
Antimicrobial Efficacy of an Ultraviolet-C Device against Microorganisms Related to Contact Lens Adverse Events


Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Ultraviolet C device:
4.2. Contact lenses and Lens cases
4.3. Strains and microbial conditions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stellwagen, A.; MacGregor, C.; Kung, R.; Konstantopoulos, A.; Hossain, P. Personal hygiene risk factors for contact lens-related microbial keratitis. BMJ Open Ophthalmol. 2020, 5, e000476. [Google Scholar] [CrossRef] [PubMed]
- Dutta, D.; Willcox, M.D.P. Antimicrobial contact lenses and lens cases: A review. Eye Contact Lens 2014, 40, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Shi, G.; Liu, H.; Jiang, X.; Deng, J.; Zhu, C.; Yuan, Y.; Ke, B. Microbial Contamination of Rigid Gas Permeable (RGP) Trial Lenses and Lens Cases in China. Curr. Eye Res. 2020, 45, 550–555. [Google Scholar] [CrossRef]
- Stapleton, F.; Keay, L.; Edwards, K.; Naduvilath, T.; Dart, J.K.; Brian, G.; Holden, B.A. The Incidence of Contact Lens–Related Microbial Keratitis in Australia. Ophthalmology 2008, 115, 1655–1662. [Google Scholar] [CrossRef] [PubMed]
- Sankaridurg, P.R.; Sharma, S.; Willcox, M.; Naduvilath, T.J.; Sweeney, D.F.; Holden, B.A.; Rao, G.N. Bacterial colonization of disposable soft contact lenses is greater during corneal infiltrative events than during asymptomatic extended lens wear. J. Clin. Microbiol. 2000, 38, 4420–4424. [Google Scholar] [CrossRef] [Green Version]
- Brewitt, H. Contact lenses. Infections and hygiene. Ophthalmologe 1997, 94, 311–316. [Google Scholar] [CrossRef]
- Chalmers, R.L.; Hickson-Curran, S.B.; Keay, L.; Gleason, W.J.; Albright, R. Rates of Adverse Events With Hydrogel and Silicone Hydrogel Daily Disposable Lenses in a Large Postmarket Surveillance Registry: The TEMPO Registry. Investig. Opthalmol. Vis. Sci. 2015, 56, 654–663. [Google Scholar] [CrossRef] [Green Version]
- Ting, D.S.J.; Ho, C.S.; Deshmukh, R.; Said, D.G.; Dua, H.S. Infectious keratitis: An update on epidemiology, causative microorganisms, risk factors, and antimicrobial resistance. Eye 2021, 35, 1084–1101. [Google Scholar] [CrossRef]
- Dai, T.; Vrahas, M.S.; Murray, C.K.; Hamblin, M.R. Ultraviolet C irradiation: An alternative antimicrobial approach to localized infections? Expert Rev. Anti-Infect. Ther. 2012, 10, 185–195. [Google Scholar] [CrossRef] [Green Version]
- Gurzadyan, G.G.; Görner, H.; Schulte-Frohlinde, D. Ultraviolet (193, 216 and 254 nm) Photoinactivation of Escherichia coli Strains with Different Repair Deficiencies. Radiat. Res. 1995, 141, 244. [Google Scholar] [CrossRef]
- Chang, J.C.; Ossoff, S.F.; Lobe, D.C.; Dorfman, M.H.; Dumais, C.M.; Qualls, R.G.; Johnson, J.D. UV inactivation of pathogenic and indicator microorganisms. Appl. Environ. Microbiol. 1985, 49, 1361–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gritz, D.C.; Lee, T.Y.; McDonnell, P.J.; Shih, K.; Baron, N. Ultraviolet radiation for the sterilization of contact lenses. CLAO J. 1990, 16, 294–298. [Google Scholar] [PubMed]
- Harris, M.G.; Fluss, L.; Lem, A.; Leong, H. Ultraviolet Disinfection of Contact Lenses. Optom. Vis. Sci. 1993, 70, 839–842. [Google Scholar] [CrossRef] [PubMed]
- Lonnen, J.; Putt, K.S.; Kernick, E.R.; Lakkis, C.; May, L.; Pugh, R.B. The Efficacy of Acanthamoeba Cyst Kill and Effects Upon Contact Lenses of a Novel Ultraviolet Lens Disinfection System. Am. J. Ophthalmol. 2014, 158, 460–468.e2. [Google Scholar] [CrossRef]
- Admoni, M.M.; Bartolomei, A.; Qureshi, M.N.; Bottone, E.J.; Asbell, P.A. Disinfection Efficacy in an Integrated Ultraviolet Light Contact Lens Care System. Eye Contact Lens Sci. Clin. Pract. 1994, 20, 246–248. [Google Scholar] [CrossRef]
- Choate, W.; Fontana, F.; Potter, J.; Schachet, J.; Shaw, R.; Soulsby, M.; White, E. Evaluation of the PuriLens contact lens care system: An automatic care system incorporating UV disinfection and hydrodynamic shear cleaning. CLAO J. 2000, 26, 134–140. [Google Scholar]
- Conner-Kerr, T.; Sullivan, P.K.; Gaillard, J.; Franklin, M.; Jones, R.M. The effects of ultraviolet radiation on antibiotic-resistant bacteria in vitro. Ostomy Wound Manag. 1998, 44, 50–56. [Google Scholar]
- Dean, S.J.; Petty, A.; Swift, S.; McGhee, J.J.; Sharma, A.; Shah, S.; Craig, J.P. Efficacy and safety assessment of a novel ultraviolet C device for treating corneal bacterial infections. Clin. Exp. Ophthalmol. 2011, 39, 156–163. [Google Scholar] [CrossRef]
- Thai, T.P.; Keast, D.; Campbell, K.; Woodbury, M.G.; Houghton, P. Effect of ultraviolet light C on bacterial colonization in chronic wounds. Ostomy Wound Manag. 2005, 51, 32–45. [Google Scholar]
- Guridi, A.; Sevillano, E.; de la Fuente, I.; Mateo, E.; Eraso, E.; Quindós, G. Disinfectant Activity of A Portable Ultraviolet C Equipment. Int. J. Environ. Res. Public Health 2019, 16, 4747. [Google Scholar] [CrossRef] [Green Version]
- Umezawa, K.; Asai, S.; Inokuchi, S.; Miyachi, H. A Comparative Study of the Bactericidal Activity and Daily Disinfection Housekeeping Surfaces by a New Portable Pulsed UV Radiation Device. Curr. Microbiol. 2012, 64, 581–587. [Google Scholar] [CrossRef]
- Bentley, J.J.; Santoro, D.; Gram, D.W.; Dujowich, M.; Marsella, R. Can ultraviolet light C decrease the environmental burden of antimicrobial-resistant and -sensitive bacteria on textiles? Vet. Dermatol. 2016, 27, 457-e121. [Google Scholar] [CrossRef] [PubMed]
- Dutta, D.; Cole, N.; Willcox, M. Factors influencing bacterial adhesion to contact lenses. Mol. Vis. 2012, 18, 14–21. [Google Scholar]
- Willcox, M.D.P.; Chen, R.; Kalaiselvan, P.; Yasir, M.; Rasul, R.; Kumar, N.; Dutta, D. The Development of an Antimicrobial Contact Lens—From the Laboratory to the Clinic. Curr. Protein Pept. Sci. 2020, 21, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Szczotka-Flynn, L.B.; Pearlman, E.; Ghannoum, M. Microbial Contamination of Contact Lenses, Lens Care Solutions, and Their Accessories: A Literature Review. Eye Contact Lens Sci. Clin. Pract. 2010, 36, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Yasir, M.; Dutta, D.; Willcox, M.D. Activity of Antimicrobial Peptides and Ciprofloxacin against Pseudomonas aeruginosa Biofilms. Molecules 2020, 25, 3843. [Google Scholar] [CrossRef] [PubMed]
- Casciaro, B.; Dutta, D.; Loffredo, M.R.; Marcheggiani, S.; McDermott, A.M.; Willcox, M.D.; Mangoni, M.L. Esculentin-1a derived peptides kill Pseudomonas aeruginosa biofilm on soft contact lenses and retain antibacterial activity upon immobilization to the lens surface. Biopolymers 2017. [Google Scholar] [CrossRef]
- Dutta, D.; Willcox, M.D. A Laboratory Assessment of Factors That Affect Bacterial Adhesion to Contact Lenses. Biology 2013, 2, 1268–1281. [Google Scholar] [CrossRef] [Green Version]
- Iyer, S.A.; Tuli, S.S.; Wagoner, R.C. Fungal Keratitis: Emerging Trends and Treatment Outcomes. Eye Contact Lens Sci. Clin. Pract. 2006, 32, 267–271. [Google Scholar] [CrossRef] [Green Version]
- Fleming, D.; Rumbaugh, K.P. Approaches to Dispersing Medical Biofilms. Microorganisms 2017, 5, 15. [Google Scholar] [CrossRef]
- Wu, Y.T.-Y.; Willcox, M.; Zhu, H.; Stapleton, F. Contact lens hygiene compliance and lens case contamination: A review. Contact Lens Anterior Eye 2015, 38, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Dutta, D.; Cole, N.; Kumar, N.; Willcox, M. Broad Spectrum Antimicrobial Activity of Melimine Covalently Bound to Contact Lenses. Investig. Opthalmol. Vis. Sci. 2013, 54, 175–182. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
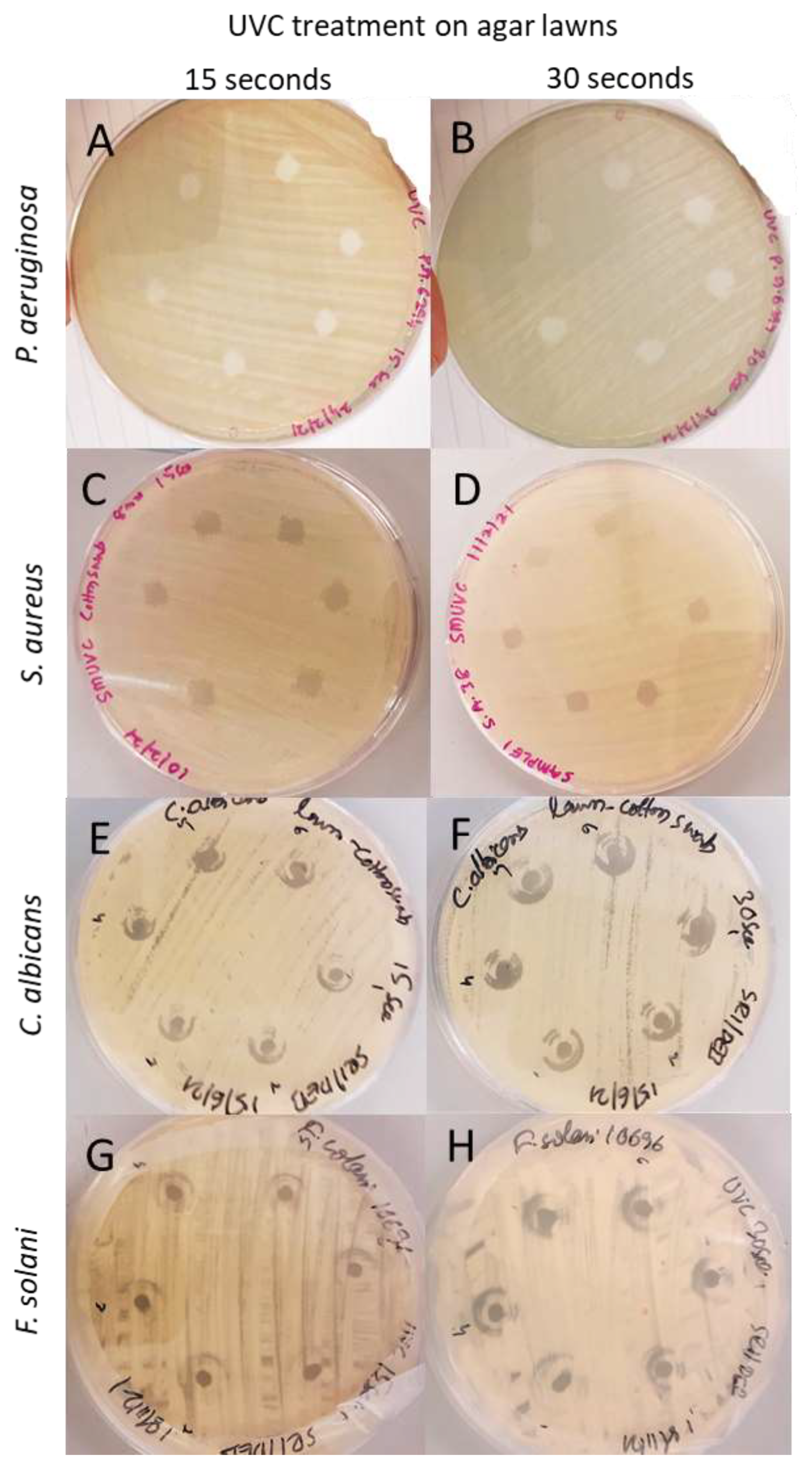
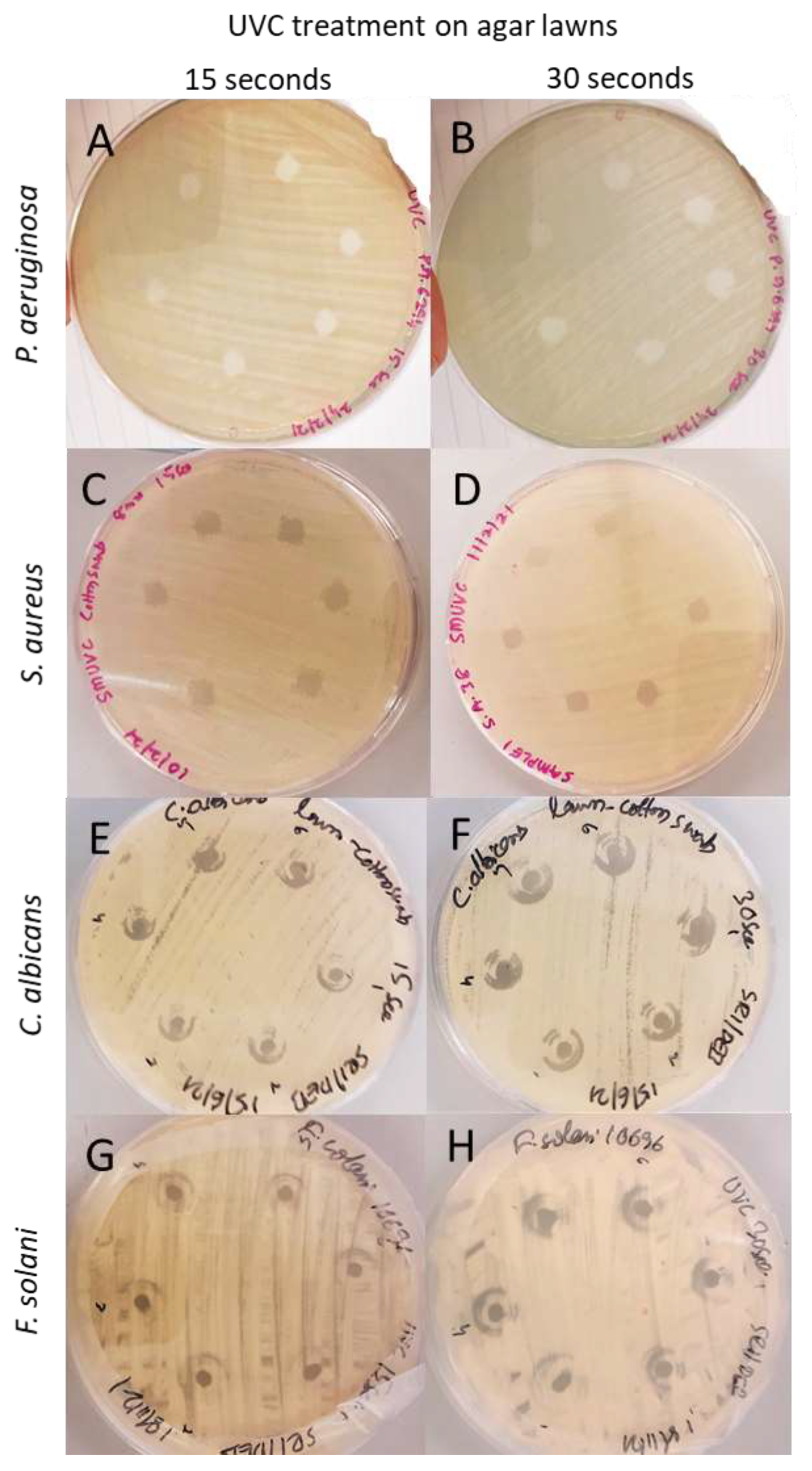
| Microorganisms | 15 s Exposure | 30 s Exposure |
|---|---|---|
| P. aeruginosa 6294 | 7.2 ± 0.3 | 7.5 ± 0.4 |
| S. aureus 38 | 6.9 ± 0.3 | 7.1 ± 0.4 |
| C. albicans ATCC 76615 | 5.5 ± 0.4 | 5.9 ± 0.2 |
| F. solani ATCC 10696 | 5.0 ± 0.4 | 5.8 ± 0.5 |
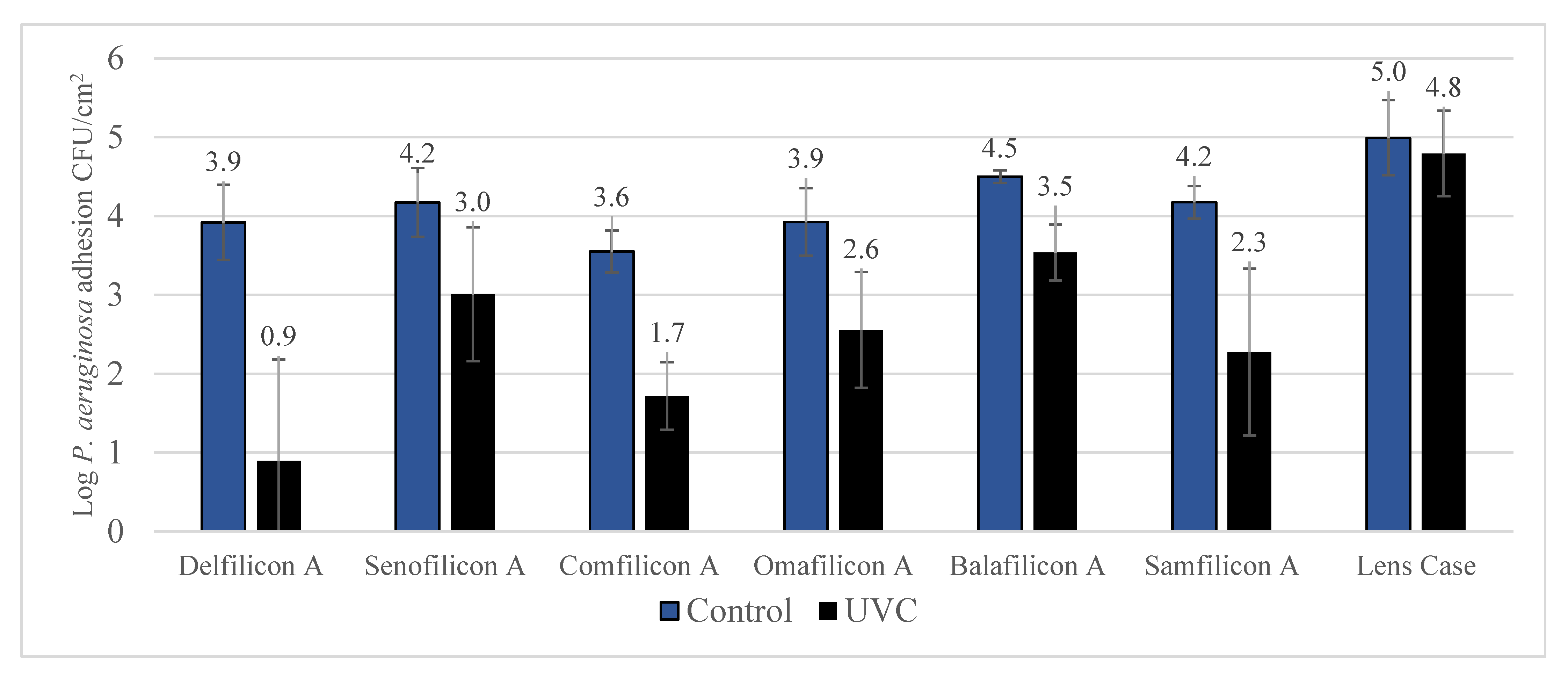
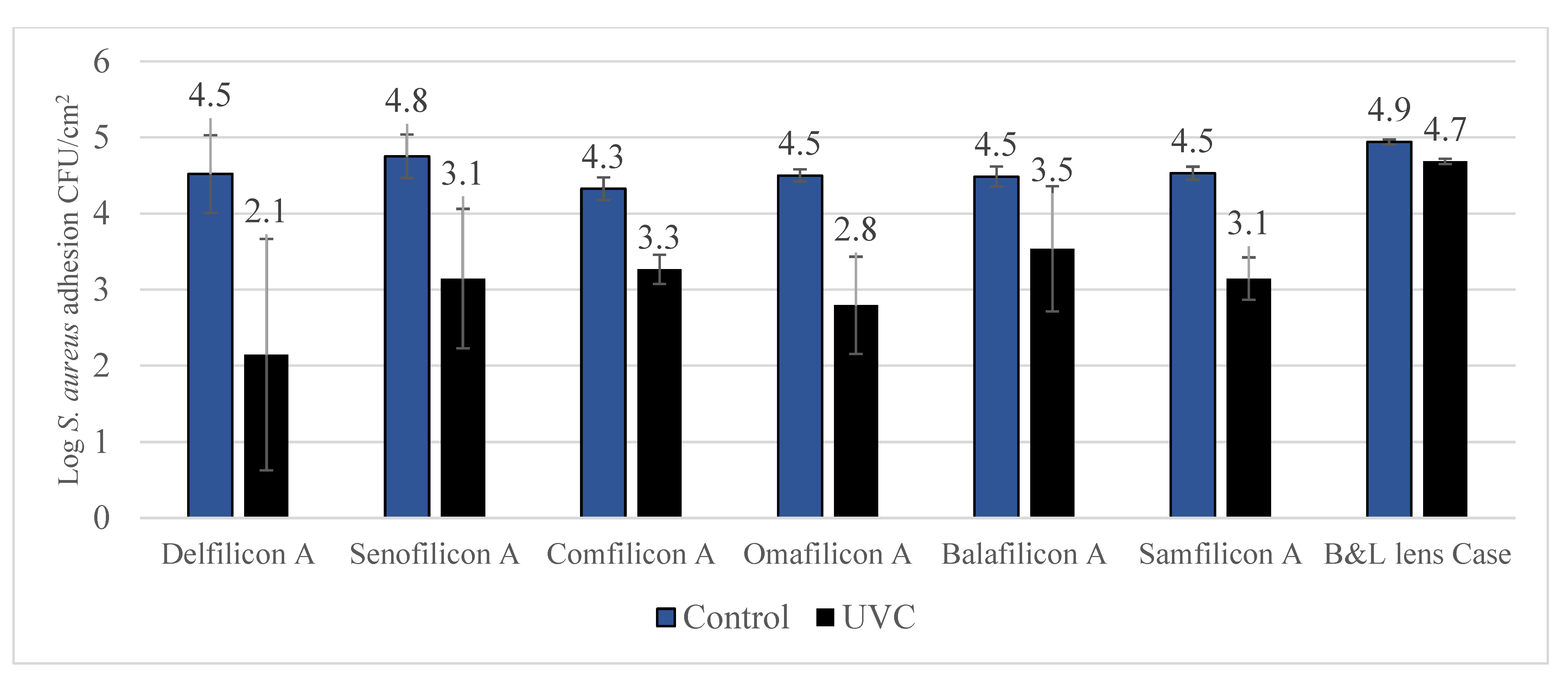
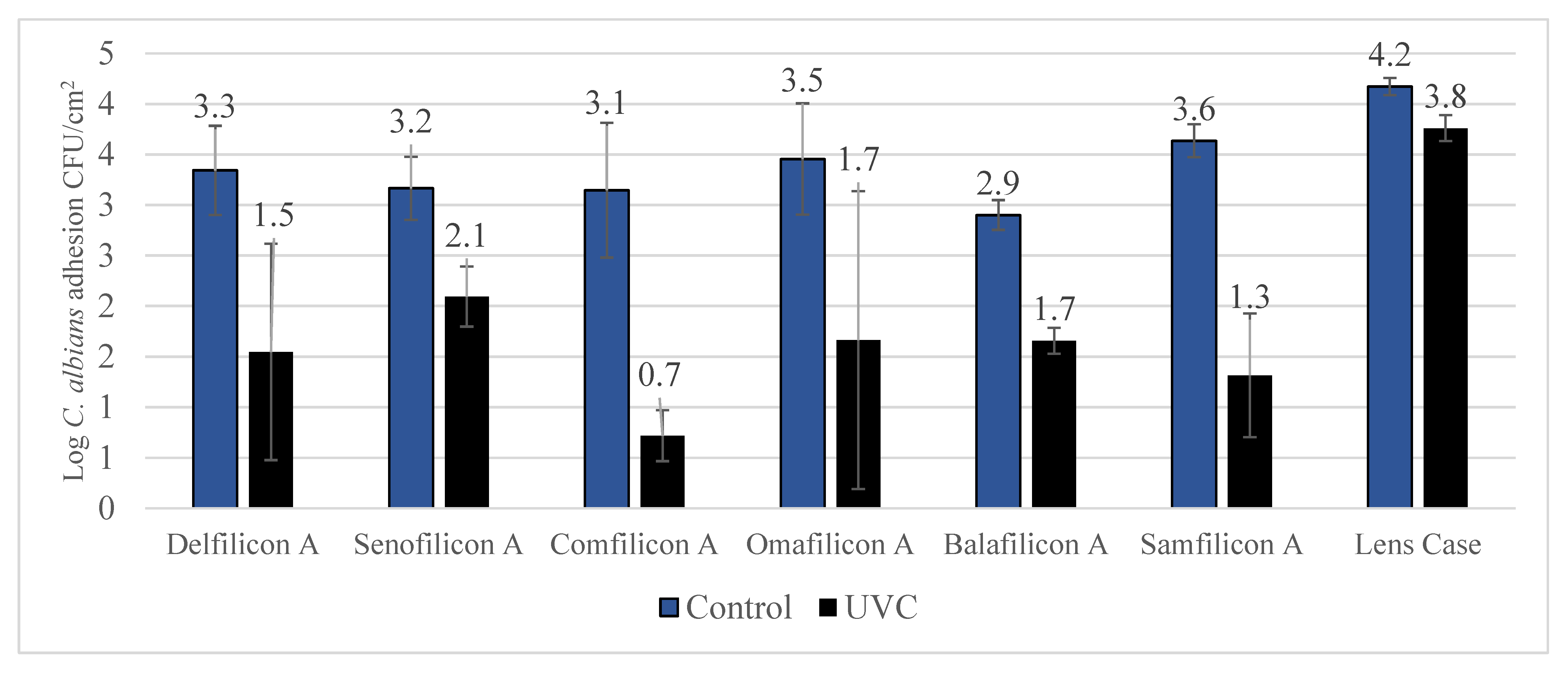
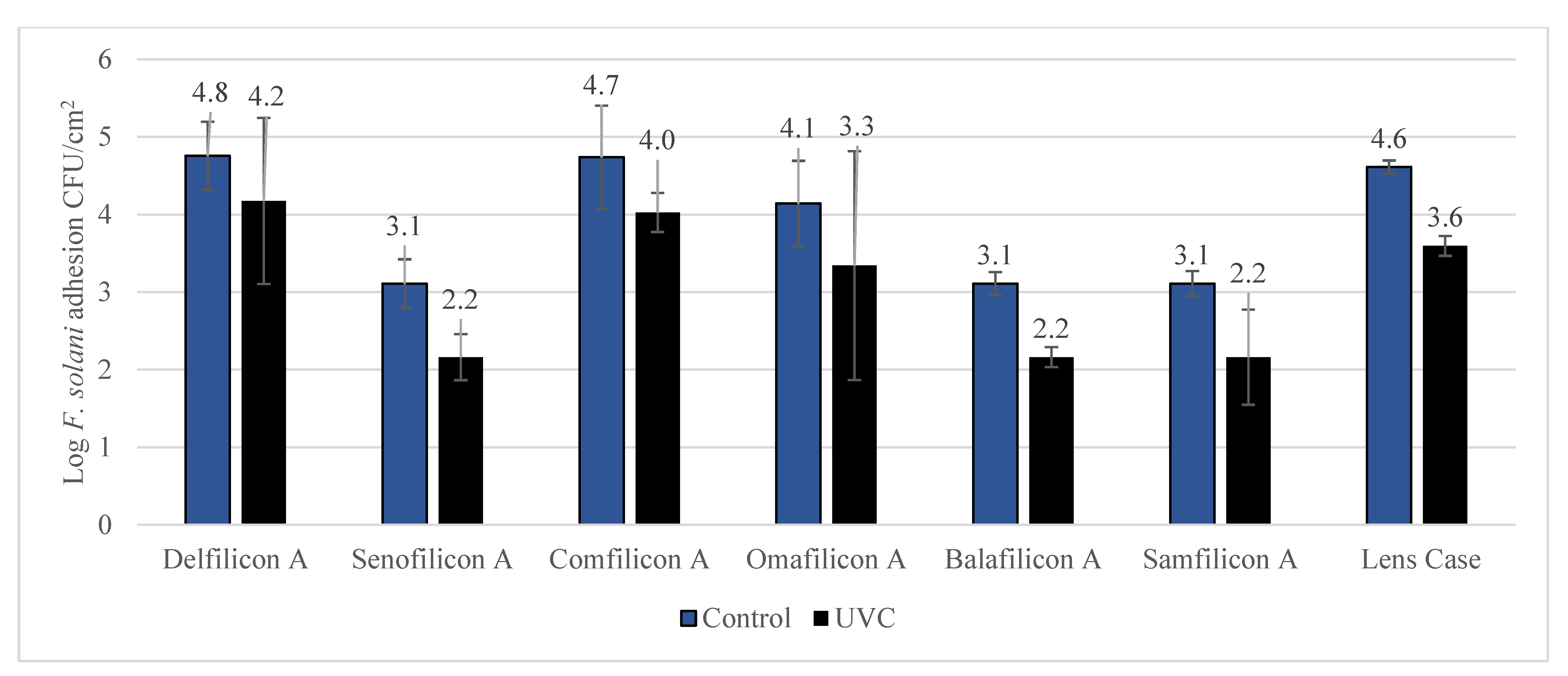
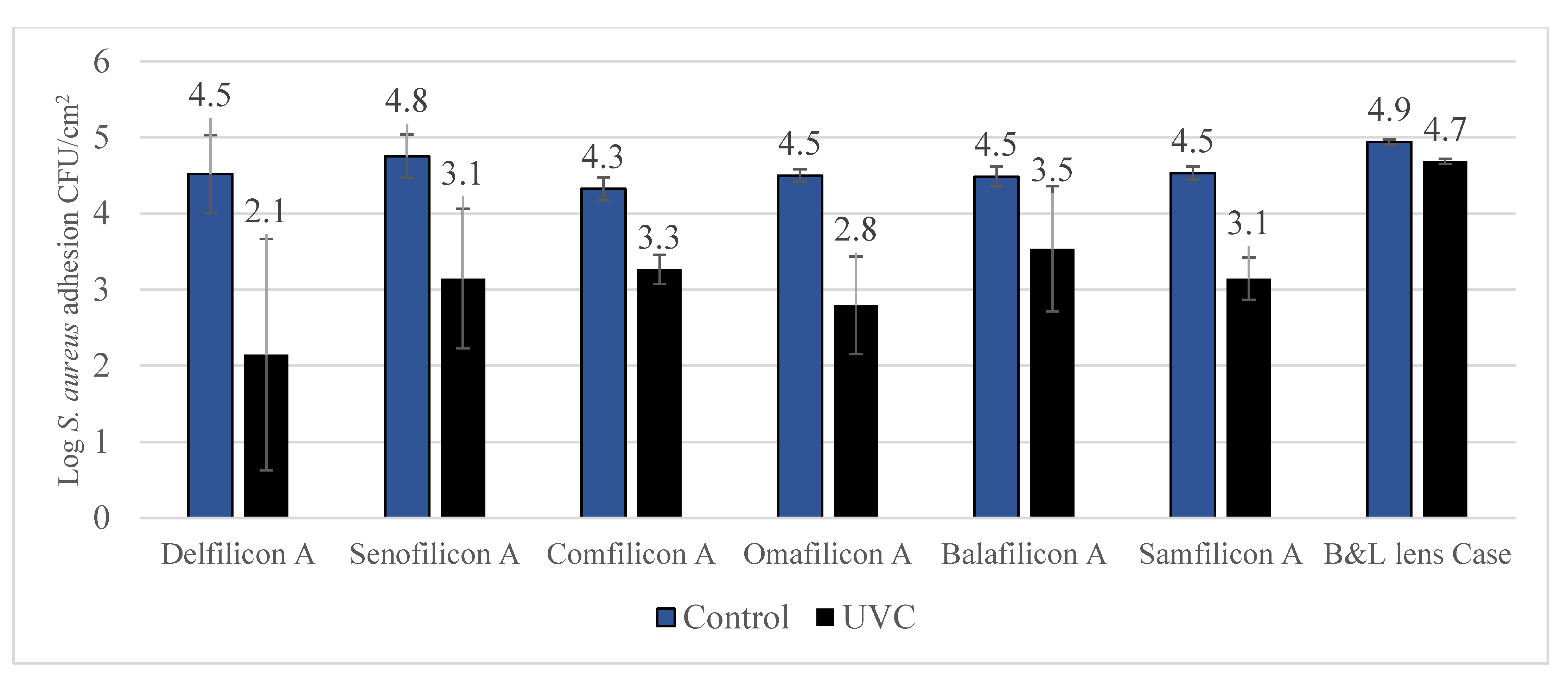
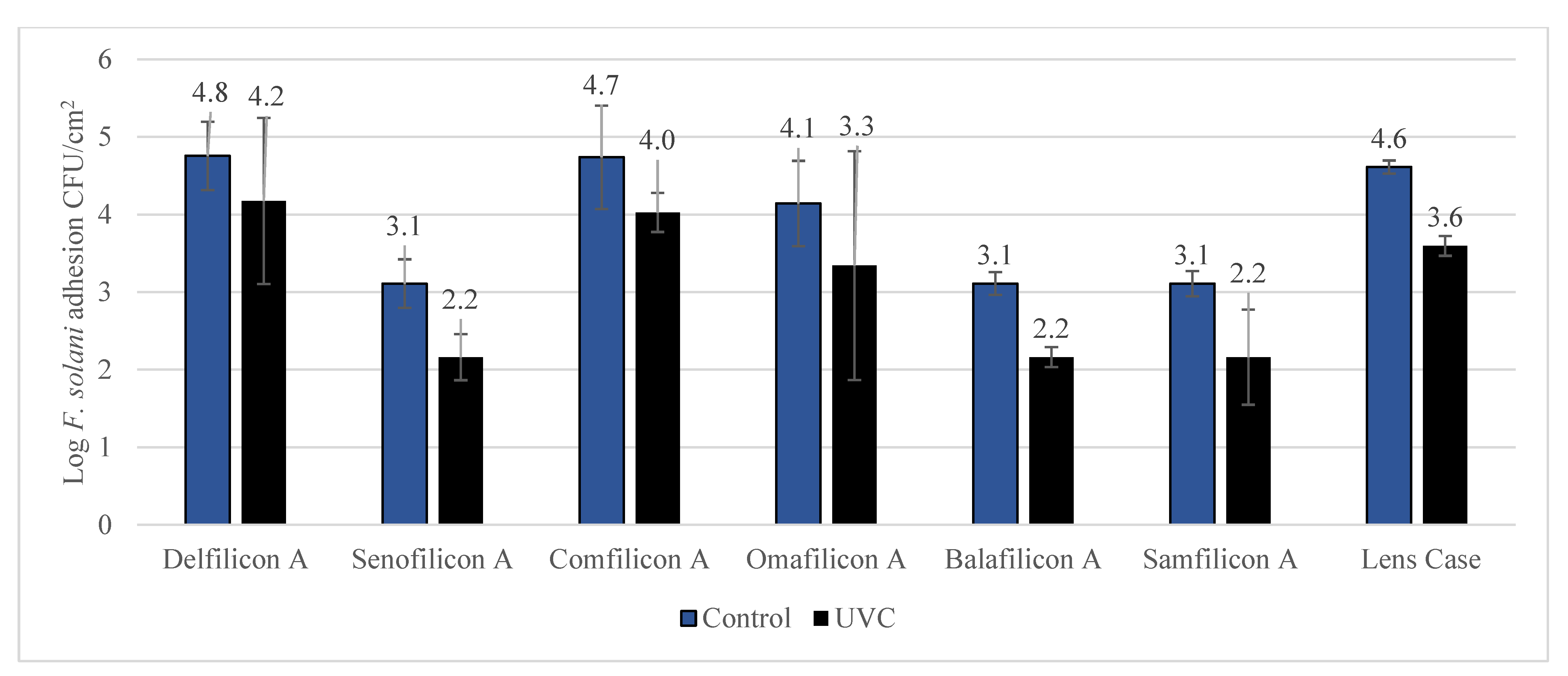
| Contact Lenses | P. aeruginosa | S. aureus | C. albicans | F. solani |
|---|---|---|---|---|
| Delefilcon A | 99.9 ± 5.2 * | 99.6 ± 10.3 * | 98.4 ± 26.7 * | 76.0 ± 5.3 * |
| Senofilcon A | 93.2 ± 4.3 * | 97.5 ± 8.9 * | 91.5 ± 13.3 * | 68.3 ± 7.3 * |
| Comfilcon A | 98.5 ± 14.3 * | 91.2 ± 5.8 * | 99.6 ± 4.2 * | 80.5 ± 13.1 * |
| Omafilcon A | 97.6 ± 15.5 * | 98.0 ± 8.5 * | 98.4 ± 17.8 * | 73.7 ± 8.6 * |
| Balafilcon A | 89.0 ± 7.8 * | 88.8 ± 13.3 * | 94.3 ± 3.4 * | 71.5 ± 10.3 |
| Samfilcon A | 98.7 ± 7.1 * | 95.9 ± 7.8 * | 99.5 ± 10.3 * | 79.9 ± 26.3 |
| Lens Case | 36.7 ± 13.3 | 44.7 ± 12.6 * | 61.2 ± 3.4 * | 90.4 ± 3.3 * |
| Proprietary Name | Total Dailes1 | Acuvue Oasys | Biofinity | Proclear | Purevision2 | Ultra |
|---|---|---|---|---|---|---|
| United States Adopted Name (USAN) | Delfilicon A | Senofilicon A | Comfilicon A | Omafilicon A | Balafilicon A | Samfilicon A |
| Lens material | Silicone hydrogel | Silicone hydrogel | Silicone hydrogel | Hydrogel | Silicone Hydrogel | Silicone Hydrogel |
| Manufacturer | Alcon | Johnson & Johnson | Cooper vision | Cooper vision | Bausch & Lomb | Bausch & Lomb |
| Water content (%) | Gradient | 38 | 48 | 62 | 36 | 46 |
| Oxygen transmissibility (DK/t) | 156 | 147 | 160 | 37 | 130 | 163 |
| Centre thickness (mm) -3.00DS | 0.09 mm | 0.07 mm | 0.08 mm | 0.09 mm | 0.07 mm | 0.07 mm |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dumpati, S.; Naroo, S.A.; Shah, S.; Dutta, D. Antimicrobial Efficacy of an Ultraviolet-C Device against Microorganisms Related to Contact Lens Adverse Events. Antibiotics 2022, 11, 699. https://doi.org/10.3390/antibiotics11050699
Dumpati S, Naroo SA, Shah S, Dutta D. Antimicrobial Efficacy of an Ultraviolet-C Device against Microorganisms Related to Contact Lens Adverse Events. Antibiotics. 2022; 11(5):699. https://doi.org/10.3390/antibiotics11050699
Chicago/Turabian StyleDumpati, Srikanth, Shehzad A. Naroo, Sunil Shah, and Debarun Dutta. 2022. "Antimicrobial Efficacy of an Ultraviolet-C Device against Microorganisms Related to Contact Lens Adverse Events" Antibiotics 11, no. 5: 699. https://doi.org/10.3390/antibiotics11050699
APA StyleDumpati, S., Naroo, S. A., Shah, S., & Dutta, D. (2022). Antimicrobial Efficacy of an Ultraviolet-C Device against Microorganisms Related to Contact Lens Adverse Events. Antibiotics, 11(5), 699. https://doi.org/10.3390/antibiotics11050699