Abstract
Among the most widespread childhood infections, Helicobacter pylori (H. pylori) develops potentially life-threatening conditions in adults if not appropriately treated. Helicobacter pylori is a common human pathogen that was first described in the stomach many years ago. The discovery of H. pylori was crucial in gastroenterology; this bacterium is associated with chronic gastritis, peptic ulcers, gastric cancer, and lymphoid tissue lymphoma related to the gastric mucosa. Studies published so far estimate that approximately 10% of subjects infected with H. pylori develop a peptic ulcer, and 1–3% of subjects develop gastric cancer. The clinical manifestations are variable and characteristically depend on the individual factors of the host. Various methods of detection and diagnosis of H. pylori infection have been developed, each with advantages, disadvantages, and/or limitations. Available diagnostic tests are usually performed using invasive (endoscopy, biopsy, rapid urease test, cultures, and molecular tests) and noninvasive methods (urea breath test, stool antigen examination, and serological and molecular tests). Although there is extensive accessibility for diagnosing and treating H. pylori infection, the prevalence of antibiotic resistance is not negligible. Thus, numerous studies and meta-analyses are focused on a new orientation of gastroenterologists in diagnosing and treating H. pylori infections. A fascinating perspective hypothesis is the administration of probiotics to reduce H. pylori adhesion to gastric epithelial cells, preventing H. pylori colonization, especially in children, or reinfection with H. pylori in high-risk adult patients.
1. Introduction
Among the most widespread childhood infections, Helicobacter pylori (H. pylori) develops potentially life-threatening conditions in adults if not appropriately treated. H. pylori is a common human pathogen that was first described in the stomach many years ago [1]. In 1983, H. pylori was isolated from the gastric antrum by Marshall and Warren and described as a Gram-negative, flagellated, and microaerophilic bacterium [2]. The discovery of H. pylori is of crucial importance in gastroenterology; this bacterium is associated with chronic gastritis, peptic ulcers, gastric cancer, and lymphoid tissue lymphoma associated with the gastric mucosa [3].
This paper aims to summarize the most recent findings in the treatment and diagnosis of H. pylori infections in adult and pediatric populations. This narrative review presents data on prevalence, clinical manifestations, diagnostic methods, and the most recent treatment regimens. Through this paper, we aim to fix the gaps in the current literature and raise the alarm among adult and pediatric patients who require correct treatment in order not to develop complications in adult life.
It is essential to understand that antibiotic regimens have increased antibiotic resistance tremendously, and therefore, often, the proper treatment for H. pylori infection can be a challenge for the doctor.
2. Prevalence and Mode of Transmission
Various studies over time have shown that the prevalence of H. pylori infection varies according to age, geographic area, and socioeconomic status [4].
Population studies suggest that at least 50% of people are infected with H. pylori.
Oral–oral is the main route of transmission of H. pylori, explaining the incidence of infection among members of the same family [5]. Fecal–oral transmission is the second route of infection described after exposure to contaminated water, mainly due to poor sanitation conditions [6].
For this reason, it is essential to evidentiate that improving socioeconomic status and living conditions dramatically influence the reduction of the prevalence of H. pylori infection [7].
3. Pathogenesis
H. pylori is a mobile, microaerophilic, Gram-negative, rod-shaped bacterium capable of colonizing the acid environment existing in the stomach. In most cases, H. pylori infection is contracted in childhood. It is estimated that 30% of the young population is or will become infected with H. pylori at some point during their lifetime. The interactions between the pathogen agent’s virulence factors and the host’s immune response seem crucial in developing the pathologies associated with this infection, such as gastritis, peptic ulcers, or gastric cancer (Figure 1). Studies published so far estimate that approximately 10% of subjects infected with H. pylori develop peptic ulcers, and 1%-3% of subjects develop gastric cancer [8,9].
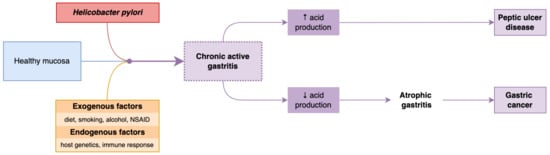
Figure 1.
Physiopathology of H. pylori infection.
Inside the stomach, H. pylori produces urease, which favors the hydrolysis of urea with the generation of carbon dioxide and ammonia. Ammonia neutralizes gastric acid, and carbon dioxide prevents bacteria’s survival in the stomach by raising the acidity of the medium. H. pylori, due to its helical shape and flagellar movements, penetrates the mucus layer and gastric epithelium, and secondarily, the epithelial cells, determined by a synergic action of adhesins and membrane proteins, subsequently triggering an inflammatory response in the host cells. Gastric intestinal metaplasia, peptic ulcers, chronic atrophic gastritis, gastric cancer, and lymphoid tissue lymphomas (MALT) [10] were complications that led the World Health Organization (WHO) to classify H. pylori as one of the carcinogenic agents of class 1 [11]. Previous studies have concentrated mainly on the role of H. pylori in developing inflammations and gastric cancer and demonstrated that eradicating H. pylori can reduce the incidence of gastric cancer [12] and atrophic gastritis [13]. The guidelines regarding the management of precancerous epithelial diseases (MAPS II) in 2019 [14] recommended, as primary objectives, the prevention of H. pylori infection, considering its proven role in the process of gastric carcinogenesis, as well as the eradication of H. pylori in patients with known gastric or intestinal metaplasia and chronic atrophic gastritis.
4. Clinical Manifestations and Diagnosis
According to the pathogenic mechanisms, H. pylori-positive subjects can present various clinical manifestations [15]. The clinical manifestations are variable and characteristically depend on the individual factors of the host, as the type of initial damage to the gastric mucosa is correlated with the progression of various gastric diseases. The predominant development of antral gastritis is associated with the appearance of a peptic ulcer. In contrast, corpus gastritis and multifocal atrophy correlate with gastric ulcers, gastric atrophy, intestinal metaplasia, and gastric carcinomas [16] (Figure 2). The most frequent clinical manifestations in medical practice are chronic gastritis and peptic ulcers; for this reason, detecting and eradicating the infection are essential steps in managing these conditions [17].
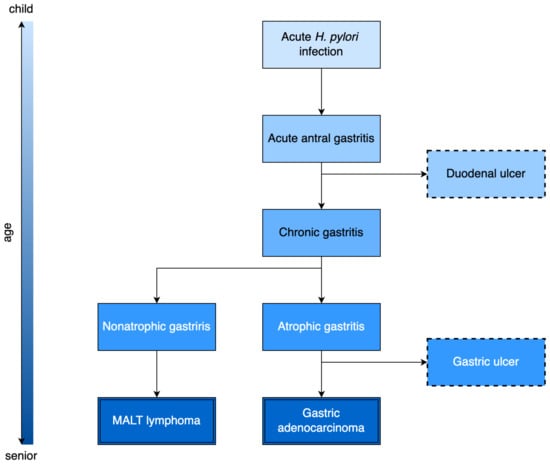
Figure 2.
Timeline of clinical manifestations in patients infected with H. pylori.
Recent studies have associated H. pylori infection with a comprehensive pathology of extra digestive effects, with the condition being related to allergic, neurological, dermatological, ocular, hematological, cardiovascular, and metabolic diseases, a fact that amplified the detection and eradication importance [18].
5. Diagnostic Methods in H. pylori Infection
Various methods of detecting H. pylori infection have been developed, each with advantages, disadvantages, and/or limitations. The first choice depends both on the availability and accessibility of the laboratories and the clinical conditions of the patients. Additionally, available diagnostic tests that are usually performed include invasive (endoscopic) and noninvasive methods. Non-invasive diagnostic tests are represented by the urea breath test, stool antigen examination, and serological and molecular tests. Invasive tests include an endoscopy, a biopsy, a rapid urease test, cultures, and molecular tests [19].
5.1. Noninvasive Diagnostic Tests
5.1.1. Urea Breath Test
The urea breath test (UBT) was the first method of diagnosis and still represents the most popular noninvasive test for diagnosing H. pylori infection. UBT presents multiple advantages in detecting H. pylori infection, especially in children and teenagers, being a simple, non-invasive, and reliable method, with a sensitivity and specificity of 75% to 100% [20].
A recently published meta-analysis evaluating the diagnostic accuracy of H. pylori infection using UBT in adult patients with specific dyspeptic symptoms revealed a sensitivity of 96% and a common specificity of 93% [21].
UBT is also helpful for epidemiological studies and for evaluating eradication therapy efficiency [16].
5.1.2. Stool Antigen Test
The stool antigen test (SAT) is a noninvasive method with remarkable sensitivity and specificity, 94% to 97%, used to diagnose H. pylori infection [22].
Also used to confirm eradication after anti-infective therapy, the cumulative sensitivity and specificity for the monoclonal SAT were 93% and 96%, respectively, according to data published in global meta-analyses [22].
The accuracy of the stool antigen diagnosis is influenced by factors such as the use of antibiotics, PPI, or other drugs such as N-acetylcysteine, and the coexistence of complications such as upper digestive hemorrhage. Before testing, sample preservation, temperature, and transport time can influence the diagnostic accuracy of the SAT [23,24].
5.1.3. Serological Tests
Currently, numerous serological tests are available based on the detection of anti-H. pylori IgG antibodies; the EIA test is the most used. Serological tests are frequently used in the screening of epidemiological studies due to their acceptability for patients, prompt result, and inexpensive cost.
The accuracy of serological tests is not affected by digestive hemorrhaging, gastric atrophy, antibiotics, or PPIs, which cause false negative results in other methods.
The disadvantage of serological tests is the impossibility of evaluating the efficacy of the eradication therapy because the levels of anti-H. pylori antibodies can persist in the blood for a long time, even after the eradication of the infection. Antibody-based tests do not distinguish between active infection and previous exposure to H. pylori, so further confirmation is required before the initiation of eradication therapy [16].
The determination of H. pylori antibodies has a decisive role in studies related to the pathogenesis of the infection and the assessment of virulence factors because specific antigenic proteins can be detected via immunological techniques, thus conferring an additional diagnostic value. Potential biomarkers have been tested to identify subjects infected with H. pylori strains with a high risk of developing complications and assess the prognosis of diseases associated with H. pylori infection.
Thereby, in patients affected by H. pylori, the detection of serum CagA, VacA, and GroEL antibodies was correlated with the development of gastric precancerous lesions and even gastric cancer, making these serum markers potential predictive factors for patients infected with high-risk strains [25,26].
5.1.4. Polymerase Chain Reaction
A PCR test detects H pylori in stool and is a reliable and fast technique that offers the advantage of identifying specific genotypes, with a possible role in determining the antibiotic resistance of bacteria [27,28].
The detection of infection through PCR in the oral cavity uses H. pylori-specific primer sets based on specific complete genome sequences of 48 H. pylori strains, increasing the diagnostic accuracy [29].
5.2. Invasive Tests
5.2.1. Endoscopy
Conventional endoscopic examination is routinely performed to evaluate lesions associated with H. pylori (chronic atrophic gastritis, peptic ulcers, MALT lymphomas, and gastric cancer). Endoscopy is also used for taking biopsy samples from the gastric mucosa for further determinations, such as rapid urease tests, histopathological examinations, cultures, and molecular methods. The biopsy is preferably performed from the gastric antrum.
Chromoendoscopy with phenol red is a method used for detecting H. pylori infection due to the specific urease activity of the bacterium, but its sensitivity (73–81%) and specificity (76–81%) are low [30,31].
Confocal laser endomicroscopy (CLE) represents an endoscopic method that allows the histological examination of the gastric mucosa. Characteristic for the positive diagnosis of H. pylori infection is the presence, at laser confocal endomicroscopy, of white spots, neutrophils, and sometimes micro-abscesses. The accuracy, sensitivity, and specificity of this method have been evaluated in various studies at 92.8%, 89.2%, and 95.7%, respectively [32].
5.2.2. Histological Examination
The histological examination is the gold standard for diagnosing H. pylori infection. The examiner’s experience influences the accuracy of the diagnosis, size, site, number of biopsies, and staining procedures, as well as the use of inhibitors of the proton pump (PPI) and antibiotics.
5.2.3. The Rapid Test with Urease
The rapid urease test (RUT) is considered the most useful invasive test in the diagnosis of H. pylori infection because it is quickly available, not expensive, easy to perform, and, in particular, has a sensitivity of over 85–95% and a specificity between 95% and 100%, with increased accuracy with the number of gastric biopsies [33].
5.2.4. Microbiological Culture
The cultivation of H. pylori from the gastric biopsy sample is a diagnostic method with a specificity of approximately 100% but less sensitivity, with variability between 85% and 95%. Culturing allows the isolation of H. pylori for subsequent phenotypic and genotypic characterization, with a role in the efficiency of the therapeutic scheme. The cultivation of H. pylori provides the ability to manage and assess antibiotic resistance in extensive observational studies [16].
5.2.5. Polymerase Chain Reaction
PCR is widely used to detect H. pylori infection from gastric biopsy samples, saliva, and stool. Compared to conventional tests, PCR offers a sensitivity and specificity above 95%. PCR provides information on H. pylori’s virulence factors by detecting specific mutations that determine antibiotic resistance, such as resistance to macrolides and fluoroquinolones [34,35].
6. Therapeutic Management
Currently, it is considered appropriate to detect and treat the infection in the following categories of patients:
Patients diagnosed with intestinal metaplasia, MALT lymphoma, gastric atrophy, or early gastric cancer; elderly patients with dyspeptic syndrome or with suspicious lesions described at endoscopy; young symptomatic patients diagnosed through non-invasive tests; chronic users of NSAIDs or anticoagulants, especially those with a history of gastritis or peptic ulcers; patients diagnosed with iron deficiency anemia, a deficit of the B12 vitamin, or idiopathic thrombocytopenic purpura.
According to recent studies, a comprehensive approach toward H. pylori testing and treatment policies is recommended, including tests for family members of infected patients and high-risk populations (i.e., immigrants from countries with a high prevalence of infection), especially in countries where there is an increased rate of gastric cancer and where screening programs have been developed for the entire population. The ideal methods of diagnosis, the need for cultures and an antibiogram before prescribing the treatment, and the confirmation of eradication still need to be elucidated, requiring extensive additional studies.
Most therapeutic regimens are recommended empirically, with no data on the resistance to specific classes of antibiotics. According to the latest recommendations, the optimal treatment for H. pylori infection might have an eradication rate of at least 90% [36].
The published data describe different concepts of medical practices in different regions of Europe, with consequent heterogeneous results: seven-day regimens are very common in South-East Europe (60%) and less frequently used in South-West Europe (1.7%). An observation was made regarding triple therapy: it is very rarely prescribed in Central and South-West Europe and much more frequently in East, South-East, and North Europe.
H. pylori treatment uses a combination of antimicrobial and antisecretory agents (Figure 3). To achieve the bactericidal effect of antimicrobial agents, it is necessary to increase the gastric pH, which is provided by administering an antisecretory treatment. Probiotics are used as adjunctive therapy to eradicate H. pylori, although their pathogenic mechanism is unclear [37].
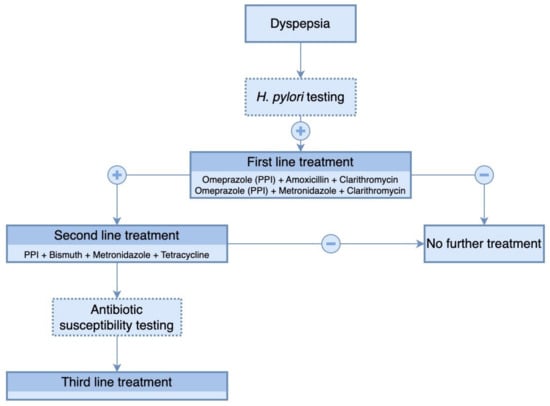
Figure 3.
Therapeutic algorithm for eradication of H. pylori infection.
As resistance against single antibiotic therapy develops rapidly, a combination of several antibiotics is recommended [38].
Triple therapy, including clarithromycin and amoxicillin, was the most frequently used regimen, with eradication rates below 86%. Among all antibiotic regimens prescribed, only concomitant therapy with clarithromycin, amoxicillin, and metronidazole achieved a 90% eradication rate. In regions where bismuth salt was used in quadruple therapy, eradication rates were highest, exceeding 90%.
Thus, according to the most recent published data [37], quadruple therapy is recommended, being the only one that achieves an eradication rate of approximately 90%:
Quadruple treatment with PPIs, amoxicillin, clarithromycin, and metronidazole, for 14 days.
Triple therapy plus bismuth salt: PPI, bismuth salt, amoxicillin, and clarithromycin, for 14 days.
Bismuth quadruple therapy: PPI, bismuth salt, tetracycline, and metronidazole, for 10 days.
If the first line of treatment fails, the Maastricht Consensus V recommends rescue therapy with PPIs, amoxicillin plus quinolone (levofloxacin or moxifloxacin), for 10–14 days.
If the second line of treatment also fails, cultures with antibiotic susceptibility tests or molecular determinations are recommended [16].
6.1. Antibiotic Resistance of H. pylori
Currently, drug resistance of H. pylori is associated with antibiotic resistance included in eradication regimens (clarithromycin, metronidazole, amoxicillin, fluoroquinolones, and tetracycline). The mechanism of antibiotic resistance refers to structural changes in the gene sequence. Intracellular drug activation is inhibited, with subsequent enzymatic deactivation.
The efficacy of antibiotic administration is reduced in the acidic environment of the stomach, a fact also explained by the thickness of the gastric mucosa of approximately 200 μm, which leads to a decrease in the eradication rate.
This describes the capacity of H. pylori to form biofilms composed of bacteria and an extracellular matrix, self-secreted, that adhere to various surfaces. Biofilms increase the antibiotic resistance of H. pylori by creating a barrier that reduces the penetration of the antibiotic, the promotion of gene mutation, and the overexpression of the efflux pumps involved in drug resistance. The extracellular matrix also creates an effective but non-specific barrier that does not allow antibiotic penetration, favoring efflux pumps’ overexpression. This encapsulation of H. pylori causes a significant increase in its viability. Considering these particular aspects of H. pylori’s ability to develop microfilms that can increase antibiotic resistance, it becomes imperative to investigate alternatives to improve the efficiency of drug administration, annihilate virulence factors, and implicitly contribute to eradicating the infection [39,40,41].
According to the data available in the literature, the resistance of H. pylori to the classes of antibiotics used is different depending on the geographical area and the national health programs, giving results that tend to be uniform at the global level and an increase in antibiotic resistance for H. pylori regardless of local socio-economic status. Triple therapy regimens (with clarithromycin and amoxicillin) are most commonly prescribed. However, they have a failure rate estimated at over 20–30% of patients, a failure that appears due to an increasing resistance to clarithromycin.
Quadruple therapy regimens without bismuth (PPI, amoxicillin, clarithromycin, and metronidazole) have been recommended with improved eradication rates, with the mention that this regimen is not as effective in the case of double resistance of both metronidazole and clarithromycin. Available literature estimates that over the last 20 years, clarithromycin resistance has increased yearly by 3.7% [42].
Associating bismuth with therapeutic regimens is beneficial, especially in areas with increased antibiotic resistance. Bismuth has a solid bacteriostatic effect with prominent synergic benefits in various therapies when combined with several antibiotics. Bismuth is most associated with the quadruple therapy regimen, along with PPIs, tetracycline, and metronidazole. The association of bismuth with triple therapy regimens also improved H. pylori infection eradication rates [15].
The excessive use of macrolides in treating respiratory infections (azithromycin, erythromycin) and cross-resistance between antibiotics may be responsible for the increase in microbial resistance to clarithromycin observed in more and more geographical areas in cohort studies [3].
Consequently, various therapeutic regimens have been used to treat H. pylori. In geographical areas with high resistance to clarithromycin, the combination of metronidazole concurrently with PPIs, clarithromycin, and amoxicillin twice a day (a quadruple therapy regimen) increases the efficacy of the treatment, with an eradication rate of over 90% [43]. Clarithromycin can be replaced by levofloxacin (250/500 mg) in triple therapy regions, with clarithromycin resistance above 15–20% and quinolone resistance below 10%, therapy will increase the eradication rate [44,45]. The frequent, exhaustive, and sometimes incorrect use of antibiotics influenced the selection of multi-resistant germs. Macrolides and fluoroquinolones, used to eradicate H. pylori, are also widely used in other infectious pathologies; prescribing them should be performed judiciously. For example, the increasing prescription of quinolones in urinary tract infections has increased Escherichia coli resistance, leading to the emergence of multidrug-resistant species [46].
6.2. Probiotics
A new approach to H. pylori therapy is the association of probiotics, based on multiple clinical studies focused on an association that has become imperative, mainly due to the increase in antibiotic resistance. Probiotics are live microbial species with anti-inflammatory and antioxidant characteristics that can improve the intestinal microbiome, antagonize the action of pathogens, and modulate the immune status [47]. Frequently used probiotic bacteria are Lactobacillus and Bifidobacterium species [48].
According to the studies carried out by Kim et al., the prescription of probiotics for H. pylori infection increases the eradication and reduces the side effects of classical antimicrobial therapy. A common characteristic of these bacteria is their capacity of the anaerobic digestion of carbohydrates and the production of lactic acid. These microorganisms have an increased resistance to low gastric pH and a tolerance to wide temperature variations [49].
Previous studies focused on the significance of probiotics (Lactobacillus, Saccharomyces boulardii, or Bacillus clausii) in improving side effects associated with H. pylori eradication therapy [50,51,52,53,54,55,56,57,58].
The benefits of probiotic therapy in H. pylori infection are an increased eradication rate and improved treatment compliance by preventing associated side effects [55].
Several factors, such as the type of H. pylori strain, the extent of the inflammation, and the density of H. pylori colonization, determine the clinical impact of H. pylori infection. The risk of peptic ulcers and gastric cancer increases with the extent of the infection. For this reason, the effort to eradicate H. pylori will decrease the risk of diseases associated with H. pylori infection, justifying the association of probiotics with classical therapies [59,60].
6.3. Mechanism of Action of Probiotics
6.3.1. Non-Immunological Mechanism
The acidic pH of the stomach is the first line of defense against pathogenic bacteria that penetrate the gastric mucosal barrier. The administration of probiotics amplifies this protection, thanks to the generation of antimicrobial substances that compete with H. pylori for adhesion receptors, increasing mucin production and stabilizing the gastric mucosa barrier [61] (Figure 4).
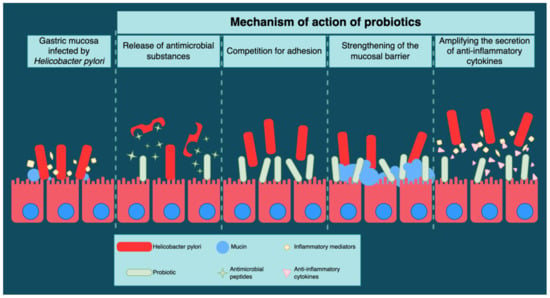
Figure 4.
Probiotics’ mechanism of action in H. pylori therapy.
Antimicrobial Substances
Probiotics release short-chain fatty acids that inhibit H. pylori development. Releasing short-chain fatty acids produced during carbohydrate metabolism, such as acetic, propionic, and lactic acids, determines a reduction in gastric pH.
Antimicrobial compounds related to the bacteriocin classes are synthesized by certain Lactobacillus species (Figure 4). Bacteriocins possess a peptide structure with antimicrobial potential and are implicitly anti-H. pylori [62].
Competition for Adhesion
The mechanisms of the inhibition of the adhesion of H. pylori to the gastric epithelial cells by probiotics depend on the state of the epithelial mucosa, the density of receptors associated with the gastric mucosal adhesion, and the host’s immune status (Figure 4).
The Mucosal Barrier
Mucous surfaces have their own capacity to protect against noxious and pathogenic agents in the intestinal lumen. Mucins are formed by complex glycoproteins that protect the intestinal mucosa from microbial pathogens [63]. A study performed in 2014 by Hanish et al. described the ability of H. pylori to suppress mucin gene expression in gastric cells. This ability of mucins restores the permeability of the gastric mucosa membrane and inhibits the adhesion of H. pylori to the epithelial cells [64] (Figure 4).
6.3.2. Immunological Mechanisms
The release of different inflammatory mediators, such as chemokines and cytokines, represents a characteristic inflammatory response to the infection caused by H. pylori. The role of probiotics consists of modulating the immunological response by amplifying the secretion of anti-inflammatory cytokines, leading to a reduction in gastric inflammation [65] (Figure 4).
Lactobacillus, Bifidobacterium, and Saccharomyces are beneficial probiotics in eradicating H. pylori and reducing the side effects of antimicrobial therapy, such as nausea, vomiting, diarrhea, and epigastric pain, improving drug tolerance and patient compliance. Probiotics should be administered concurrently with standard triple therapy due to the significant increase in the H. pylori eradication rate and the reduction in side effects.
6.4. Efficacity of Different Probiotics
The association of Lactobacillus acidophilus/Bifidobacterium animalis, Lactobacillus acidophilus/Bifidobacterium bifidum, Lactobacillus helveticus/Lactobacillus rhamnosus, and Lactobacillus acidophilus/Bifidobacterium longum/Enterococcus faecalis administered in association with standard triple therapy reduced the incidence of secondary effects and the occurrence of antibiotic-associated diarrhea. Emara et al. studied the role of probiotics in histological improvement, demonstrating a decrease in H. pylori density on the luminal part of the epithelium, thus improving the histological degree of inflammation in the corpus and gastric antrum [66].
On the other hand, the eradication of H. pylori could be improved by the intestinal microbiota, according to available data [16,67]. The association of probiotics with the triple therapy scheme (Streptococcus faecium and Bacillus subtilis) can reduce the occurrence of antibiotic-resistant bacterial strains [68].
Guillemard et al. conducted a randomized controlled trial on 136 adults undergoing 14 days of H. pylori triple therapy, using fermented milk containing yogurt strains and Lactobacillus paracasei CNCM I-1518, Lactobacillus paracasei CNCM I-3689, and Lactobacillus rhamnosus CNCM I-3690 as a probiotic. They suggested the probiotic had a protective effect, preserving short-chain fatty acid production and gut microbiota homeostasis. However, the product’s effect on antibiotic-associated diarrhea and gastrointestinal symptoms was negligible, as both occurrences had an unexpectedly low frequency in the control population [69].
A prospective randomized placebo-controlled trial conducted by Viazis et al. evaluated the efficacy of the combined use of four probiotic strains—Lactobacillus acidophilus, Lactiplantibacillus planatarum, Saccharomyces boulardii, and Bifidobacterium lactis. The probiotic mixture was administered to patients receiving a quadruple eradication regimen. They discovered that probiotic use yielded an increase in H. pylori eradication rate (92.0% in the test group vs. 86.8% in the control group) and a significant decrease in treatment-associated severe symptoms (1.2% in the test group vs. 14.6% in the control group) [70].
Chen et al. measured the effect of probiotics on the bacterial load of H. pylori in a double-blinded, randomized, controlled trial. The researchers used only strains of Lactobacillus acidophilus and Lactobacillus rhamnosus, without PPIs or antibiotics. They concluded that probiotics lowered the bacterial load for the duration of the treatment in the test group, but with no significant difference between groups 2 weeks after the treatment stopped. Eradication of H. pylori was observed in none of the patients [71].
7. Particular Aspects of H. pylori Infection in Pediatric Patients
In industrialized countries, the incidence of infection in the pediatric field increases with age [72]. According to epidemiological studies, H. pylori infection in children is influenced by environmental factors, factors of the gastric mucosa of the host, and bacterial virulence [73], and it could be carried throughout life if left untreated.
According to the guidelines of the European Society of Pediatric Gastroenterology and Nutrition (ESPGHAN)/North American Society of Pediatric Gastroenterology and Nutrition (NASPGHAN), a positive culture accompanied by another examination (a rapid urease test) is necessary for diagnosis.
The risk factors related to the infection are represented by environmental and family characteristics, such as hygiene factors, sanitary conditions at home, the number of people living in the house, and the family history of dyspeptic disorders. Other risk factors are represented by the history of previously prescribed antibiotic treatments for other infectious pathologies (e.g., respiratory tract, which is common in children). The preferred administration of clarithromycin or amoxicillin/clavulanic acid determined the increase in antibiotic resistance of H. pylori. Recent studies propose dental plaque and caries as reservoirs for H. pylori in the pediatric population [74,75].
The infection appears around ten years of age, with most patients being asymptomatic for long periods. Clinical manifestations are non-specific, and some may be justified only by the presence of complications. Frequent symptoms such as nausea or epigastric pain may decrease in frequency and intensity or even disappear with or without the eradication of the bacteria. A meta-analysis documented a statistically significant association with epigastric pain but no statistically significant association with other nonspecific digestive symptoms, such as vomiting, diarrhea, flatulence, abdominal pain, or constipation [76].
In a recent study, Kolasa-Kicińska et al. highlighted the association between H. pylori infection and idiopathic short stature. They detected lower insulin-like growth factor 1 and ghrelin levels in infected children, hypothesizing that the decline in growth rate in this subpopulation is directly caused by diminished concentrations of these two hormones [77].
The literature supports the link between iron deficiency anemia and H. pylori infection in pediatric patients. However, the direct connection between these two pathological entities is not clear, and causality has not yet been proven. Likely, this association is simply due to the low socio-economic status of the analyzed cohorts, predisposing patients to both iron deficiency and H. pylori infection [78].
An association between chronic tonsillitis and H. pylori infection was recently described in the literature. This association is not present in the adult population, but only in children. Researchers state that chronic tonsillitis could be relevant to pediatric H. pylori infection [79]. Another association observed is between H. pylori and celiac disease. A recent study confirmed this correlation but could not clarify the causality, emphasizing the need for future research [80].
One cross-sectional study by Wang et al. suggests a negative correlation between asthma and H. pylori in pediatric patients. In the studied cohort, 3.77% of the H. pylori-positive group were diagnosed with asthma, while it was diagnosed in 7.23% of the H. pylori-negative group [81].
Symptoms such as vomiting, a digestive hemorrhage, iron-deficiency anemia, and malnutrition may be due to complications of H. pylori infection or other etiological diagnoses and therefore require further investigation.
The positive diagnosis in children must be performed using invasive methods, and the response evaluation after the eradication therapy using non-invasive methods [82].
The most common endoscopic diagnosis in children is nodular gastritis. Initially, H. pylori colonizes the antrum and can produce antral gastritis. Unlike in adults, peptic ulcers in children are rare. Gastric atrophy and intestinal metaplasia are less common in children than in adults [83].
The sensitivity of all invasive methods is influenced by antibiotics, bismuth, proton pump inhibitors (PPIs), and upper gastrointestinal bleeding. Culture has a high specificity of 100%, but the sensitivity is diminished by antibiotics, PPIs, bismuth, and active digestive bleeding, and a negative culture does not exclude the diagnosis [19,84]. PCR offers excellent specificity and sensitivity, allowing the detection of specific mutations that lead to antibiotic resistance. RUT is a rapid method with high sensitivity and specificity, even though the sensitivity decreases in young children after using antibiotics, PPIs, and bismuth. Histology allows a positive diagnosis and appreciates the degree of chronic inflammation, lymphoid follicles, atrophic gastritis, and intestinal metaplasia. Neutrophil infiltration is less significant in children than in adults, but infiltration by lymphocytes, plasma cells, and immunosuppressive regulatory T cells is predominant [19,84].
Non-invasive tests are not the first step in detecting H. pylori infection in children, except in cases where endoscopy cannot be performed. The stool antigen test and the urea breath test are used to evaluate eradication and are indicated four weeks after therapy. If SAT is positive after treatment, it is recommended to perform UBT in children. Some studies suggest a non-invasive test evaluation annually, especially in high-prevalence areas or in patients at risk [85].
H. pylori serological tests in serum, blood, urine, and saliva are not modified by PPI or antimicrobial treatment and have a high sensitivity. Still, they are used for epidemiological purposes with anti-H. pylori antibodies remaining positive for a while after eradication, so they do not allow for differentiation between current and chronic infection.
The treatment of H. pylori infection in pediatric patients is based on protocols of the ESPGHAN/NASPGHAN guidelines, revised in 2016.
The first-line treatment is recommended according to the antimicrobial susceptibility of the H. pylori strain or the tendency of antimicrobial resistance in the respective region. Eradication control should preferably be performed through a non-invasive test (a urea breath test in children over six years old or a stool antigen test) 4–8 weeks after the end of the antibiotic treatment. The main causes of treatment failure are antimicrobial resistance, side effects of therapy, and low compliance to the treatment in the pediatric population [82,86,87]. One novel finding suggests that the expression of inflammatory cytokines heavily influences the success rate of H. pylori eradication therapy. Raised concentrations of IL-1β, IL-6, and TNF-α seem to represent risk factors for the failure of eradication [88].
Without a treatment regimen, eradication is highly unlikely. Spontaneous eradication is mainly described in young children, but the eradication rate reduces with age [89].
Standard triple therapy based on clarithromycin is widely prescribed, especially in the primary care network. Alternative regimens are only recommended in specialist centers. The widespread use of antibiotics (clarithromycin for respiratory infections) in the general population has increased antibiotic resistance [82,86,87,90,91].
Future studies evaluating compliance with different treatment regimens, higher PPI doses, and quadruple therapies are sometimes needed, particularly in patients with unknown susceptibility, multidrug-resistant strains, or triple therapy failure.
Available data on probiotics in H. pylori infection suggest that Lactobacillus supplementation to therapy at high doses and for long periods decreases the risk of adverse effects, such as diarrhea [92].
The administration of probiotics as supportive therapy along with the standard regimen reduced the eradication rate by approximately 13% (84.0% versus 71.4%). According to a meta-analysis by Fang et al. [92], it may reduce the incidence of therapy-associated diarrhea.
Efforts to investigate and treat H. pylori infection in children should be based on providing tangible benefits, such as lower complication rates, interrelation with allergic, parasitic, or immunological diseases, antimicrobial resistance, and the few treatment alternatives available to the pediatric population.
8. Conclusions
The prevalence of antibiotic resistance to clarithromycin and metronidazole in H. pylori infection is not negligible, a finding that highlights the need for a new orientation of gastroenterology teams in diagnosing and treating H. pylori infections.
The exhaustive treatment with antibiotics increases the pressure on the medical community, so implementing local and national screening and surveillance programs and developing new non-invasive techniques in clinical practice are imperative to amplify the efficacy of chronic H. pylori infection treatment.
H. pylori infection remains a vital pathogen implicated in digestive pathology. A better understanding of the behavior of the immune system at different ages, favoring the persistence of infection in childhood, and then gastric complications in adults, may help to develop global strategies for reducing the prevalence of H. pylori to prevent the long-term adverse effects associated with H. pylori infection.
Associating probiotics with traditional treatment regimens increases the eradication rate due to the reduced side effects of antibiotics and improved treatment compliance. However, this effect might be specific to the strain, dose, or duration of the therapy.
A fascinating perspective hypothesis is the administration of probiotics to reduce H. pylori adhesion to gastric epithelial cells, preventing H. pylori colonization, especially in children, or reinfection with H. pylori in high-risk patients.
Researchers’ results are encouraging, but further clinical trials are needed. Additional studies will clarify the appropriate probiotic strain choice, dosage, and duration of administration.
Author Contributions
Conceptualization, C.M.M., R.C., M.O. and P.M.; methodology, C.M.V.; software, A.I.S.P.; validation, C.M.M., M.P. and C.M.V.; formal analysis, R.C. and M.O.; investigation, S.B. and D.P.; resources, C.M.M.; data curation, C.M.V. and M.P.; writing—original draft preparation, I.C.M., G.A.I. and M.D.P.; writing—review and editing, C.M.M. and C.M.V.; visualization, M.S. and P.M.; supervision, C.M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Moodley, Y.; Linz, B.; Bond, R.P.; Nieuwoudt, M.; Soodyall, H.; Schlebusch, C.M.; Bernhöft, S.; Hale, J.; Suerbaum, S.; Mugisha, L.; et al. Age of the Association between Helicobacter pylori and Man. PLoS Pathog. 2012, 8, e1002693. [Google Scholar] [CrossRef] [PubMed]
- Marshall, B.J.; Warren, J.R. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984, 1, 1311–1315. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhu, Y.; Lu, N.-H. Novel and Effective Therapeutic Regimens for Helicobacter pylori in an Era of Increasing Antibiotic Resistance. Front. Cell. Infect. Microbiol. 2017, 7, 168. [Google Scholar] [CrossRef] [PubMed]
- Peleteiro, B.; Bastos, A.; Ferro, A.; Lunet, N. Prevalence of Helicobacter pylori Infection Worldwide: A Systematic Review of Studies with National Coverage. Dig. Dis. Sci. 2014, 59, 1698–1709. [Google Scholar] [CrossRef]
- Urita, Y.; Watanabe, T.; Kawagoe, N.; Takemoto, I.; Tanaka, H.; Kijima, S.; Kido, H.; Maeda, T.; Sugasawa, Y.; Miyazaki, T.; et al. Role of infected grandmothers in transmission of Helicobacter pylori to children in a Japanese rural town. J. Paediatr. Child Health 2013, 49, 394–398. [Google Scholar] [CrossRef]
- Goh, K.-L.; Chan, W.-K.; Shiota, S.; Yamaoka, Y. Epidemiology of Helicobacter pylori Infection and Public Health Implications. Helicobacter 2011, 16 (Suppl. S1), 1–9. [Google Scholar] [CrossRef]
- Łaszewicz, W.; Iwańczak, F.; Iwańczak, B.; Annabhani, A.; Bała, G.; Bąk-Romaniszyn, L.; Budzyńska, A.; Cader, J.; Celiński, K.; Cichy, W.; et al. Seroprevalence of Helicobacter pylori infection in Polish children and adults depending on socioeconomic status and living conditions. Adv. Med. Sci. 2014, 59, 147–150. [Google Scholar] [CrossRef]
- Backert, S.; Clyne, M. Pathogenesis of Helicobacter pylori Infection. Helicobacter 2011, 16 (Suppl. S1), 19–25. [Google Scholar] [CrossRef]
- Abadi, A.T.B.; Ierardi, E.; Lee, Y.Y. Why do we still have Helicobacter Pylori in our Stomachs. Malays. J. Med. Sci. 2015, 22, 70–75. [Google Scholar]
- Yamaoka, Y. How to eliminate gastric cancer-related death worldwide? Nat. Rev. Clin. Oncol. 2018, 15, 407–408. [Google Scholar] [CrossRef]
- Plummer, M.; Franceschi, S.; Vignat, J.; Forman, D.; De Martel, C. Global burden of gastric cancer attributable to Helicobacter pylori. Int. J. Cancer 2015, 136, 487–490. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Chiang, T.-H.; Chou, C.-K.; Tu, Y.-K.; Liao, W.-C.; Wu, M.-S.; Graham, D.Y. Association Between Helicobacter pylori Eradication and Gastric Cancer Incidence: A Systematic Review and Meta-analysis. Gastroenterology 2016, 150, 1113–1124.e5. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.J.; Kook, M.-C.; Kim, Y.-I.; Cho, S.-J.; Lee, J.Y.; Kim, C.G.; Park, B.; Nam, B.-H. Helicobacter pylori Therapy for the Prevention of Metachronous Gastric Cancer. N. Engl. J. Med. 2018, 378, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Pimentel-Nunes, P.; Libânio, D.; Marcos-Pinto, R.; Areia, M.; Leja, M.; Esposito, G.; Garrido, M.; Kikuste, I.; Megraud, F.; Matysiak-Budnik, T.; et al. Management of epithelial precancerous conditions and lesions in the stomach (MAPS II): European Society of Gastrointestinal Endoscopy (ESGE), European Helicobacter and Microbiota Study Group (EHMSG), European Society of Pathology (ESP), and Sociedade Portuguesa de Endoscopia Digestiva (SPED) guideline update 2019. Endoscopy 2019, 51, 365–388. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Venerito, M.; Schulz, C. Helicobacter pylori Infection: New Facts in Clinical Management. Curr. Treat. Options Gastroenterol. 2018, 16, 605–615. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; O’morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection—The Maastricht IV/Florence Consensus Report. Gut 2012, 61, 646–664. [Google Scholar] [CrossRef]
- Liu, L.; Gao, H.; Wang, H.; Zhu, K.; Yu, W.; Zhang, Y.; Guo, J. Comparison of Esophageal Function Tests to Investigate the Effect of Helicobacter Pylori Infection on Gastroesophageal Reflux Disease (GERD). J. Pharmacol. Exp. Ther. 2018, 24, 4791–4797. [Google Scholar] [CrossRef]
- Gravina, A.G.; Zagari, R.M.; De Musis, C.; Romano, L.; Loguercio, C.; Romano, M. Helicobacter pylori and extragastric diseases: A review. World J. Gastroenterol. 2018, 24, 3204–3221. [Google Scholar] [CrossRef]
- Wang, Y.K.; Kuo, F.C.; Liu, C.J.; Wu, M.C.; Shih, H.Y.; Wang, S.S.; Wu, J.Y.; Kuo, C.H.; Huang, Y.K.; Wu, D.C. Diagnosis of Helicobacter pylori infection: Current options and developments. World J. Gastroenterol. 2015, 21, 11221–11235. [Google Scholar] [CrossRef]
- Guarner, J.; Kalach, N.; Elitsur, Y.; Koletzko, S. Helicobacter pylori diagnostic tests in children: Review of the literature from 1999 to 2009. Eur. J. Pediatr. 2010, 169, 15–25. [Google Scholar] [CrossRef]
- Ferwana, M.; Abdulmajeed, I.; Alhajiahmed, A.; Madani, W.; Firwana, B.; Hasan, R.; Altayar, O.; Limburg, P.J.; Murad, M.H.; Knawy, B. Accuracy of urea breath test in Helicobacter pylori infection: Meta-analysis. World J. Gastroenterol. 2015, 21, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Gisbert, J.P.; De La Morena, F.; Abraira, V. Accuracy of monoclonal stool antigen test for the diagnosis of H. pylori infection: A systematic review and meta-analysis. Am. J. Gastroenterol. 2006, 101, 1921–1930. [Google Scholar] [CrossRef] [PubMed]
- Demirtürk, L.; Yazgan, Y.; Tarçın, O.; Özel, M.; Diler, M.; Öncül, O.; Yıldırım, Ş. Does N-acetyl cystein affect the sensitivity and specificity of Helicobacter pylori stool antigen test? Helicobacter 2003, 8, 120–123. [Google Scholar] [CrossRef]
- Shimoyama, T. Stool antigen tests for the management of Helicobacter pylori infection. World J. Gastroenterol. 2013, 19, 8188–8191. [Google Scholar] [CrossRef] [PubMed]
- Pan, K.F.; Formichella, L.; Zhang, L.; Zhang, Y.; Ma, J.L.; Li, Z.X.; Liu, C.; Wang, Y.M.; Goettner, G.; Ulm, K.; et al. Helicobacter pylori antibody responses and evolution of precancerous gastric lesions in a Chinese population. Int. J. Cancer 2014, 134, 2118–2125. [Google Scholar] [CrossRef] [PubMed]
- Karami, N.; Talebkhan, Y.; Saberi, S.; Esmaeili, M.; Oghalaie, A.; Abdirad, A.; Mostafavi, E.; Hosseini, M.E.; Mohagheghi, M.A.; Mohammadi, M. Seroreactivity to Helicobacter pylori Antigens as a Risk Indicator of Gastric Cancer. Asian Pac. J. Cancer Prev. 2013, 14, 1813–1817. [Google Scholar] [CrossRef] [PubMed]
- Sicinschi, L.A.; Correa, P.; Bravo, L.E.; Peek, R.M.; Wilson, K.T.; Loh, J.T.; Yepez, M.C.; Gold, B.D.; Thompson, D.T.; Cover, T.L.; et al. Non-invasive Genotyping of Helicobacter pylori cagA, vacA, and hopQ from Asymptomatic Children. Helicobacter 2012, 17, 96–106. [Google Scholar] [CrossRef]
- Xiong, L.J.; Tong, Y.; Wang, Z.; Mao, M. Detection of clarithromycin-resistant Helicobacter pylori by stool PCR in children: A comprehensive review of literature. Helicobacter 2013, 18, 89–101. [Google Scholar] [CrossRef]
- Ogaya, Y.; Nomura, R.; Watanabe, Y.; Nakano, K. Detection of Helicobacter pylori DNA in inflamed dental pulp specimens from Japanese children and adolescents. J. Med. Microbiol. 2015, 64, 117–123. [Google Scholar] [CrossRef]
- Cho, Y.-S.; Chae, H.-S.; Na Jang, S.; Kim, J.-S.; Son, H.S.; Kim, H.-K.; Kim, B.-W.; Han, S.-W.; Choi, K.-Y.; Lee, H.K.; et al. Comparison of the 13C-urea breath test and the endoscopic phenol red mucosal pH test in the quantification of Helicobacter pylori infection loading. Korean J. Intern. Med. 2008, 23, 134–139. [Google Scholar] [CrossRef]
- Hernández-Garcés, H.R.; Castellanos-González, V.V.; González-Fabián, L.; Infante-Velázquez, M.; Peña, K.; Andrain-Sierra, Y. Chromoendoscopy with red phenol in the diagnosis of Helicobacter pylori infection. Rev. Esp. Enferm. Dig. 2012, 104, 4–9. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ji, R.; Li, Y.Q.; Gu, X.M.; Yu, T.; Zuo, X.L.; Zhou, C.J. Confocal laser endomicroscopy for diagnosis of Helicobacter pylori infection: A prospective study. J. Gastroenterol. Hepatol. 2010, 25, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Vaira, D.; Vakil, N.; Gatta, L.; Ricci, C.; Perna, F.; Saracino, I.; Fiorini, G.; Holton, J. Accuracy of a new ultrafast rapid urease test to diagnose Helicobacter pylori infection in 1000 consecutive dyspeptic patients. Aliment. Pharm. 2010, 31, 331–338. [Google Scholar]
- Momtaz, H.; Souod, N.; Dabiri, H.; Sarshar, M. Study of Helicobacter pylori genotype status in saliva, dental plaques, stool and gastric biopsy samples. World J. Gastroenterol. 2012, 18, 2105–2111. [Google Scholar] [CrossRef] [PubMed]
- Lehours, P.; Mégraud, F. Helicobacter pylori molecular diagnosis. Expert Rev. Mol. Diagn. 2011, 11, 351–355. [Google Scholar] [CrossRef]
- Graham, D.Y.; Lee, Y.; Wu, M. Rational Helicobacter pylori Therapy: Evidence-Based Medicine Rather Than Medicine-Based Evidence. Clin. Gastroenterol. Hepatol. 2014, 12, 177–186.e3, Discussion e12–13. [Google Scholar] [CrossRef] [PubMed]
- Safavi, M.; Sabourian, R.; Foroumadi, A. Treatment of Helicobacter pylori infection: Current and future insights. World J. Clin. Cases 2016, 4, 5–19. [Google Scholar] [CrossRef]
- Pohl, D.; Keller, P.M.; Bordier, V.; Wagner, K. Review of current diagnostic methods and advances in Helicobacter pylori diagnostics in the era of next generation sequencing. World J. Gastroenterol. 2019, 25, 4629–4660. [Google Scholar] [CrossRef]
- Lai, Y.; Wei, W.; Du, Y.; Gao, J.; Li, Z. Biomaterials for Helicobacter pylori therapy: Therapeutic potential and future perspectives. Gut Microbes 2022, 14, 2120747. [Google Scholar] [CrossRef]
- Flores-Treviño, S.; Mendoza-Olazarán, S.; Bocanegra-Ibarias, P.; Maldonado-Garza, H.J.; Garza-González, E. Helicobacter pylori drug resistance: Therapy changes and challenges. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 819–827. [Google Scholar] [CrossRef]
- Nguyen, C.T.; Davis, K.A.; Nisly, S.A.; Li, J. Treatment of Helicobacter pylori in Special Patient Populations. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2019, 39, 1012–1022. [Google Scholar] [CrossRef]
- Schubert, J.P.; Warner, M.S.; Rayner, C.K.; Roberts-Thomson, I.C.; Mangoni, A.A.; Costello, S.; Bryant, R.V. Increasing Helicobacter pylori clarithromycin resistance in Australia over 20 years. Intern. Med. J. 2022, 52, 1554–1560. [Google Scholar] [CrossRef] [PubMed]
- Federico, A.; Gravina, A.G.; Miranda, A.; Loguercio, C.; Romano, M. Eradication of Helicobacter pylori infection: Which regimen first? World J. Gastroenterol. 2014, 20, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef] [PubMed]
- De Brito, B.B.; Da Silva, F.A.F.; Soares, A.S.; Pereira, V.A.; Santos, M.L.C.; Sampaio, M.M.; Neves, P.H.M.; De Melo, F.F. Pathogenesis and clinical management of Helicobacter pylori gastric infection. World J. Gastroenterol. 2019, 25, 5578–5589. [Google Scholar] [CrossRef] [PubMed]
- Testerman, T.L.; Morris, J. Beyond the stomach: An updated view of Helicobacter pylori pathogenesis, diagnosis, and treatment. World J. Gastroenterol. 2014, 20, 12781–12808. [Google Scholar] [CrossRef]
- Lü, M.; Yu, S.; Deng, J.; Yan, Q.; Yang, C.; Xia, G.; Zhou, X. Efficacy of Probiotic Supplementation Therapy for Helicobacter pylori Eradication: A Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2016, 11, e0163743. [Google Scholar] [CrossRef]
- Ruggiero, P. Use of probiotics in the fight against Helicobacter pylori. World J. Gastrointest. Pathophysiol. 2014, 5, 384–391. [Google Scholar] [CrossRef]
- Na Kim, M.; Kim, N.; Lee, S.H.; Park, Y.S.; Hwang, J.-H.; Kim, J.-W.; Jeong, S.-H.; Lee, D.H.; Kim, J.S.; Jung, H.C.; et al. The Effects of Probiotics on PPI-Triple Therapy for Helicobacter pylori Eradication. Helicobacter 2008, 13, 261–268. [Google Scholar] [CrossRef]
- Nista, E.C.; Candelli, M.; Cremonini, F.; Cazzato, I.A.; Zocco, M.A.; Franceschi, F.; Cammarota, G.; Gasbarrini, G.; Gasbarrini, A. Bacillus clausii therapy to reduce side-effects of anti-Helicobacter pylori treatment: Randomized, double-blind, placebo controlled trial. Aliment. Pharmacol. Ther. 2004, 20, 1181–1188. [Google Scholar] [CrossRef]
- Tong, J.L.; Ran, Z.H.; Shen, J.; Zhang, C.X.; Xiao, S.D. Meta-analysis: The effect of supplementation with probiotics on eradication rates and adverse events during Helicobacter pylori eradication therapy. Aliment. Pharmacol. Ther. 2007, 25, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Dong, J.; Yu, X. Meta-Analysis: Lactobacillus Containing Quadruple Therapy Versus Standard Triple First-Line Therapy for Helicobacter pylori Eradication. Helicobacter 2009, 14, 449–459. [Google Scholar] [CrossRef]
- Szajewska, H.; Horvath, A.; Piwowarczyk, A. Meta-analysis: The effects of Saccharomyces boulardii supplementation on Helicobacter pylori eradication rates and side effects during treatment. Aliment. Pharmacol. Ther. 2010, 32, 1069–1079. [Google Scholar] [CrossRef]
- Wang, Z.-H.; Gao, Q.-Y.; Fang, J.-Y. Meta-Analysis of the Efficacy and Safety of Lactobacillus-containing and Bifidobacterium-containing Probiotic Compound Preparation in Helicobacter pylori Eradication Therapy. J. Clin. Gastroenterol. 2013, 47, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Dang, Y.; Reinhardt, J.D.; Zhou, X.; Zhang, G. The Effect of Probiotics Supplementation on Helicobacter pylori Eradication Rates and Side Effects during Eradication Therapy: A Meta-Analysis. PLoS ONE 2014, 9, e111030. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.M.; Qian, W.; Qin, Y.Y.; He, J.; Zhou, Y.H. Probiotics in Helicobacter pylori eradication therapy: A systematic review and meta-analysis. World J. Gastroenterol. 2015, 21, 4345–4357. [Google Scholar] [CrossRef]
- Szajewska, H.; Horvath, A.; Kołodziej, M. Systematic review with meta-analysis: Saccharomyces boulardii supplementation and eradication of Helicobacter pylori infection. Aliment. Pharmacol. Ther. 2015, 41, 1237–1245. [Google Scholar] [CrossRef]
- McFarland, L.V.; Huang, Y.; Wang, L.; Malfertheiner, P. Systematic review and meta-analysis: Multi-strain probiotics as adjunct therapy for Helicobacter pylori eradication and prevention of adverse events. United Eur. Gastroenterol. J. 2016, 4, 546–561. [Google Scholar] [CrossRef]
- Yang, J.-C.; Lu, C.-W.; Lin, C.-J. Treatment of Helicobacter pylori infection: Current status and future concepts. World J. Gastroenterol. 2014, 20, 5283–5293. [Google Scholar] [CrossRef]
- Feng, J.-R.; Wang, F.; Qiu, X.; McFarland, L.V.; Chen, P.-F.; Zhou, R.; Liu, J.; Zhao, Q.; Li, J. Efficacy and safety of probiotic-supplemented triple therapy for eradication of Helicobacter pylori in children: A systematic review and network meta-analysis. Eur. J. Clin. Pharmacol. 2017, 73, 1199–1208. [Google Scholar] [CrossRef]
- Bhatia, S.J.; Kochar, N.; Abraham, P.; Nair, N.G.; Mehta, A.P. Lactobacillus acidophilus inhibits growth of Campylobacter pylori in vitro. J. Clin. Microbiol. 1989, 27, 2328–2330. [Google Scholar] [CrossRef] [PubMed]
- Aiba, Y.; Nakano, Y.; Koga, Y.; Takahashi, K.; Komatsu, Y. A highly acid-resistant novel strain of Lactobacillus johnsonii No. 1088 has antibacterial activity, including that against Helicobacter pylori, and inhibits gastrin-mediated acid production in mice. Microbiologyopen 2015, 4, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Mack, D.R.; Ahrne, S.; Hyde, L.; Wei, S.; Hollingsworth, M.A. Extracellular MUC3 mucin secretion follows adherence of Lactobacillus strains to intestinal epithelial cells in vitro. Gut 2003, 52, 827–833. [Google Scholar] [CrossRef]
- Hanisch, F.G.; Bonar, D.; Schloerer, N.; Schroten, H. Human Trefoil Factor 2 Is a Lectin That Binds α-GlcNAc-capped Mucin Glycans with Antibiotic Activity against Helicobacter pylori. J. Biol. Chem. 2014, 289, 27363–27375. [Google Scholar] [CrossRef]
- Wiese, M.; Eljaszewicz, A.; Andryszczyk, M.; Gronek, S.; Gackowska, L.; Kubiszewska, I.; Kaszewski, W.; Helmin-Basa, A.; Januszewska, M.; Motyl, I.; et al. Immunomodulatory effects of Lactobacillous plantarum and Helicobacter pylori CagA? on the expression of selected superficial molecules on monocyte and lymphocyte and the synthesis of cytokines in whole blood culture. J. Physiol. Pharmacol. Off. J. Pol. Physiol. Soc. 2012, 63, 217–224. [Google Scholar]
- Emara, M.H.; Elhawari, S.A.; Yousef, S.; Radwan, M.I.; Abdel-Aziz, H.R. Emerging Role of Probiotics in the Management of Helicobacter Pylori Infection: Histopathologic Perspectives. Helicobacter 2016, 21, 3–10. [Google Scholar] [CrossRef]
- Jakobsson, H.E.; Jernberg, C.; Andersson, A.F.; Sjölund-Karlsson, M.; Jansson, J.K.; Engstrand, L. Short-Term Antibiotic Treatment Has Differing Long-Term Impacts on the Human Throat and Gut Microbiome. PLoS ONE 2010, 5, e9836. [Google Scholar] [CrossRef]
- Oh, B.; Kim, B.S.; Kim, J.W.; Kim, J.S.; Koh, S.J.; Kim, B.G.; Lee, K.L.; Chun, J. The Effect of Probiotics on Gut Microbiota during the Helicobacter pylori Eradication: Randomized Controlled Trial. Helicobacter 2016, 21, 165–174. [Google Scholar] [CrossRef]
- Guillemard, E.; Poirel, M.; Schäfer, F.; Quinquis, L.; Rossoni, C.; Keicher, C.; Wagner, F.; Szajewska, H.; Barbut, F.; Derrien, M.; et al. A Randomised, Controlled Trial: Effect of a Multi-Strain Fermented Milk on the Gut Microbiota Recovery after Helicobacter pylori Therapy. Nutrients 2021, 13, 3171. [Google Scholar] [CrossRef]
- Viazis, N.; Argyriou, K.; Kotzampassi, K.; Christodoulou, D.K.; Apostolopoulos, P.; Georgopoulos, S.D.; Liatsos, C.; Giouleme, O.; Koustenis, K.; Veretanos, C.; et al. A Four-Probiotics Regimen Combined with A Standard Helicobacter pylori-Eradication Treatment Reduces Side Effects and Increases Eradication Rates. Nutrients 2022, 14, 632. [Google Scholar] [CrossRef]
- Chen, M.J.; Chen, C.C.; Huang, Y.C.; Tseng, C.C.; Hsu, J.T.; Lin, Y.F.; Fang, Y.J.; Wu, M.S.; Liou, J.M.; Taiwan Gastrointestinal Disease; et al. The efficacy of Lactobacillus acidophilus and rhamnosus in the reduction of bacterial load of Helicobacter pylori and modification of gut microbiota-a double-blind, placebo-controlled, randomized trial. Helicobacter 2021, 26, e12857. [Google Scholar] [CrossRef] [PubMed]
- Helaly, G.H.; El-Afandy, N.M.; Hassan, A.A.; Dowidar, N.L.; Sharaf, S.M. Diagnostic Value of Housekeeping [glmM] Gene Expression in Antral Biopsies in Comparison to Rapid Urease Test and Histological Detection of Helicobacter Pylori Infection. Egypt. J. Med. Microbiol. 2009, 18, 119–130. [Google Scholar]
- Xu, C.; Wu, Y.; Xu, S. Association between Helicobacter pylori infection and growth outcomes in children: A meta-analysis. Helicobacter 2022, 27, e12861. [Google Scholar] [CrossRef]
- Mehdipour, A.; Chaboki, P.; Rasouli Asl, F.; Aghaali, M.; Sharifinejad, N.; Shams, S. Comparing the prevalence of Helicobacter pylori and virulence factors cagA, vacA, and dupA in supra-gingival dental plaques of children with and without dental caries: A case-control study. BMC Oral Health 2022, 22, 170. [Google Scholar] [CrossRef] [PubMed]
- Sruthi, M.A.; Mani, G.; Ramakrishnan, M.; Selvaraj, J. Dental caries as a source of Helicobacter pylori infection in children: An RT-PCR study. Int. J. Paediatr. Dent. 2023, 33, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Spee, L.A.A.; Madderom, M.B.; Pijpers, M.; Van Leeuwen, Y.; Berger, M.Y. Association Between Helicobacter pylori and Gastrointestinal Symptoms in Children. Pediatrics 2010, 125, e651–e669. [Google Scholar] [CrossRef] [PubMed]
- Kolasa-Kicińska, M.; Stawerska, R.; Stawerski, P.; Kałużyński, A.; Czkwianianc, E.; Lewiński, A. Effects of Helicobacter pylori Infection on Ghrelin and Insulin-like Growth Factor 1 Secretion in Children with Idiopathic Short Stature. J. Clin. Med. 2022, 11, 5868. [Google Scholar] [CrossRef]
- Lupu, A.; Miron, I.C.; Cianga, A.L.; Cernomaz, A.T.; Lupu, V.V.; Munteanu, D.; Ghica, D.C.; Fotea, S. The Relationship between Anemia and Helicobacter Pylori Infection in Children. Children 2022, 9, 1324. [Google Scholar] [CrossRef]
- Wu, X.; Wang, W.; Fang, L.; Shi, L.; Rao, X. Is Helicobacter pylori colonization associated with chronic tonsillitis?—A meta-analysis and systematic review. Am. J. Otolaryngol. 2022, 43, 103515. [Google Scholar] [CrossRef]
- Yue, M.; Chen, Q.; Zhou, X.; Li, L.; Lu, C. Is Helicobacter pylori Infection Associated with Celiac Disease? A Meta-analysis. Turk. J. Gastroenterol. 2022, 33, 205–212. [Google Scholar] [CrossRef]
- Wang, D.; Chen, Y.; Ding, Y.; Tu, J. Inverse association between Helicobacter pylori infection and childhood asthma in a physical examination population: A cross-sectional study in Chongqing, China. BMC Pediatr. 2022, 22, 615. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.L.; Koletzko, S.; Goodman, K.; Bontems, P.; Cadranel, S.; Casswall, T.; Czinn, S.; Gold, B.D.; Guarner, J.; Elitsur, Y.; et al. Joint ESPGHAN/NASPGHAN Guidelines for the Management of Helicobacter pylori in Children and Adolescents (Update 2016). J. Craniofacial Surg. 2017, 64, 991–1003. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, G.; Gottrand, F. Does gastric atrophy exist in children? World J. Gastroenterol. 2006, 12, 6274–6279. [Google Scholar] [CrossRef] [PubMed]
- Sabbagh, P.; Mohammadnia-Afrouzi, M.; Javanian, M.; Babazadeh, A.; Koppolu, V.; Vasigala, V.R.; Nouri, H.R.; Ebrahimpour, S. Diagnostic methods for Helicobacter pylori infection: Ideals, options, and limitations. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 55–66. [Google Scholar] [CrossRef] [PubMed]
- Kayali, S.; Manfredi, M.; Gaiani, F.; Bianchi, L.; Bizzarri, B.; Leandro, G.; Di Mario, F.; Angelis, G.L.D. Helicobacter pylori, transmission routes and recurrence of infection: State of the art. Acta Biomed. 2018, 89, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Leal, Y.A.; Flores, L.L.; Fuentes-Pananá, E.M.; Cedillo-Rivera, R.; Torres, J. 13C-Urea Breath Test for the Diagnosis of Helicobacter pylori Infection in Children: A Systematic Review and Meta-Analysis. Helicobacter 2011, 16, 327–337. [Google Scholar] [CrossRef]
- Leal, Y.A.; Cedillo-Rivera, R.; Simón, J.A.; Velazquez, J.; Flores, L.L.; Torres, J. Utility of Stool Sample–based Tests for the Diagnosis of Helicobacter pylori Infection in Children. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 718–728. [Google Scholar] [CrossRef]
- Zhang, S.; Zhang, Y.; Chen, S.; Teng, Y.; Li, C. Effects of inflammatory cytokines on eradication and recurrence of Helicobacter pylori infection in children. Pak. J. Med. Sci. 2022, 38, 1883–1887. [Google Scholar] [CrossRef]
- O’Ryan, M.L.; Lucero, Y.; Rabello, M.; Mamani, N.; Salinas, A.M.; Peña, A.; Torres-Torreti, J.P.; Mejías, A.; Ramilo, O.; Suarez, N.; et al. Persistent and TransientHelicobacter pyloriInfections in Early Childhood. Clin. Infect. Dis. 2015, 61, 211–218. [Google Scholar] [CrossRef]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef]
- Megraud, F.; Coenen, S.; Versporten, A.; Kist, M.; Lopez-Brea, M.; Hirschl, A.M.; Andersen, L.P.; Goossens, H.; Glupczynski, Y.; Study Group participants. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013, 62, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.-R.; Zhang, G.-Q.; Cheng, J.-Y.; Li, Z.-Y. Efficacy of Lactobacillus-supplemented triple therapy for Helicobacter pylori infection in children: A meta-analysis of randomized controlled trials. Eur. J. Pediatr. 2019, 178, 7–16. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).