Long-Term Suppressive Therapeutic-Drug-Monitoring-Guided Dalbavancin Therapy for Cardiovascular Prosthetic Infections

 , , , , , ,
, , , , , ,  ,
,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cojutti, P.G.; Tedeschi, S.; Gatti, M.; Zamparini, E.; Meschiari, M.; Siega, P.D.; Mazzitelli, M.; Soavi, L.; Binazzi, R.; Erne, E.M.; et al. Population Pharmacokinetic and Pharmacodynamic Analysis of Dalbavancin for Long-Term Treatment of Subacute and/or Chronic Infectious Diseases: The Major Role of Therapeutic Drug Monitoring. Antibiotics 2022, 11, 996. [Google Scholar] [CrossRef]
- Tobudic, S.; Forstner, C.; Burgmann, H.; Lagler, H.; Steininger, C.; Traby, L.; Vossen, M.G.; Winkler, S.; Thalhammer, F. Real-world experience with dalbavancin therapy in gram-positive skin and soft tissue infection, bone and joint infection. Infection 2019, 47, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Rappo, U.; Dunne, M.W.; Puttagunta, S.; Baldassarre, J.S.; Su, S.; Desai-Krieger, D.; Inoue, M. Epithelial Lining Fluid and Plasma Concentrations of Dalbavancin in Healthy Adults after a Single 1,500-Milligram Infusion. Antimicrob. Agents Chemother. 2019, 63, e01024-19. [Google Scholar] [CrossRef] [PubMed]
- Buckwalter, M.; Dowell, J.A. Population pharmacokinetic analysis of dalbavancin, a novel lipoglycopeptide. J. Clin. Pharmacol. 2005, 45, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Dunne, M.W.; Puttagunta, S.; Sprenger, C.R.; Rubino, C.; Van Wart, S.; Baldassarre, J. Extended-duration dosing and distribution of dalbavancin into bone and articular tissue. Antimicrob. Agents Chemother. 2015, 59, 1849–1855. [Google Scholar] [CrossRef]
- Silva, V.; Miranda, C.; Bezerra, M.; Antão, H.S.; Guimarães, J.; Prada, J.; Pires, I.; Maltez, L.; Pereira, J.E.; Capelo, J.L.; et al. Anti-biofilm activity of dalbavancin against methicillin-resistant Staphylococcus aureus (MRSA) isolated from human bone infection. J. Chemother. 2021, 33, 469–475. [Google Scholar] [CrossRef]
- Dunne, M.W.; Puttagunta, S.; Giordano, P.; Krievins, D.; Zelasky, M.; Baldassarre, J. A Randomized Clinical Trial of Single-Dose Versus Weekly Dalbavancin for Treatment of Acute Bacterial Skin and Skin Structure Infection. Clin. Infect. Dis. 2016, 62, 545–551. [Google Scholar] [CrossRef]
- De Vito, A.; Fiore, V.; Colpani, A.; Zauli, B.; Fanelli, C.; Tiseo, G.; Occhineri, S.; Babudieri, S.; Falcone, M.; Madeddu, G. The current and future off-label uses of dalbavancin: A narrative review. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 1222–1238. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef]
- Fazili, T.; Bansal, E.; Garner, D.; Gomez, M.; Stornelli, N. Dalbavancin as sequential therapy for infective endocarditis due to Gram-positive organisms: A review. Int. J. Antimicrob. Agents 2023, 61, 106749. [Google Scholar] [CrossRef]
- Gatti, M.; Viale, P.; Cojutti, P.G.; Zamparini, E.; De Paolis, M.; Giannella, M.; Pea, F.; Tedeschi, S. A descriptive case series of the relationship between maintenance of conservative PK/PD efficacy thresholds of dalbavancin over time and clinical outcome in long-term treatment of staphylococcal osteoarticular infections. Int. J. Antimicrob. Agents 2023, 61, 106773. [Google Scholar] [CrossRef] [PubMed]
- Cojutti, P.G.; Rinaldi, M.; Gatti, M.; Tedeschi, S.; Viale, P.; Pea, F. Usefulness of therapeutic drug monitoring in estimating the duration of dalbavancin optimal target attainment in staphylococcal osteoarticular infections: A proof-of-concept. Int. J. Antimicrob. Agents 2021, 58, 106445. [Google Scholar] [CrossRef]
- Hidalgo-Tenorio, C.; Sadyrbaeva-Dolgova, S.; Enríquez-Gómez, A.; Muñoz, P.; Plata-Ciezar, A.; Miró, J.M.; Alarcón, A.; Martínez-Marcos, F.J.; Loeches, B.; Escrihuela-Vidal, F.; et al. EN-DALBACEN 2.0 Cohort: Real-life study of dalbavancin as sequential/consolidation therapy in patients with infective endocarditis due to Gram-positive cocci. Int. J. Antimicrob. Agents 2023, 62, 106918. [Google Scholar] [CrossRef] [PubMed]
- Ivanovic, B.; Trifunovic, D.; Matic, S.; Petrovic, J.; Sacic, D.; Tadic, M. Prosthetic valve endocarditis—A trouble or a challenge? J. Cardiol. 2018, 73, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Wilson, W.R.; Bower, T.C.; Creager, M.A.; Amin-Hanjani, S.; O’gara, P.T.; Lockhart, P.B.; Darouiche, R.O.; Ramlawi, B.; Derdeyn, C.P.; Bolger, A.F.; et al. Vascular Graft Infections, Mycotic Aneurysms, and Endovascular Infections: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e412–e460. [Google Scholar] [CrossRef] [PubMed]
- Delgado, V.; Marsan, N.A.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. 2023 ESC Guidelines for the management of endocarditis. Eur. Heart J. 2023, 44, 3948–4042. [Google Scholar] [CrossRef]
- Hitzenbichler, F.; Mohr, A.; Camboni, D.; Simon, M.; Salzberger, B.; Hanses, F. Dalbavancin as long-term suppressive therapy for patients with Gram-positive bacteremia due to an intravascular source—A series of four cases. Infection 2021, 49, 181–186. [Google Scholar] [CrossRef]
- Arrieta-Loitegui, M.; Caro-Teller, J.M.; Ortiz-Pérez, S.; López-Medrano, F.; San Juan-Garrido, R.; Ferrari-Piquero, J.M. Effectiveness, safety and cost analysis of dalbavancin in clinical practice. Eur. J. Hosp. Pharm. 2022, 29, 55–58. [Google Scholar] [CrossRef]
- Suárez, M.; Pérez-Landeiro, A.; Sanjurjo, A.; Lima, O.; Sousa, A.; López, A.; Martínez-Lamas, L.; Cabrera, X.; Rubianes, M.; Pérez-Rodríguez, M.T. Comparison of Dalbavancin with standard of care in the management of infective endocarditis: Efficacy, safety, and cost analysis. Int. J. Infect. Dis. 2023. [Google Scholar] [CrossRef]
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef]
- Frazier, J.D.; Stoudenmire, L.L.; Wagner, J.L.; Thomas, G.M.; Steele, G.M.; Henao-Martínez, A.F.; Franco-Paredes, C.; Chastain, D.B. Dalbavancin vs standard of care for Staphylococcus aureus bacteraemia in patients unable to receive outpatient parenteral antimicrobial therapy. Int. J. Antimicrob. Agents 2023, 62, 106842. [Google Scholar] [CrossRef] [PubMed]
- Senneville, E.; Cuervo, G.; Gregoire, M.; Hidalgo-Tenorio, C.; Jehl, F.; Miro, J.M.; Seaton, A.; Söderquist, B.; Soriano, A.; Thalhammer, F.; et al. Expert Opinion on Dose Regimen and Therapeutic Drug Monitoring for Long-Term Use of Dalbavancin: Expert Review Panel. Int. J. Antimicrob. Agents 2023, 62, 106960. [Google Scholar] [CrossRef] [PubMed]
- Barone, R.; Conti, M.; Cojutti, P.G.; Gatti, M.; Viale, P.; Pea, F. Fast and Simple Liquid Chromatography-Isotope Dilution Tandem Mass Spectrometry Method for Therapeutic Drug Monitoring of Dalbavancin in Long-Term Treatment of Subacute and/or Chronic Infections. Pharmaceutics 2023, 15, 480. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | ||
|---|---|---|
| Variable | Total N = 14 | |
| Demographic characteristics and comorbidities | ||
| Age (years), median IQR | 69.5 | (45–81) |
| Male, n (%) | 11 | (78.6) |
| Charlson Comorbidity Index, median IQR | 5 | (0–10) |
| eGFR (mL/min/1.73 m2), median IQR | 68 | (32–122) |
| Albumin (g/dL), median IQR | 3.55 | (2.8–4.0) |
| Type of infection, n (%) | ||
| Prosthetic valve endocarditis | 8 | (57.1) |
| Prosthetic vascular grafts infections | 7 | (50) |
| Multiple site infection | 4 | (28.6) |
| Cardiac implantable electronic devices infections | 3 | (21.4) |
| Microbiological isolates, n (%) | ||
| Staphylococcus aureus | 5 | (35.7) |
| Methicillin-Sensitive Staphylococcus aureus | 4 | (28.6) |
| Viridans streptococcus | 3 | (21.4) |
| Coagulase-Negative stafilococci | 2 | (14.3) |
| Enterococcus faecalis | 1 | (7.1) |
| Gemella morbillorum | 1 | (7.1) |
| Corynebacterium striatum | 1 | (7.1) |
| Polymicrobial | 1 | (7.1) |
| Unknown | 1 | (7.1) |
| Treatment characteristics | ||
| Antibiotic first regimens, n (%) | ||
| Daptomycin | 4 | (28.6) |
| Ceftriaxone | 4 | (28.6) |
| Oxacillin | 3 | (21.4) |
| Rifampicin | 3 | (21.4) |
| Vancomycin | 2 | (14.3) |
| Doxycycline | 1 | (7.1) |
| Cefazoline | 1 | (7.1) |
| Gentamycin | 1 | (7.1) |
| Cefotaxime | 1 | (7.1) |
| Ampicillin | 1 | (7.1) |
| First line antibiotic median duration (weeks), median IQR | 3 | (1–5) |
| Reason for dalbavancin administration, n (%) | ||
| Facilitate discharge | 11 | (78.6) |
| Adverse events | 2 | (14.3) |
| Poor compliance to therapy | 1 | (7.1) |
| Median duration of dalbavancin therapy (weeks), median IQR | 13 | (5–49) |
| Median duration of dalbavancin therapy for indications, median IQR | ||
| Cardiac implantable electronic devices infections (CEDIs) | 25 | (9–53) |
| Prosthetic vascular grafts infections (PVGI) | 18.5 | (13–46) |
| Prosthetic valve endocarditis (PVEs) | 13 | (7–46) |
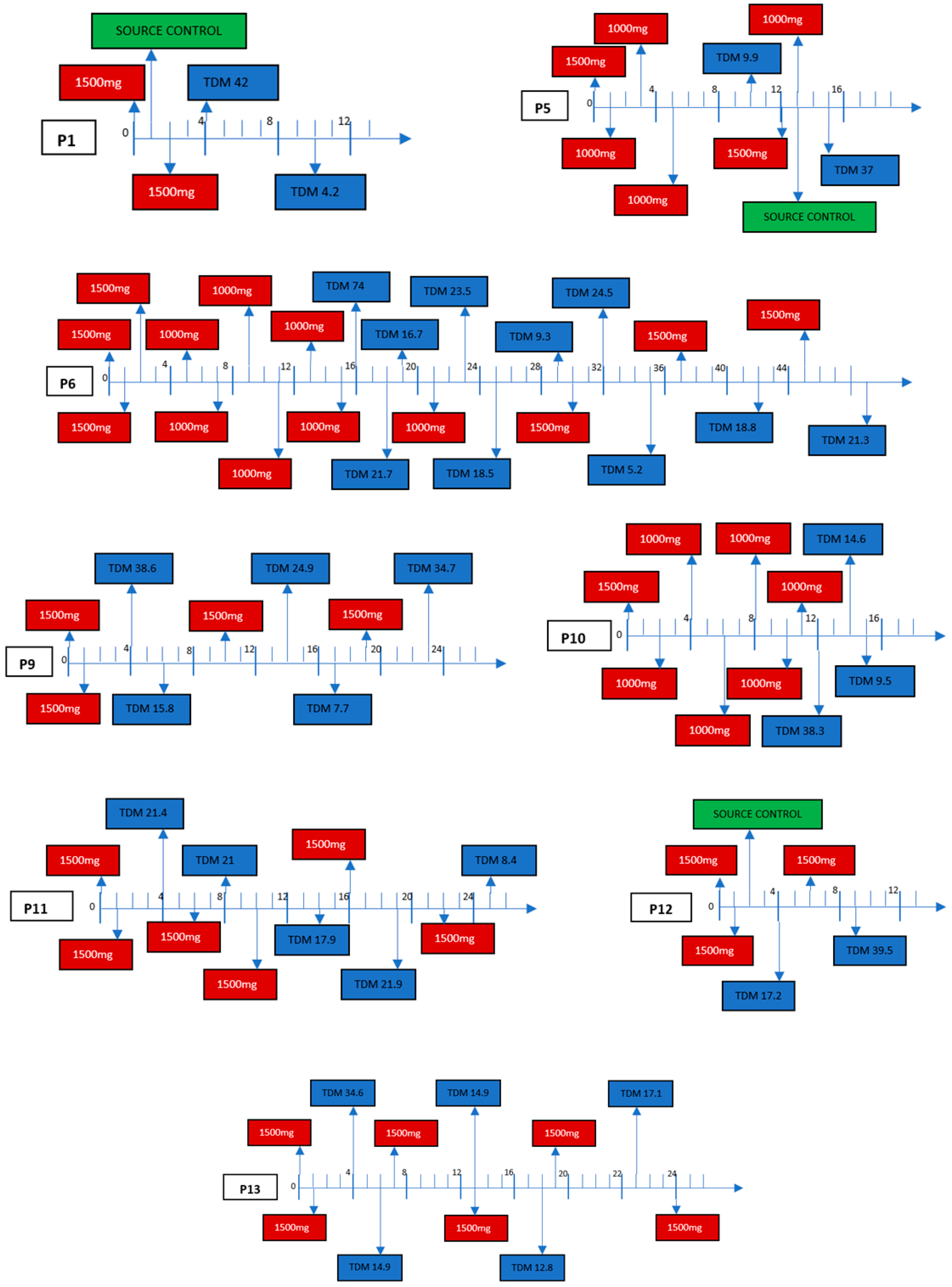
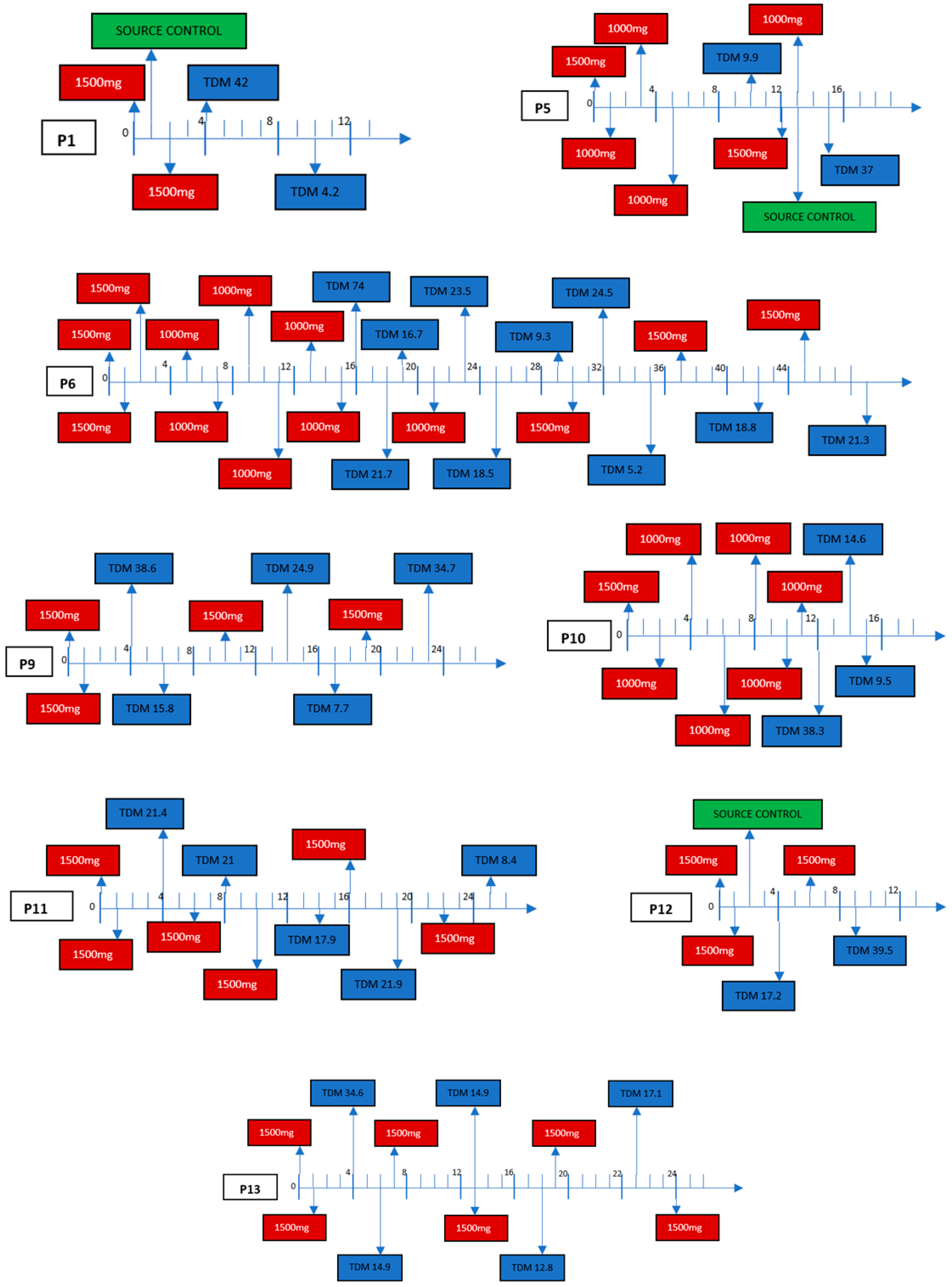
| Dalbavancin dosages and monitoring, n (%) | ||
| TDM | 9/14 | (64.3) |
| Dalbavancin regimens, n (%) | ||
| 1500 mg + 1500 mg, then according TDM | 7 | (50) |
| 1500 mg +1500 mg | 4 | (28.6) |
| 1500 mg + 1500 mg then 1000 mg every 14 d | 3 | (21.4) |
| Clinical outcomes | ||
| Complete source control with implant removal, n (%) | 4/14 | (28.6) |
| Median follow-up (weeks), median IQR | 65 | (23–144) |
| Clinical cure at the EOT (n = 13) | 10/13 | (76.9) |
| Clinical cure at six months of follow-up (n = 12) | 9/12 | (75) |
| Clinical cure in TDM-guided group (n = 8) | 7/8 | (87.5) |
| Microbiological cure at the EOT (n = 13) | 10/13 | (76.9) |
| Microbiological relapse after treatment interruption (n = 13) | 1/13 | (8.3) |
| Clinical cure by dalbavancin indications at the EOT, n (%) | ||
| Prosthetic valve endocarditis (n = 8) | 6/8 | (75) |
| Prosthetic vascular grafts infections (n = 6) | 5/6 | (83.3) |
| Cardiac implantable electronic devices infections (n = 3) | 2/3 | (66.6) |
| Adverse effect reactions | ||
| Rash, n (%) | 1 | (7.1) |
| Impaired renal function, n (%) | 1 | (7.1) |
| Patient | Type of Infection | Aetiology | First Regimen | First Regimen Duration | Dalbavancin Regimen | Dalbavancin Duration | CCI | Prosthetic Removal | TDM | Clinical Success End of Treatment (Total Weeks from Beginning of Antibiotic Therapy) | Clinical Success Six Months Follow-Up | Follow-Up (Weeks) | Death (Weeks from End of Treatment) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 (62 y) | CEDI infection | MSSA | Oxacillin | 3 weeks | 1500 mg + 1500 mg | 6 weeks | 4 | Yes | Yes | Yes (9 w) | Yes | 65 w | No |
| 2 (80 y) | Periprosthetic aortic abscess at the mitro-aortic junction + thoracic aortic endoprosthesis infection in myelofibrosis (PVE + PVGI) | Unknown | Doxycycline + rifampin, then daptomycin + ceftriaxone | 3 weeks | 1500 mg + 1500 mg then 1000 mg every 14 d | 13 weeks | 9 | No | No | No (16 w) | No | - | Yes (47 w) |
| 3 (45 y) | Periprosthetic aortic abscess (PVE) | Gemella morbillorum | Vancomycin + gentamycin then daptomycin + gentamycin | 3 weeks | 1500 mg + 1500 mg | 6 weeks | 1 | Yes | No | Yes (9 w) | Yes | 144 w | No |
| 4 (80 y) | Prosthetic aortic endocarditis (PVE) | Enterococcus faecalis | Ceftriaxone + ampicillin then daptomycin + ceftriaxone | 4 weeks | 1500 mg + 1500 mg | 6 weeks | 7 | No | No | Yes (10 w) | Yes | 46 w | Yes (46 w) |
| 5 (56 y) | Aortic endoprosthesis infection (PVGI) | Staphylococcus capitis | Daptomycin + ceftriaxone then oxacillin + rifampin | 3 weeks | 1500 mg + 1500 mg then 1000 mg every 14 d | 17 weeks | 3 | Yes | Yes | Yes (20 w) | Yes | 78 w | No |
| 6 (50 y) | CEDI infection with peripheric embolization and spondylodiscitis | MSSA | Daptomycin + cefazolin then daptomycin then teicoplanin | 4 weeks | 1500 mg + 1500 mg then 1000 mg every 14 d, then according TDM | 49 weeks | 4 | Partial | Yes | No (53 w) | No | - | No |
| 7 (80 y) | Prosthetic aortic endocarditis with peripheric embolization with stroke, splenic and intestinal infarctions (PVE) | MSSA | Cefazolin + rifampin | 4 weeks | 1500 mg + 1500 mg, missing data concerning timing additional doses | 8 weeks | 10 | No | No | No (12 w) | No | - | Yes (21 w) |
| 8 (69 y) | Prosthetic aortic endocarditis (PVE) | Streptococcus mitis/oralis | Daptomycin + ceftriaxone | 1 week | 1500 mg + 1500 mg | 6 weeks | 7 | No | No | Yes (7 w) | Yes | 91 w | Yes (91 w) |
| 9 (81 y) | Prosthetic aortic endocarditis and CEDI infection, spondylodiscitis (PVE + CEDI infection) | Staphylococcus lugdunensis | Oxacillin | 1 weeks | 1500 mg + 1500 mg then according TDM | 24 weeks | 8 | No | Yes | Yes (25 w) | Yes | 44 w | Yes (44 w) |
| 10 (51 y) | Prosthetic aortic endocarditis with splenic abscess and spondylodiscitis + ascending aorta endoprosthesis infection (PVE + PVGI) | Streptococcus sanguinis | Daptomycin + ceftriaxone then daptomycin + ampicillin | 4 weeks | 1500 mg + 1500 mg then 1000 mg every 14d | 14 weeks | 0 | No | Yes | Yes (18 w) | Yes | 83 w | No |
| 11 (70 y) | Axillo-femoral bypass infection (PVGI) | MRSA | Vancomycin | 3 weeks | 1500 mg + 1500 mg then according TDM | 26 weeks | 5 | No | Yes | Yes (29 w) | Yes | 23 w | No |
| 12 (56 y) | Aortic endoprosthesis infection (PVGI) | MSSA + Acinetobacter baumanniii | Oxacillin + rifampin then association with cotrimoxazole | 3 weeks | 1500 mg + 1500 mg then according TDM | 11 weeks | 3 | Yes | Yes | Yes (14 w) | Yes | 38 w | No |
| 13 (78 y) | Prosthetic aortic endocarditis + ascending aorta endoprosthesis infection (PVE + PVGI) | Sreptococcus pasteurianus | Cefotaxime then ampicillin | 6 weeks | 1500 mg + 1500 mg then according TDM | 41 weeks | 3 | No | Yes | Yes (47 w) | - | - | No |
| 14 (72 y) | Endovascular graft infection (PVGI) | C. striatum | Teicoplanin then linezolid | 5 weeks | 1500 mg + 1500 mg then according TDM | ongoing | 6 | Partial | Yes | - | - | - | No |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gallerani, A.; Gatti, M.; Bedini, A.; Casolari, S.; Orlando, G.; Puzzolante, C.; Franceschini, E.; Menozzi, M.; Santoro, A.; Barp, N.; et al. Long-Term Suppressive Therapeutic-Drug-Monitoring-Guided Dalbavancin Therapy for Cardiovascular Prosthetic Infections. Antibiotics 2023, 12, 1639. https://doi.org/10.3390/antibiotics12111639
Gallerani A, Gatti M, Bedini A, Casolari S, Orlando G, Puzzolante C, Franceschini E, Menozzi M, Santoro A, Barp N, et al. Long-Term Suppressive Therapeutic-Drug-Monitoring-Guided Dalbavancin Therapy for Cardiovascular Prosthetic Infections. Antibiotics. 2023; 12(11):1639. https://doi.org/10.3390/antibiotics12111639
Chicago/Turabian StyleGallerani, Altea, Milo Gatti, Andrea Bedini, Stefania Casolari, Gabriella Orlando, Cinzia Puzzolante, Erica Franceschini, Marianna Menozzi, Antonella Santoro, Nicole Barp, and et al. 2023. "Long-Term Suppressive Therapeutic-Drug-Monitoring-Guided Dalbavancin Therapy for Cardiovascular Prosthetic Infections" Antibiotics 12, no. 11: 1639. https://doi.org/10.3390/antibiotics12111639
APA StyleGallerani, A., Gatti, M., Bedini, A., Casolari, S., Orlando, G., Puzzolante, C., Franceschini, E., Menozzi, M., Santoro, A., Barp, N., Volpi, S., Soffritti, A., Pea, F., Mussini, C., & Meschiari, M. (2023). Long-Term Suppressive Therapeutic-Drug-Monitoring-Guided Dalbavancin Therapy for Cardiovascular Prosthetic Infections. Antibiotics, 12(11), 1639. https://doi.org/10.3390/antibiotics12111639