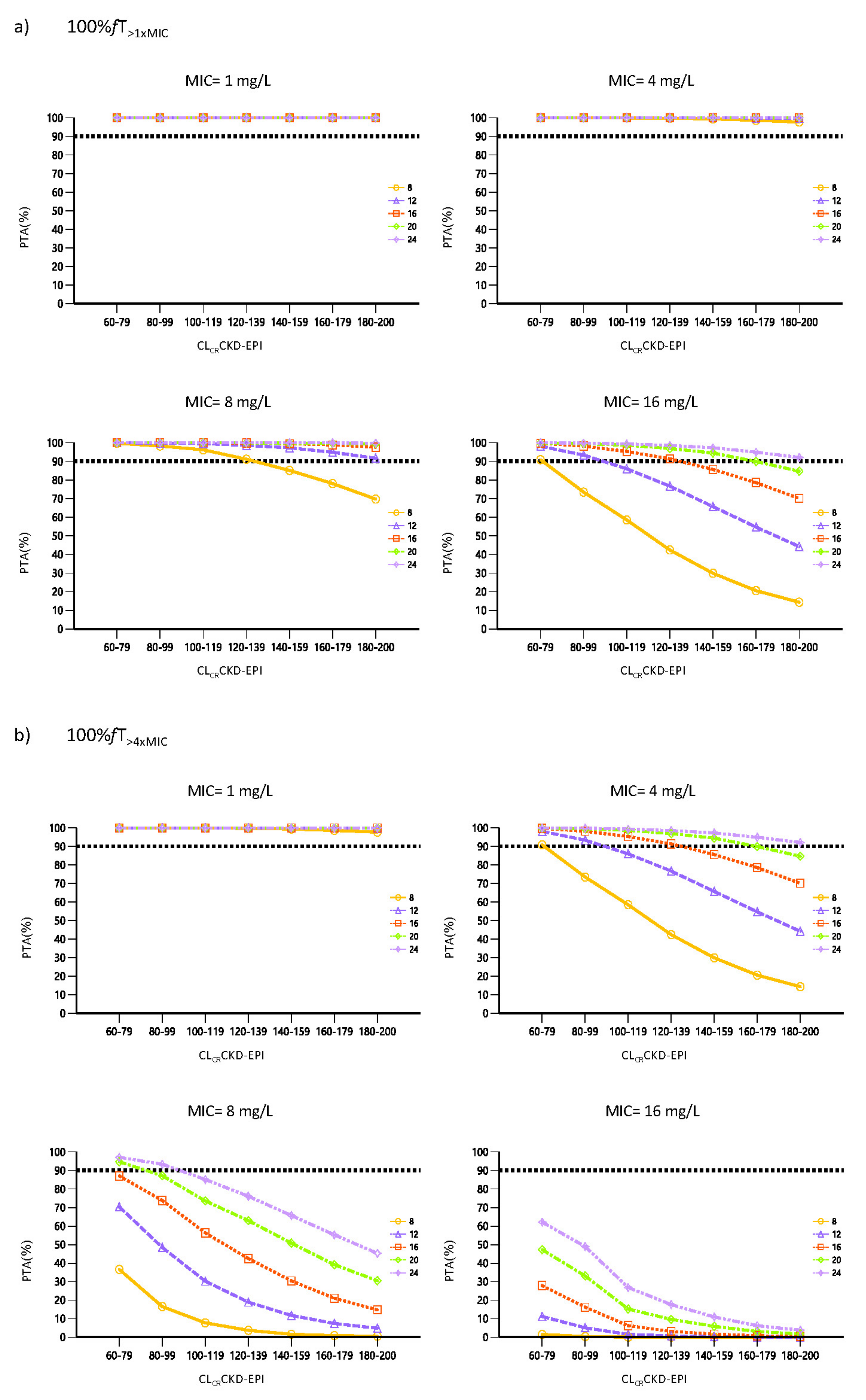
2.4. Probability of Target Attainment and Cumulative Fraction of Response
3. Discussion
4. Material and Methods
4.1. Study Design
4.2. Patient Population
4.3. Dosage, Sampling and Data Collection
4.4. Bioanalysis
4.5. Population Pharmacokinetics Analysis
4.5.1. Base Model Development
4.5.2. Covariate Model
4.5.3. Model Evaluation
4.6. Monte Carlo Simulations
4.7. Probability of Target Attainment and Cumulative Fraction of Response
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott1, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, S.; Ruokonen, E.; Varpula, T.; Ala-Kokko, T.I.; Pettilä, V. Long-term outcome and quality-adjusted life years after severe sepsis. Crit. Care Med. 2009, 37, 1268–1274. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, C.; Scherag, A.; Adhikari, N.K.; Hartog, C.S. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am. J. Respir. Crit. Care Med. 2016, 193, 259–272. [Google Scholar] [CrossRef] [PubMed]
- Claeys, K.C.; Zasowski, E.J.; Trinh, T.D.; Lagnf, A.M.; Davis, S.L.; Rybak, M.J. Antimicrobial Stewardship Opportunities in Critically Ill Patients with Gram-Negative Lower Respiratory Tract Infections: A Multicenter Cross-Sectional Analysis. Infect. Dis. Ther. 2018, 7, 135–146. [Google Scholar] [CrossRef]
- Craig, W.A. Basic pharmacodynamics of antibacterials with clinical applications to the use of β-lactams, glycopeptides, and linezolid. Infect. Dis. Clin. N. Am. 2003, 17, 479–501. [Google Scholar] [CrossRef]
- Delattre, I.K.; Taccone, F.S.; Jacobs, F.; Hites, M.; Dugernier, T.; Spapen, H.; Laterre, P.F.; Wallemacq, P.E.; Van Bambeke, F.; Tulkens, P.M. Optimizing β-lactams treatment in critically-ill patients using pharmacokinetics/pharmacodynamics targets: Are first conventional doses effective? Expert Rev. Anti. Infect. Ther. 2017, 15, 677–688. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Hope, W.W.; Roberts, J.A. Applying pharmacokinetic/pharmacodynamic principles in critically Ill patients: Optimizing efficacy and reducing resistance development. Semin. Respir. Crit. Care Med. 2015, 36, 136–153. [Google Scholar] [CrossRef]
- Blot, S.I.; Pea, F.; Lipman, J. The effect of pathophysiology on pharmacokinetics in the critically ill patient-Concepts appraised by the example of antimicrobial agents. Adv. Drug Deliv. Rev. 2014, 77, 3–11. [Google Scholar] [CrossRef]
- Hosein, S.; Udy, A.A.; Lipman, J. Physiological Changes in the Critically Ill Patient with Sepsis. Curr. Pharm. Biotechnol. 2011, 12, 1991–1995. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef]
- Roberts, J.A.; Kirkpatrick, C.M.J.; Roberts, M.S.; Dalley, A.J.; Lipman, J. First-dose and steady-state population pharmacokinetics and pharmacodynamics of piperacillin by continuous or intermittent dosing in critically ill patients with sepsis. Int. J. Antimicrob. Agents 2010, 35, 156–163. [Google Scholar] [CrossRef]
- Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M.; Myburgh, J.; Paterson, D.L.; et al. A Multicenter Randomized Trial of Continuous versus Intermittent β-Lactam Infusion in Severe Sepsis. Am. J. Respir. Crit. Care Med. 2015, 192, 1298–1305. [Google Scholar] [CrossRef]
- Lee, Y.R.; Miller, P.D.; Alzghari, S.K.; Blanco, D.D.; Hager, J.D.; Kuntz, K.S. Continuous Infusion Versus Intermittent Bolus of Beta-Lactams in Critically Ill Patients with Respiratory Infections: A Systematic Review and Meta-analysis. Eur. J. Drug Metab. Pharmacokinet. 2018, 43, 155–170. [Google Scholar] [CrossRef]
- Langgartner, J.; Lehn, N.; Glück, T.; Herzig, H.; Kees, F. Comparison of the pharmacokinetics of piperacillin and sulbactam during intermittent and continuous intravenous infusion. Chemotherapy 2007, 53, 370–377. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Sulaiman, H.; Mat-Nor, M.B.; Rai, V.; Wong, K.K.; Hasan, M.S.; Abd Rahman, A.N.; Jamal, J.A.; Wallis, S.C.; Lipman, J.; et al. Beta-Lactam Infusion in Severe Sepsis (BLISS): A prospective, two-centre, open-labelled randomised controlled trial of continuous versus intermittent beta-lactam infusion in critically ill patients with severe sepsis. Intensive Care Med. 2016, 42, 1535–1545. [Google Scholar] [CrossRef]
- Asín-Prieto, E.; Rodríguez-Gascón, A.; Trocóniz, I.F.; Soraluce, A.; Maynar, J.; Sánchez-Izquierdo, J.Á.; Isla, A. Population pharmacokinetics of piperacillin and tazobactam in critically ill patients undergoing continuous renal replacement therapy: Application to pharmacokinetic/pharmacodynamic analysis. J. Antimicrob. Chemother. 2014, 69, 180–189. [Google Scholar] [CrossRef]
- Bue, M.; Sou, T.; Okkels, A.S.L.; Hanberg, P.; Thorsted, A.; Friberg, L.E.; Andersson, T.L.; Öbrink-Hansen, K.; Christensen, S. Population pharmacokinetics of piperacillin in plasma and subcutaneous tissue in patients on continuous renal replacement therapy. Int. J. Infect. Dis. 2020, 92, 133–140. [Google Scholar] [CrossRef]
- Roberts, D.M.; Liu, X.; Roberts, J.A.; Nair, P.; Cole, L.; Roberts, M.S.; Lipman, J.; Bellomo, R. A multicenter study on the effect of continuous hemodiafiltration intensity on antibiotic pharmacokinetics. Crit. Care 2015, 19, 84. [Google Scholar] [CrossRef]
- Tamme, K.; Oselin, K.; Kipper, K.; Tasa, T.; Metsvaht, T.; Karjagin, J.; Herodes, K.; Kern, H.; Starkopf, J. Pharmacokinetics and pharmacodynamics of piperacillin/tazobactam during high volume haemodiafiltration in patients with septic shock. Acta Anaesthesiol. Scand. 2016, 60, 230–240. [Google Scholar] [CrossRef]
- Ulldemolins, M.; Martín-Loeches, I.; Llauradó-Serra, M.; Fernández, J.; Vaquer, S.; Rodríguez, A.; Pontes, C.; Calvo, G.; Torres, A.; Soy, D. Piperacillin population pharmacokinetics in critically ill patients with multiple organ dysfunction syndrome receiving continuous venovenous haemodiafiltration: Effect of type of dialysis membrane on dosing requirements. J. Antimicrob. Chemother. 2016, 71, 1651–1659. [Google Scholar] [CrossRef]
- Dhaese, S.A.M.; Colin, P.; Willems, H.; Heffernan, A.; Gadeyne, B.; Van Vooren, S.; Depuydt, P.; Hoste, E.; Stove, V.; Verstraete, A.G.; et al. Saturable elimination of piperacillin in critically ill patients: Implications for continuous infusion. Int. J. Antimicrob. Agents 2019, 54, 741–749. [Google Scholar] [CrossRef]
- Udy, A.A.; Lipman, J.; Jarrett, P.; Klein, K.; Wallis, S.C.; Patel, K.; Kirkpatrick, C.M.J.; Kruger, P.S.; Paterson, D.L.; Roberts, M.S.; et al. Are standard doses of piperacillin sufficient for critically ill patients with augmented creatinine clearance? Crit. Care 2015, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Dhaese, S.A.M.; Roberts, J.A.; Carlier, M.; Verstraete, A.G.; Stove, V.; De Waele, J.J. Population pharmacokinetics of continuous infusion of piperacillin in critically ill patients. Int. J. Antimicrob. Agents 2018, 51, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Klastrup, V.; Thorsted, A.; Storgaard, M.; Christensen, S.; Friberg, L.E.; Öbrink-Hansen, K. Population Pharmacokinetics of Piperacillin following Continuous Infusion in Critically Ill Patients and Impact of Renal Function on Target Attainment. Antimicrob. Agents Chemother. 2020, 64, e02556-19. [Google Scholar] [CrossRef] [PubMed]
- Öbrink-Hansen, K.; Juul, R.V.; Storgaard, M.; Thomsen, M.K.; Hardlei, T.F.; Brock, B.; Kreilgaard, M.; Gjedsted, J. Population pharmacokinetics of piperacillin in the early phase of septic shock: Does standard dosing result in therapeutic plasma concentrations? Antimicrob. Agents Chemother. 2015, 59, 7018–7026. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, A.S.; Wallis, S.C.; Jarrett, P.; Starr, T.; Stuart, J.; Lassig-Smith, M.; Mejia, J.L.O.; Roberts, M.S.; Roger, C.; Udy, A.A.; et al. Population pharmacokinetics of piperacillin in nonobese, obese, and morbidly obese critically ill patients. Antimicrob. Agents Chemother. 2017, 61, e01276-16. [Google Scholar] [CrossRef]
- Sukarnjanaset, W.; Jaruratanasirikul, S.; Wattanavijitkul, T. Population pharmacokinetics and pharmacodynamics of piperacillin in critically ill patients during the early phase of sepsis. J. Pharmacokinet. Pharmacodyn. 2019, 46, 251–261. [Google Scholar] [CrossRef]
- Wallenburg, E.; ter Heine, R.; Schouten, J.A.; Raaijmakers, J.; ten Oever, J.; Kolwijck, E.; Burger, D.M.; Pickkers, P.; Frenzel, T.; Brüggemann, R.J.M. An Integral Pharmacokinetic Analysis of Piperacillin and Tazobactam in Plasma and Urine in Critically Ill Patients. Clin. Pharmacokinet. 2022, 61, 907–918, Correction in Clin. Pharmacokinet. 2022, 61, 1325–1329. [Google Scholar] [CrossRef]
- Vinks, A.A.; Den Hollander, J.G.; Overbeek, S.E.; Jelliffe, R.W.; Mouton, J.W. Population pharmacokinetic analysis of nonlinear behavior of piperacillin during intermittent or continuous infusion in patients with cystic fibrosis. Antimicrob. Agents Chemother. 2003, 47, 541–547. [Google Scholar] [CrossRef]
- Felton, T.W.; Hope, W.W.; Lomaestro, B.M.; Butterfield, J.M.; Kwa, A.L.; Drusano, G.L.; Lodise, T.P. Population pharmacokinetics of extended-infusion piperacillin-tazobactam in hospitalized patients with nosocomial infections. Antimicrob. Agents Chemother. 2012, 56, 4087–4094. [Google Scholar] [CrossRef]
- Esteve-Pitarch, E.; Gumucio-Sanguino, V.D.; Cobo-Sacristán, S.; Shaw, E.; Maisterra-Santos, K.; Sabater-Riera, J.; Pérez-Fernandez, X.L.; Rigo-Bonnin, R.; Tubau-Quintano, F.; Carratalà, J.; et al. Continuous Infusion of Piperacillin/Tazobactam and Meropenem in ICU Patients Without Renal Dysfunction: Are Patients at Risk of Underexposure? Eur. J. Drug Metab. Pharmacokinet. 2021, 46, 527–538. [Google Scholar] [CrossRef]
- Landersdorfer, C.B.; Bulitta, J.B.; Kirkpatrick, C.M.J.; Kinzig, M.; Holzgrabe, U.; Drusano, G.L.; Stephan, U.; Sörgel, F. Population pharmacokinetics of piperacillin at two dose levels: Influence of nonlinear pharmacokinetics on the pharmacodynamic profile. Antimicrob. Agents Chemother. 2012, 56, 5715–5723. [Google Scholar] [CrossRef]
- Welling, P.G.; Craig, W.A.; Bundtzen, R.W.; Kwok, F.W.; Gerber, A.U.; Madsen, P.O. Pharmacokinetics of Piperacillin in subjects with various degrees of renal function. Antimicrob. Agents Chemother. 1983, 23, 881–887. [Google Scholar] [CrossRef]
- Baptista, J.P.; Neves, M.; Rodrigues, L.; Teixeira, L.; Pinho, J.; Pimentel, J. Accuracy of the estimation of glomerular filtration rate within a population of critically ill patients. J. Nephrol. 2014, 27, 403–410. [Google Scholar] [CrossRef]
- Palacio-Lacambra, M.E.; Comas-Reixach, I.; Blanco-Grau, A.; Suñé-Negre, J.M.; Segarra-Medrano, A.; Montoro-Ronsano, J.B. Comparison of the Cockcroft–Gault, MDRD and CKD-EPI equations for estimating ganciclovir clearance. Br. J. Clin. Pharmacol. 2018, 84, 2120–2128. [Google Scholar] [CrossRef]
- Abdul-Aziz, M.H.; Alffenaar, J.W.C.; Bassetti, M.; Bracht, H.; Dimopoulos, G.; Marriott, D.; Neely, M.N.; Paiva, J.A.; Pea, F.; Sjovall, F.; et al. Antimicrobial therapeutic drug monitoring in critically ill adult patients: A Position Paper#. Intensive Care Med. 2020, 46, 1127–1153. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Póvoa, P. Antibiotics in critically ill patients: A systematic review of the pharmacokinetics of β-lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef]
- Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.R.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M.; Myburgh, J.; Paterson, D.L.; et al. Continuous infusion of beta-lactam antibiotics in severe sepsis: A multicenter double-blind, randomized controlled trial. Clin. Infect. Dis. 2013, 56, 236–244. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.-H.; Davis, J.S.; Dulhunty, J.M.; Cotta, M.O.; Myburgh, J.; Bellomo, R.; Lipman, J. Continuous versus intermittent beta-lactam infusion in severe sepsis: A meta-analysis of individual patient data from randomized trials. Am. J. Respir. Crit. Care Med. 2016, 194, 681–691. [Google Scholar] [CrossRef]
- Kondo, Y.; Ota, K.; Imura, H.; Hara, N.; Shime, N. Prolonged versus intermittent β-lactam antibiotics intravenous infusion strategy in sepsis or septic shock patients: A systematic review with meta-Analysis and trial sequential analysis of randomized trials. J. Intensive Care 2020, 8, 77. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Voulgaris, G.L.; Maliaros, A.; Samonis, G.; Falagas, M.E. Prolonged versus short-term intravenous infusion of antipseudomonal β-lactams for patients with sepsis: A systematic review and meta-analysis of randomised trials. Lancet Infect. Dis. 2018, 18, 108–120. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Varghese, J.M.; Altukroni, M.; Briscoe, S.; McWhinney, B.C.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Subtherapeutic initial β-lactam concentrations in select critically Ill patients: Association between augmented renal clearance and low trough drug concentrations. Chest 2012, 142, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Huttner, A.; Von Dach, E.; Renzoni, A.; Huttner, B.D.; Affaticati, M.; Pagani, L.; Daali, Y.; Pugin, J.; Karmime, A.; Fathi, M.; et al. Augmented renal clearance, low β-lactam concentrations and clinical outcomes in the critically ill: An observational prospective cohort study. Int. J. Antimicrob. Agents 2015, 45, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Sime, F.B.; Udy, A.A.; Roberts, J.A. Augmented renal clearance in critically ill patients: Etiology, definition and implications for beta-lactam dose optimization. Curr. Opin. Pharmacol. 2015, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Udy, A.A.; Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.R.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M.; Myburgh, J.; et al. Association between augmented renal clearance and clinical outcomes in patients receiving β-lactam antibiotic therapy by continuous or intermittent infusion: A nested cohort study of the BLING-II randomised, placebo-controlled, clinical trial. Int. J. Antimicrob. Agents 2017, 49, 624–630. [Google Scholar] [CrossRef]
- Occhipinti, D.J.; Pendland, S.L.; Schoonover, L.L.; Rypins, E.B.; Danziger, L.H.; Rodvold, K.A. Pharmacokinetics and Pharmacodynamics of Two Multiple-Dose Piperacillin-Tazobactam Regimens. Antimicrob. Agents Chemother. 1997, 41, 2511–2517. [Google Scholar] [CrossRef]
- Zander, J.; Döbbeler, G.; Nagel, D.; Scharf, C.; Huseyn-Zada, M.; Jung, J.; Frey, L.; Vogeser, M.; Zoller, M. Variability of piperacillin concentrations in relation to tazobactam concentrations in critically ill patients. Int. J. Antimicrob. Agents 2016, 48, 435–439. [Google Scholar] [CrossRef]
- Roberts, J.A.; Roberts, M.S.; Robertson, T.A.; Dalley, A.J.; Lipman, J. Piperacillin penetration into tissue of critically ill patients with sepsis-bolus versus continuous administration? Crit. Care Med. 2009, 37, 926–933. [Google Scholar] [CrossRef]
- Rigo-Bonnin, R.; Ribera, A.; Arbiol-Roca, A.; Cobo-Sacristán, S.; Padullés, A.; Murillo, Ò.; Shaw, E.; Granada, R.; Pérez-Fernández, X.L.; Tubau, F.; et al. Development and validation of a measurement procedure based on ultra-high performance liquid chromatography-tandem mass spectrometry for simultaneous measurement of β-lactam antibiotic concentration in human plasma. Clin. Chim. Acta 2017, 468, 215–224. [Google Scholar] [CrossRef]
- Bauer, R. NONMEM User’s Guide; Icon Development Solutions: Ellicot City, MD, USA, 2011. [Google Scholar]
- Jonsson, E.N.; Karlsson, M.O. Xpose-An S-PLUS based population pharmacokinetic/pharmacodynamic model building aid for NONMEM. Comput. Methods Programs Biomed. 1998, 58, 51–64. [Google Scholar] [CrossRef]
- Lindbom, L.; Pihlgren, P.; Jonsson, N. PsN-Toolkit-A collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput. Methods Programs Biomed. 2005, 79, 241–257. [Google Scholar] [CrossRef]
- Phoenix-WinNonlin. 1998–2020. Certara LP. Ver 64 8.3.4. 295. Available online: https://www.certara.com/software/phoenix-winnonlin/ (accessed on 15 January 2023).
- Yamaoka, K.; Nakagawa, T.; Uno, T. Application of Akaike’s information criterion (AIC) in the evaluation of linear pharmacokinetic equations. J. Pharmacokinet. Biopharm. 1978, 6, 165–175. [Google Scholar] [CrossRef]
- Anderson, B.J.; Holford, N.H.G. Mechanistic basis of using body size and maturation to predict clearance in humans. Drug Metab. Pharmacokinet. 2009, 24, 25–36. [Google Scholar] [CrossRef]
- Savic, R.M.; Karlsson, M.O. Importance of shrinkage in empirical bayes estimates for diagnostics: Problems and solutions. AAPS J. 2009, 11, 558–569. [Google Scholar] [CrossRef]
- Efron, B. Bootstrap methods: Another look at the jackknife. Ann. Stat. 1979, 7, 1–26. [Google Scholar] [CrossRef]
- Bergstrand, M.; Hooker, A.C.; Wallin, J.E.; Karlsson, M.O. Prediction-corrected visual predictive checks for diagnosing nonlinear mixed-effects models. AAPS J. 2011, 13, 143–151. [Google Scholar] [CrossRef]
- European Committe on Antimicrobial Susceptibility Testing (EUCAST). 2022. Clinical Breakpoints. Available online: https://www.eucast.org/ (accessed on 15 January 2023).
- Mouton, J.W.; Dudley, M.N.; Cars, O.; Derendorf, H.; Drusano, G.L. Standardization of pharmacokinetic/pharmacodynamic (PK/PD) terminology for anti-infective drugs: An update. J. Antimicrob. Chemother. 2005, 55, 601–607. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value |
|---|---|
| Number of patients, n | 106 |
| Age (years) | 65 (50–72) |
| Males, n (%) | 71 (66.98%) |
| Weight (kg) | 72 (65–84) |
| BMI (kg/m2) | 26.2 (23–29) |
| Caucasian, n (%) CLCRCKD-EPI (mL/min/1.73 m2) | 102 (96.23%) 97.1 (86–114) |
| CLCRCG (mL/min) CLCRMDRD-4 (mL/min/1.73 m2) Albumin (g/L) Neurocritical status, n (%) Drainage carriers, n (%) Ventilated, n (%) Vasoactive drugs, n (%) | 109.4 (84–143) 116.3 (89–146) 29 (26–33) 36 (33.96%) 37 (34.91%) 63 (59.43%) 45 (42.45%) |
| Parameter | Base Model Parameter Estimates (RSE%) [SHR%] | Final Model Parameter Estimates (RSE%) [SHR%] | Median (95% CI) Bootstrap Results a |
|---|---|---|---|
| Pharmacokinetic parameter | |||
| CL (L/h) | 11.9 (7.19) | 12.0 (6.03) × (CLCRCKD-EPI/99.24) | 11.95 (10.36–13.42) |
| Vc (L) | 20.4 (10.00) | 20.7 (8.94) | 20.29 (9.20–25.05) |
| Vp (L) | 65.3 (58.04) | 62.4 (50.80) | 66.32 (15.45–181.76) |
| CLD (L/h) | 5.6 (30.00) | 4.77 (26.4) | 5.16 (3.19–52.05) |
| Between-patient variability | |||
| ω2CL | 0.253 (22.41) [14.60] | 0.190 (24.42) [17.16] | 0.181 (0.103–0.296) |
| Residual variability | |||
| σ2 | 0.148 (15.27) [14.11] | 0.140 (15.7) [13.45] | 0.135 (0.099–0.181) |
| PK/PD Target | CLCRCKD-EPI (mL/min/1.73 m2) | CFR (%) According to Different Daily Dose of Piperacillin in CI (g) | ||||
|---|---|---|---|---|---|---|
| 8 | 12 | 16 | 20 | 24 | ||
| 100% fT>1×MIC | 60–79 | 98.64 | 99.74 | 99.97 | 99.98 | 100.00 |
| 80–99 | 95.77 | 99.02 | 99.74 | 99.93 | 99.98 | |
| 100–119 | 93.11 | 97.89 | 99.33 | 99.82 | 99.91 | |
| 120–139 | 89.52 | 96.33 | 98.74 | 99.55 | 99.79 | |
| 140–159 | 86.10 | 94.42 | 97.83 | 99.17 | 99.61 | |
| 160–179 | 82.67 | 92.22 | 96.65 | 98.48 | 99.26 | |
| 180–200 | 79.28 | 89.93 | 95.15 | 97.68 | 98.83 | |
| 100% fT>4×MIC | 60–79 | 65.80 | 79.23 | 86.45 | 91.10 | 93.87 |
| 80–99 | 51.08 | 70.50 | 80.77 | 87.08 | 91.01 | |
| 100–119 | 40.53 | 61.55 | 73.64 | 80.87 | 85.64 | |
| 120–139 | 30.46 | 53.51 | 67.69 | 76.57 | 81.73 | |
| 140–159 | 22.88 | 45.57 | 61.41 | 71.78 | 77.61 | |
| 160–179 | 17.39 | 38.30 | 55.09 | 66.08 | 73.15 | |
| 180–200 | 13.74 | 31.77 | 48.76 | 60.92 | 68.87 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Casanova, J.; Esteve-Pitarch, E.; Colom-Codina, H.; Gumucio-Sanguino, V.D.; Cobo-Sacristán, S.; Shaw, E.; Maisterra-Santos, K.; Sabater-Riera, J.; Pérez-Fernandez, X.L.; Rigo-Bonnin, R.; et al. Predictive Factors of Piperacillin Exposure and the Impact on Target Attainment after Continuous Infusion Administration to Critically Ill Patients. Antibiotics 2023, 12, 531. https://doi.org/10.3390/antibiotics12030531
Martínez-Casanova J, Esteve-Pitarch E, Colom-Codina H, Gumucio-Sanguino VD, Cobo-Sacristán S, Shaw E, Maisterra-Santos K, Sabater-Riera J, Pérez-Fernandez XL, Rigo-Bonnin R, et al. Predictive Factors of Piperacillin Exposure and the Impact on Target Attainment after Continuous Infusion Administration to Critically Ill Patients. Antibiotics. 2023; 12(3):531. https://doi.org/10.3390/antibiotics12030531
Chicago/Turabian StyleMartínez-Casanova, Javier, Erika Esteve-Pitarch, Helena Colom-Codina, Víctor Daniel Gumucio-Sanguino, Sara Cobo-Sacristán, Evelyn Shaw, Kristel Maisterra-Santos, Joan Sabater-Riera, Xosé L. Pérez-Fernandez, Raül Rigo-Bonnin, and et al. 2023. "Predictive Factors of Piperacillin Exposure and the Impact on Target Attainment after Continuous Infusion Administration to Critically Ill Patients" Antibiotics 12, no. 3: 531. https://doi.org/10.3390/antibiotics12030531
APA StyleMartínez-Casanova, J., Esteve-Pitarch, E., Colom-Codina, H., Gumucio-Sanguino, V. D., Cobo-Sacristán, S., Shaw, E., Maisterra-Santos, K., Sabater-Riera, J., Pérez-Fernandez, X. L., Rigo-Bonnin, R., Tubau-Quintano, F., Carratalà, J., & Padullés-Zamora, A. (2023). Predictive Factors of Piperacillin Exposure and the Impact on Target Attainment after Continuous Infusion Administration to Critically Ill Patients. Antibiotics, 12(3), 531. https://doi.org/10.3390/antibiotics12030531