
ICU-Associated Gram-Negative Bloodstream Infection: Risk Factors Affecting the Outcome Following the Emergence of Colistin-Resistant Isolates in a Regional Greek Hospital

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
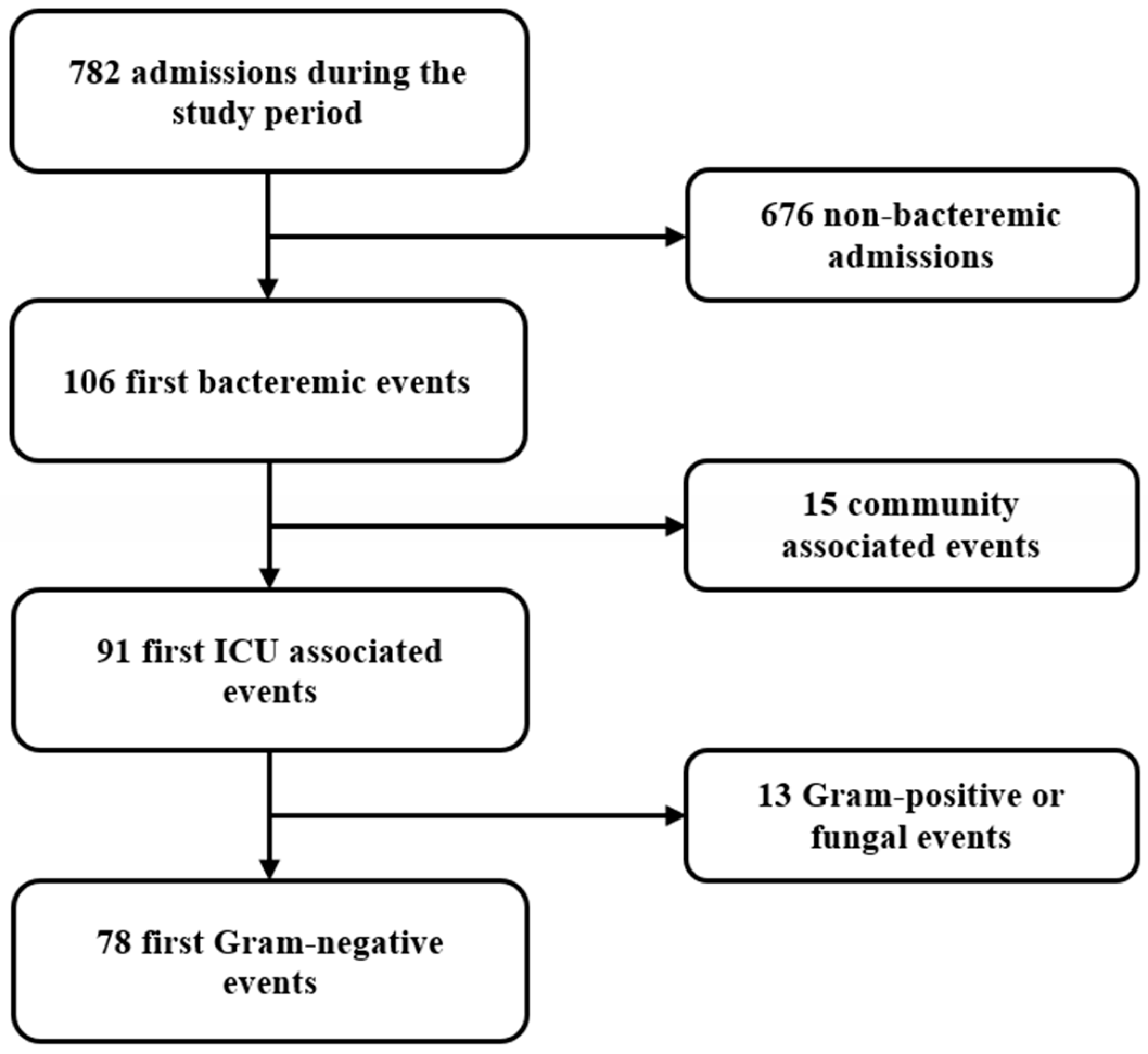
2.1. Study Design, Setting, and Selection Criteria
2.2. Variables
2.3. Definitions
2.4. Outcome
2.5. Statistical Analysis
3. Results
3.1. Population
3.2. Infection
3.3. Sensitivity Analyses for the Occurrence of the Colistin-Resistant Phenotype
3.4. Treatment
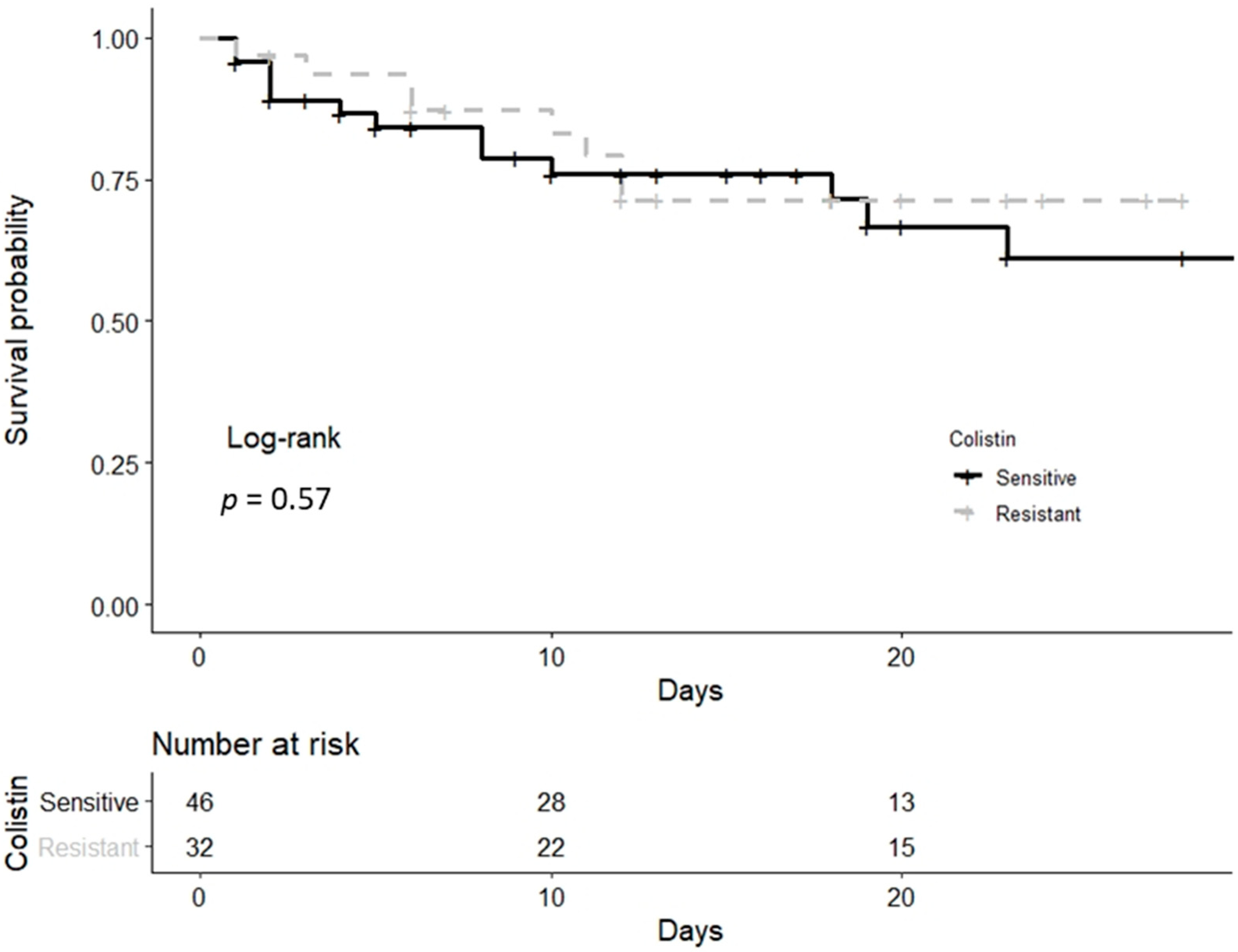
3.5. Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| APACHE II | Acute Physiology Assessment and Chronic Health Evaluation |
| AUC | area under the curve |
| BSI | bloodstream infection |
| CI | confidence interval |
| CR | colistin-resistant |
| CRG | colistin-resistant group |
| CSG | colistin-sensitive group |
| CVC | central venous catheter |
| EUCAST | European Committee On Antimicrobial Susceptibility Testing |
| GN | Gram-negative |
| ICU | intensive care unit |
| IQR | interquartile range |
| MDR | multi-drug-resistant |
| SOFA | sequential organ failure assessment |
References
- Vincent, J.L.; Rello, J.; Marshall, J.; Silva, E.; Anzueto, A.; Martin, C.D.; Moreno, R.; Lipman, J.; Gomersall, C.; Sakr, Y.; et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009, 302, 2323–2329. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; Koulenti, D.; Laupland, K.; Misset, B.; Valles, J.; Bruzzi de Carvalho, F.; Paiva, J.A.; Cakar, N.; Ma, X.; Eggimann, P.; et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: The EUROBACT International Cohort Study. Intensive Care Med. 2012, 38, 1930–1945. [Google Scholar] [CrossRef] [PubMed]
- Kadri, S.S.; Adjemian, J.; Lai, Y.L.; Spaulding, A.B.; Ricotta, E.; Prevots, D.R.; Palmore, T.N.; Rhee, C.; Klompas, M.; Dekker, J.P.; et al. Difficult-to-Treat Resistance in Gram-negative Bacteremia at 173 US Hospitals: Retrospective Cohort Analysis of Prevalence, Predictors, and Outcome of Resistance to All First-line Agents. Clin. Infect. Dis. 2018, 67, 1803–1814. [Google Scholar] [CrossRef] [PubMed]
- Sherry, N.; Howden, B. Emerging Gram-negative resistance to last-line antimicrobial agents fosfomycin, colistin and ceftazidime-avibactam-epidemiology, laboratory detection and treatment implications. Expert Rev. Anti-Infect. Ther. 2018, 16, 289–306. [Google Scholar] [CrossRef] [PubMed]
- Olaitan, A.O.; Morand, S.; Rolain, J.-M. Mechanisms of polymyxin resistance: Acquired and intrinsic resistance in bacteria. Front. Microbiol. 2014, 5, 643. [Google Scholar] [CrossRef]
- Zak-Doron, Y.; Dishon Benattar, Y.; Pfeffer, I.; Daikos, G.L.; Skiada, A.; Antoniadou, A.; Durante-Mangoni, E.; Andini, R.; Cavezza, G.; Leibovici, L.; et al. The Association between Empirical Antibiotic Treatment and Mortality in Severe Infections Caused by Carbapenem-resistant Gram-negative Bacteria: A Prospective Study. Clin. Infect. Dis. 2018, 67, 1815–1823. [Google Scholar] [CrossRef]
- Dickstein, Y.; Lellouche, J.; Ben Dalak Amar, M.; Schwartz, D.; Nutman, A.; Daitch, V.; Yahav, D.; Leibovici, L.; Skiada, A.; Antoniadou, A.; et al. Treatment Outcomes of Colistin- and Carbapenem-resistant Acinetobacter baumannii Infections: An Exploratory Subgroup Analysis of a Randomized Clinical Trial. Clin. Infect. Dis. 2019, 69, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Xavier, B.B.; Lammens, C.; Ruhak, R.; Kumar-Singh, S.; Butaye, P.; Goossens, H.; Malhotra-Kumar, S. Identification of a novel plasmid-mediated colistin-resistance gene, mcr-2, in Escherichia coli, Belgium, June 2016. Eurosurveillance 2016, 21, 30280. [Google Scholar] [CrossRef]
- Ni, W.; Li, Y.; Guan, J.; Zhao, J.; Cui, J.; Wang, R.; Liu, Y. Effects of Efflux Pump Inhibitors on Colistin Resistance in Multidrug-Resistant Gram-Negative Bacteria. Antimicrob. Agents Chemother. 2016, 60, 3215–3218. [Google Scholar] [CrossRef]
- Miyakis, S.; Pefanis, A.; Tsakris, A. The challenges of antimicrobial drug resistance in Greece. Clin. Infect. Dis. 2011, 53, 177–184. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Antimicrobial Susceptibility Testing of Colistin-Problems Detected with Several Commercially Available Products. 2016. Available online: http://www.eucast.org (accessed on 15 December 2017).
- Kalil, A.; Meterski, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. 2016, 63, e61–e111. [Google Scholar] [CrossRef]
- Pronovost, P.; Needham, D.; Berenholtz, S.; Sinopoli, D.; Chu, H.; Cosgrove, S.; Sexton, B.; Hyzy, R.; Welsh, R.; Roth, G.; et al. An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU. N. Engl. J. Med. 2006, 355, 2725–2732. [Google Scholar] [CrossRef] [PubMed]
- Institute for Healthcare Improvement. How-to Guide: Prevent Ventilator-Associated Pneumonia. Available online: http://www.ihi.org (accessed on 10 May 2018).
- Nation, R.L.; Garonzik, S.M.; Thamlikitkul, V.; Giamarellos-Bourboulis, E.J.; Forrest, A.; Paterson, D.L.; Li, J.; Silveira, F.P. Dosing Guidance for Intravenous Colistin in Critically Ill Patients. Clin. Infect. Dis. 2017, 64, 565–571. [Google Scholar] [CrossRef]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters Version 7.0. Available online: http://www.eucast.org (accessed on 10 December 2017).
- World Medical Association Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: http://www.wma.net (accessed on 15 December 2018).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. For the STROBE Initiative Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, e296. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef]
- Korvick, J.A.; Bryan, C.S.; Farber, B.; Beam, T.R., Jr.; Schenfeld, L.; Muder, R.R.; Weinbaum, D.; Lumish, R.; Gerding, D.N.; Wagener, M.M. Prospective observational study of Klebsiella bacteremia in 230 patients: Outcome for antibiotic combinations versus monotherapy. Antimicrob. Agents Chemother. 1992, 36, 2639–2644. [Google Scholar] [CrossRef]
- Lambert, M.-L.; Suetens, C.; Savey, A.; Palomar, M.; Hiesmayr, M.; Morales, I.; Agodi, A.; Frank, U.; Mertens, K.; Schumacher, M.; et al. Clinical outcomes of health-care-associated infections and antimicrobial resistance in patients admitted to European intensive-care units: A cohort study. Lancet Infect. Dis. 2011, 11, 30–38. [Google Scholar] [CrossRef]
- Haverkate, M.R.; Derde, L.P.G.; Brun-Buisson, C.; Bonten, M.J.M.; Bootsma, M.C.J. Duration of colonization with antimicrobial-resistant bacteria after ICU discharge. Intensive Care Med. 2014, 40, 564–571. [Google Scholar] [CrossRef][Green Version]
- Woudt, S.H.S.; de Greeff, S.C.; Schoffelen, A.F.; Vlek, A.L.M.; Bonten, M.J.M. Antibiotic Resistance and the Risk of Recurrent Bacteremia. Clin. Infect. Dis. 2018, 66, 1651–1657. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef] [PubMed]
- Falcone, M.; Russo, A.; Iacovelli, A.; Restuccia, G.; Ceccarelli, G.; Giordano, A.; Farcomeni, A.; Morelli, A.; Venditti, M. Predictors of outcome in ICU patients with septic shock caused by Klebsiella pneumoniae carbapenemase–producing K. pneumoniae. Clin. Microbiol. Infect. 2016, 22, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Mermel, L.A.; Allon, M.; Bouza, E.; Craven, D.E.; Flynn, P.; O’Grady, N.P.; Raad, I.I.; Rijnders, B.J.A.; Sherertz, R.J.; Warren, D.K. Clinical Practice Guidelines for the Diagnosis and Management of Intravascular Catheter-Related Infection: 2009 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2009, 49, 1–45. [Google Scholar] [CrossRef]
- Girometti, N.; Lewis, R.E.; Giannella, M.; Ambretti, S.; Bartoletti, M.; Tedeschi, S.; Tumietto, F.; Cristini, F.; Trapani, F.; Gaibani, P.; et al. Klebsiella pneumoniae Bloodstream Infection Epidemiology and Impact of Inappropriate Empirical Therapy. Medicine 2014, 93, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Ong, D.S.Y.; Frencken, J.F.; Klein Klouwenberg, P.M.C.; Juffermans, N.; van der Poll, T.; Bonten, M.J.M.; Cremer, O.L.; MARS Consortium. Short-Course Adjunctive Gentamicin as Empirical Therapy in Patients with Severe Sepsis and Septic Shock: A Prospective Observational Cohort Study. Clin. Infect. Dis. 2017, 64, 1731–1736. [Google Scholar] [CrossRef]
- Vesin, A.; Azoulay, E.; Ruckly, S.; Vignoud, L.; Rusinovà, K.; Benoit, D.; Soares, M.; Azeivedo-Maia, P.; Abroug, F.; Benbenishty, J.; et al. Reporting and handling missing values in clinical studies in intensive care units. Intensive Care Med. 2013, 39, 1396–1404. [Google Scholar] [CrossRef]
- Nunez, E.; Steyerberg, E.W.; Nunez, J. Regression Modeling Strategies. Rev. Esp. Cardiol. 2011, 64, 501–507. [Google Scholar]
- The R Project for Statistical Computing. Available online: http://www.r-project.org (accessed on 15 April 2021).
- Rohas, L.J.; Salim, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Marshall, S.; Rudin, S.D.; et al. Colistin Resistance in Carbapenem-Resistant Klebsiella pneumoniae: Laboratory Detection and Impact on Mortality. Clin. Infect. Dis. 2017, 64, 711–718. [Google Scholar]
- Baggs, J.; Jernigan, J.A.; Laufer Halpin, A.; Epstein, L.; Hatfield, K.M.; McDonald, L.C. Risk of Subsequent Sepsis within 90 Days after a Hospital Stay by Type of Antibiotic Exposure. Clin. Infect. Dis. 2018, 66, 1004–1012. [Google Scholar] [CrossRef]
- Papathanakos, G.; Andrianopoulos, I.; Papathanasiou, A.; Priavali, E.; Koulenti, D.; Koulouras, V. Colistin-Resistant Acinetobacter Baumannii Bacteremia: A Serious Threat for Critically Ill Patients. Microorganisms 2020, 8, 287. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Del Bono, V.; Trecarichi, E.M.; De Rosa, F.G.; Giannella, M.; Bassetti, M.; Bartoloni, A.; Losito, A.R.; Corcione, C.; Bartoletti, M.; et al. Risk factors for bloodstream infections due to colistin-resistant KPC-producing Klebsiella pneumoniae: Results from a multicenter case–control–control study. Clin. Microbiol. Infect. 2015, 21, 1106.e1–1106.e8. [Google Scholar] [CrossRef]
- van Duin, D.; Lok, J.J.; Earley, M.; Cober, E.; Richter, S.S.; Perez, F.; Salata, R.A.; Kalayjian, R.C.; Watkins, R.R.; Doi, Y.; et al. Colistin versus Ceftazidime-Avibactam in the Treatment of Infections Due to Carbapenem-Resistant Enterobacteriaceae. Clin. Infect. Dis. 2018, 66, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Karaiskos, I.; Lagou, S.; Pontikis, K.; Rapti, V.; Poulakou, G. The “Old” and the “New” Antibiotics for MDR Gram-Negative Pathogens: For Whom, When, and How. Front. Public Health 2019, 7, 151. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Poulakou, G.; Ruppe, E.; Bouza, E.; Van Hal, S.J.; Brink, A. Antimicrobial resistance in the next 30 years, humankind, bugs and drugs: A visionary approach. Intensive Care Med. 2017, 43, 1464–1475. [Google Scholar] [CrossRef] [PubMed]
- Beseiro, A.; Moreno, A.; Fernandez, N.; Vallejo, J.A.; Aranda, J.; Adler, B.; Harper, M.; Boyce, J.D.; Bou, G. Biological Cost of Different Mechanisms of Colistin Resistance and Their Impact on Virulence in Acinetobacter baumannii. Antimicrob. Agents Chemother. 2014, 58, 518–526. [Google Scholar] [CrossRef]
- Liu, E.; Jia, P.; Li, X.; Zhou, M.; Kudinha, T.; Wu, C.; Xu, Y.; Yang, Q. In vitro and in vivo Effect of Antimicrobial Agent Combinations against Carbapenem-Resistant Klebsiella pneumoniae with Different Resistance Mechanisms in China. Infect. Drug Resist. 2021, 14, 917–928. [Google Scholar] [CrossRef]
- Fyfe, C.; LeBlanc, G.; Close, B.; Nordmann, P.; Dumas, J.; Grossman, T.H. Eravacycline Is Active against Bacterial Isolates Expressing the Polymyxin Resistance Gene mcr-1. Antimicrob. Agents Chemother. 2016, 60, 6989–6990. [Google Scholar] [CrossRef] [PubMed]
- Jana, B.; Cain, A.K.; Doerrler, W.T.; Boinett, C.J.; Fookes, M.C.; Parkhill, J.; Guardabassi, L. The secondary resistome of multidrug-resistant Klebsiella pneumoniae. Sci. Rep. 2017, 7, 42483. [Google Scholar] [CrossRef]
- Panta, P.R.; Kumar, S.; Stafford, S.F.; Billiot, C.E.; Douglass, M.V.; Herrera, C.M.; Trent, M.S.; Doerrler, W.T. A DedA Family Membrane Protein Is Required for Burkholderia thailandensis Colistin Resistance. Front. Microbiol. 2019, 10, 2532. [Google Scholar] [CrossRef]
- Jousset, A.B.; Bonnin, R.A.; Rosinski-Chupin, I.; Girlich, D.; Cuzon, G.; Cabanel, N.; Frech, H.; Farfour, E.; Dortet, L.; Glaser, P.; et al. A 4.5-Year Within-Patient Evolution of a Colistin-Resistant Klebsiella pneumoniae Carbapenemase–Producing, K. pneumoniae Sequence Type 258. Clin. Infect. Dis. 2018, 67, 1388–1394. [Google Scholar] [CrossRef]
- Mattia Palmieri, M.; D’Andrea, M.M.; Pelegrin, A.C.; Perrot, N.; Mirande, C.; Blanc, B.; Legakis, N.; Goossens, H.; Rossolini, G.M.; van Belkum, A. Abundance of Colistin-Resistant, OXA-23- and ArmA-Producing Acinetobacter baumannii Belonging to International Clone 2 in Greece. Front. Microbiol. 2020, 11, 294. [Google Scholar]
- Mavroidi, A.; Katsiari, M.; Likousi, S.; Palla, E.; Roussou, Z.; Nikolaou, C.; Maguina, A.; Platsouka, E.D. Characterization of ST258 Colistin-Resistant, blaKPC-Producing Klebsiella pneumoniae in a Greek Hospital. Microb. Drug Resist. 2016, 22, 392–398. [Google Scholar] [CrossRef]
- Brennan-Krohn, T.; Kirby, J.E. When One Drug Is Not Enough: Context, Methodology, and Future Prospects in Antibacterial Synergy Testing. Clin. Lab. Med. 2019, 39, 345–358. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 78) | Colistin-Resistant (n = 32) | Colistin-Sensitive (n = 46) | p-Value ** | Odds Ratio (95% CI) ## | |
|---|---|---|---|---|---|
| On admission | |||||
| Age, years | 66 (50.2–76) | 72 (59–78) | 62.5 (47.7–74.5) | 0.07 | |
| Male | 51 (65.4) | 22 (68.7) | 29 (63) | 0.64 | |
| Charlson Comorbidity Index | 3 (1–5) | 4 (2–5) | 2.5 (1–5) | 0.25 | |
| APACHE II | 19 (13–24) | 21.5 (15.2–25) | 17.5 (10.7–21) | 0.01 | 1.11 (1.03–1.21) |
| SOFA score | 8 (5–10) | 9 (6.2–10) | 7 (3.5–10.5) | 0.15 | |
| Prior ICU stay, previous year | 27 (34.6) | 12 (37.5) | 15 (32.6) | 0.80 | |
| Medical patients | 48 (61.5) | 23 (71.9) | 25 (54.3) | 0.16 | |
| Immunosuppression | 9 (11.5) | 6 (18.7) | 3 (6.5) | 0.14 | |
| Admission due to infection | 21 (26.9) | 6 (18.7) | 15 (32.6) | 0.20 | 0.35 (0.1–1.07) |
| Antibiotics in the previous 3 months | 48 (61.5) | 19 (59.4) | 29 (63) | 0.64 | |
| Before the event | |||||
| CVC for at least 48 h | 61 (78.2) | 25 (78.1) | 36 (78.3) | >0.99 | |
| Antibiotics in the ICU | 61 (78.2) | 24 (75) | 37 (80.4) | 0.59 | |
| Maximum number of drugs with AGNA at any time | 0.29 | ||||
| None given | 17 (21.8) | 8 (25) | 9 (19.6) | ||
| Single | 31 (39.7) | 9 (28.1) | 22 (47.8) | ||
| Two | 9 (11.6) | 3 (9.4) | 6 (13) | ||
| Three | 10 (12.8) | 5 (15.6) | 5 (10.9) | ||
| Four | 11 (14.1) | 7 (21.9) | 4 (8.7) | ||
| Antibiotic classes/class members * | |||||
| Third & fourth generation cephalosporins | 26 (33.3) | 11 (34.4) | 15 (32.6) | ||
| Colistin | 28 (35.9) | 14 (43.8) | 14 (30.4) | ||
| Tigecycline | 24 (30.8) | 13 (40.7) | 11 (23.9) | ||
| Carbapenems | 33 (42.3) | 14 (43.8) | 19 (41.3) | ||
| Aminoglycosides | 10 (12.8) | 5 (15.6) | 5 (10.9) | ||
| Quinolones | 13 (16.7) | 10 (31.2) | 3 (6.5) | ||
| Ampicillin/sulbactam | 15 (19.2) | 8 (25) | 7 (15.2) | ||
| Piperacillin/tazobactam | 9 (11.5) | 4 (12.5) | 5 (10.9) | ||
| Ceftazidime/avibactam | 7 (9) | 4 (12.5) | 3 (6.5) | ||
| Index day | NA | ||||
| Event, days | 10 (6–18) | 12 (5.2–21.5) | 9.5 (6–17.2) | 0.66 | |
| Timing of the event | 0.34 | ||||
| >48 h stay | 67 (85.9) | 26 (81.3) | 41 (89.1) | ||
| <48 h stay | 11 (14.1) | 6 (18.7) | 5 (10.9) | ||
| Source | 0.73 | ||||
| Primary | 32 (41) | 13 (40.6) | 19 (41.3) | ||
| Catheter-related # | 25 (32.1) | 12 (37.5) | 13 (28.3) | ||
| Urinary | 5 (6.4) | 3 (9.4) | 2 (4.3) | ||
| Intraabdominal | 5 (6.4) | 1 (3.1) | 4 (8.7) | ||
| Surgical site infection | 5 (6.4) | 1 (3.1) | 4 (8.7) | ||
| Lung/pleural empyema | 4 (5.1) | 1 (3.1) | 3 (6.5) | ||
| Bone/joint | 2 (2.6) | 1 (3.1) | 1 (2.2) | ||
| Source control performed | 30 (38.5) | 15 (46.9) | 15 (32.6) | 0.24 | |
| Pitt bacteremia score | 3 (1–4) | 4 (2–4.7) | 3 (1–4.2) | 0.25 | |
| Septic shock | 43 (55.1) | 18 (56.2) | 25 (54.3) | >0.99 | |
| Temperature max, °C | 38.5 (37.9–39) | 38.5 (37.9–39) | 38.5 (37.7–39) | 0.97 | |
| Fever | 49 (62.8) | 22 (68.7) | 32 (69.6) | >0.99 | |
| Hypothermia | 4 (5.1) | 0 (0) | 4 (8.7) | 0.14 | |
| SOFA score | 6.5 (3.8–11) | 8 (5–12.7) | 5 (3–11) | 0.07 | - |
| White Blood Cells /mm3, ×1000 | 13.4 (9.5–18.1) | 13.94 (11.47–19.63) | 12.97 (9.25–16.83) | 0.69 | |
| Leucopenia | 2 (2.6) | 1 (3.1) | 1 (2.2) | >0.99 | |
| CRP, mg/L | 121 (62.7–155) | 125 (58–204) | 119 (63.2–141) | 0.34 | |
| Procalcitonin, μg/L | 1.23 (0.34–2.08) | 1.51 (0.51–2.94) | 1.01 (0.22–2.16) | 0.19 | |
| Final model’s accuracy, AUC (95% CI) | 0.71 (0.59–0.83) | ||||
| Overall | Colistin-Resistant Group | Colistin-Sensitive Group | ||
|---|---|---|---|---|
| Pathogen * | ||||
| Acinetobacter baumannii | 29 | 12 | 17 | |
| Klebsiella pneumoniae | 24 | 8 | 16 | |
| Pseudomonas aeruginosa | 10 | 0 | 10 | |
| Proteus mirabilis | 6 | 6 | 0 | |
| Enterobacter cloace | 4 | 0 | 4 | |
| Providencia stuartii | 4 | 4 | 0 | |
| Serratia marcescens | 2 | 2 | 0 | |
| Carbapenem-resistant | 57 | 24 | 33 | |
| Event > 48 h | 47 | 19 | 28 | |
| Event < 48 h | 10 | 5 | 5 | |
| Colistin MIC (ng/mL) # | ||||
| =2 | - | - | 8 | |
| =1 | - | - | 4 | |
| ≤0.5 | - | - | 34 | |
| Dead (n = 21) | Alive (n = 57) | p-Value # | Hazard Ratio (95% CI) ## | |
|---|---|---|---|---|
| Age | 75 (67–79) | 62 (47–73) | <0.01 | |
| Male | 12 (57.1) | 39 (68.4) | 0.42 | |
| APACHE II | 20 (19–25) | 17 (12–22) | 0.04 | |
| CCI | 4 (4–5) | 2 (1–4) | 0.01 | |
| SOFA Admission | 10 (8–12.2) | 7 (4–10) | 0.01 ** | |
| Prior ICU admission * | 8 (38.1) | 19 (33.3) | 0.79 | |
| Infectious admission | 7 (33.3) | 14 (24.6) | 0.57 | |
| Medical admission | 10 (47.6) | 38 (66.7) | 0.19 | |
| Immunosuppression | 2 (9.5) | 7 (14) | >0.99 | |
| Source control | 10 (47.6) | 20 (35.1) | 0.43 | |
| Pitt bacteremia score | 4 (4–6) | 3 (1–4) | <0.01 | |
| Septic shock | 20 (95.2) | 23 (40.4) | <0.01 | |
| Colistin-resistance status | 0.80 | |||
| -Colistin-resistant | 8 (38.1) | 24 (42.1) | ||
| -Colistin-sensitive | 13 (61.9) | 33 (57.9) | ||
| Colistin MIC ≤ 0.5 | 12 (57.1) | 32 (56.1) | >0.99 | |
| Empirical colistin for at least 3 days | 8 (38.1) | 25 (43.9) | 0.80 | |
| SOFA index day | 13 (11–16) | 5 (3–9) | <0.01 ** | 1.23 (1.03–1.48) |
| Temperature index day, °C | 38 (36.8–38.5) | 38.7 (38.1–39.2) | 0.01 | |
| WBC index day, 103/mm3, ×1000 | 13.63 (10.44–17.88) | 13.43 (9.31–18.14) | 0.99 | |
| CRP index day, mg/L | 109.4 (71.83–136.25) | 126 (61.08–154.5) | 0.53 | |
| Procalcitonin index day, ng/mL | 1.33 (1.13–5.63) | 0.84 (0.32–1.94) | 0.20 | |
| Five-day empirical treatment with colistin | 6 (28.6) | 20 (35.1) | 0.79 | |
| Ten-day colistin treatment, post-event | 5 (23.8) | 16 (28.1) | 0.58 | |
| One appropriate drug within 24 h post-event | 7 (33.3) | 21 (36.8) | >0.99 | |
| One appropriate drug within 48 h post-event | 8 (38.1) | 25 (43.9) | 0.80 | |
| Two appropriate drugs within 24 h post-event | 3 (14.3) | 7 (12.3) | >0.99 | |
| Two appropriate drugs within 48 h post-event | 3 (14.3) | 11 (19.3) | 0.75 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karvouniaris, M.; Poulakou, G.; Tsiakos, K.; Chatzimichail, M.; Papamichalis, P.; Katsiaflaka, A.; Oikonomou, K.; Katsioulis, A.; Palli, E.; Komnos, A. ICU-Associated Gram-Negative Bloodstream Infection: Risk Factors Affecting the Outcome Following the Emergence of Colistin-Resistant Isolates in a Regional Greek Hospital. Antibiotics 2022, 11, 405. https://doi.org/10.3390/antibiotics11030405
Karvouniaris M, Poulakou G, Tsiakos K, Chatzimichail M, Papamichalis P, Katsiaflaka A, Oikonomou K, Katsioulis A, Palli E, Komnos A. ICU-Associated Gram-Negative Bloodstream Infection: Risk Factors Affecting the Outcome Following the Emergence of Colistin-Resistant Isolates in a Regional Greek Hospital. Antibiotics. 2022; 11(3):405. https://doi.org/10.3390/antibiotics11030405
Chicago/Turabian StyleKarvouniaris, Marios, Garyphallia Poulakou, Konstantinos Tsiakos, Maria Chatzimichail, Panagiotis Papamichalis, Anna Katsiaflaka, Katerina Oikonomou, Antonios Katsioulis, Eleni Palli, and Apostolos Komnos. 2022. "ICU-Associated Gram-Negative Bloodstream Infection: Risk Factors Affecting the Outcome Following the Emergence of Colistin-Resistant Isolates in a Regional Greek Hospital" Antibiotics 11, no. 3: 405. https://doi.org/10.3390/antibiotics11030405
APA StyleKarvouniaris, M., Poulakou, G., Tsiakos, K., Chatzimichail, M., Papamichalis, P., Katsiaflaka, A., Oikonomou, K., Katsioulis, A., Palli, E., & Komnos, A. (2022). ICU-Associated Gram-Negative Bloodstream Infection: Risk Factors Affecting the Outcome Following the Emergence of Colistin-Resistant Isolates in a Regional Greek Hospital. Antibiotics, 11(3), 405. https://doi.org/10.3390/antibiotics11030405