


Successful Control of an Outbreak by Phenotypically Identified Extended-Spectrum Beta-Lactamase–Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit

 ,
,  ,
,
Abstract
:1. Introduction
2. Results
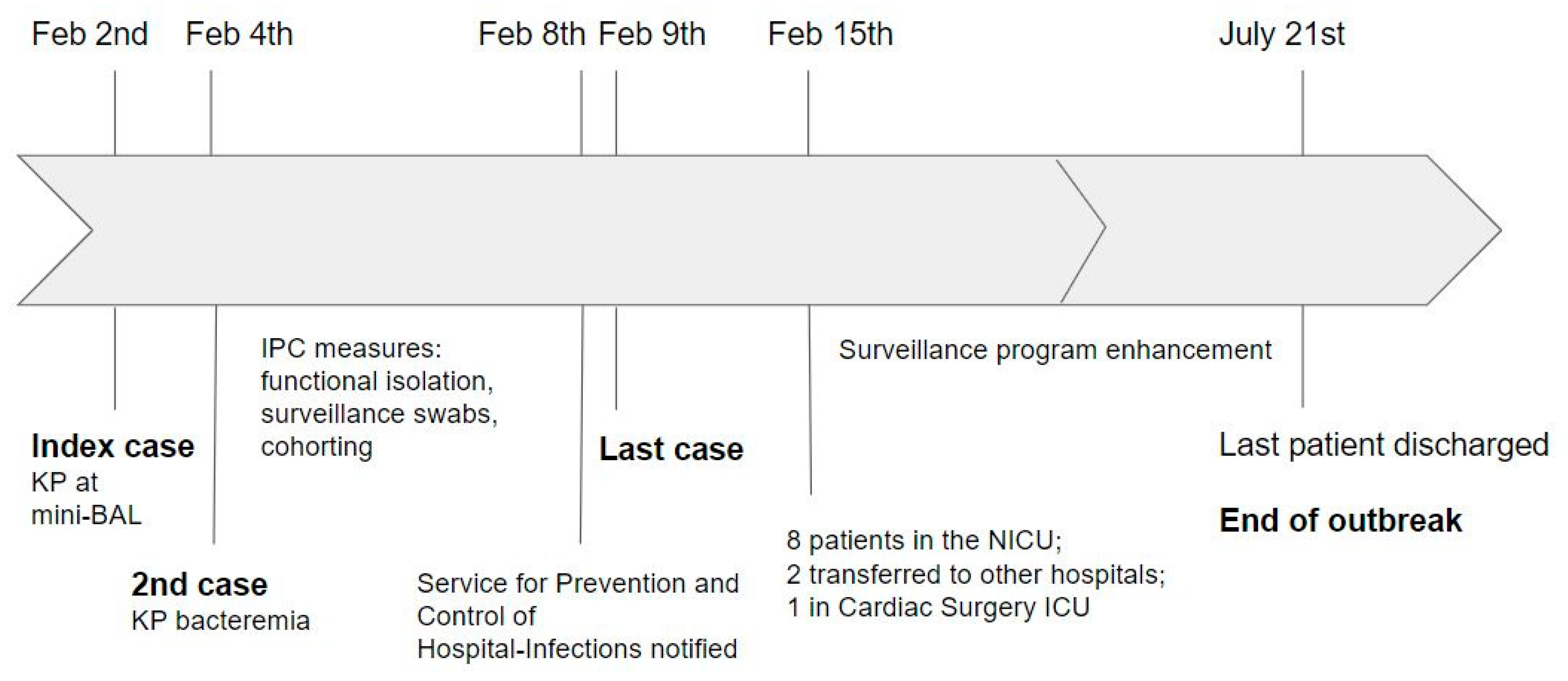
2.1. Outbreak Management
2.2. Reinforcement and Enhancement of Infection Control Program
2.3. Treatment
2.4. Antibiotic Resistance and Molecular Characteristics
2.5. Environmental and Staff Surveillance
3. Materials and Methods
3.1. Study Design, Setting, and Population
3.2. Case Definition and Inclusion Criteria
3.3. Data Collection
3.4. Outcomes
3.5. Outbreak Management Strategies and Treatment
3.6. Identification of ESBL Isolates in Cultures and Antimicrobial Susceptibility Testing
3.7. Genotyping Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polin, R.A.; Denson, S.; Brady, M.T. Committee on Fetus and Newborn, Committee on Infectious Diseases. Strategies for prevention of health care-associated infections in the NICU. Pediatrics 2012, 129, e1085–e1089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cailes, B.; Vergnano, S.; Kortsalioudaki, C.; Heath, P.; Sharland, M. The current and future roles of neonatal infection surveillance programmes in combating antimicrobial resistance. Early Hum. Dev. 2015, 91, 613–618. [Google Scholar] [CrossRef] [PubMed]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Pant, S.; Brower, C.; Røttingen, J.A.; Klugman, K.; Davies, S. Access to effective antimicrobials: A worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef]
- Janda, J.M.; Abbott, S.L. The Changing Face of the Family Enterobacteriaceae (Order: “Enterobacterales”): New Members, Taxonomic Issues, Geographic Expansion, and New Diseases and Disease Syndromes. Clin. Microbiol. Rev. 2021, 34, e00174-20. [Google Scholar] [CrossRef] [PubMed]
- Folgori, L.; Bielicki, J.; Heath, P.T.; Sharland, M. Antimicrobial-resistant Gram-negative infections in neonates: Burden of disease and challenges in treatment. Curr. Opin. Infect. Dis. 2017, 30, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Almogbel, M.; Altheban, A.; Alenezi, M.; Al-Motair, K.; Menezes, G.A.; Elabbasy, M.; Hammam, S.; Hays, J.P.; Khan, M.A. CTX-M-15 Positive Escherichia coli and Klebsiella pneumoniae Outbreak in the Neonatal Intensive Care Unit of a Maternity Hospital in Ha’il, Saudi Arabia. Infect. Drug Resist. 2021, 14, 2843–2849. [Google Scholar] [CrossRef]
- Frenk, S.; Rakovitsky, N.; Temkin, E.; Schechner, V.; Cohen, R.; Kloyzner, B.S.; Schwaber, M.J.; Solter, E.; Cohen, S.; Stepansky, S.; et al. Investigation of Outbreaks of Extended-Spectrum Beta-Lactamase-Producing Klebsiella Pneumoniae in Three Neonatal Intensive Care Units Using Whole Genome Sequencing. Antibiotics 2020, 9, 705. [Google Scholar] [CrossRef]
- Shao, L.; Yao, B.; Yang, J.; Li, X.; Ye, K.; Zhang, Y.; Wang, C. Characterization of a multidrug-resistant Klebsiella pneumoniae ST3330 clone responsible for a nosocomial outbreak in a neonatal intensive care unit. Ann. Palliat. Med. 2020, 9, 1092–1102. [Google Scholar] [CrossRef]
- Wang, Y.; Luo, C.; Du, P.; Hu, J.; Zhao, X.; Mo, D.; Du, X.; Xu, X.; Li, M.; Lu, H.; et al. Genomic Epidemiology of an Outbreak of Klebsiella pneumoniae ST471 Producing Extended-Spectrum β-Lactamases in a Neonatal Intensive Care Unit. Infect. Drug Resist. 2020, 13, 1081–1090. [Google Scholar] [CrossRef] [Green Version]
- Chapman, P.; Forde, B.M.; Roberts, L.W.; Bergh, H.; Vesey, D.; Jennison, A.V.; Moss, S.; Paterson, D.L.; Beatson, S.A.; Harris, P.N.A. Genomic Investigation Reveals Contaminated Detergent as the Source of an Extended-Spectrum-β-Lactamase-Producing Klebsiella michiganensis Outbreak in a Neonatal Unit. J. Clin. Microbiol. 2020, 58, e01980-19. [Google Scholar] [CrossRef]
- Baek, E.H.; Kim, S.E.; Kim, S.; Lee, S.; Cho, O.H.; In Hong, S.; Shin, J.H.; Hwang, I. Successful control of an extended-spectrum beta-lactamase-producing Klebsiella pneumoniae ST307 outbreak in a neonatal intensive care unit. BMC Infect. Dis. 2020, 20, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadot, L.; Bruguière, H.; Jumas-Bilak, E.; Didelot, M.N.; Masnou, A.; de Barry, G.; Cambonie, G.; Parer, S.; Romano-Bertrand, S. Extended spectrum beta-lactamase-producing Klebsiella pneumoniae outbreak reveals incubators as pathogen reservoir in neonatal care center. Eur. J. Pediatr. 2019, 178, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Peltier, F.; Choquet, M.; Decroix, V.; Adjidé, C.C.; Castelain, S.; Guiheneuf, R.; Pluquet, E. Characterization of a multidrug-resistant Klebsiella pneumoniae ST607-K25 clone responsible for a nosocomial outbreak in a neonatal intensive care unit. J. Med. Microbiol. 2019, 68, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Corbella, M.; Caltagirone, M.; Gaiarsa, S.; Mariani, B.; Sassera, D.; Bitar, I.; Muzzi, A.; Migliavacca, R.; Scudeller, L.; Stronati, M.; et al. Characterization of an Outbreak of Extended-Spectrum β-Lactamase-Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit in Italy. Microb. Drug Resist. 2018, 24, 1128–1136. [Google Scholar] [CrossRef]
- Haller, S.; Eller, C.; Hermes, J.; Kaase, M.; Steglich, M.; Radonić, A.; Dabrowski, P.W.; Nitsche, A.; Pfeifer, Y.; Werner, G.; et al. What caused the outbreak of ESBL-producing Klebsiella pneumoniae in a neonatal intensive care unit, Germany 2009 to 2012? Reconstructing transmission with epidemiological analysis and whole-genome sequencing. BMJ Open 2015, 5, e007397. [Google Scholar] [CrossRef] [Green Version]
- Stapleton, P.J.; Murphy, M.; McCallion, N.; Brennan, M.; Cunney, R.; Drew, R.J. Outbreaks of extended spectrum beta-lactamase-producing Enterobacteriaceae in neonatal intensive care units: A systematic review. ADC Fetal Neonatal Ed. 2016, 101, 72–78. [Google Scholar] [CrossRef]
- Giuffrè, M.; Bonura, C.; Geraci, D.M.; Saporito, L.; Catalano, R.; Di Noto, S.; Nociforo, F.; Corsello, G.; Mammina, C. Successful control of an outbreak of colonization by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae sequence type 258 in a neonatal intensive care unit, Italy. J. Hosp. Infect. 2013, 85, 233–236. [Google Scholar] [CrossRef] [Green Version]
- Cantey, J.B.; Sreeramoju, P.; Jaleel, M.; Treviño, S.; Gander, R.; Hynan, L.; Hill, J.; Brown, C.; Chung, W.; Siegel, J.D.; et al. Prompt Control of an Outbreak Caused by Extended-Spectrum β-Lactamase–Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit. J. Pediatr. 2013, 163, 672–679. [Google Scholar] [CrossRef]
- Gastmeier, P.; Loui, A.; Stamm-Balderjahn, S.; Hansen, S.; Zuschneid, I.; Sohr, D.; Behnke, M.; Obladen, M.; Vonberg, R.-P.; Rüden, H. Outbreaks in neonatal intensive care units—They are not like others. Am. J. Infect. Control 2007, 35, 172–176. [Google Scholar] [CrossRef]
- Brooks, B.; Olm, M.R.; Firek, B.A.; Baker, R.; Geller-McGrath, D.; Reimer, S.R.; Soenjoyo, K.R.; Yip, J.S.; Dahan, D.; Thomas, B.C.; et al. The developing premature infant gut microbiome is a major factor shaping the microbiome of neonatal intensive care unit rooms. Microbiome 2018, 6, 112. [Google Scholar] [CrossRef]
- A Clock, S.; Ferng, Y.-H.; Tabibi, S.; Alba, L.; Patel, S.J.; Jia, H.; DeLaMora, P.; Perlman, J.M.; A Paul, D.; Zaoutis, T.; et al. Colonization With Antimicrobial-Resistant Gram-Negative Bacilli at Neonatal Intensive Care Unit Discharge. J. Pediatr. Infect. Dis. Soc. 2016, 6, 219–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordberg, V.; Jonsson, K.; Giske, C.G.; Iversen, A.; Aspevall, O.; Jonsson, B.; Camporeale, A.; Norman, M.; Navér, L. Neonatal intestinal colonization with extended-spectrum β-lactamase-producing Enterobacteriaceae-a 5-year follow-up study. Clin. Microbiol. Infect. Dis. 2018, 24, 1004–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibrahim, N.A.; Bakry, M.M.; Tahir, N.A.M.; Zaini, N.R.M.; Shah, N.M. A Prospective Cohort Study of Factors Associated with Empiric Antibiotic De-escalation in Neonates Suspected with Early Onset Sepsis (EOS). Pediatr. Drugs 2020, 22, 321–330. [Google Scholar] [CrossRef] [PubMed]
- Folgori, L.; Tersigni, C.; Hsia, Y.; Kortsalioudaki, C.; Heath, P.; Sharland, M.; Bielicki, J. The relationship between Gram-negative colonization and bloodstream infections in neonates: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2018, 24, 251–257. [Google Scholar] [CrossRef] [Green Version]
- Seidel, J.; Haller, S.; Eckmanns, T.; Harder, T. Routine screening for colonization by Gram-negative bacteria in neonates at intensive care units for the prediction of sepsis: Systematic review and meta-analysis. J. Hosp. Infect. 2018, 99, 367–380. [Google Scholar] [CrossRef]
- Dicker, R.C.; Coronado, F.; Koo, D. Epidemic Disease Occurrence. In Principles of Epidemiology in Public Health Practice: An Introduction to Applied Epidemiology and Biostatistics, 3rd ed.; US Department of Health and Human Services: Atlanta, GA, USA, 2006. [Google Scholar]
- Sood, G.; Perl, T.M. Outbreaks in Health Care Settings. Infect. Dis. Clin. N. Am. 2016, 30, 661–687. [Google Scholar] [CrossRef]
- Anthony, M.; Bedford-Russell, A.; Cooper, T.; Fry, C.; Heath, P.; Kennea, N.; McCartney, M.; Patel, B.; Pollard, T.; Sharland, M.; et al. Managing and preventing outbreaks of Gram-negative infections in UK neonatal units: Table 1. Arch. Dis. Child. -Fetal Neonatal Ed. 2013, 98, F549–F553. [Google Scholar] [CrossRef]
- Decembrino, L.; Maini, A.; Decembrino, N.; Maggi, I.; Lacerenza, S. Management of outbreaks in neonatal intensive care units. Early Hum. Dev. 2014, 90, S54–S56. [Google Scholar] [CrossRef]
- World Health Organization. Implementation Manual to Prevent and Control the Spread of Carbapenem-Resistant Organisms at the National and Health Care Facility Level; World Health Organization: Geneva, Switzerland, 2019; (WHO/UHC/SDS/2019.6). Licence: CC BY-NC-SA 3.0 IGO.
- Mukherjee, S.; Mitra, S.; Dutta, S.; Basu, S. Neonatal Sepsis: The Impact of Carbapenem-Resistant and Hypervirulent Klebsiella pneumoniae. Front. Med. 2021, 8, 634349. [Google Scholar] [CrossRef]
- Marando, R.; Seni, J.; Mirambo, M.M.; Falgenhauer, L.; Moremi, N.; Mushi, M.; Kayange, N.; Manyama, F.; Imirzalioglu, C.; Chakraborty, T.; et al. Predictors of the extended-spectrum-beta lactamases producing Enterobacteriaceae neonatal sepsis at a tertiary hospital, Tanzania. Int. J. Med. Microbiol. 2018, 308, 803–811. [Google Scholar] [CrossRef]
- Fabbri, G.; Panico, M.; Dallolio, L.; Suzzi, R.; Ciccia, M.; Sandri, F.; Farruggia, P. Outbreak of Ampicillin/Piperacillin-Resistant Klebsiella Pneumoniae in a Neonatal Intensive Care Unit (NICU): Investigation and Control Measures. Int. J. Environ. Res. Public Heal. 2013, 10, 808–815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rettedal, S.; Löhr, I.H.; Natås, O.; Giske, C.G.; Sundsfjord, A.; Øymar, K. First outbreak of extended-spectrum β-lactamase-producing Klebsiella pneumoniae in a Norwegian neonatal intensive care unit; associated with contaminated breast milk and resolved by strict cohorting. APMIS 2012, 120, 612–621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Snyder, G.M. Introduction to Transmission of Infection: Potential Agents Transmitted by Endoscopy. Gastrointest. Endosc. Clin. New Am. 2020, 30, 611–618. [Google Scholar] [CrossRef] [PubMed]
- Piperaki, E.-T.; Syrogiannopoulos, G.A.; Tzouvelekis, L.S.; Daikos, G.L. Klebsiella pneumoniae: Virulence, Biofilm and Antimicrobial Resistance. Pediatr. Infect. Dis. J. 2017, 36, 1002–1005. [Google Scholar] [CrossRef]
- Ransjö, U.; Lytsy, B.; Melhus, Å.; Aspevall, O.; Artinger, C.; Eriksson, B.-M.; Günther, G.; Hambraeus, A. Hospital outbreak control requires joint efforts from hospital management, microbiology and infection control. J. Hosp. Infect. 2010, 76, 26–31. [Google Scholar] [CrossRef]
- Bushuven, S.; Dietz, A.; Bushuven, S.; Dettenkofer, M.; Langer, T. Interprofessional perceptions and emotional impact of multidrug-resistant organisms: A qualitative study. Am. J. Infect. Control. 2019, 47, 876–882. [Google Scholar] [CrossRef]
- European Center for Disease Prevention and Control. Economic Evaluations of Interventions to Prevent Healthcare-Associated Infections. Stockholm: ECDC. 2017. Available online: https://www.ecdc.europa.eu/en/publications-data/economic-evaluations-interventions-prevent-healthcare-associated-infections (accessed on 30 September 2022).
- Storr, J.; Twyman, A.; Zingg, W.; Damani, N.; Kilpatrick, C.; Reilly, J.; Price, L.; Egger, M.; Grayson, M.L.; Kelley, E.; et al. WHO Guidelines Development Group. Core components for effective infection prevention and control programmes: New WHO evidence-based recommendations. Antimicrob. Resist. Infect. Control. 2017, 6, 6. [Google Scholar] [CrossRef] [Green Version]
- Bauer, M.S.; Damschroder, L.J.; Hagedorn, H.; Smith, J.; Kilbourne, A.M. An introduction to implementation science for the non-specialist. BMC Psychol. 2015, 3, 1–12. [Google Scholar] [CrossRef]


{kind=link}
| Patient | MLST Scheme | ST Clone | Standard Housekeeping Loci | Type of Specimen | Antimicrobial Resistance Phenotype | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| gapA | infB | mdh | pgi | phoE | rpoB | tonB | |||||
| 1 | K. pneumoniae | ST 45 | 2 | 1 | 1 | 6 | 7 | 1 | 12 | Mini-BAL, pharyngeal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin |
| 2 | Blood culture, pharyngeal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 3 | Blood culture, pharyngeal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin, Piperacillin/tazobactam | |||||||||
| 4 | Cutaneous and pharyngeal swab, blood culture | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 5 | Pharyngeal swab, blood culture | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 6 | Pharyngeal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 7 | Rectal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin, piperacillin/tazobactam, amikacin | |||||||||
| 8 | Rectal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin, piperacillin/tazobactam, amikacin | |||||||||
| 9 | Rectal and pharyngeal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 10 | Rectal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 11 | Rectal and pharyngeal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), ciprofloxacin, gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 12 | Rectal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
| 13 | Rectal swab | Amoxicillin-clavulanic acid, cephalosporins (except ceftazidime/avibactam and ceftolozane/tazobactam), gentamicin, trimethoprim/sulphamethoxazole, tobramycin | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priante, E.; Minotti, C.; Contessa, C.; Boschetto, M.; Stano, P.; Dal Bello, F.; De Canale, E.; Lolli, E.; Baldo, V.; Baraldi, E.; et al. Successful Control of an Outbreak by Phenotypically Identified Extended-Spectrum Beta-Lactamase–Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit. Antibiotics 2022, 11, 1649. https://doi.org/10.3390/antibiotics11111649
Priante E, Minotti C, Contessa C, Boschetto M, Stano P, Dal Bello F, De Canale E, Lolli E, Baldo V, Baraldi E, et al. Successful Control of an Outbreak by Phenotypically Identified Extended-Spectrum Beta-Lactamase–Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit. Antibiotics. 2022; 11(11):1649. https://doi.org/10.3390/antibiotics11111649
Chicago/Turabian StylePriante, Elena, Chiara Minotti, Cristina Contessa, Margherita Boschetto, Paola Stano, Federico Dal Bello, Ettore De Canale, Elisabetta Lolli, Vincenzo Baldo, Eugenio Baraldi, and et al. 2022. "Successful Control of an Outbreak by Phenotypically Identified Extended-Spectrum Beta-Lactamase–Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit" Antibiotics 11, no. 11: 1649. https://doi.org/10.3390/antibiotics11111649
APA StylePriante, E., Minotti, C., Contessa, C., Boschetto, M., Stano, P., Dal Bello, F., De Canale, E., Lolli, E., Baldo, V., Baraldi, E., & Donà, D. (2022). Successful Control of an Outbreak by Phenotypically Identified Extended-Spectrum Beta-Lactamase–Producing Klebsiella pneumoniae in a Neonatal Intensive Care Unit. Antibiotics, 11(11), 1649. https://doi.org/10.3390/antibiotics11111649