

Antibiotic-Loaded Coatings to Reduce Fracture-Related Infections: Retrospective Case Series of Patients with Increased Infectious Risk

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Patients and Trauma Characteristics
2.2. Surgical Treatment
2.3. Outcomes
3. Discussion
4. Materials and Methods
4.1. Methods
- Antibiotic coating based on polylactic acid supplemented with gentamicin, affixed to the surface of the implant at the manufacturing stage. This coating appears to be commercially available only for tibial intramedullary nails (CN—PROtect Expert Tibial Nail, Synthes);
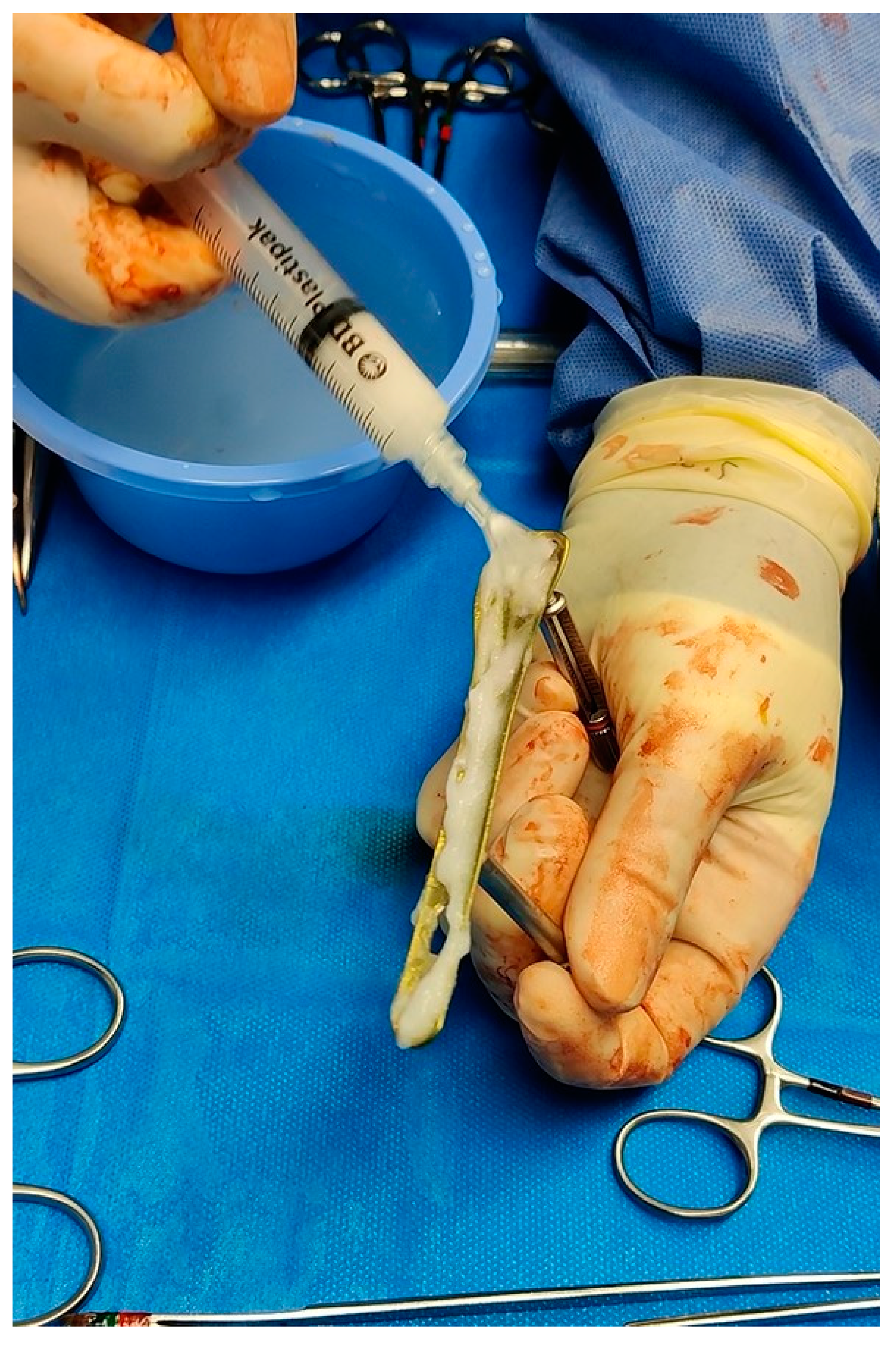
- Polylactic-acid-based rapid resorption hydrogel supplemented with antibiotic of choice, applied to the implant surface directly in the operating room. The antibiotic used in all cases was gentamicin, whether or not associated with vancomycin. Such a device can be applied to all types of implants (ALH—Defensive Antibacterial Coating, Novagenit);
- Both.
- Tibia fractures treated with antibiotic-coated nail (CN);
- Fractures treated with coated implants using ALH;
- At least 12 months of clinical–radiographic follow-up;
- The presence of an increased risk of infection, defined as the presence of one or more of these factors: exposed fractures; polytrauma patients; CCI ≥ 4, in which several known infectious risk factors are assessed (advanced age, obesity, diabetes, hepatopathy, vascular disease, history of smoking, COPD).
- Exclusion criteria were:
- Patients undergoing first implant and/or revision prosthetic replacement with antibiotic cement;
- Presence of surgical site infection, superficial or deep, ongoing or previous;
- Presence of neoplastic diseases with prognosis <6 months;
- Previous diagnosis of immunodepression or immunosuppressive therapy for organ transplantation;
- Known allergy to antibiotics or coating components;
- Pregnancy or expectation of pregnancy during the study period;
- Breastfeeding.
4.2. Surgical Technique and Hydrogel Preparation
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Filipović, U.; Dahmane, R.G.; Ghannouchi, S.; Zore, A.; Bohinc, K. Bacterial Adhesion on Orthopedic Implants. Adv. Colloid Interface Sci. 2020, 283, 102228. [Google Scholar] [CrossRef] [PubMed]
- Walter, N.; Rupp, M.; Lang, S.; Alt, V. The Epidemiology of Fracture-Related Infections in Germany. Sci. Rep. 2021, 11, 10443. [Google Scholar] [CrossRef]
- Ovaska, M.T.; Mäkinen, T.J.; Madanat, R.; Vahlberg, T.; Hirvensalo, E.; Lindahl, J. Predictors of Poor Outcomes Following Deep Infection after Internal Fixation of Ankle Fractures. Injury 2013, 44, 1002–1006. [Google Scholar] [CrossRef] [PubMed]
- Schmidmaier, G.; Lucke, M.; Wildemann, B.; Haas, N.P.; Raschke, M. Prophylaxis and Treatment of Implant-Related Infections by Antibiotic-Coated Implants: A Review. Injury 2006, 37 (Suppl. S2), S105–S112. [Google Scholar] [CrossRef] [PubMed]
- Mauffrey, C.; Herbert, B.; Young, H.; Wilson, M.L.; Hake, M.; Stahel, P.F. The Role of Biofilm on Orthopaedic Implants: The “Holy Grail” of Post-Traumatic Infection Management? Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2016, 42, 411–416. [Google Scholar] [CrossRef]
- Foster, A.L.; Moriarty, T.F.; Zalavras, C.; Morgenstern, M.; Jaiprakash, A.; Crawford, R.; Burch, M.-A.; Boot, W.; Tetsworth, K.; Miclau, T.; et al. The Influence of Biomechanical Stability on Bone Healing and Fracture-Related Infection: The Legacy of Stephan Perren. Injury 2021, 52, 43–52. [Google Scholar] [CrossRef]
- Corrigan, R.A.; Sliepen, J.; Dudareva, M.; IJpma, F.F.A.; Govaert, G.; Atkins, B.L.; Rentenaar, R.; Wouthuyzen-Bakker, M.; McNally, M. Causative Pathogens Do Not Differ between Early, Delayed or Late Fracture-Related Infections. Antibiotics 2022, 11, 943. [Google Scholar] [CrossRef]
- Tan, G.; Xu, J.; Chirume, W.M.; Zhang, J.; Zhang, H.; Hu, X. Antibacterial and Anti-Inflammatory Coating Materials for Orthopedic Implants: A Review. Coatings 2021, 11, 1401. [Google Scholar] [CrossRef]
- Malizos, K.; Blauth, M.; Danita, A.; Capuano, N.; Mezzoprete, R.; Logoluso, N.; Drago, L.; Romanò, C.L. Fast-Resorbable Antibiotic-Loaded Hydrogel Coating to Reduce Post-Surgical Infection after Internal Osteosynthesis: A Multicenter Randomized Controlled Trial. J. Orthop. Traumatol. 2017, 18, 159–169. [Google Scholar] [CrossRef]
- De Meo, D.; Ceccarelli, G.; Iaiani, G.; Lo Torto, F.; Ribuffo, D.; Persiani, P.; Villani, C. Clinical Application of Antibacterial Hydrogel and Coating in Orthopaedic and Traumatology Surgery. Gels Basel Switz. 2021, 7, 126. [Google Scholar] [CrossRef]
- Baertl, S.; Walter, N.; Engelstaedter, U.; Ehrenschwender, M.; Hitzenbichler, F.; Alt, V.; Rupp, M. What Is the Most Effective Empirical Antibiotic Treatment for Early, Delayed, and Late Fracture-Related Infections? Antibiotics 2022, 11, 287. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Boot, W.; Dimas, K.; Malizos, K.; Hänsch, G.M.; Stuyck, J.; Gawlitta, D.; Romanò, C.L. Does Implant Coating with Antibacterial-Loaded Hydrogel Reduce Bacterial Colonization and Biofilm Formation in Vitro? Clin. Orthop. 2014, 472, 3311–3323. [Google Scholar] [CrossRef]
- Giavaresi, G.; Meani, E.; Sartori, M.; Ferrari, A.; Bellini, D.; Sacchetta, A.C.; Meraner, J.; Sambri, A.; Vocale, C.; Sambri, V.; et al. Efficacy of Antibacterial-Loaded Coating in an in Vivo Model of Acutely Highly Contaminated Implant. Int. Orthop. 2014, 38, 1505–1512. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Reul, M.; Nijs, S. The Use of Gentamicin-Coated Nails in Complex Open Tibia Fracture and Revision Cases: A Retrospective Analysis of a Single Centre Case Series and Review of the Literature. Injury 2015, 46, 2433–2437. [Google Scholar] [CrossRef]
- Trentinaglia, M.T.; Van Der Straeten, C.; Morelli, I.; Logoluso, N.; Drago, L.; Romanò, C.L. Economic Evaluation of Antibacterial Coatings on Healthcare Costs in First Year Following Total Joint Arthroplasty. J. Arthroplast. 2018, 33, 1656–1662. [Google Scholar] [CrossRef] [PubMed]
- De Meo, D.; Calogero, V.; Are, L.; Cavallo, A.U.; Persiani, P.; Villani, C. Antibiotic-Loaded Hydrogel Coating to Reduce Early Postsurgical Infections in Aseptic Hip Revision Surgery: A Retrospective, Matched Case-Control Study. Microorganisms 2020, 8, E571. [Google Scholar] [CrossRef]
- De Meo, D.; Cannari, F.M.; Petriello, L.; Persiani, P.; Villani, C. Gentamicin-Coated Tibia Nail in Fractures and Nonunion to Reduce Fracture-Related Infections: A Systematic Review. Mol. Basel Switz. 2020, 25, E5471. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Gustilo, R.B.; Anderson, J.T. Prevention of Infection in the Treatment of One Thousand and Twenty-Five Open Fractures of Long Bones: Retrospective and Prospective Analyses. J. Bone Jt. Surg. Am. 1976, 58, 453–458. [Google Scholar] [CrossRef]
- Wise, B.T.; Connelly, D.; Rocca, M.; Mascarenhas, D.; Huang, Y.; Maceroli, M.A.; Gage, M.J.; Joshi, M.; Castillo, R.C.; O’Toole, R.V. A Predictive Score for Determining Risk of Surgical Site Infection After Orthopaedic Trauma Surgery. J. Orthop. Trauma 2019, 33, 506–513. [Google Scholar] [CrossRef]
- Corona, P.S.; Altayó, M.; Amat, C.; Vicente, M.; Velez, R. Reconstruction of Infected Post-Traumatic Bone Defects of the Distal Femur with the CompressⓇ Implant. Preliminary Results of a Staged Non-Biological Strategy. Injury 2021, 52, 606–615. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.; Fuchs, T.; Jenks, M.; Fleetwood, K.; Franz, D.; Iff, J.; Raschke, M. Systematic Review and Meta-Analysis of the Additional Benefit of Local Prophylactic Antibiotic Therapy for Infection Rates in Open Tibia Fractures Treated with Intramedullary Nailing. Int. Orthop. 2014, 38, 1025–1030. [Google Scholar] [CrossRef]
- Perisano, C.; Greco, T.; Polichetti, C.; Inverso, M.; Maccauro, G. Antibiotic-Coated Nail in Open Tibial Fracture: A Retrospective Case Series. J. Funct. Morphol. Kinesiol. 2021, 6, 97. [Google Scholar] [CrossRef] [PubMed]
- Greco, T.; Cianni, L.; Polichetti, C.; Inverso, M.; Maccauro, G.; Perisano, C. Uncoated vs. Antibiotic-Coated Tibia Nail in Open Diaphyseal Tibial Fracture (42 According to AO Classification): A Single Center Experience. BioMed Res. Int. 2021, 2021, 7421582. [Google Scholar] [CrossRef]
- Walter, N.; Popp, D.; Freigang, V.; Nerlich, M.; Alt, V.; Rupp, M. Treatment of Severely Open Tibial Fractures, Non-Unions, and Fracture-Related Infections with a Gentamicin-Coated Tibial Nail—Clinical Outcomes Including Quality of Life Analysis and Psychological ICD-10-Based Symptom Rating. J. Orthop. Surg. 2021, 16, 270. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.H.; Galanis, A.; Balasubramanian, P.; Iliadis, A.D.; Heidari, N.; Vris, A. A Major Trauma Centre Experience with Gentamicin-Coated Tibial Intramedullary Nails (ETN PROtectTM) in Acute Primary Open Fracture Fixation and Complex Revision Surgery. Eur. J. Orthop. Surg. Traumatol. 2022, 94. [Google Scholar] [CrossRef]
- Franz, D.; Raschke, M.; Giannoudis, P.V.; Leliveld, M.; Metsemakers, W.J.; Verhofstad, M.H.J.; Craig, J.A.; Shore, J.; Smith, A.; Muehlendyck, C.; et al. Use of Antibiotic Coated Intramedullary Nails in Open Tibia Fractures: A European Medical Resource Use and Cost-Effectiveness Analysis. Injury 2021, 52, 1951–1958. [Google Scholar] [CrossRef]
- Badarudeen, S.; Shu, A.C.; Ong, K.L.; Baykal, D.; Lau, E.; Malkani, A.L. Complications After Revision Total Hip Arthroplasty in the Medicare Population. J. Arthroplasty 2017, 32, 1954–1958. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebše, R. The EBJIS Definition of Periprosthetic Joint Infection. Bone Jt. J. 2021, 103-B, 18–25. [Google Scholar] [CrossRef]
- McNally, M.; Govaert, G.; Dudareva, M.; Morgenstern, M.; Metsemakers, W.-J. Definition and Diagnosis of Fracture-Related Infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef]
- Schmolders, J.; Hischebeth, G.T.R.; Friedrich, M.J.; Randau, T.M.; Wimmer, M.D.; Kohlhof, H.; Molitor, E.; Gravius, S. Evidence of MRSE on a Gentamicin and Vancomycin Impregnated Polymethyl-Methacrylate (PMMA) Bone Cement Spacer after Two-Stage Exchange Arthroplasty Due to Periprosthetic Joint Infection of the Knee. BMC Infect. Dis. 2014, 14, 144. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Patients Characteristics | ||
|---|---|---|
| Age | 63.14 ± 24.84 | |
| Gender | Male | 54.05% (20) |
| Female | 45.95% (17) | |
| BMI | 24.86 ± 3.91 | |
| CCI | 3.20 ± 2.77 | |
| Diabetes | 16.21% (6) | |
| Vascular Pathology Smoking History | 8.11% (3) | |
| 18.92% (7) | ||
| COPD | 10.81% (4) | |
| Patients’ Comorbidities (n) | 0 | 46% (17) |
| 1 | 29% (11) | |
| 2 | 11% (4) | |
| ≥3 | 14% (5) | |
| Trauma Characteristics | N (%) | |
|---|---|---|
| Polytrauma | 37.84% (14) | |
| Gustilo–Anderson classification [19] | 35.14% (13) | |
| GA 1 | 30.77% (4) | |
| GA 2 | 38.46% (5) | |
| GA 3a | 15.38% (2) | |
| GA 3b | 7.69% (1) | |
| GA 3c | 7.69% (1) | |
| ASA | 1 | 35.14% (13) |
| 2 | 40.54% (15) | |
| 3 | 21.62% (8) | |
| 4 | 2.70% (1) | |
| Intra/extra articular | ||
| Intraarticular | 43.24% (16) | |
| Extraarticular | 56.76% (21) | |
| Fracture | ||
| Tibia | 32.43% (12) | |
| Periprosthetic | 29.74% (11) | |
| Femur | 24.32% (9) | |
| Pelvis | 5.41% (2) | |
| Humerus | 2.70% (1) | |
| Ulna | 2.70% (1) | |
| Radius | 2.70% (1) | |
| Pre-Op Infection Risk Score [20] | 6.40% | |
| Surgical Treatment Characteristics | N (%) | |
|---|---|---|
| Percutaneous/MIPO Surgery | 21.62% (8) | |
| Graft | ||
| No graft | 91.89% (34) | |
| Autologous | 5.41% (2) | |
| Synthetic | 2.70% (1) | |
| Length of surgery (minutes) | 194.59 ± 76.21 | |
| Implants | ||
| Tibia intramedullary nail | 27.03% (10) | |
| Femoral plate and cerclages | 27.03% (10) | |
| THA | 8.10% (3) | |
| THA + cerclages | 5.41% (2) | |
| THA + plate + cerclages | 5.41% (2) | |
| Tibia and fibula plate and screws | 5.41% (2) | |
| Femoral intramedullary nail | 5.41% (2) | |
| Femoral intramedullary nail + cerclages | 2.70% (1) | |
| Femur plate and screws | 2.70% (1) | |
| Radius plate and screws | 2.70% (1) | |
| Pelvis plate and screws | 2.70% (1) | |
| Shoulder endoprosthesis | 2.70% (1) | |
| Ulna plate and screws | 2.70% (1) | |
| Coating | ||
| Coated nail | 10.81% (4) | |
| Antibiotic-loaded hydrogel | 72.97% (27) | |
| Coated ail + antibiotic-loaded hydrogel | 16.22% (6) | |
| Local antibiotic | ||
| Gentamicin | 72.97% (27) | |
| Gentamicin + vancomycin | 27.03% (10) | |
| Blood transfusions (patients) | 72.97% (27) | |
| Length of stay (days) | 20.24 ± 17.14 | |
| Outcomes | ||
|---|---|---|
| Infection | 2.70% (1) | |
| Other complications | ||
| Delay of consolidation | 2.70% (1) | |
| Aseptic loosening | 2.70% (1) | |
| Time to heal (months) | 7.11 ± 2.71 | |
| SF-12 | ||
| MCS-12 | 47.85 ± 11.71 | |
| PCS-12 | 43.85 ± 10.25 | |
| Follow-up (months) | 34.41 ± 9.46 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Meo, D.; Cera, G.; Pica, R.; Perfetti, F.; Martini, P.; Perciballi, B.; Ceccarelli, G.; Persiani, P.; Villani, C. Antibiotic-Loaded Coatings to Reduce Fracture-Related Infections: Retrospective Case Series of Patients with Increased Infectious Risk. Antibiotics 2023, 12, 287. https://doi.org/10.3390/antibiotics12020287
De Meo D, Cera G, Pica R, Perfetti F, Martini P, Perciballi B, Ceccarelli G, Persiani P, Villani C. Antibiotic-Loaded Coatings to Reduce Fracture-Related Infections: Retrospective Case Series of Patients with Increased Infectious Risk. Antibiotics. 2023; 12(2):287. https://doi.org/10.3390/antibiotics12020287
Chicago/Turabian StyleDe Meo, Daniele, Gianluca Cera, Roberta Pica, Fabiano Perfetti, Paolo Martini, Beatrice Perciballi, Giancarlo Ceccarelli, Pietro Persiani, and Ciro Villani. 2023. "Antibiotic-Loaded Coatings to Reduce Fracture-Related Infections: Retrospective Case Series of Patients with Increased Infectious Risk" Antibiotics 12, no. 2: 287. https://doi.org/10.3390/antibiotics12020287
APA StyleDe Meo, D., Cera, G., Pica, R., Perfetti, F., Martini, P., Perciballi, B., Ceccarelli, G., Persiani, P., & Villani, C. (2023). Antibiotic-Loaded Coatings to Reduce Fracture-Related Infections: Retrospective Case Series of Patients with Increased Infectious Risk. Antibiotics, 12(2), 287. https://doi.org/10.3390/antibiotics12020287