
Microbial Contamination and Antibiotic Resistance in Marketed Food in Bangladesh: Current Situation and Possible Improvements

 ,
, 
 , , , , , ,
, , , , , ,  and
and 
Abstract
1. Introduction
2. Results
2.1. General Characteristics of Food Vendors and Shops
2.2. Microbial Contamination in Food
2.3. Quantification of Bacteria
2.4. Antimicrobial Resistance
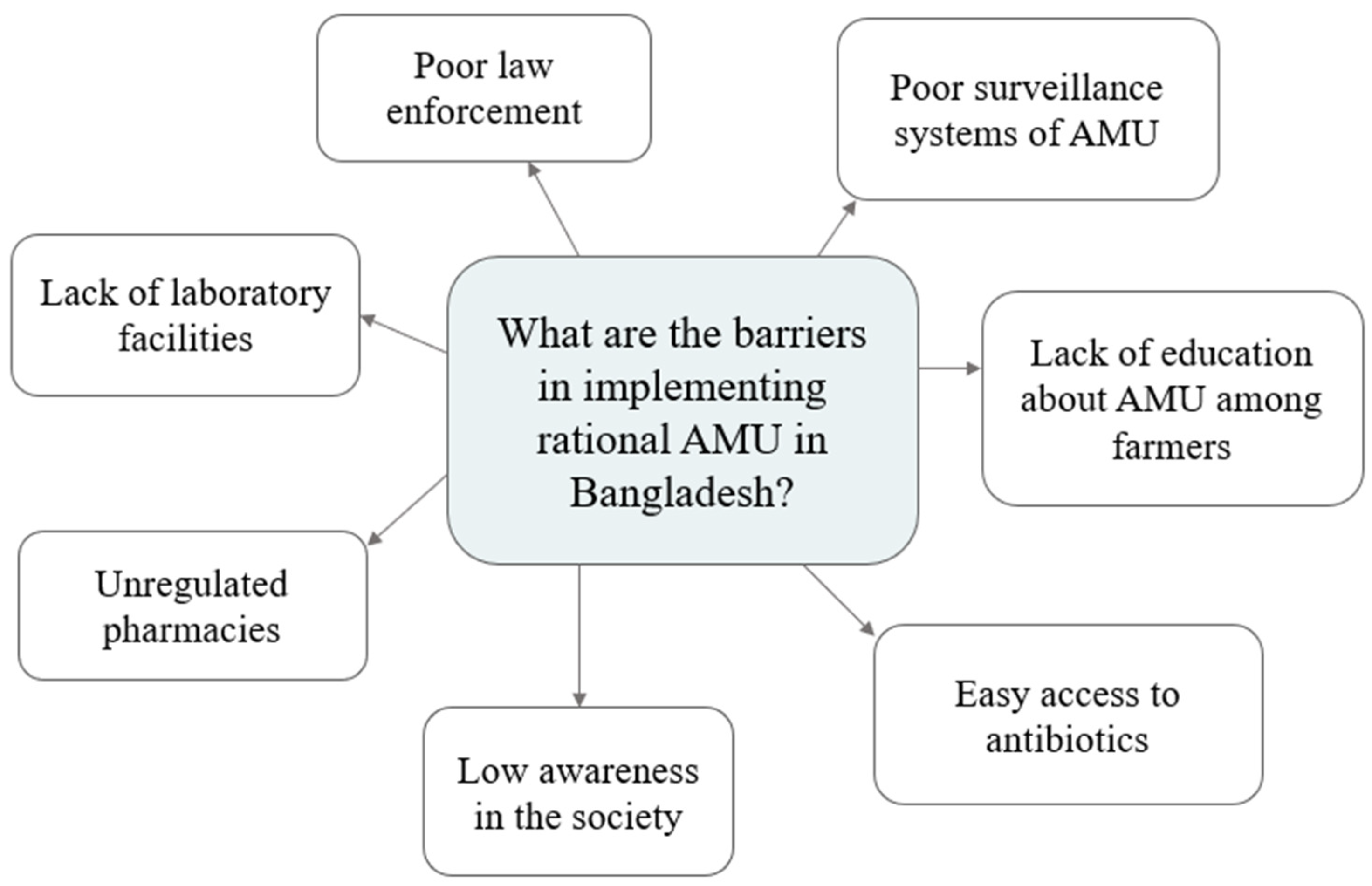
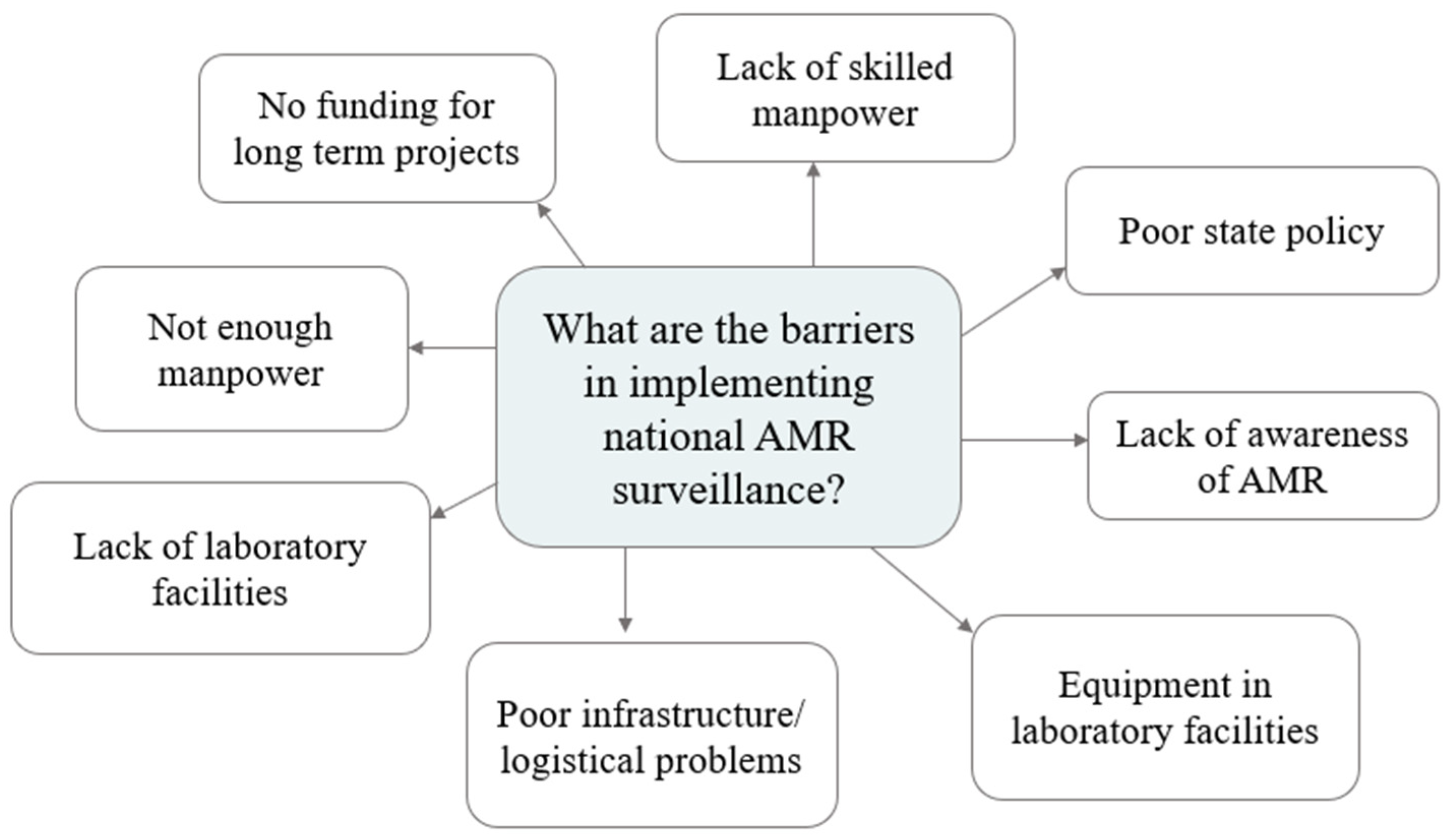
2.5. Qualitative Results on AMU Situation and AMR Prevention in Bangladesh
3. Discussion
4. Materials and Methods
4.1. Study Design and Areas
4.1.1. Study Design
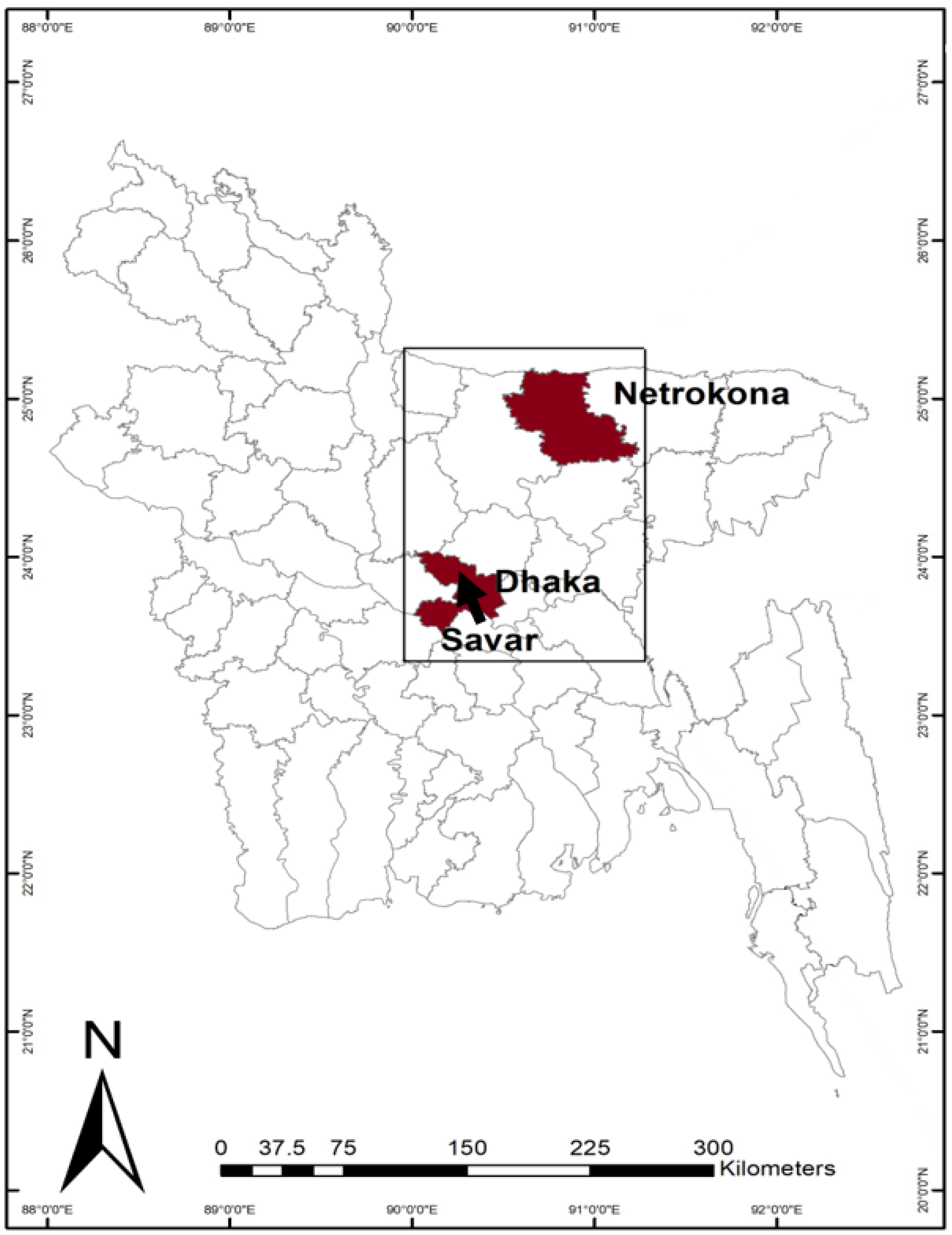
4.1.2. Study Areas
4.2. Sample Collection and Analysis
4.2.1. Sample Collection
4.2.2. Microbial Analysis
4.2.3. Antimicrobial Resistant Analysis
4.2.4. Questionnaires
4.3. Qualitative Interview
4.4. Data Management and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Boeckel, T.P.; Brower, C.; Gilbert, M.; Grenfell, B.T.; Levin, S.A.; Robinson, T.P.; Teillant, A.; Laxminarayan, R. Global trends in antimicrobial use in food animals. Proc. Natl. Acad. Sci. USA 2015, 112, 5649–5654. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S. Antimicrobial resistance: A top ten global public health threat. EClinicalMedicine 2021, 41, 101221. [Google Scholar] [CrossRef]
- Hickman, R.A.; Leangapichart, T.; Lunha, K.; Jiwakanon, J.; Angkititrakul, S.; Magnusson, U.; Sunde, M.; Järhult, J.D. Exploring the Antibiotic Resistance Burden in Livestock, Livestock Handlers and Their Non-Livestock Handling Contacts: A One Health Perspective. Front. Microbiol. 2021, 12, 777. [Google Scholar] [CrossRef] [PubMed]
- Van, T.T.H.; Yidana, Z.; Smooker, P.M.; Coloe, P.J. Antibiotic use in food animals worldwide, with a focus on Africa: Pluses and minuses. J. Glob. Antimicrob. Resist. 2020, 20, 170–177. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hara, G.L.; Gould, I.M.; Goossens, H.; et al. Antibiotic resistance-the need for global solutions. Lancet. Infect. Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef]
- Schmiege, D.; Evers, M.; Kistemann, T.; Falkenberg, T. What drives antibiotic use in the community? A systematic review of determinants in the human outpatient sector. Int. J. Hyg. Environ. Health 2020, 226, 113497. [Google Scholar] [CrossRef] [PubMed]
- Klein, E.Y.; Tseng, K.K.; Pant, S.; Laxminarayan, R.; Eili, D.; Klein, Y. Tracking global trends in the effectiveness of antibiotic therapy using the Drug Resistance Index. BMJ Glob. Heal. 2019, 4, 1315. [Google Scholar] [CrossRef]
- Schmiege, D.; Falkenberg, T.; Moebus, S.; Kistemann, T.; Evers, M. Associations between socio-spatially different urban areas and knowledge, attitudes, practices and antibiotic use: A cross-sectional study in the Ruhr Metropolis, Germany. PLoS ONE 2022, 17, e0265204. [Google Scholar] [CrossRef]
- Islam, K.B.M.S.; Islam, K.B.M.S.; Shiraj-Um-Mahmuda, S.; Hazzaz-Bin-Kabir, M. Antibiotic Usage Patterns in Selected Broiler Farms of Bangladesh and their Public Health Implications. J. Public Health Dev. Ctries. 2016, 2, 276–284. [Google Scholar]
- Chereau, F.; Opatowski, L.; Tourdjman, M.; Vong, S. Risk assessment for antibiotic resistance in South East Asia. BMJ 2017, 358, j3393. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Hardcastle, T.C.; Haque, M.; Lugova, H.; Dhingra, S.; Sharma, P.; Islam, S.; et al. Surveillance of antimicrobial resistance in low- and middle-income countries: A scattered picture. Antimicrob. Resist. Infect. Control 2021, 10, 1–19. [Google Scholar] [CrossRef]
- Sulis, G.; Sayood, S.; Gandra, S. Antimicrobial resistance in low- and middle-income countries: Current status and future directions. Expert Rev. Anti-Infect. Ther. 2022, 20, 147–160. [Google Scholar] [CrossRef] [PubMed]
- Hoque, R.; Ahmed, S.M.; Naher, N.; Islam, M.A.; Rousham, E.K.; Islam, B.Z.; Hassan, S. Tackling antimicrobial resistance in Bangladesh: A scoping review of policy and practice in human, animal and environment sectors. PLoS ONE 2020, 15, e0227947. [Google Scholar] [CrossRef]
- Khan, S.A.; Imtiaz, M.A.; Sayeed, M.A.; Shaikat, A.H.; Hassan, M.M. Antimicrobial resistance pattern in domestic animal—Wildlife—environmental niche via the food chain to humans with a Bangladesh perspective; A systematic review. BMC Vet. Res. 2020, 16, 302. [Google Scholar] [CrossRef]
- Ahmed, I.; Rabbi, M.B.; Sultana, S. Antibiotic resistance in Bangladesh: A systematic review. Int. J. Infect. Dis. 2019, 80, 54–61. [Google Scholar] [CrossRef]
- Rifat, M.A.; Talukdar, I.H.; Lamichhane, N.; Atarodi, V.; Alam, S.S. Food safety knowledge and practices among food handlers in Bangladesh: A systematic review. Food Control 2022, 142, 109262. [Google Scholar] [CrossRef]
- Al Banna, M.H.; Disu, T.R.; Kundu, S.; Ahinkorah, B.O.; Brazendale, K.; Seidu, A.A.; Okyere, J.; Rahman, N.; Mondal, S.; Matubber, B.; et al. Factors associated with food safety knowledge and practices among meat handlers in Bangladesh: A cross-sectional study. Environ. Health Prev. Med. 2021, 26, 1–12. [Google Scholar] [CrossRef]
- Road Map of National Action Plan of ARC. Available online: https://rr-asia.woah.org/wp-content/uploads/2020/03/bangladesh_roadmap.pdf (accessed on 15 November 2022).
- Government of Bangladesh. The National Antimicrobial Resistance (AMR) Surveillance Strategy of Bangladesh 2020–2025. 2020. Available online: https://old.iedcr.gov.bd/website/images/files/AMR/2020-12-16_Final_National%20AMR%20Surveillance%20Strategy.pdf (accessed on 15 November 2022).
- Orubu, E.S.F.; Zaman, M.H.; Rahman, M.T.; Wirtz, V.J. Veterinary antimicrobial resistance containment in Bangladesh: Evaluating the national action plan and scoping the evidence on implementation. J. Glob. Antimicrob. Resist. 2020, 21, 105–115. [Google Scholar] [CrossRef]
- Nahar, P.; Unicomb, L.; Lucas, P.J.; Uddin, M.R.; Islam, M.A.; Nizame, F.A.; Khisa, N.; Akter, S.M.S.; Rousham, E.K. What contributes to inappropriate antibiotic dispensing among qualified and unqualified healthcare providers in Bangladesh? A qualitative study. BMC Health Serv. Res. 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Kalam, M.A.; Rahman, M.S.; Alim, M.A.; Shano, S.; Afrose, S.; Jalal, F.A.; Akter, S.; Khan, S.A.; Islam, M.M.; Uddin, M.B.; et al. Knowledge, Attitudes, and Common Practices of Livestock and Poultry Veterinary Practitioners Regarding the AMU and AMR in Bangladesh. Antibiotics 2022, 11, 80. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Akhtar, Z.; Hassan, M.Z.; Chowdhury, S.; Rashid, M.M.; Aleem, M.A.; Ghosh, P.K.; Mah-E-muneer, S.; Parveen, S.; Ahmmed, M.K.; et al. Pattern of Antibiotic Dispensing at Pharmacies According to the WHO Access, Watch, Reserve (AWaRe) Classification in Bangladesh. Antibiotics 2022, 11, 247. [Google Scholar] [CrossRef] [PubMed]
- Darj, E.; Newaz, M.S.; Zaman, M.H. Pharmacists’ perception of their challenges at work, focusing on antimicrobial resistance: A qualitative study from Bangladesh. Glob. Health Action 2019, 12 (Suppl. 1), 1735126. [Google Scholar] [CrossRef]
- Lucas, P.J.; Uddin, M.R.; Khisa, N.; Salim Akter, S.M.; Unicomb, L.; Nahar, P.; Islam, M.A.; Nizame, F.A.; Rousham, E.K. Pathways to antibiotics in Bangladesh: A qualitative study investigating how and when households access medicine including antibiotics for humans or animals when they are ill. PLoS ONE 2019, 14, e0225270. [Google Scholar] [CrossRef]
- Nigad Nipa, M.; Mohammad Mazumdar, R.; Mahmudul Hasan, M.; Fakruddin, M.; Islam, S.; Bhuiyan, H.R.; Iqbal, A. Prevalence of multi drug resistant bacteria on raw salad vegetables sold in major markets of Chittagong city, Bangladesh. Middle-East J. Sci. Res. 2011, 10, 70–77. [Google Scholar]
- Senderovich, Y.; Izhaki, I.; Halpern, M. Fish as Reservoirs and Vectors of Vibrio cholerae. PLoS ONE 2010, 5, e8607. [Google Scholar] [CrossRef]
- Parvin, I.; Shahid, A.S.M.S.B.; Das, S.; Shahrin, L.; Ackhter, M.M.; Alam, T.; Khan, S.H.; Chisti, M.J.; Clemens, J.D.; Ahmed, T.; et al. Vibrio cholerae O139 persists in Dhaka, Bangladesh since 1993. PLoS Negl. Trop. Dis. 2021, 15, e0009721. [Google Scholar] [CrossRef] [PubMed]
- Azman, A.S.; Lauer, S.A.; Bhuiyan, T.R.; Luquero, F.J.; Leung, D.T.; Hegde, S.T.; Harris, J.B.; Paul, K.K.; Khaton, F.; Ferdous, J.; et al. Vibrio cholerae O1 transmission in Bangladesh: Insights from a nationally representative serosurvey. Lancet Microbe 2020, 1, e336–e343. [Google Scholar] [CrossRef] [PubMed]
- Ayandele, A.A.; Oladipo, E.K.; Oyebisi, O.; Kaka, M.O. Prevalence of Multi-Antibiotic Resistant Escherichia coli and Klebsiella species obtained from a Tertiary Medical Institution in Oyo State, Nigeria. Qatar Med. J. 2020, 2020, 9. [Google Scholar] [CrossRef]
- Chea, R.; Nguyen-Viet, H.; Tum, S.; Unger, F.; Lindahl, J.; Grace, D.; Ty, C.; Koam, S.; Sina, V.; Sokchea, H.; et al. Experimental cross-contamination of chicken salad with Salmonella enterica serovars Typhimurium and London during food preparation in Cambodian households. PLoS ONE 2022, 17, e0270425. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.T.; Lin, Y.T.; Wan, T.W.; Wang, D.Y.; Lin, H.Y.; Lin, C.Y.; Chen, Y.C.; Teng, L.J. Distribution of antibiotic resistance genes among Staphylococcus species isolated from ready-to-eat foods. J. Food Drug Anal. 2019, 27, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Xu, S.; Tang, Z.; Li, Z.; Zhang, L. Use of antimicrobials in food animals and impact of transmission of antimicrobial resistance on humans. Biosaf. Health 2021, 3, 32–38. [Google Scholar] [CrossRef]
- Nelson, D.W.; Moore, J.E.; Rao, J.R. Antimicrobial resistance (AMR): Significance to food quality and safety. Food Qual. Saf. 2019, 3, 15–22. [Google Scholar] [CrossRef]
- Pérez-Rodríguez, F.; Mercanoglu Taban, B. A State-of-Art Review on Multi-Drug Resistant Pathogens in Foods of Animal Origin: Risk Factors and Mitigation Strategies. Front. Microbiol. 2019, 10, 2091. [Google Scholar] [CrossRef] [PubMed]
- Mola, I.; Onibokun, A.; Oranusi, S. Prevalence of multi-drug resistant bacteria associated with foods and drinks in Nigeria (2015–2020): A systematic review. Ital. J. Food Saf. 2021, 10, 9417. [Google Scholar] [CrossRef]
- Rupa, F.A.; Sultana, M.; Inatsu, Y.; Bari, M.L.; Hossain, M.A. Prevalence of Antibiotic Resistant Bacteria on Tomato Surfaces and Effectiveness of Disinfectants in Reducing the Microbial Load. J. Food Sci. Eng. 2012, 2, 293. [Google Scholar]
- Martin, N.H.; Trmcic, A.; Hsieh, T.H.; Boor, K.J.; Wiedmann, M. The Evolving Role of Coliforms As Indicators of Unhygienic Processing Conditions in Dairy Foods. Front. Microbiol. 2016, 7, 1549. [Google Scholar] [CrossRef]
- Feng, P.; Weagant, S.D.; Grant, M.A.; Burkhardt, W. BAM Chapter 4: Enumeration of Escherichia coli and the Coliform Bacteria|FDA. Available online: https://www.fda.gov/food/laboratory-methods-food/bam-chapter-4-enumeration-escherichia-coli-and-coliform-bacteria (accessed on 10 November 2022).
- Hassan, M.M. Scenario of Antibiotic Resistance in Developing Countries. In Antimicrobial Resistance—A One Health Perspective; Mares, M., Lim, S.H.E., Lai, K.-S., Eds.; IntechOpen: London, UK, 2021. [Google Scholar]
- Khan, M.S.; Durrance-Bagale, A.; Legido-Quigley, H.; Mateus, A.; Hasan, R.; Spencer, J.; Hanefeld, J. ‘LMICs as reservoirs of AMR’: A comparative analysis of policy discourse on antimicrobial resistance with reference to Pakistan. Health Policy Plan. 2019, 34, 178–187. [Google Scholar] [CrossRef]
- Onyeaka, H.; Ekwebelem, O.C.; Eze, U.A.; Onwuka, Q.I.; Aleke, J.; Nwaiwu, O.; Chionuma, J.O. Improving Food Safety Culture in Nigeria: A Review of Practical Issues. Foods 2021, 10, 1878. [Google Scholar] [CrossRef]
- Minarini, L.A.D.R.; Andrade, L.N.d.; De Gregorio, E.; Grosso, F.; Naas, T.; Zarrilli, R.; Camargo, I.L.B.C. Editorial: Antimicrobial Resistance as a Global Public Health Problem: How Can We Address It? Front. Public Health 2020, 8, 612844. [Google Scholar] [CrossRef] [PubMed]
- Talebi Bezmin Abadi, A.; Rizvanov, A.A.; Haertlé, T.; Blatt, N.L. World Health Organization Report: Current Crisis of Antibiotic Resistance. Bionanoscience 2019, 9, 778–788. [Google Scholar] [CrossRef]
- Laxminarayan, R. The overlooked pandemic of antimicrobial resistance. Lancet 2022, 399, 606–607. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.; Truman, A.; Wilkinson, B. Antibiotics: Past, present and future. Curr. Opin. Microbiol. 2019, 51, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Fair, R.J.; Tor, Y. Antibiotics and bacterial resistance in the 21st century. Perspect. Medicin. Chem. 2014, 6, 25–64. [Google Scholar] [CrossRef]
- World Health Organization. Worldwide Country Situation Analysis: Response to Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2015; pp. 1–50. [Google Scholar]
- Bangladesh National Parliament Bangladesh Gazette. In Fish Feed and Animal Feed Act; 2010; pp. 2811–2818. Available online: www.bangladeshtradeportal.gov.bd/kcfinder/upload/files/Fish%20Feed%20and%20Animal%20Feed%20Act,%202010.pdf (accessed on 15 November 2022).
- Ministry of Fisheries And Livestock. The Animal Feed Rule; Ministry of Fisheries And Livestock: Dhaka, Bangladesh, 2013. [Google Scholar]
- Directorate General of Drug Administration. DGDA Meeting Minutes 253rd Meeting; Directorate General of Drug Administration: Dhaka, Bangladesh, 2022. [Google Scholar]
- Sharma, G.; Mutua, F.; Deka, R.P.; Shome, R.; Bandyopadhyay, S.; Shome, B.; Goyal Kumar, N.; Grace, D.; Dey, T.K.; Venugopal, N.; et al. A qualitative study on antibiotic use and animal health management in smallholder dairy farms of four regions of India. Infect. Ecol. Epidemiol. 2020, 10, 1792033. [Google Scholar] [CrossRef]
- Chauhan, A.S.; George, M.S.; Chatterjee, P.; Lindahl, J.; Grace, D.; Kakkar, M. The social biography of antibiotic use in smallholder dairy farms in India. Antimicrob. Resist. Infect. Control 2018, 7, 60. [Google Scholar] [CrossRef] [PubMed]
- WHO. Turning Plans into Action for Antimicrobial Resistance (AMR) Working Paper 2.0: Implementation and Coordination; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- ReAct Antibiotic Pollution: India Scores a Global First with Effluent Limits. Available online: https://www.reactgroup.org/news-and-views/news-and-opinions/year-2020/antibiotic-pollution-india-scores-a-global-first-with-effluent-limits/ (accessed on 14 November 2022).
- Pavic, A.; Groves, P.J.; Bailey, G.; Cox, J.M. A validated miniaturized MPN method, based on ISO 6579:2002, for the enumeration of Salmonella from poultry matrices. J. Appl. Microbiol. 2010, 109, 25–34. [Google Scholar] [CrossRef] [PubMed]
- ISO 6579-1:2017; Microbiology of the food chain—Horizontal method for the detection, enumeration and serotyping of Salmonella—Part 1: Detection of Salmonella spp. International Standards Organization: Geneva, Switzerland, 2017.
- ISO 21872-1:2017; Microbiology of the food chain—Horizontal method for the determination of Vibrio spp.—Part 1: Detection of potentially enteropathogenic Vibrio parahaemolyticus, Vibrio cholerae and Vibrio vulnificus 2017. International Standards Organization: Geneva, Switzerlan, 2017.
- ISO 16654:2001; ISO Microbiology of food and animal feeding stuffs—Horizontal method for the detection of Escherichia coli O157. International Standards Organization: Geneva, Switzerland, 2001; Volume 6, pp. 1–20.
- ISO 9308-1:2014; Water quality—Enumeration of Escherichia coli and coliform bacteria—Part 1: Membrane filtration method for waters with low bacterial background flora. International Standards Organization: Geneva, Switzerland, 2014.
- CLSI Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria, 3rd ed.; Document M45; Clinical and Laboratory Standards Institute: Berwyn, PA, USA, 2016.




{kind=link}
{kind=link}
{kind=link}
| Female (%) | Male (%) | Total (%) | |
|---|---|---|---|
| Total number of respondents in each category | 15 (100%) | 838 (100%) | 853 (100%) |
| Age of respondents | |||
| <20 | 1 (6.67%) | 30 (3.58%) | 31 (3.63%) |
| 20–35 | 9 (60.00%) | 420 (50.12%) | 429 (50.29%) |
| 36–50 | 5 (33.33%) | 357 (42.60%) | 362 (42.44%) |
| >51 | 0 | 30 (3.58%) | 30 (3.52%) |
| N/A | 0 | 1 (0.12%) | 1 (0.12%) |
| Highest education completed | |||
| Illiterate | 7 (46.67%) | 192 (22.91%) | 199 (22.51%) |
| Primary | 1 (6.67%) | 325 (38.78%) | 326 (38.22%) |
| Grade 5–10 | 2 (13.33%) | 216 (25.78%) | 218 (25.56%) |
| High school | 0 | 44 (5.25%) | 44 (5.16%) |
| Graduation and above | 5 (33.33%) | 61 (7.28%) | 66 (7.74%) |
| Study site | |||
| Rural | 2 (13.33%) | 250 (29.83%) | 252 (29.54%) |
| Peri-urban | 5 (33.33%) | 250 (29.83%) | 255 (29.89%) |
| Urban | 8 (53.33%) | 338 (40.33%) | 346 (40.56%) |
| Market type | |||
| Supershop | 6 (40%) | 115 (13.72%) | 121 (14.19%) |
| Traditional | 9 (60%) | 723 (86.28%) | 732 (85.81%) |
| Type of product sold | |||
| Chicken | 2 (13.33%) | 315 (37.59%) | 317 (37.16%) |
| Fish | 0 | 213 (25.42%) | 213 (24.97%) |
| Tomato | 13 (86.67%) | 310 (36.99%) | 323 (37.87%) |
| Is the product cooled | |||
| No | 14 (93.33%) | 697 (83.17%) | 711 (83.35%) |
| Yes, unspecified | 0 | 5 (0.60%) | 5 (0.59%) |
| Yes, in cool box | 0 | 52 (6.21%) | 52 (6.10%) |
| Yes, open to the environment but on ice | 1 (6.67%) | 84 (10.02%) | 85 (9.96%) |
| Sample Type and Bacteria | No. of Positive/Total Samples Tested by Areas (%) | |||
|---|---|---|---|---|
| Rural | Peri-Urban | Urban | Overall | |
| Tomato | ||||
| Salmonella spp. | 15/96 (15.63%) | 2/96 (2.08%) | 10 /174 (5.75%) | 27/366 (7.38%) |
| Escherichia coli | 10/96 (10.42%) | 29/96 (30.21%) | 13/174 (7.47%) | 52/366 (14.21%) |
| Chicken | ||||
| Salmonella spp. | 25/95 (26.32%) | 14/94 (14.89%) | 23/170 (13.53%) | 62/359 (17.27%) |
| Fish | ||||
| Escherichia coli | 27/61 (44.26%) | 22/65 (33.85%) | 18/123 (14.63%) | 67/249 (26.91%) |
| Vibrio cholerae | 24/61 (39.34%) | 26/65 (40.00%) | 62/123 (50.41%) | 112/249 (44.98%) |
| Overall | 101/409 (24.69%) | 93/416 (22.36%) | 126/764 (16.49%) | 320/1589 (20.14%) |
| Antibiotic | S | I | R |
|---|---|---|---|
| Amoxicillin + clavulanic acid | ≥18 | 14–17 | ≤13 |
| Cefixime | ≥19 | 16–18 | ≤15 |
| Ceftriaxone | ≥23 | 20–22 | ≤19 |
| Ceftriaxone | ≥18 | 13–17 | ≤12 |
| Erythromycin | ≥23 | 14–22 | ≤13 |
| Gentamicin | ≥15 | 13–14 | ≤12 |
| Streptomycin | ≥15 | 12–14 | ≤11 |
| Penicillin G | ≥29 | - | ≤28 |
| Tetracycline | ≥15 | 12–14 | ≤11 |
| Sulfamethoxazole + trimethoprim | ≥16 | 11–15 | ≤10 |
| Nalidixic acid | ≥19 | 14–18 | ≤13 |
| Tomato | Chicken | Fish | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Salmonella spp. | Escherichia coli | Salmonella spp. | Escherichia coli | Vibrio cholerae | Total | |||||||
| Total isolates | 27 | 51 | 62 | 67 | 112 | 319 | ||||||
| Amoxicillin + Clavulanic acid | 10 | 37.0% | 11 | 21.6% | 23 | 37.1% | 10 | 14.9% | 25 | 22.3% | 79 | 24.8% |
| Cefixime | 0 | 0.0% | 6 | 11.8% | 3 | 4.8% | 14 | 20.9% | 23 | 20.5% | 46 | 14.4% |
| Ceftriaxone | 0 | 0.0% | 4 | 7.8% | 4 | 6.5% | 7 | 10.4% | 24 | 21.4% | 39 | 12.2% |
| Chloramphenicol | 4 | 14.8% | 15 | 29.4% | 13 | 21.0% | 26 | 38.8% | 9 | 8.0% | 67 | 21.0% |
| Erythromycin | 17 | 63.0% | 35 | 68.6% | 54 | 87.1% | 30 | 44.8% | 36 | 32.1% | 172 | 53.9% |
| Gentamicin | 5 | 18.5% | 4 | 7.8% | 13 | 21.0% | 12 | 17.9% | 27 | 24.1% | 61 | 19.1% |
| Streptomycin | 7 | 25.9% | 40 | 78.4% | 33 | 53.2% | 44 | 65.7% | 39 | 34.8% | 163 | 51.1% |
| Penicillin | 20 | 74.1% | 51 | 100.0% | 60 | 96.8% | 67 | 100.0% | 112 | 100.0% | 310 | 97.2% |
| Tetracycline | 17 | 63.0% | 35 | 68.6% | 58 | 93.5% | 46 | 68.7% | 16 | 14.3% | 172 | 53.9% |
| Sulfamethoxazole + Trimethoprim | 8 | 29.6% | 24 | 47.1% | 44 | 71.0% | 34 | 50.7% | 24 | 21.4% | 134 | 42.0% |
| Nalidixic acid | 6 | 22.2% | 14 | 27.5% | 31 | 50.0% | 24 | 35.8% | 25 | 22.3% | 100 | 31.3% |
| Multidrug resistance | 16 | 59.3% | 48 | 94.1% | 59 | 95.2% | 58 | 86.6% | 50 | 44.6% | 231 | 72.4% |
| Positive Samples from Cultivation/Total Samples Analysed | Number MDR of Positive Samples (%) | Prevalence of MDR out of All Samples Analysed (%) | |
|---|---|---|---|
| Tomato | |||
| Salmonella spp. | 27/366 | 16/27 (59.25%) | 16/366 (4.37%) |
| Escherichia coli | 51/366 | 48/51 (94.12%) | 48/366 (13.11%) |
| Chicken | |||
| Salmonella spp. | 62/359 | 59/62 (95.16%) | 59/359 (16.43%) |
| Fish | |||
| Escherichia coli | 67/249 | 58/67 (86.56%) | 58/249 (23.29%) |
| Vibrio cholerae | 112/249 | 50/112 (44.64%) | 50/249 (20.08%) |
| Total | 319/1589 | 231/319 (72.41%) | 231/1589 (14.53%) |
| Isolates | MAR Index < 0.25 | MAR Index 0.26–0.5 | MAR Index 0.6–0.75 | MAR Index > 0.75 | |
|---|---|---|---|---|---|
| Total | 319 | 83 (26.0%) | 144 (45.1%) | 87 (27.3%) | 5 (1.6%) |
| Tomato | |||||
| Salmonella spp. | 27 | 11 (40.7%) | 9 (33.3%) | 7 (25.9%) | 0 |
| Escherichia coli | 51 | 3 (5.8%) | 33 (64.7%) | 15 (29.4%) | 0 |
| Chicken | |||||
| Salmonella spp. | 62 | 3 (4.8%) | 31 (50%) | 25 (40.3%) | 3 (4.8%) |
| Fish | |||||
| Escherichia coli | 67 | 7 (10.4%) | 41 (61.2%) | 19 (28.4%) | 0 |
| Vibrio cholerae | 112 | 59 (52.7%) | 30 (26.8%) | 21 (18.7%) | 2 (1.8%) |
| Food | Fresh Fish | Chicken (Poultry) | Tomato |
|---|---|---|---|
| Approximate amount collected | ~300 g edible portion per vendor | >300 g broiler per vendor | ~150–300 g tomatoes per vendor |
| Sampling procedures | Several smaller fish (if <3–6 cm wide), one whole fish, or small pieces of multiple larger fish | One small whole chicken, or ½ of a larger chicken | 2–4 tomatoes, depending on size |
| Preparing samples at laboratory | Fish meat was collected by cutting at 3 to 4 different sites of the fish collected (approximate total of 50 g); excluding all bone, gills, intestine, and fluid. Fish meat was then cut into small pieces and homogenized before weighing 25 g as sample. | Chicken carcass (whole or a part) was collected by cutting from 3 to 4 different sites of the body (approximate total of 50 g); excluding bone. Chicken meat was then cut into small pieces and homogenized before weighing of 25 g as sample. | Tomato samples were prepared by cutting the tomatoes into small pieces (approximate total of 40–50 g), then and homogenized before weighing of 25 g as sample. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samad, M.A.; Eberson, L.; Begum, R.; Alam, M.G.S.; Talukdar, F.; Akter, R.; Dang-Xuan, S.; Sharma, G.; Islam, S.; Siddiky, N.A.; et al. Microbial Contamination and Antibiotic Resistance in Marketed Food in Bangladesh: Current Situation and Possible Improvements. Antibiotics 2023, 12, 555. https://doi.org/10.3390/antibiotics12030555
Samad MA, Eberson L, Begum R, Alam MGS, Talukdar F, Akter R, Dang-Xuan S, Sharma G, Islam S, Siddiky NA, et al. Microbial Contamination and Antibiotic Resistance in Marketed Food in Bangladesh: Current Situation and Possible Improvements. Antibiotics. 2023; 12(3):555. https://doi.org/10.3390/antibiotics12030555
Chicago/Turabian StyleSamad, Mohammed Abdus, Linnea Eberson, Ruhena Begum, Mohammad Gazi Shah Alam, Faisol Talukdar, Rahima Akter, Sinh Dang-Xuan, Garima Sharma, Shariful Islam, Nure Alam Siddiky, and et al. 2023. "Microbial Contamination and Antibiotic Resistance in Marketed Food in Bangladesh: Current Situation and Possible Improvements" Antibiotics 12, no. 3: 555. https://doi.org/10.3390/antibiotics12030555
APA StyleSamad, M. A., Eberson, L., Begum, R., Alam, M. G. S., Talukdar, F., Akter, R., Dang-Xuan, S., Sharma, G., Islam, S., Siddiky, N. A., Uddin, A. A., Asheak Mahmud, M., Sarker, M. S., Rahman, M. S., Grace, D., & Lindahl, J. F. (2023). Microbial Contamination and Antibiotic Resistance in Marketed Food in Bangladesh: Current Situation and Possible Improvements. Antibiotics, 12(3), 555. https://doi.org/10.3390/antibiotics12030555