


Staphylococcal Scalded Skin Syndrome in Neonates: Case Series and Overview of Outbreaks



Abstract
1. Introduction
2. Case Description
3. Review
3.1. Clinical Picture
3.2. Differential Diagnosis
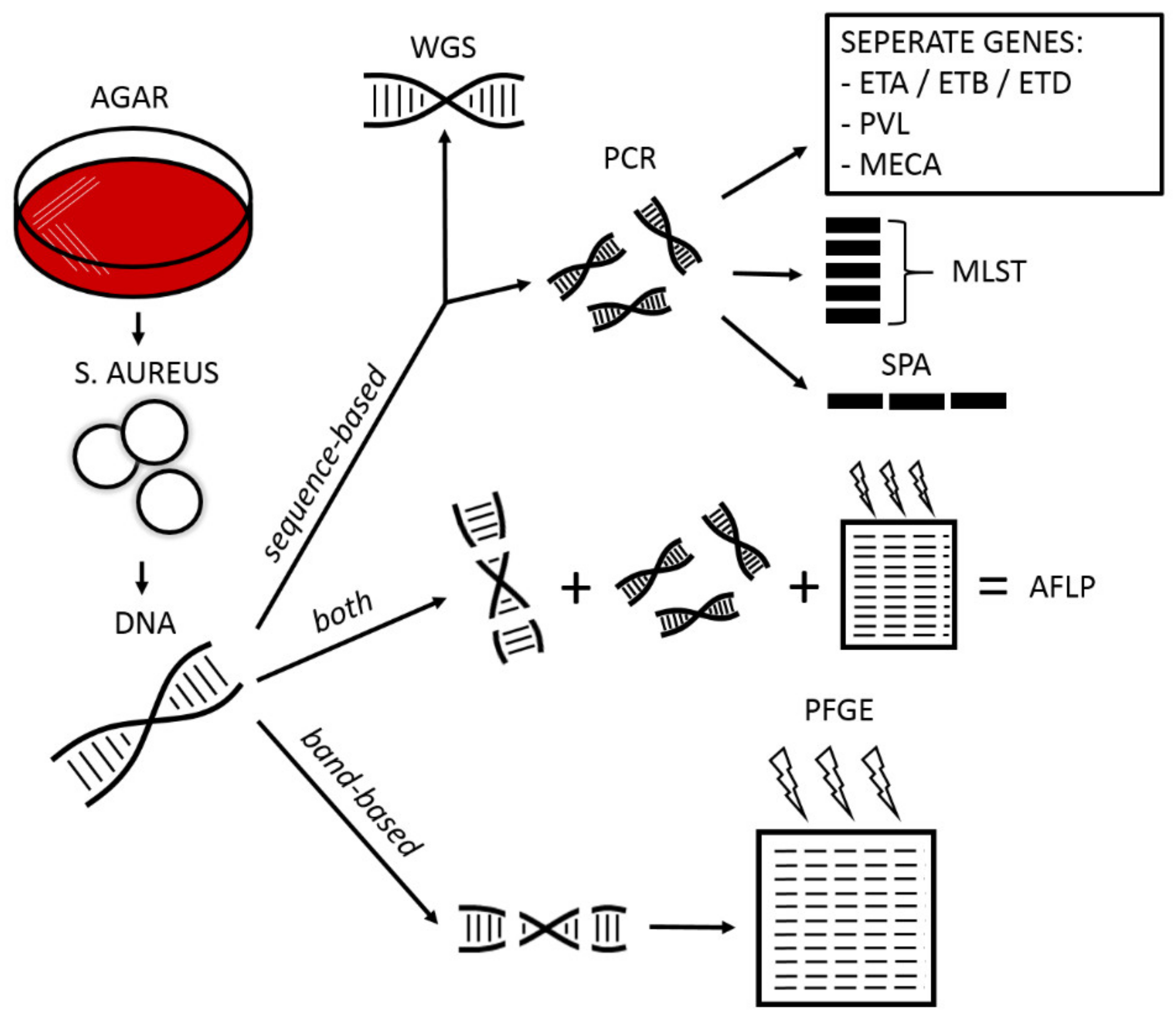
3.3. Diagnostic Techniques
3.4. Management
3.4.1. Treatment
3.4.2. Outbreak Containment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country a | Year | Patients (n) | Time Period (Months) | Age Range b (Days) | Gestational Age c (Weeks) | SSSS d | Intensive Care e | Recurrence | MSSA/MRSA | Source f |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Nusman (this report) | NL | 2019 | 4 | 0.5 | 7–10 | 31.9 ± 5.4 | 3/4 | 1/4 | 2/4 | MSSA | N/S |
| Gopal Rao [43] | UK | 2019 | 12 | 2 | - | 31.7 ± 2.7 | 0/12 | 1/12 | - | MSSA | U |
| Pimentel de Araujo [44] | IT | 2018 | 12 | 8 | 3–17 | - | 10/12 | - | - | MSSA | U |
| Lamanna [45] | IT | 2017 | 3 | 2 | 3–9 | - | 3/3 | - | - | MRSA | P/S |
| Lee [46] | KOR | 2014 | 6 | 1 | 6–14 | - | 0/6 | 1/6 | - | MRSA | U |
| Sanchini [47] | IT | 2013 | 9 | 1 | 4–27 | - | 0/6 | 0/6 | - | MRSA | E/N/S |
| Paranthaman [48] | UK | 2012 | 8 | 4 | 6–10 | >37 | 8/8 | 0/8 | - | Both | S |
| Alsubaie [49] | SAU | 2012 | 13 | 1 | 2–16 | 38.2 ± 1.6 | 0/13 | 0/13 | 0/13 | MRSA | U |
| Neylon [50] | IRE | 2010 | 10 | 2.5 | 5–13 | 38.6 ± 1.1 g | 5/10 | 0/10 | - | Both | U |
| Gould [51] | SCO | 2009 | 7 | 6 | 4–48 | - | 5/7 h | 0/10 | - | MRSA | U |
| Kurlenda [52] | POL | 2009 | 6 | 1 | 5–34 | >37 | 4/6 | 0/10 | - | MSSA | U |
| James [53] | USA | 2008 | 11 | 8 | 4–23 | >37 | 0/11 | 0/10 | - | MRSA | N/S |
| El Helali [54] | FRA | 2005 | 13 | 3 | 4–18 | 39.1 (37–41) | 13/13 | 1 i | - | MRSA | N/S |
| Weist [55] | GER | 2000 | 10 | 4 | 4–9 | >37 | 0/10 | 0/10 | - | MSSA | E |
| Zafar [56] | USA | 1995 | 22 | 6 | 3–29 | >37 | 0/22 | - | 0/22 | MRSA | N/S |
| Dave [57] | UK | 1994 | 30 | 3 | - | - | 21/23 | - | 9/30 | MRSA | E/S |
| Richardson [58] | UK | 1990 | 12 | 1.5 | 3–17 | - | 4/11 | - | - | MRSA | S |
| Dancer [59] | UK | 1988 | 12 | 2 | 3–16 | - | 12/12 | - | - | MRSA | P/S |
| Kaplan [60] | USA | 1986 | A = 84 | 32 | - | - | 2/84 | - | - | - | E |
| B = 51 | 11 | - | - | 0/51 | - | - | - | E/N/S | |||
| Dowsett [61] | UK | 1984 | 13 | 2 | - | - | 9/13 | - | - | MRSA | U |
| Curran [62] | USA | 1980 | 68 | 4 | 4–15 | - | 68/68 | - | - | - | U |
| Faden [63] | USA | 1976 | 4 | 0.25 | 4–7 | - | 1/4 | 0/4 | 0/4 | MRSA | S |
| Benson [64] | UK | 1962 | 12 | 1 | 2–11 | - | 4/12 | 0/12 | 0/12 | - | P/S |
| Howells [65] | UK | 1961 | 14 | 3 | 4–10 | - | 1/14 | 1/14 | - | - | P/S |
3.4.3. Host Characteristics
3.4.4. Pathogen Characteristics
4. Conclusions
Literature Search Strategy and Selection Criteria
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Staiman, A.; Hsu, D.Y.; Silverberg, J.I. Epidemiology of staphylococcal scalded skin syndrome in U.S. children. Br. J. Dermatol. 2017, 178, 704–708. [Google Scholar] [CrossRef] [PubMed]
- Mockenhaupt, M.; Idzko, M.; Grosber, M.; Schöpf, E.; Norgauer, J. Epidemiology of staphylococcal scalded skin syndrome in Germany. J. Investig. Dermatol. 2005, 124, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Lamand, V.; Dauwalder, O.; Tristan, A.; Casalegno, J.S.; Meugnier, H.; Bes, M.; Dumitrescu, O.; Croze, M.; Vandenesch, F.; Etienne, J.; et al. Epidemiological data of staphylococcal scalded skin syndrome in France from 1997 to 2007 and microbiological characteristics of Staphylococcus aureus associated strains. Clin. Microbiol. Infect. 2012, 18, E514–E521. [Google Scholar] [CrossRef] [PubMed]
- Lipový, B.; Brychta, P.; Chaloupková, Z.; Suchánek, I. Staphylococcal scalded skin syndrome in the Czech Republic: An epidemiological study. Burns 2011, 38, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Hanakawa, Y.; Schechter, N.M.; Lin, C.; Garza, L.; Li, H.; Yamaguchi, T.; Fudaba, Y.; Nishifuji, K.; Sugai, M.; Amagai, M.; et al. Molecular mechanisms of blister formation in bullous impetigo and staphylococcal scalded skin syndrome. J. Clin. Investig. 2002, 110, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.K.C.; Barankin, B.; Leong, K.F. Staphylococcal-scalded skin syndrome: Evaluation, diagnosis, and management. World J. Pediatr. 2018, 14, 116–120. [Google Scholar] [CrossRef]
- Ladhani, S.; Joannou, C.L.; Lochrie, D.P.; Evans, R.W.; Poston, S.M. Clinical, microbial, and biochemical aspects of the exfoliative toxins causing staphylococcal scalded-skin syndrome. Clin. Microbiol. Rev. 1999, 12, 224–242. [Google Scholar] [CrossRef]
- Rifai, S.; Barbancon, V.; Prevost, G.; Piemont, Y. Synthetic exfoliative toxin A and B DNA probes for detection of toxigenic Staphylococcus aureus strains. J. Clin. Microbiol. 1989, 27, 504–506. [Google Scholar] [CrossRef]
- Li, M.Y.; Hua, Y.; Wei, G.H.; Qiu, L. Staphylococcal scalded skin syndrome in neonates: An 8-year retrospective study in a single institution. Pediatr. Dermatol. 2013, 31, 43–47. [Google Scholar] [CrossRef]
- Fertitta, L.; Welfringer-Morin, A.; Rigourd, V.; Jamet, A.; Hadj-Rabia, S.; Lesage, F.; Bodemer, C. Neonatal staphylococcal scalded skin syndrome in a breastfed neonate. J. Eur. Acad. Dermatol. Venereol. 2019, 34, e36–e38. [Google Scholar] [CrossRef]
- Haveman, L.M.; Fleer, A.; De Vries, L.S.; Gerards, L.J. Congenital staphylococcal scalded skin syndrome in a premature infant. Acta Paediatr. 2004, 93, 1661–1662. [Google Scholar] [CrossRef]
- Hubiche, T.; Bes, M.; Roudiere, L.; Langlaude, F.; Etienne, J.; Del Giudice, P. Mild staphylococcal scalded skin syndrome: An underdiagnosed clinical disorder. Br. J. Dermatol. 2011, 166, 213–215. [Google Scholar] [CrossRef]
- Norbury, W.B.; Gallagher, J.J.; Herndon, D.N.; Branski, L.K.; Oehring, P.E.; Jeschke, M.G. Neonate twin with staphylococcal scalded skin syndrome from a renal source. Pediatr. Crit. Care Med. 2010, 11, e20–e23. [Google Scholar] [CrossRef]
- Bae, S.H.; Lee, J.-B.; Won, Y.H.; Kim, S.-J.; Lee, S.-C.; Yun, S.J. Case of bullous impetigo with enormous bulla developing into staphylococcal scalded skin syndrome. J. Dermatol. 2015, 43, 459–460. [Google Scholar] [CrossRef]
- Yamasaki, O.; Yamaguchi, T.; Sugai, M.; Chapuis-Cellier, C.; Arnaud, F.; Vandenesch, F.; Etienne, J.; Lina, G. Clinical manifestations of staphylococcal scalded-skin syndrome depend on serotypes of exfoliative toxins. J. Clin. Microbiol. 2005, 43, 1890–1893. [Google Scholar] [CrossRef]
- Wang, E.A.; Chambers, C.J.; Silverstein, M. A rare presentation of congenital syphilis: Pemphigus syphiliticus in a newborn infant with extensive desquamation of the extremities. Pediatr. Dermatol. 2018, 35, e110–e113. [Google Scholar] [CrossRef]
- Chakraborty, R.; Luck, S. Syphilis is on the increase: The implications for child health. Arch. Dis. Child. 2008, 93, 105–109. [Google Scholar] [CrossRef]
- Herremans, T.; Kortbeek, L.; Notermans, D.W. A review of diagnostic tests for congenital syphilis in newborns. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 495–501. [Google Scholar] [CrossRef]
- Witte, M.; Zillikens, D.; Schmidt, E. Diagnosis of Autoimmune Blistering Diseases. Front. Med. 2018, 5, 296. [Google Scholar] [CrossRef]
- Lin, L.; Zeng, X.; Chen, Q. Pemphigus and pregnancy. Analysis and summary of case reports over 49 years. Saudi Med. J. 2015, 36, 1033–1038. [Google Scholar] [CrossRef]
- Frca, J.H.; Rscn, J.D.; Frcpch, A.G.; Frca, R.H. Epidermolysis bullosa in children: Pathophysiology, anaesthesia and pain management. Paediatr. Anaesth 2002, 12, 388–397. [Google Scholar]
- Vos, P.; Hogers, R.; Bleeker, M.; Reijans, M.; Van De Lee, T.; Hornes, M.; Friters, A.; Pot, J.; Paleman, J.; Kuiper, M.; et al. AFLP: A new technique for DNA fingerprinting. Nucleic Acids Res. 1995, 23, 4407–4414. [Google Scholar] [CrossRef] [PubMed]
- Melles, D.C.; van Leeuwen, W.B.; Snijders, S.V.; Horst-Kreft, D.; Peeters, J.K.; Verbrugh, H.A.; van Belkum, A. Comparison of multilocus sequence typing (MLST), pulsed-field gel electrophoresis (PFGE), and amplified fragment length polymorphism (AFLP) for genetic typing of Staphylococcus aureus. J. Microbiol. Methods 2007, 69, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Kuroda, M.; Ohta, T.; Uchiyama, I.; Baba, T.; Yuzawa, H.; Kobayashi, I.; Cui, L.; Oguchi, A.; Aoki, K.-I.; Nagai, Y.; et al. Whole genome sequencing of meticillin-resistant Staphylococcus aureus. Lancet 2001, 357, 1225–1240. [Google Scholar] [CrossRef] [PubMed]
- Diep, B.A. Use of whole-genome sequencing for outbreak investigations. Lancet Infect. Dis. 2013, 13, 99–101. [Google Scholar] [CrossRef]
- Sabat, A.J.; Budimir, A.; Nashev, D.; Sá-Leão, R.; van Dijl, J.M.; Laurent, F.; Grundmann, H.; Friedrich, A.W.; on behalf of the ESCMID Study Group of Epidemiological Markers (ESGEM). Overview of molecular typing methods for outbreak detection and epidemiological surveillance. Eurosurveillance 2013, 18, 20380. [Google Scholar] [CrossRef]
- Lo, W.T.; Wang, C.C. Panton-Valentine leukocidin in the pathogenesis of community-associated methicillin-resistant Staphylococcus aureus infection. Pediatr. Neonatol. 2011, 52, 59–65. [Google Scholar] [CrossRef]
- Peacock, S.J.; Paterson, G.R. Mechanisms of Methicillin Resistance in Staphylococcus aureus. Annu. Rev. Biochem. 2015, 84, 577–601. [Google Scholar] [CrossRef]
- Deurenberg, R.H.; Stobberingh, E.E. The evolution of Staphylococcus aureus. Infect. Genet. Evol. 2008, 8, 747–763. [Google Scholar] [CrossRef]
- Maiden, M.C.J.; Bygraves, J.A.; Feil, E.; Morelli, G.; Russell, J.E.; Urwin, R.; Zhang, Q.; Zhou, J.; Zurth, K.; Caugant, D.A.; et al. Multilocus sequence typing: A portable approach to the identification of clones within populations of pathogenic microorganisms. Proc. Natl. Acad. Sci. USA 1998, 95, 3140–3145. [Google Scholar] [CrossRef]
- Frénay, H.M.; Bunschoten, A.E.; Schouls, L.M.; van Leeuwen, W.J.; Vandenbroucke-Grauls, C.M.; Verhoef, J.; Mooi, F.R. Molecular typing of methicillin-resistant Staphylococcus aureus on the basis of protein A gene polymorphism. Eur. J. Clin. Microbiol. Infect. Dis. 1996, 15, 60–64. [Google Scholar] [CrossRef]
- Choi, J.H.; Lee, H.; Choi, E.H. Antimicrobial Resistance and Molecular Analysis of Staphylococcus aureus in Staphylococcal Scalded Skin Syndrome among Children in Korea. J. Korean Med. Sci. 2021, 36, e22. [Google Scholar] [CrossRef]
- Wang, Z.; Feig, J.L.; Mannschreck, D.B.; Cohen, B.A. Antibiotic sensitivity and clinical outcomes in staphylococcal scalded skin syndrome. Pediatr. Dermatol. 2019, 37, 222–223. [Google Scholar] [CrossRef]
- Braunstein, I.; Wanat, K.A.; Abuabara, K.; McGowan, K.L.; Yan, A.C.; Treat, J.R. Antibiotic sensitivity and resistance patterns in pediatric staphylococcal scalded skin syndrome. Pediatr. Dermatol. 2013, 31, 305–308. [Google Scholar] [CrossRef]
- Liy-Wong, C.; Pope, E.; Weinstein, M.; Lara-Corrales, I. Staphylococcal scalded skin syndrome: An epidemiological and clinical review of 84 cases. Pediatr. Dermatol. 2020, 38, 149–153. [Google Scholar] [CrossRef]
- Kapoor, V.; Travadi, J.; Braye, S. Staphylococcal scalded skin syndrome in an extremely premature neonate: A case report with a brief review of literature. J. Paediatr. Child Health 2008, 44, 374–376. [Google Scholar] [CrossRef]
- Saida, K.; Kawasaki, K.; Hirabayashi, K.; Akazawa, Y.; Kubota, S.; Kasuga, E.; Kusakari, M.; Ishida, T.; Kitamura, M.; Baba, A.; et al. Exfoliative toxin A staphylococcal scalded skin syndrome in preterm infants. Eur. J. Pediatr. 2014, 174, 551–555. [Google Scholar] [CrossRef]
- Kong, C.; Neoh, H.-M.; Nathan, S. Targeting Staphylococcus aureus Toxins: A Potential form of Anti-Virulence Therapy. Toxins 2016, 8, 72. [Google Scholar] [CrossRef]
- Davidson, J.; Polly, S.; Hayes, P.J.; Fisher, K.R.; Talati, A.J.; Patel, T. Recurrent Staphylococcal Scalded Skin Syndrome in an Extremely Low-Birth-Weight Neonate. Am. J. Perinatol. Rep. 2017, 07, e134–e137. [Google Scholar] [CrossRef]
- Duijsters, C.E.; Halbertsma, F.J.; Kornelisse, R.F.; La Arents, N.; Andriessen, P. Recurring staphylococcal scalded skin syndrome in a very low birth weight infant: A case report. J. Med. Case Rep. 2009, 3, 7313. [Google Scholar] [CrossRef]
- Wolinsky, E.; Lipsitz, P.; Rammelkamp, C. Acquisition of staphylococci by newborns. Direct versus indirect transmission. Lancet 1960, 2, 620–622. [Google Scholar] [CrossRef] [PubMed]
- Gerber, S.I.; Jones, R.C.; Scott, M.V.; Price, J.S.; Dworkin, M.S.; Filippell, M.B.; Rearick, T.; Pur, S.L.; McAuley, J.B.; Lavin, M.A.; et al. Management of outbreaks of methicillin-resistant Staphylococcus aureus infection in the neonatal intensive care unit: A consensus statement. Infect. Control Hosp. Epidemiol. 2006, 27, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Rao, G.G.; Batura, R.; Nicholl, R.; Coogan, F.; Patel, B.; Bassett, P.; Kearns, A.M. Outbreak report of investigation and control of an outbreak of Panton-Valentine Leukocidin-positive methicillin-sensitive Staphylococcus aureus (PVL-MSSA) infection in neonates and mothers. BMC Infect. Dis. 2019, 19, 178. [Google Scholar]
- De Araujo, F.P.; Tinelli, M.; Battisti, A.; Ercoli, A.; Anesi, A.; Pantosti, A.; Monaco, M. An outbreak of skin infections in neonates due to a Staphylococcus aureus strain producing the exfoliative toxin A. Infection 2018, 46, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Lamanna, O.; Bongiorno, D.; Bertoncello, L.; Grandesso, S.; Mazzucato, S.; Pozzan, G.B.; Cutrone, M.; Chirico, M.; Baesso, F.; Brugnaro, P.; et al. Rapid containment of nosocomial transmission of a rare community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) clone, responsible for the Staphylococcal Scalded Skin Syndrome (SSSS). Ital. J. Pediatr. 2017, 43, 5. [Google Scholar] [CrossRef]
- Lee, H.; Kim, E.S.; Choi, C.; Seo, H.; Shin, M.; Bok, J.H.; Cho, J.E.; Kim, C.J.; Shin, J.W.; Kim, T.S.; et al. Outbreak among healthy newborns due to a new variant of USA300-related meticillin-resistant Staphylococcus aureus. J. Hosp. Infect. 2014, 87, 145–151. [Google Scholar] [CrossRef]
- Sanchini, A.; Spitoni, M.; Monaco, M.; Raglio, A.; Grigis, A.; Petrò, W.; Menchini, M.; Pesenti, A.; Goglio, A.; Pantosti, A. Outbreak of skin and soft tissue infections in a hospital newborn nursery in Italy due to community-acquired meticillin-resistant Staphylococcus aureus USA300 clone. J. Hosp. Infect. 2013, 83, 36–40. [Google Scholar] [CrossRef]
- Paranthaman, K.; Bentley, A.; Milne, L.M.; Kearns, A.; Loader, S.; Thomas, A.; Thompson, F.; Logan, M.; Newitt, S.; Puleston, R. Nosocomial outbreak of staphyloccocal scalded skin syndrome in neonates in England, December 2012 to March 2013. Eurosurveillance 2014, 19, 20880. [Google Scholar] [CrossRef]
- Alsubaie, S.; Bahkali, K.; Somily, A.M.; Alzamil, F.; Alrabiaah, A.; Alaska, A.; Alkhattaf, F.; Kambal, A.; Al-Qahtani, A.A.; Al-Ahdal, M.N. Nosocomial transmission of community-acquired methicillin-resistant Staphylococcus aureus in a well-infant nursery of a teaching hospital. Pediatr. Int. 2012, 54, 786–792. [Google Scholar] [CrossRef]
- Neylon, O.; O’Connell, N.H.; Slevin, B.; Powell, J.; Monahan, R.; Boyle, L.; Whyte, D.; Mannix, M.; McElligott, F.; Kearns, A.M.; et al. Neonatal staphylococcal scalded skin syndrome: Clinical and outbreak containment review. Eur. J. Pediatr. 2010, 169, 1503–1509. [Google Scholar] [CrossRef]
- Gould, I.M.; Girvan, E.K.; Browning, R.A.; Mackenzie, F.M.; Edwards, G.F.S. Report of a hospital neonatal unit outbreak of community-associated methicillin-resistant Staphylococcus aureus. Epidemiol. Infect. 2009, 137, 1242–1248. [Google Scholar] [CrossRef]
- Kurlenda, J.; Grinholc, M.; Krzysztoń-Russjan, J.; Wiśniewska, K. Epidemiological investigation of nosocomial outbreak of staphylococcal skin diseases in neonatal ward. Antonie Van Leeuwenhoek 2009, 95, 387–394. [Google Scholar] [CrossRef]
- James, L.; Gorwitz, R.J.; Jones, R.C.; Watson, J.T.; Hageman, J.C.; Jernigan, D.B.; Lord, Y.; Caballes, N.; Cortes, C.; Golash, R.G.; et al. Methicillin-resistant Staphylococcus aureus infections among healthy full-term newborns. Arch. Dis. Child. Fetal Neonatal. Ed. 2008, 93, F40–F44. [Google Scholar] [CrossRef]
- El Helali, N.; Carbonne, A.; Naas, T.; Kerneis, S.; Fresco, O.; Giovangrandi, Y.; Fortineau, N.; Nordmann, P.; Astagneau, P. Nosocomial outbreak of staphylococcal scalded skin syndrome in neonates: Epidemiological investigation and control. J. Hosp. Infect. 2005, 61, 130–138. [Google Scholar] [CrossRef]
- Weist, K.; Wendt, C.; Petersen, L.R.; Versmold, H.; Rüden, H. An outbreak of pyodermas among neonates caused by ultrasound gel contaminated with methicillin-susceptible Staphylococcus aureus. Infect. Control Hosp. Epidemiol. 2000, 21, 761–764. [Google Scholar] [CrossRef]
- Zafar, A.; Butler, R.; Reese, D.; Gaydos, L.; Mennonna, P. Use of 0.3% triclosan (Bacti-Stat) to eradicate an outbreak of methicillin-resistant Staphylococcus aureus in a neonatal nursery. Am. J. Infect. Control 1995, 23, 200–208. [Google Scholar] [CrossRef]
- Dave, J.; Reith, S.; Nash, J.Q.; Marples, R.R.; Dulake, C. A double outbreak of exfoliative toxin-producing strains of Staphylococcus aureus in a maternity unit. Epidemiol. Infect. 1994, 112, 103–114. [Google Scholar] [CrossRef][Green Version]
- Richardson, J.; Quoraishi, A.; Francis, B.; Marples, R. Beta-lactamase-negative, methicillin-resistant Staphylococcus aureus in a newborn nursery: Report of an outbreak and laboratory investigations. J. Hosp. Infect. 1990, 16, 109–121. [Google Scholar] [CrossRef]
- Dancer, S.; Simmons, N.; Poston, S.; Noble, W. Outbreak of staphylococcal scalded skin syndrome among neonates. J. Infect. 1988, 16, 87–103. [Google Scholar] [CrossRef]
- Kaplan, M.H.; Chmel, H.; Hsieh, H.C.; Stephens, A.; Brinsko, V. Importance of exfoliatin toxin A production by Staphylococcus aureus strains isolated from clustered epidemics of neonatal pustulosis. J. Clin. Microbiol. 1986, 23, 83–91. [Google Scholar] [CrossRef]
- Dowsett, E.; Petts, D.; Baker, S.; DeSaxe, M.; Coe, A.; Naidoo, J.; Noble, W. Analysis of an outbreak of staphylococcal scalded skin syndrome: Strategies for typing ‘non-typable’ strains. J. Hosp. Infect. 1984, 5, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Curran, J.P.; Al-Salihi, F.L. Neonatal staphylococcal scalded skin syndrome: Massive outbreak due to an unusual phage type. Pediatrics 1980, 66, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Faden, H.S.; Burke, J.P.; Glasgow, L.A.; Everett, J.R., 3rd. Nursery outbreak of scalded-skin syndrome. Scarlatiniform rash due to phage group I Staphylococcus aureus. Am. J. Dis. Child. 1976, 130, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Benson, P.F.; Rankin, G.L.; Rippey, J.J. An outbreak of exfoliative dermatitis of the newborn (Ritter’s disease) due to Staphylococcus aureus, phage-type 55/71. Lancet 1962, 1, 999–1002. [Google Scholar] [CrossRef] [PubMed]
- Howells, C.H.L.; Jones, H.E. Two outbreaks of neonatal skin sepsis caused by Staphylococcus aureus, phage type 71. Arch. Dis. Child. 1961, 36, 214–216. [Google Scholar] [CrossRef][Green Version]
- Rieger-Fackeldey, E.; Plano, L.; Krämer, A.; Schulze, A. Staphylococcal scalded skin syndrome related to an exfoliative toxin A- and B-producing strain in preterm infants. Eur. J. Pediatr. 2002, 161, 649–652. [Google Scholar] [CrossRef]
- Arora, P.; Kalra, V.K.; Rane, S.; McGrath, E.; Zegarra-Linares, R.; Chawla, S. Staphylococcal scalded skin syndrome in a preterm newborn presenting within first 24 h of life. BMJ Case Rep. 2011, 2011, bcr0820114733. [Google Scholar] [CrossRef]
- Tenenbaum, T.; Hoehn, T.; Hadzik, B.; Stannigel, H.; MacKenzie, C.R.; Mayatepek, E.; Schroten, H. Exchange transfusion in a preterm infant with hyperbilirubinemia, staphylococcal scalded skin syndrome (SSSS) and sepsis. Eur. J. Pediatr. 2006, 166, 733–735. [Google Scholar] [CrossRef]
- Hennigan, K.; Riley, C. Staphylococcal Scalded Skin Syndrome: A Case Review. Neonatal Netw. 2016, 35, 8–12. [Google Scholar] [CrossRef]
- Horner, A.; Hörner, R.; Salla, A.; Nunes, M.S.; Garzon, L.R.; Rampelotto, R.F.; Martini, R.; dos Santos, S.O.; Gindri, L.; de Abreu Rodrigues, M.; et al. Staphylococcal scalded skin syndrome in a premature newborn caused by methicillin-resistant Staphylococcus aureus: Case report. Sao Paulo Med. J. 2015, 133, 450–453. [Google Scholar] [CrossRef]
- Shi, D.; Ishii, S.; Sato, T.; Yamazaki, H.; Matsunaga, M.; Higuchi, W.; Takano, T.; Yabe, S.; Tanaka, K.; Yamamoto, T. Staphylococcal scalded skin syndrome in an extremely low-birth-weight neonate: Molecular characterization and rapid detection by multiplex and real-time PCR of methicillin-resistant Staphylococcus aureus. Pediatr. Int. 2011, 53, 211–217. [Google Scholar] [CrossRef]
- Hütten, M.; Heimann, K.; Baron, J.M.; Wenzl, T.G.; Merk, H.-F.; Ott, H. Staphylococcal scalded skin syndrome as a harbinger of late-onset staphylococcal septicaemia in a premature infant of very low birth weight. Acta Derm. Venereol. 2008, 88, 416–417. [Google Scholar]
- Coleman, J.C.; Dobson, N.R. Diagnostic dilemma: Extremely low birth weight baby with staphylococcal scalded-skin syndrome or toxic epidermal necrolysis. J. Perinatol. 2006, 26, 714–716. [Google Scholar] [CrossRef][Green Version]
- Makhoul, I.R.; Kassis, I.; Hashman, N.; Sujov, P. Staphylococcal scalded-skin syndrome in a very low birth weight premature infant. Pediatrics 2001, 108, E16. [Google Scholar] [CrossRef]
- Chao, S.C.; Richard, G.; Lee, J.Y. Netherton syndrome: Report of two Taiwanese siblings with staphylococcal scalded skin syndrome and mutation of SPINK5. Br. J. Dermatol. 2005, 152, 159–165. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nusman, C.M.; Blokhuis, C.; Pajkrt, D.; Visser, D.H. Staphylococcal Scalded Skin Syndrome in Neonates: Case Series and Overview of Outbreaks. Antibiotics 2023, 12, 38. https://doi.org/10.3390/antibiotics12010038
Nusman CM, Blokhuis C, Pajkrt D, Visser DH. Staphylococcal Scalded Skin Syndrome in Neonates: Case Series and Overview of Outbreaks. Antibiotics. 2023; 12(1):38. https://doi.org/10.3390/antibiotics12010038
Chicago/Turabian StyleNusman, Charlotte M., Charlotte Blokhuis, Dasja Pajkrt, and Douwe H. Visser. 2023. "Staphylococcal Scalded Skin Syndrome in Neonates: Case Series and Overview of Outbreaks" Antibiotics 12, no. 1: 38. https://doi.org/10.3390/antibiotics12010038
APA StyleNusman, C. M., Blokhuis, C., Pajkrt, D., & Visser, D. H. (2023). Staphylococcal Scalded Skin Syndrome in Neonates: Case Series and Overview of Outbreaks. Antibiotics, 12(1), 38. https://doi.org/10.3390/antibiotics12010038