
Antimicrobial Stewardship Using Biomarkers: Accumulating Evidence for the Critically Ill


Abstract
1. Introduction
2. Results and Discussion
2.1. Antimicrobial Stewardship through PCT-Guidance for Lower Respiratory Tract Infections
2.2. Antimicrobial Stewardship through PCT-Guidance in Sepsis
2.3. Real-World Data
2.4. Antimicrobial Stewardship through Other Biomarkers
2.5. Antimicrobial Stewardship Using Biomarkers in the COVID-19 Era
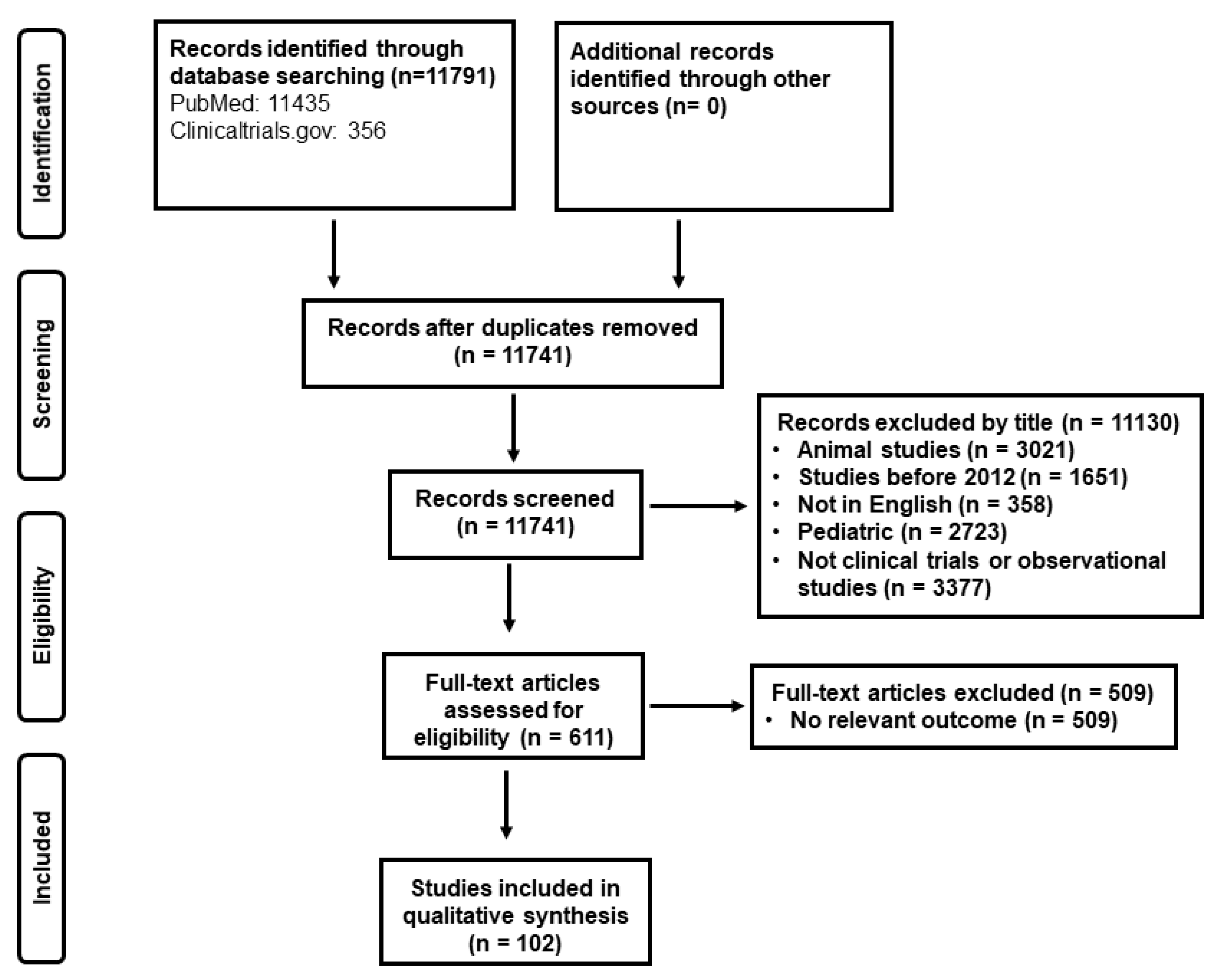
3. Materials and Methods
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- The Biomarker Definitions Working Group. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Sankar, V.; Webster, N.R. Clinical application of sepsis biomarkers. J. Anesth. 2013, 27, 269–283. [Google Scholar] [CrossRef]
- Pierrakos, C.; Vincent, J.L. Sepsis biomarkers: A review. Crit. Care 2010, 14, R15. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Jaccard-Stolz, D.; Bingisser, R.; Gencay, M.M.; Huber, P.R.; Tamm, M.; Müller, B. Effect of procalcitonin-guided treatment on antibiotic use and outcome in lower respiratory tract infections: Cluster-randomised, single-blinded intervention trial. Lancet 2004, 363, 600–607. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Stolz, D.; Bingisser, R.; Muller, C.; Miedinger, D.; Huber, P.R.; Zimmerli, W.; Harbarth, S.; Tamm, M.; Muller, B. Procalcitonin guidance of antibiotic therapy in community-acquired pneumonia: A randomized trial. Am. J. Respir. Crit. Care Med. 2006, 174, 84–93. [Google Scholar] [CrossRef]
- Stolz, D.; Christ-Crain, M.; Bingisser, R.; Leuppi, J.; Miedinger, D.; Müller, C.; Huber, P.; Müller, B.; Tamm, M. Antibiotic treatment of exacerbations of COPD: A randomized, controlled trial comparing procalcitonin-guidance with standard therapy. Chest 2007, 131, 9–19. [Google Scholar] [CrossRef]
- Briel, M.; Schuetz, P.; Mueller, B.; Young, J.; Schild, U.; Nusbaumer, C.; Périat, P.; Bucher, H.C.; Christ-Crain, M. Procalcitonin-guided antibiotic use vs a standard approach for acute respiratory tract infections in primary care. Arch. Intern. Med. 2008, 168, 2000–2008. [Google Scholar] [CrossRef]
- Kristoffersen, K.; Søgaard, O.; Wejse, C.; Black, F.; Greve, T.; Tarp, B.; Storgaard, M.; Sodemann, M. Antibiotic treatment interruption of suspected lower respiratory tract infections based on a single procalcitonin measurement at hospital admission—A randomized trial. Clin. Microbiol. Infect. 2009, 15, 481–487. [Google Scholar] [CrossRef]
- Schuetz, P.; Christ-Crain, M.; Thomann, R.; Falconnier, C.; Wolbers, M.; Widmer, I.; Neidert, S.; Fricker, T.; Blum, C.; Schild, U.; et al. Effect of procalcitonin-based guidelines vs standard guidelines on antibiotic use in lower respiratory tract infections: The ProHOSP randomized controlled trial. JAMA 2009, 302, 1059–1066. [Google Scholar] [CrossRef]
- Burkhardt, O.; Ewig, S.; Haagen, U.; Giersdorf, S.; Hartmann, O.; Wegscheider, K.; Hummers-Pradier, E.; Welte, T. Procalcitonin guidance and reduction of antibiotic use in acute respiratory tract infection. Eur. Respir. J. 2010, 36, 601–607. [Google Scholar] [CrossRef]
- Long, W.; Deng, X.; Zhang, Y.; Lu, G.; Xie, J.; Tang, J. Procalcitonin guidance for reduction of antibiotic use in low-risk outpatients with community-acquired pneumonia. Respirology 2011, 16, 819–824. [Google Scholar] [CrossRef]
- Tang, J.; Long, W.; Yan, L.; Zhang, Y.; Xie, J.; Lu, G.; Yang, C. Procalcitonin guided antibiotic therapy of acute exacerbations of asthma: A randomized controlled trial. BMC Infect. Dis. 2013, 13, 596. [Google Scholar] [CrossRef]
- Ogasawara, T.; Umezawa, H.; Naito, Y.; Takeuchi, T.; Kato, S.; Yano, T.; Kasamatsu, N.; Hashizume, I. Procalcitonin-guided antibiotic therapy in aspiration pneumonia and an assessment of the continuation of oral intake. Respir. Investig. 2014, 52, 107–113. [Google Scholar] [CrossRef]
- Long, W.; Li, L.-J.; Huang, G.-Z.; Zhang, X.-M.; Zhang, Y.-C.; Tang, J.-G.; Zhang, Y.; Lu, G. Procalcitonin guidance for reduction of antibiotic use in patients hospitalized with severe acute exacerbations of asthma: A randomized controlled study with 12-month follow-up. Crit. Care 2014, 18, 471. [Google Scholar] [CrossRef]
- Verduri, A.; Luppi, F.; D’amico, R.; Balduzzi, S.; Vicini, R.; Liverani, A.; Ruggieri, V.; Plebani, M.; Barbaro, M.P.F.; Spanevello, A.; et al. Antibiotic treatment of severe exacerbations of chronic obstructive pulmonary disease with procalcitonin: A randomized noninferiority trial. PLoS ONE 2015, 10, e0118241. [Google Scholar] [CrossRef]
- Branche, A.R.; Walsh, E.E.; Vargas, R.; Hulbert, B.; Formica, M.A.; Baran, A.; Peterson, D.R.; Falsey, A.R. Serum procalcitonin measurement and viral testing to guide antibiotic use for respiratory infections in hospitalized adults: A randomized controlled trial. J. Infect. Dis. 2015, 212, 1692–1700. [Google Scholar] [CrossRef]
- Corti, C.; Fally, M.; Fabricius-Bjerre, A.; Mortensen, K.; Jensen, B.N.; Andreassen, H.; Porsbjerg, C.; Knudsen, J.D.; Jensen, J.-U. Point-of-care procalcitonin test to reduce antibiotic exposure in patients hospitalized with acute exacerbation of COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 1381–1389. [Google Scholar] [CrossRef]
- Ulm, L.; Hoffmann, S.; Nabavi, D.; Hermans, M.; Mackert, B.-M.; Hamilton, F.; Schmehl, I.; Jungehuelsing, G.-J.; Montaner, J.; Bustamante, A.; et al. The randomized controlled STRAWINSKI trial: Procalcitonin-guided antibiotic therapy after stroke. Front. Neurol. 2017, 8, 153. [Google Scholar] [CrossRef]
- Bremmer, D.N.; DiSilvio, B.E.; Hammer, C.; Beg, M.; Vishwanathan, S.; Speredelozzi, D.; Moffa, M.A.; Hu, K.; Abdulmassih, R.; Makadia, J.T.; et al. Impact of procalcitonin guidance on management of adults hospitalized with chronic obstructive pulmonary disease exacerbations. J. Gen. Intern. Med. 2018, 33, 692–697. [Google Scholar] [CrossRef]
- Daubin, C.; Valette, X.; Thiollière, F.; Mira, J.P.; Hazera, P.; Annane, D.; Labbe, V.; Floccard, B.; Fournel, F.; Terzi, N.; et al. Procalcitonin algorithm to guide initial antibiotic therapy in acute exacerbations of COPD admitted to the ICU: A randomized multicenter study. Intensive Care Med. 2018, 44, 428–437. [Google Scholar] [CrossRef]
- Huang, D.T.; Yealy, D.M.; Filbin, M.R.; Brown, A.M.; Chang, C.-C.H.; Doi, Y.; Donnino, M.W.; Fine, J.; Fine, M.J.; Fischer, M.A.; et al. Procalcitonin-guided use of antibiotics for lower respiratory tract infection. N. Engl. J. Med. 2018, 379, 236–249. [Google Scholar] [CrossRef]
- van der Does, Y.; Limper, M.; Jie, K.E.; Schuit, S.C.E.; Jansen, H.; Pernot, N.; van Rosmalen, J.; Poley, M.J.; Ramakers, C.; Patka, P.; et al. Procalcitonin-guided antibiotic therapy in patients with fever in a general emergency department population: A multicentre non-inferiority randomized clinical trial (HiTEMP study). Clin. Microbiol. Infect. 2018, 24, 1282–1289. [Google Scholar] [CrossRef]
- Townsend, J.; Adams, V.; Galiatsatos, P.; Pearse, D.; Pantle, H.; Masterson, M.; Kisuule, F.; Jacob, E.; Kiruthi, C.; Ortiz, P.; et al. Procalcitonin-guided antibiotic therapy reduces antibiotic use for lower respiratory tract infections in a united states medical center: Results of a clinical trial. Open Forum Infect. Dis. 2018, 5, ofy327. [Google Scholar] [CrossRef]
- Montassier, E.; Javaudin, F.; Moustafa, F.; Nandjou, D.; Maignan, M.; Hardouin, J.-B.; Annoot, C.; Ogielska, M.; Orer, P.-L.; Schotté, T.; et al. Guideline-based clinical assessment versus procalcitonin-guided antibiotic use in pneumonia: A pragmatic randomized trial. Ann. Emerg. Med. 2019, 74, 580–591. [Google Scholar] [CrossRef]
- Akagi, T.; Nagata, N.; Wakamatsu, K.; Harada, T.; Miyazaki, H.; Takeda, S.; Ushijima, S.; Aoyama, T.; Yoshida, Y.; Yatsugi, H.; et al. Procalcitonin-guided antibiotic discontinuation might shorten the duration of antibiotic treatment without increasing pneumonia recurrence. Am. J. Med. Sci. 2019, 358, 33–44. [Google Scholar] [CrossRef]
- Möckel, M.; De Boer, R.A.; Slagman, A.; Von Haehling, S.; Schou, M.; Vollert, J.O.; Wiemer, J.C.; Ebmeyer, S.; Martín-Sánchez, F.J.; Maisel, A.S.; et al. Improve management of acute heart failure with ProcAlCiTonin in EUrope: Results of the randomized clinical trial IMPACT EU Biomarkers in Cardiology (BIC)18. Eur. J. Heart Fail. 2020, 22, 267–275. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and treatment of adults with community-acquired pneumonia, an official clinical practice guideline of the American thoracic society and infectious diseases society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration. FDA News Release: FDA Clears Test to Help Manage Antibiotic Treatment for Lower Respiratory Tract Infections and Sepsis. 2017. Available online: https://www.fda.gov/news-events/press-announcements/fda-clears-test-help-manage-antibiotic-treatment-lower-respiratory-tract-infections-and-sepsis (accessed on 29 January 2022).
- Nobre, V.; Harbarth, S.; Graf, J.D.; Rohner, P.; Pugin, J. Use of procalcitonin to shorten antibiotic treatment duration in septic patients: A randomized trial. Am. J. Respir. Crit. Care Med. 2008, 177, 498–505. [Google Scholar] [CrossRef]
- Schroeder, S.; Hochreiter, M.; Koehler, T.; Schweiger, A.-M.; Bein, B.; Keck, F.S.; Von Spiegel, T. Procalcitonin (PCT)-guided algorithm reduces length of antibiotic treatment in surgical intensive care patients with severe sepsis: Results of a prospective randomized study. Langenbecks Arch. Surg. 2009, 394, 221–226. [Google Scholar] [CrossRef]
- Hochreiter, M.; Köhler, T.; Schweiger, A.M.; Keck, F.S.; Bein, B.; Von Spiegel, T.; Schroeder, S. Procalcitonin to guide duration of antibiotic therapy in intensive care patients: A randomized prospective controlled trial. Crit. Care 2009, 13, R83. [Google Scholar] [CrossRef]
- Stolz, D.; Smyrnios, N.; Eggimann, P.; Pargger, H.; Thakkar, N.; Siegemund, M.; Marsch, S.; Azzola, A.; Rakic, J.; Mueller, B.; et al. Procalcitonin for reduced antibiotic exposure in ventilator-associated pneumonia: A randomised study. Eur. Respir. J. 2009, 34, 1364–1375. [Google Scholar] [CrossRef]
- Bouadma, L.; Luyt, C.-E.; Tubach, F.; Cracco, C.; Alvarez, A.; Schwebel, C.; Schortgen, F.; Lasocki, S.; Veber, B.; Dehoux, M.; et al. Use of procalcitonin to reduce patients’ exposure to antibiotics in intensive care units (PRORATA trial): A multicentre randomised controlled trial. Lancet 2010, 375, 463–474. [Google Scholar] [CrossRef]
- Jensen, J.U.; Hein, L.; Lundgren, B.; Bestle, M.H.; Mohr, T.T.; Andersen, M.H.; Thornberg, K.J.; Løken, J.; Steensen, M.; Fox, Z.; et al. Procalcitonin-guided interventions against infections to increase early appropriate antibiotics and improve survival in the intensive care unit: A randomized trial. Crit. Care Med. 2011, 39, 2048–2058. [Google Scholar] [CrossRef]
- Layios, N.; Lambermont, B.; Canivet, J.-L.; Morimont, P.; Preiser, J.-C.; Garweg, C.; LeDoux, D.; Frippiat, F.; Piret, S.; Giot, J.-B.; et al. Procalcitonin usefulness for the initiation of antibiotic treatment in intensive care unit patients. Crit. Care Med. 2012, 40, 2304–2309. [Google Scholar] [CrossRef]
- Qu, R.; Ji, Y.; Ling, Y.; Ye, C.Y.; Yang, S.M.; Liu, Y.Y.; Yang, R.Y.; Luo, Y.F.; Guo, Z. Procalcitonin is a good tool to guide duration of antibiotic therapy in patients with severe acute pancreatitis. A randomized prospective single-center controlled trial. Saudi Med. J. 2012, 33, 382–387. [Google Scholar]
- Deliberato, R.O.; Marra, A.R.; Sanches, P.R.; Martino, M.D.V.; Ferreira, C.E.D.S.; Pasternak, J.; Paes, A.T.; Pinto, L.M.; dos Santos, O.F.P.; Edmond, M. Clinical and economic impact of procalcitonin to shorten antimicrobial therapy in septic patients with proven bacterial infection in an intensive care setting. Diagn. Microbiol. Infect. Dis. 2013, 76, 266–271. [Google Scholar] [CrossRef]
- Oliveira, C.F.; Botoni, F.A.; Oliveira, C.R.; Silva, C.B.; Pereira, H.A.; Serufo, J.C.; Nobre, V. Procalcitonin versus C-reactive protein for guiding antibiotic therapy in sepsis: A randomized trial. Crit. Care Med. 2013, 41, 2336–2343. [Google Scholar] [CrossRef]
- Annane, D.; Maxime, V.; Faller, J.P.; Mezher, C.; Clec’h, C.; Martel, P.; Gonzales, H.; Feissel, M.; Cohen, Y.; Capellier, G.; et al. Procalcitonin levels to guide antibiotic therapy in adults with non-microbiologically proven apparent severe sepsis: A randomised controlled trial. BMJ Open 2013, 3, e002186. [Google Scholar] [CrossRef]
- Shehabi, Y.; Sterba, M.; Garrett, P.M.; Rachakonda, K.S.; Stephens, D.; Harrigan, P.; Walker, A.; Bailey, M.; Johnson, B.; Millis, D.; et al. Procalcitonin algorithm in critically ill adults with undifferentiated infection or suspected sepsis. A randomized controlled trial. Am. J. Respir. Crit. Care Med. 2014, 190, 1102–1110. [Google Scholar] [CrossRef]
- de Jong, E.; van Oers, J.A.; Beishuizen, A.; Vos, P.; Vermeijden, W.J.; Haas, L.E.; Loef, B.G.; Dormans, T.; van Melsen, G.C.; Kluiters, Y.C.; et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: A randomised, controlled, open-label trial. Lancet Infect. Dis. 2016, 16, 819–827. [Google Scholar] [CrossRef]
- Bloos, F.; Trips, E.; Nierhaus, A.; Briegel, J.; Heyland, D.K.; Jaschinski, U.; Moerer, O.; Weyland, A.; Marx, G.; Gründling, M.; et al. Effect of sodium selenite administration and procalcitonin-guided therapy on mortality in patients with severe sepsis or septic shock: A randomized clinical trial. JAMA Intern. Med. 2016, 176, 1266–1276. [Google Scholar] [CrossRef]
- Jeon, K.; Suh, J.K.; Jang, E.J.; Cho, S.; Ryu, H.G.; Na, S.; Hong, S.B.; Lee, H.J.; Kim, J.Y.; Lee, S.M. Procalcitonin-guided treatment on duration of antibiotic therapy and cost in septic patients (PRODA): A multi-center randomized controlled trial. J. Korean Med. Sci. 2019, 34, e110. [Google Scholar] [CrossRef]
- Beye, F.; Vigneron, C.; Dargent, A.; Prin, S.; Andreu, P.; Large, A.; Quenot, J.P.; Bador, J.; Bruyere, R.; Charles, P.E. Adhering to the procalcitonin algorithm allows antibiotic therapy to be shortened in patients with ventilator-associated pneumonia. J. Crit. Care 2019, 53, 125–131. [Google Scholar] [CrossRef]
- Kyriazopoulou, E.; Liaskou-Antoniou, L.; Adamis, G.; Panagaki, A.; Melachroinopoulos, N.; Drakou, E.; Marousis, K.; Chrysos, G.; Spyrou, A.; Alexiou, N.; et al. Procalcitonin to reduce long-term infection-associated adverse events in sepsis. A randomized trial. Am. J. Respir. Crit. Care Med. 2021, 203, 202–210. [Google Scholar] [CrossRef]
- Chomba, R.N.; Moeng, M.S.; Lowman, W. Procalcitonin-guided antibiotic therapy for suspected and confirmed sepsis of patients in a surgical trauma ICU: A prospective, two period cross-over, interventional study. S. Afr. J. Surg. 2020, 5, 143–149. [Google Scholar] [CrossRef]
- Mazlan, M.Z.; Ismail, M.A.; Ali, S.; Salmuna, Z.N.; Shukeri, W.F.W.M.; Omar, M. Efficacy and safety of the point-of-care procalcitonin test for determining the antibiotic treatment duration in patients with ventilator-associated pneumonia in the intensive care unit: A randomised controlled trial. Anaesthesiol. Intensive Ther. 2021, 53, 207–214. [Google Scholar] [CrossRef]
- Vishalashi, S.G.; Gupta, P.; Verma, P.K. Serum procalcitonin as a biomarker to determine the duration of antibiotic therapy in adult patients with sepsis and septic shock in intensive care units: A prospective study. Indian J. Crit. Care Med. 2021, 25, 507–511. [Google Scholar]
- Use of a Respiratory Multiplex PCR and Procalcitonin to Reduce Antibiotics Exposure in Patients with Severe Confirmed COVID-19 Pneumonia (MultiCov). Available online: https://clinicaltrials.gov/ct2/show/NCT04334850 (accessed on 29 January 2022).
- Voiriot, G.; Fartoukh, M.; Durand-Zaleski, I.; Berard, L.; Rousseau, A.; Armand-Lefevre, L.; Verdet, C.; Argaud, L.; Klouche, K.; Megarbane, B.; et al. Combined use of a broad-panel respiratory multiplex PCR and procalcitonin to reduce duration of antibiotics exposure in patients with severe community-acquired pneumonia (MULTI-CAP): A multicentre, parallel-group, open-label, individual randomised trial conducted in French intensive care units. BMJ Open 2021, 11, e048187. [Google Scholar]
- Andriolo, B.N.; Andriolo, R.B.; Salomão, R.; Atallah, Á.N. Effectiveness and safety of procalcitonin evaluation for reducing mortality in adults with sepsis, severe sepsis or septic shock. Cochrane Database Syst. Rev. 2017, 1, CD010959. [Google Scholar] [CrossRef]
- Huang, H.B.; Peng, J.M.; Weng, L.; Wang, C.Y.; Jiang, W.; Du, B. Procalcitonin-guided antibiotic therapy in intensive care unit patients: A systematic review and meta-analysis. Ann. Intensive Care 2017, 7, 114. [Google Scholar] [CrossRef]
- Schuetz, P.; Wirz, Y.; Sager, R.; Christ-Crain, M.; Stolz, D.; Tamm, M.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; et al. Effect of procalcitonin-guided antibiotic treatment on mortality in acute respiratory infections: A patient level meta-analysis. Lancet Infect. Dis. 2018, 18, 95–107. [Google Scholar] [CrossRef]
- Wirz, Y.; Meier, M.A.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; Tubach, F.; Schroeder, S.; Nobre, V.; Annane, D.; et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: A patient-level meta-analysis of randomized trials. Crit. Care 2018, 22, 191. [Google Scholar] [CrossRef]
- Lam, S.W.; Bauer, S.R.; Fowler, R.; Duggal, A. Systematic review and meta-analysis of procalcitonin-guidance versus usual care for antimicrobial management in critically ill patients: Focus on subgroups based on antibiotic initiation, cessation, or mixed strategies. Crit. Care Med. 2018, 46, 684–690. [Google Scholar] [CrossRef]
- Iankova, I.; Thompson-Leduc, P.; Kirson, N.Y.; Rice, B.; Hey, J.; Krause, A.; Schonfeld, S.A.; DeBrase, C.R.; Bozzette, S.; Schuetz, P. Efficacy and safety of procalcitonin guidance in patients with suspected or confirmed sepsis: A systematic review and meta-analysis. Crit. Care Med. 2018, 46, 691–698. [Google Scholar] [CrossRef]
- Pepper, D.J.; Sun, J.; Rhee, C.; Welsh, J.; Powers, J.H., III; Danner, R.L.; Kadri, S.S. Procalcitonin-guided antibiotic discontinuation and mortality in critically ill adults: A systematic review and meta-analysis. Chest 2019, 155, 1109–1118. [Google Scholar] [CrossRef]
- Peng, F.; Chang, W.; Xie, J.F.; Sun, Q.; Qiu, H.B.; Yang, Y. Ineffectiveness of procalcitonin-guided antibiotic therapy in severely critically ill patients: A meta-analysis. Int. J. Infect. Dis. 2019, 85, 158–166. [Google Scholar] [CrossRef]
- Arulkumaran, N.; Khpal, M.; Tam, K.; Baheerathan, A.; Corredor, C.; Singer, M. Effect of antibiotic discontinuation strategies on mortality and infectious complications in critically ill septic patients: A meta-analysis and trial sequential analysis. Crit. Care Med. 2020, 48, 757–764. [Google Scholar] [CrossRef]
- Meier, M.A.; Branche, A.; Neeser, O.L.; Wirz, Y.; Haubitz, S.; Bouadma, L.; Wolff, M.; Luyt, C.E.; Chastre, J.; Tubach, F.; et al. Procalcitonin-guided antibiotic treatment in patients with positive blood cultures: A patient-level meta-analysis of randomized trials. Clin. Infect. Dis. 2019, 69, 388–396. [Google Scholar] [CrossRef]
- Heilmann, E.; Gregoriano, C.; Wirz, Y.; Luyt, C.E.; Wolff, M.; Chastre, J.; Tubach, F.; Christ-Crain, M.; Bouadma, L.; Annane, D.; et al. Association of kidney function with effectiveness of procalcitonin-guided antibiotic treatment: A patient-level meta-analysis from randomized controlled trials. Clin. Chem. Lab. Med. 2020, 59, 441–453. [Google Scholar] [CrossRef]
- Heilmann, E.; Gregoriano, C.; Annane, D.; Reinhart, K.; Bouadma, L.; Wolff, M.; Chastre, J.; Luyt, C.-E.; Tubach, F.; Branche, A.R.; et al. Duration of antibiotic treatment using procalcitonin-guided treatment algorithms in older patients: A patient-level meta-analysis from randomized controlled trials. Age Ageing 2021, 50, 1546–1556. [Google Scholar] [CrossRef]
- Gutiérrez-Pizarraya, A.; León-García, M.D.C.; De Juan-Idígoras, R.; Garnacho-Montero, J. Clinical impact of procalcitonin-based algorithms for duration of antibiotic treatment in critically ill adult patients with sepsis: A meta-analysis of randomized clinical trials. Expert Rev. Anti-Infect. Ther. 2022, 20, 103–112. [Google Scholar] [CrossRef]
- Schuetz, P.; Wahl, P.M. Additional real-world evidence supporting procalcitonin as an effective tool to improve antibiotic management and cost of the critically ill patient. Chest 2017, 151, 6–8. [Google Scholar] [CrossRef]
- Schuetz, P.; Batschwaroff, M.; Dusemund, F.; Albrich, W.; Bürgi, U.; Maurer, M.; Brutsche, M.; Huber, A.R.; Müller, B. Effectiveness of a procalcitonin algorithm to guide antibiotic therapy in respiratory tract infections outside of study conditions: A post-study survey. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 269–277. [Google Scholar] [CrossRef]
- Hohn, A.; Heising, B.; Hertel, S.; Baumgarten, G.; Hochreiter, M.; Schroeder, S. Antibiotic consumption after implementation of a procalcitonin-guided antimicrobial stewardship programme in surgical patients admitted to an intensive care unit: A retrospective before-and-after analysis. Infection 2015, 43, 405–412. [Google Scholar] [CrossRef]
- Walsh, T.L.; DiSilvio, B.E.; Hammer, C.; Beg, M.; Vishwanathan, S.; Speredelozzi, D.; Moffa, M.A.; Hu, K.; Abdulmassih, R.; Makadia, J.T.; et al. Impact of procalcitonin guidance with an educational program on management of adults hospitalized with pneumonia. Am. J. Med. 2018, 131, 201.e1–201.e8. [Google Scholar] [CrossRef]
- Balk, R.A.; Kadri, S.S.; Cao, Z.; Robinson, S.B.; Lipkin, C.; Bozzette, S.A. Effect of procalcitonin testing on health-care utilization and costs in critically ill patients in the United States. Chest 2017, 151, 23–33. [Google Scholar] [CrossRef]
- Newton, J.A.; Robinson, S.; Ling, C.L.L.; Zimmer, L.; Kuper, K.; Trivedi, K.K. Impact of procalcitonin levels combined with active intervention on antimicrobial stewardship in a community hospital. Open Forum Infect. Dis. 2019, 6, ofz355. [Google Scholar] [CrossRef]
- Collins, C.D.; Brockhaus, K.; Sim, T.; Suneja, A.; Malani, A.N. Analysis to determine cost-effectiveness of procalcitonin-guided antibiotic use in adult patients with suspected bacterial infection and sepsis. Am. J. Health Syst. Pharm. 2019, 76, 1219–1225. [Google Scholar] [CrossRef]
- Westwood, M.; Ramaekers, B.; Whiting, P.; Tomini, F.; Joore, M.; Armstrong, N.; Ryder, S.; Stirk, L.; Severens, H.; Kleijnen, J. Procalcitonin testing to guide antibiotic therapy for the treatment of sepsis in intensive care settings and for suspected bacterial infection in emergency department settings: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2015, 19, 3–236. [Google Scholar] [CrossRef]
- Langford, B.J.; Beriault, D.; Schwartz, K.L.; Seah, J.; Pasic, M.D.; Cirone, R.; Chan, A.; Downing, M. A real-world assessment of procalcitonin combined with antimicrobial stewardship in a community ICU. J. Crit. Care 2020, 57, 130–133. [Google Scholar] [CrossRef]
- Broyles, M.R. Impact of procalcitonin-guided antibiotic management on antibiotic exposure and outcomes: Real-world evidence. Open Forum Infect. Dis. 2017, 4, ofx213. [Google Scholar] [CrossRef]
- Gluck, E.; Nguyen, H.B.; Yalamanchili, K.; McCusker, M.; Madala, J.; Corvino, F.A.; Zhu, X.; Balk, R. Real-world use of procalcitonin and other biomarkers among sepsis hospitalizations in the United States: A retrospective, observational study. PLoS ONE 2018, 13, e0205924. [Google Scholar] [CrossRef]
- Chambliss, A.B. Embracing procalcitonin for antimicrobial stewardship. J. Appl. Lab. Med. 2019, 3, 712–715. [Google Scholar] [CrossRef]
- Christensen, I.; Haug, J.B.; Berild, D.; Bjørnholt, J.V.; Jelsness-Jørgensen, L.P. Hospital physicians’ experiences with procalcitonin—Implications for antimicrobial stewardship; a qualitative study. BMC Infect. Dis. 2020, 20, 515. [Google Scholar] [CrossRef]
- von Dach, E.; Albrich, W.C.; Brunel, A.S.; Prendki, V.; Cuvelier, C.; Flury, D.; Gayet-Ageron, A.; Huttner, B.; Kohler, P.; Lemmenmeier, E.; et al. Effect of C-reactive protein-guided antibiotic treatment duration, 7-day treatment, or 14-day treatment on 30-day clinical failure rate in patients with uncomplicated gram-negative bacteremia: A randomized clinical trial. JAMA 2020, 323, 2160–2169. [Google Scholar] [CrossRef]
- Borges, I.; Carneiro, R.; Bergo, R.; Martins, L.; Colosimo, E.; Oliveira, C.; Saturnino, S.; Andrade, M.V.; Ravetti, C.; Nobre, V. Duration of antibiotic therapy in critically ill patients: A randomized controlled trial of a clinical and C-reactive protein-based protocol versus an evidence-based best practice strategy without biomarkers. Crit. Care 2020, 24, 281. [Google Scholar] [CrossRef]
- Shozushima, T.; Takahashi, G.; Matsumoto, N.; Kojika, M.; Okamura, Y.; Endo, S. Usefulness of presepsin (sCD14-ST) measurements as a marker for the diagnosis and severity of sepsis that satisfied diagnostic criteria of systemic inflammatory response syndrome. J. Infect. Chemother. 2011, 17, 764–769. [Google Scholar] [CrossRef]
- Xiao, H.; Wang, G.; Wang, Y.; Tan, Z.; Sun, X.; Zhou, J.; Duan, M.; Zhi, D.; Tang, Z.; Hang, C.; et al. Potential value of presepsin guidance in shortening antibiotic therapy in septic patients: A multicenter, prospective cohort trial. Shock 2022, 57, 63–71. [Google Scholar] [CrossRef]
- Hellyer, T.P.; McAuley, D.F.; Walsh, T.S.; Anderson, N.; Morris, A.C.; Singh, S.; Dark, P.; Roy, A.I.; Perkins, G.D.; McMullan, R.; et al. Biomarker-guided antibiotic stewardship in suspected ventilator-associated pneumonia (VAPrapid2): A randomised controlled trial and process evaluation. Lancet Respir. Med. 2020, 8, 182–191. [Google Scholar] [CrossRef]
- Karakike, E.; Giamarellos-Bourboulis, E.J.; Kyprianou, M.; Fleischmann-Struzek, C.; Pletz, M.W.; Netea, M.G.; Reinhart, K.; Kyriazopoulou, E. Coronavirus disease 2019 as cause of viral sepsis: A systematic review and meta-analysis. Crit. Care Med. 2021, 49, 2042–2057. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Zhu, N.; Ranganathan, N.; Skolimowska, K.; Gilchrist, M.; Satta, G.; Cooke, G.; Holmes, A.H. Bacterial and fungal coinfection in individuals with coronavirus: A rapid review to support COVID-19 antimicrobial prescribing. Clin. Infect. Dis. 2020, 71, 2459–2468. [Google Scholar] [CrossRef]
- Arentz, M.; Yim, E.; Klaff, L.; Lokhandwala, S.; Riedo, F.X.; Chong, M.; Lee, M. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington state. JAMA 2020, 323, 1612–1614. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 Novel coronavirus-infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Goyal, P.; Choi, J.J.; Pinheiro, L.C.; Schenck, E.J.; Chen, R.; Jabri, A.; Satlin, M.J.; Campion, T.R., Jr.; Nahid, M.; Ringel, J.B.; et al. Clinical characteristics of Covid-19 in New York city. N. Engl. J. Med. 2020, 382, 2372–2374. [Google Scholar] [CrossRef]
- Atallah, N.J.; Warren, H.M.; Roberts, M.B.; Elshaboury, R.H.; Bidell, M.R.; Gandhi, R.G.; Adamsick, M.; Ibrahim, M.K.; Sood, R.; Eddine, S.B.Z.; et al. Baseline procalcitonin as a predictor of bacterial infection and clinical outcomes in COVID-19: A case-control study. PLoS ONE 2022, 17, e0262342. [Google Scholar] [CrossRef]
- Houghton, R.; Moore, N.; Williams, R.; El-Bakri, F.; Peters, J.; Mori, M.; Vernet, G.; Lynch, J.; Lewis, H.; Tavener, M.; et al. C-reactive protein-guided use of procalcitonin in COVID-19. JAC Antimicrob. Resist. 2021, 3, dlab180. [Google Scholar] [CrossRef]
- Zattera, L.; Veliziotis, I.; Benitez-Cano, A.; Ramos, I.; Larrañaga, L.; Nuñez, M.; Román, L.; Adalid, I.; Ferrando, C.; Muñoz, G.; et al. Early procalcitonin to predict mortality in critically ill COVID-19 patients: A multicentric cohort study. Minerva Anestesiol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Cheng, C.; Zheng, X.; Jin, Y.; Duan, G.; Chen, M.; Chen, S. Elevated procalcitonin is positively associated with the severity of COVID-19: A meta-analysis based on 10 cohort studies. Medicina 2021, 57, 594. [Google Scholar] [CrossRef] [PubMed]
- Van Berkel, M.; Kox, M.; Frenzel, T.; Pickkers, P.; Schouten, J. Biomarkers for antimicrobial stewardship: A reappraisal in COVID-19 times? Crit. Care 2020, 24, 600. [Google Scholar] [CrossRef] [PubMed]
- Richards, O.; Pallmann, P.; King, C.; Cheema, Y.; Killick, C.; Thomas-Jones, E.; Harris, J.; Bailey, C.; Szakmany, T. Procalcitonin increase is associated with the development of critical care-acquired infections in COVID-19 ARDS. Antibiotics 2021, 10, 1425. [Google Scholar] [CrossRef] [PubMed]
- Pink, I.; Raupach, D.; Fuge, J.; Vonberg, R.-P.; Hoeper, M.M.; Welte, T.; Rademacher, J. C-reactive protein and procalcitonin for antimicrobial stewardship in COVID-19. Infection 2021, 49, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Kooistra, E.J.; van Berkel, M.; van Kempen, N.F.; van Latum, C.R.; Bruse, N.; Frenzel, T.; van den Berg, M.J.; Schouten, J.A.; Kox, M.; Pickkers, P. Dexamethasone and tocilizumab treatment considerably reduces the value of C-reactive protein and procalcitonin to detect secondary bacterial infections in COVID-19 patients. Crit. Care 2021, 25, 281. [Google Scholar] [CrossRef]
- Moseley, P.; Jackson, N.; Omar, A.; Eldoadoa, M.; Samaras, C.; Birk, R.; Ahmed, F.; Chakrabarti, P. Single-centre experience of using procalcitonin to guide antibiotic therapy in COVID-19 intensive care patients. J. Hosp. Infect. 2022, 119, 194–195. [Google Scholar] [CrossRef]
- Calderon, M.; Li, A.; Bazo-Alvarez, J.C.; Dennis, J.; Baker, K.F.; van der Loeff, I.S.; Hanrath, A.T.; Capstick, R.; Payne, B.A.I.; Weiand, D.; et al. Evaluation of procalcitonin-guided antimicrobial stewardship in patients admitted to hospital with COVID-19 pneumonia. JAC Antimicrob. Resist. 2021, 3, dlab133. [Google Scholar] [CrossRef]
- Williams, E.J.; Mair, L.; de Silva, T.I.; Green, D.J.; House, P.; Cawthron, K.; Gillies, C.; Wigfull, J.; Parsons, H.; Partridge, D.G. Evaluation of procalcitonin as a contribution to antimicrobial stewardship in SARS-CoV-2 infection: A retrospective cohort study. J. Hosp. Infect. 2021, 110, 103–107. [Google Scholar] [CrossRef]
- Staub, M.B.; Ouedraogo, Y.; Evans, C.D.; Katz, S.E.; Talley, P.P.; Kainer, M.A.; Nelson, G.E. Analysis of a high-prescribing state’s 2016 outpatient antibiotic prescriptions: Implications for outpatient antimicrobial stewardship interventions. Infect. Control Hosp. Epidemiol. 2020, 41, 135–142. [Google Scholar] [CrossRef]


{kind=link}
| Ref | Trial Setting | PCT Algorithm Applied | N of Patients | Main Results |
|---|---|---|---|---|
| [7] | LRTI—ED Single-center—Switzerland | Initiation-cessation | PCT: 124 SOC: 119 | Prescription of antimicrobials: 44% vs. 83%, p < 0.0001 LOT: 10.3 vs. 12.8 days, p < 0.0001 Decreased cost |
| [8] | CAP (requiring hospitalization) Single-center—Switzerland | Initiation-cessation | PCT: 151 SOC: 151 | Prescription of antimicrobials: 85% vs. 99%, p < 0.0001 LOT: 5.8 vs. 12.9 days, p < 0.0001 Decreased cost |
| [9] | COPD exacerbation—ED Single-center—Switzerland | Initiation-cessation | PCT: 113 SOC: 113 | Prescription of antimicrobials: 40% vs. 72%, p < 0.0001 |
| [10] | Symptoms compatible with respiratory (upper/lower) infection—prehospital Multicenter—Switzerland | Initiation-cessation | PCT: 230 SOC: 223 | Restriction in activity at day 14: 0.14 (95% CI: −0.53 to 0.81) Prescription of antimicrobials: decrease 72% (95% CI: 66–78) |
| [11] | CAP (requiring hospitalization) Multicenter—Denmark | Initiation with PCT > 0.25 ng/mL | PCT: 103 SOC: 107 | LOT: 5.1 vs. 6.8 days, p = 0.007 |
| [12] | CAP (requiring hospitalization) Multicenter—Switzerland | Initiation-cessation | PCT: 687 SOC: 694 | Total adverse outcomes: 15.4% vs. 18.9%, OR −3.5 (95% CI: −7.6 to 0.4) LOT: 5.7 vs. 8.7 days, p < 0.05 AE due to antimicrobials: 19.8% vs. 28.1%, p < 0.05 |
| [13] | Symptoms compatible with respiratory (upper/lower) infection—prehospital | Initiation-cessation | PCT: 275 SOC: 275 | Restriction in activity at day 14: 0.04 (95% CI: 0.73 to 0.81) Prescription of antimicrobials: 21.5% vs. 36.7%, p < 0.0005 |
| [14] | CAP (requiring hospitalization) Single-center—Shanghai | Initiation-cessation | PCT: 81 SOC: 81 | Prescription of antimicrobials: 84.4% vs. 97.5%, p = 0.004 LOT: 5 vs. 7 days, p < 0.001 |
| [15] | Acute asthma exacerbation Single-center—Shanghai | Initiation | PCT: 132 SOC: 133 | Prescription of antimicrobials: 46.1% vs. 74.8%, p < 0.01 |
| [16] | Aspiration pneumonia Single-center—Japan | If initial PCT < 0.5 ng/mL treat 3 days; if 0.5–1.0 treat for 5 days; if >1.0 treat for 7 days; stop with decrease ≥90% | PCT: 53 SOC: 52 | Relapse (30 days): 25% vs. 37.5%, p = 0.19 LOT: 5 vs. 8 days, p< 0.0001 |
| [17] | Acute asthma exacerbation Single-center—Shanghai | Initiation | PCT: 90 SOC: 90 | Prescription of antimicrobials: 48.9% vs. 87.8%, p< 0.001 LOT: 6 vs. 6 days, p = 0.198 Exacerbation (1 year): 78.8% vs. 82.1%, p = 0.586 |
| [18] | COPD exacerbation Multicenter—Italy | Stop after 3 days if PCT < 0.25 ng/mL; if not treat for 10 days | PCT: 88 SOC: 90 | Exacerbation rate difference (6 months): 4.04% (90% CI: −7.23 to 15.31) |
| [19] | LRTI (requiring hospitalization)—ED Single-center—USA | Initiation, combined with multiplex PCR | PCT:151 SOC: 149 | LOT: 3 vs. 4 days, p = 0.42 Duration of symptoms: 16 vs. 20 days, p = 0.03 |
| [20] | COPD exacerbation Single-center—Denmark | Initiation-cessation | PCT: 62 SOC: 58 | LOT: 3.5 vs. 8.5 days, p = 0.0169 Patients (%) under treatment ≥5 days: 41.9 vs. 67.2, p = 0.006 |
| [21] | After stroke Multicenter—International | Initiation | PCT: 112 SOC: 115 | modified Rankin Scale (3 months): 4 vs. 4, p = 0.452 Prescription of antimicrobials: 63% vs. 45%, p = 0.01 |
| [22] * | COPD exacerbation Single-center—USA | Initiation | Before:139 After: 166 | LOT: 3 vs. 5.3 days, p = 0.01 Length of hospital stay: 2.9 vs. 4.1 days, p = 0.01 Rehospitalization (30 days): 16.6% vs. 14.5%, p = 0.25 |
| [23] | COPD exacerbation Multicenter—France | Initiation-cessation | PCT: 151 SOC: 151 | Mortality (3 months): 20% vs. 14%, LOT: no difference |
| [24] | LRTI—ED Multicenter—USA | Initiation-cessation | PCT: 826 SOC: 830 | LOT: 4.2 vs. 4.3 days, difference −0.05 (95% CI −0.6 to 0.5) Prescription of antimicrobials (30 days): 57% vs. 61.8% Length of hospital stay: 4.7 vs. 5.0 days |
| [25] | Fever ≥ 38.2 °C—ED (main infection [40%] respiratory) Two-center—Netherlands | Initiation | PCT: 275 SOC: 276 | Prescription of antimicrobials: 73% vs. 77%, p = 0.28 Readmission at ED (14 days): 7% vs. 10%, p = 0.20 Hospitalization: 74% vs. 81%, p = 0.10 Mortality (30 days): 2% vs. 4%, p = 0.11 |
| [26] ** | LRTI (requiring hospitalization)—ED Single-center—USA | Initiation-cessation | After: 174 Before: 200 | LOT: 5 vs. 6 days, p = 0.052 LOT-pneumonia: 6 vs. 7 days, p = 0.045 LOT-COPD exacerbation: 3 vs. 4 days, p = 0.01 |
| [27] | CAP—ED Multicenter—France | Initiation-cessation | PCT: 142 SOC: 143 | LOT:10 vs. 9 days, p = 0.21 AE: 15% vs. 20%, difference 5% (95% CI: −4 to 14%) Mortality (30 days): 1% vs. 2%, p > 0.05 |
| [28] *** | CAP and/or HCAP Single-center—Japan | Cessation cutoff 0.2 ng/mL | PCT: 116 SOC: 116 | LOT: 8 vs. 11 days, p < 0.001 Relapse (30 days): 4.3% vs. 6.0%, p = 0.5541 |
| [29] | Symptoms of acute heart failure—ED Multicenter—International | Initiation cutoff 0.2 ng/mL | PCT: 370 SOC: 372 | Mortality (90 days): 10.3% vs. 8.2%, p = 0.316 Mortality (30 days): 6.8% vs. 4.3%, p = 0.152 Prescription of antimicrobials: 18% vs. 14%, p = 0.145 Rehospitalization (30 days): 17.3 vs. 9.7%, p = 0.004 |
| Ref | Trial Setting | PCT Algorithm Applied | N of Patients | Main Results |
|---|---|---|---|---|
| [32] | Severe sepsis and septic shock (65% respiratory infections) Single-center—Switzerland | Cessation if ≥90% decrease or PCT < 0.25 ng/mL | PCT: 31 SOC: 37 | LOT: 3.5 vs. 6 days, p = 0.15 (ITT) 6 vs. 10 days, p = 0.003 (PP) Length of ICU stay: 4 vs. 7 days, p = 0.02 |
| [33] | Severe sepsis after intraabdominal surgery Single-center—Germany | Cessation if PCT < 1 ng/mL for 3 consecutive days | PCT: 14 SOC: 13 | LOT: 6.6 vs. 8.3 days, p < 0.001 |
| [34] | Sepsis Single-center—Germany | Cessation if PCT < 1 ng/mL or ≥65% decrease for 3 serial days | PCT: 57 SOC: 53 | LOT: 5.9 vs. 7.9 days, p < 0.001 Length of ICU stay: 15.5 vs. 17.7 days, p = 0.046 |
| [35] | VAP Multicenter—Switzerland and USA | Initiation-cessation | PCT: 50 SOC: 51 | LOT: 7 vs. 11 days, p = 0.044 |
| [36] | Sepsis (mainly [70%] respiratory infections) Multicenter—France | Initiation-cessation | PCT: 307 SOC: 314 | LOT: 6.1 vs. 9.9 days, p < 0.0001 Relapse: absolute difference 1.4% Reinfection: absolute difference 3.6% |
| [37] | Suspected infection Multicenter—Denmark | Up-escalation when PCT > 1.0 ng/mL | PCT: 604 SOC: 596 | Significantly higher antimicrobial consumption in PCT group |
| [38] | Suspected infection (60% respiratory infections) Single-center—Belgium | Initiation | PCT: 258 SOC: 251 | Antimicrobial consumption (% days in ICU): 62.6 vs. 57.7, p = 0.11 |
| [39] | Acute pancreatitis Single-center—China | Initiation-cessation PCT cutoff: 0.5 ng/mL | PCT: 35 SOC: 36 | LOT: 10.89 vs. 16.06 days, p < 0.001 Length of stay: 16.66 vs. 23.81 days, p < 0.001 |
| [40] | Sepsis Single-center—Brazil | Cessation if PCT < 0.5 ng/mL or ≥90% decrease | PCT: 42 SOC: 39 | LOT: 10 vs. 11 days, p = 0.44 (ITT) 9 vs. 13 days, p = 0.008 (PP) |
| [41] | Sepsis (60% respiratory infections) Two-center—Brazil | Cessation PCT < 0.1 ng/mL or ≥90% from baseline CRP < 25 mg/L or ≥50% decrease from baseline | PCT: 50 CRP: 47 | LOT: 7 vs. 6 days, p = 0.06 Mortality: 32.7% vs. 33.3%, p = 1.000 |
| [42] | Sepsis Multicenter—France | Initiation-cessation | PCT: 27 SOC: 26 | Patients (%) under treatment at day 5: 67 vs. 81, p = 0.24 |
| [43] | Suspected sepsis Multicenter—Australia | Initiation-cessation Cessation when PCT < 0.10 ng/mL or ≥90% decrease from baseline | PCT: 196 SOC: 198 | LOT: 9 vs. 11 days, p = 0.58 Total doses of antimicrobials: 1200 vs. 1500, p = 0.001 |
| [44] | Sepsis Multicenter—Netherlands | Cessation if PCT < 0.5 ng/mL or ≥80% from baseline for 2 serial days | PCT: 761 SOC: 785 | LOT: 5 vs. 7 days, p < 0.0001 Mortality (28 days):19.6% vs. 25%, p = 0.0122 Mortality (1 year): 34.8% vs. 40.9%, p = 0.0158 |
| [45] | Sepsis Multicenter—Germany | Cessation if PCT < 1.0 ng/mL or ≥50% decrease | PCT: 552 SOC: 537 | Mortality: 25.6% vs. 28.2%, p = 0.34 Antimicrobials/1000 ICU days: 823 vs. 862, decrease 4.5%, p = 0.02 |
| [46] | Severe sepsis and/or septic shock Multicenter—Korea | Cessation if PCT < 0.5 ng/mL or ≥90% from baseline | PCT: 23 SOC: 29 | LOT:10 vs. 13 days, p = 0.078 (ΙΤΤ), 8 vs. 14 days, p < 0.001 (PP) Mortality (28 days): 17% vs. 21%, p = 0.709 |
| [47] * | VAP Multicenter—France | Initiation-cessation | PCT: 76 No-PCT: 81 | LOT: 8 vs. 9.5 days, p = 0.02 Death and/or relapse: 51.3% vs. 46.9%, p = 0.47 |
| [48] | Sepsis-3 Multicenter—Greece | Cessation if PCT < 0.5 ng/mL or ≥80% decrease from baseline | PCT: 125 SOC: 131 | LOT: 5 vs. 10 days; p < 0.001 Mortality (28 days): 15.2% vs. 28.2%, p = 0.02 |
| [49] ** | Surgical trauma Single center—South Africa | Cessation if PCT < 0.5 ng/mL or ≥80% from baseline | PCT: 40 SOC: 40 | LOT: 9.3 vs. 10.9 days, p = 0.10 Mortality: 15% vs. 30%, p = 0.045 |
| [50] | VAP Single center—Malaysia | Cessation if PCT < 0.5 ng/mL or ≥80% from baseline | PCT: 43 SOC: 42 | LOT: 10.28 vs. 11.52 days, difference −1.25 (95%CI −2.48 to 0.01), p = 0.049 |
| [51] | Sepsis and septic shock Single center—India | Cessation if PCT < 0.01 ng/mL or ≥80% from baseline | PCT: 45 SOC: 45 | LOT: 4.98 vs. 7.73 days, p < 0.001 Length of ICU stay: 5.98 vs. 8.80 days, p < 0.001 Secondary infections: 4.4% vs. 26.7%, p = 0.014 Mortality: 8.9% vs. 15.6%, p = 0.522 Readmission: no difference |
| Ref | N of Trials | N of Patients | Focus of Interest | Main Results |
|---|---|---|---|---|
| [54] | 10 | 1215 | NA | Antibiotic duration (days): −1.28 days (95% CI −1.95 to −0.61) Mortality: RR 0.81 (95% CI 0.65 to 1.01) |
| [55] | 13 | 5136 | Antibiotic Initiation, Cessation, or Mixed Strategies | Antibiotic duration (days): −1.66 (95% CI −2.36 to −0.96) Mortality: RR 0.87 (95% CI 0.76 to 0.98) |
| [56] | 26 | 6708 | Acute respiratory infections | Antibiotic duration (days): −2.4 (95% CI −2.71 to −2.15) Mortality: OR 0.83 (95% CI 0.70 to 0.99) Antibiotic-related side-effects: OR 0.68 (95% CI 0.57 to 0.82) |
| [57] | 11 | 4482 | Subgroup of sepsis-3 | Antibiotic duration (days): −1.19 (95% CI −1.73 to −0.66) Mortality: OR 0.89 (95% CI 0.80 to 0.99) Sepsis-3, OR 0.86 (95% CI 0.76 to 0.98) |
| [58] | 15 | Antibiotic Initiation, Cessation, or Mixed Strategies | Antibiotic duration (days): −1.26 (p < 0.001) and −3.10 (p = 0.04) for cessation and mixed strategies, respectively Mortality: OR 1.00 (95% CI 0.86 to 1.15), 0.87 (95% CI 0.77 to 0.98), and 1.01 (95% CI 0.80 to 1.29) for the initiation, cessation, and mixed procalcitonin strategies, respectively | |
| [59] | 10 | 3489 | Suspected or confirmed sepsis | Antibiotic duration (days): −1.49 (95% CI −2.27 to −0.71) Mortality: RR 0.90 (95% CI 0.79 to1.03) |
| [60] | 16 | 5158 | Subgroup (5 trials) with high algorithm adherence | Mortality: RR 0.89 (95% CI 0.83 to 0.97) In high algorithm adherence, RR 0.93 (95% CI 0.71 to 1.22) |
| [61] | 16 | 6452 | NA | Antibiotic duration (days): −0.99 (95% CI −1.85 to −0.13), p = 0.02 Mortality: OR 0.90 (95% CI 0.80 to1.01) |
| [62] | 14 | 4744 | NA | Antibiotic duration (days): −1.23 (95% CI −1.61 to −0.85) Mortality: OR 0.91 (95% CI 0.82 to 1.01) |
| [63] | 13 | 523 (IPD) | Positive blood culture | Antibiotic duration (days): −2.86 (95% CI −4.88 to −0.84) Mortality: 16.6% vs. 20.0%, p = 0.263 |
| [64] | 15 | 5002 (IPD) | Kidney function (3 groups: GFR > 90, GFR 15–89 and GFR < 15) | Antibiotic duration (days): −2.06 (95% CI −2.87 to −1.25), −1.72 (95% CI −2.29 to −1.16), −2.49 (95% CI −3.59 to −1.40), pinteraction = 0.336. Overall, −2.01 (95% CI −2.45 to −1.58) Mortality: OR 1.08 (95% CI 0.79 to 1.49), 0.74 (95% CI 0.63 to 0.87), 1.03 (95% CI 0.83 to 1.29), pinteraction = 0.888. Overall, 0.88 (95% CI 0.78 to 0.98) |
| [65] | 28 | 9421 (IPD) | Age (4 groups: <75, 75–80, 81–85 and >85 years) | Antibiotic duration per age group (days): Less than 75 years: −1.99 (95% CI −2.36 to −1.62); 75–80 years: −1.98 (95% CI −2.94 to −1.02); 81–85 years: −2.20 (95% CI −3.15 to −1.25), more than 85 years: −2.10 (95% CI −3.29 to −0.91), pinteraction = 0.654. Overall, −2.01 (95% CI −2.32 to −1.69) Mortality: Less than 75 years: OR 0.87 (95% CI 0.76 to 1.00); 75–80 years 0.86 (95% CI 0.67 to 1.10); 81–85 years 1.19 (95% CI 0.76 to 1.06), pinteraction = 0.891. Overall, 0.90 (95% CI 0.81 to 1.00) |
| [66] | 12 | 42,921 | NA | Antibiotic duration (days): 1.98 days (95% CI: −2.76, −1.21) Mortality: RR 0.89 (95% CI 0.79 to 0.99) ICU-length of stay (days): −1.21 (95% CI −4.16 to 1.74) |
| Ref | Type and Setting of Study | N of Patients | Severity of COVID-19 | Main Results |
|---|---|---|---|---|
| [87] | Observational February-March 2020 Single-center, USA | 21 | Critical ICU patients | Median PCT 1.8 (0.12–9.56) |
| [88] | January-February 2020 Single-center, Wuhan China | 138 | Hospitalized Both critical/non-critical | PCT ≥ 0.05 ng/mL in 35.5% of patients Higher levels in patients requiring ICU |
| [90] | Retrospective case series March 2020 Two-center, USA | 393 | Hospitalized Both critical/non-critical | PCT ≥ 0.05 ng/mL in 16.9% of patients Higher levels in patients requiring intubation |
| [91] | Retrospective observational March-April 2020 Single-center, USA | 324 | Hospitalized Both critical/non-critical | PCT for prediction of bacteremia, AUC 0.81 (0.64–0.98) PCT for prediction of bacterial pneumonia, AUC 0.75 (0.64–0.86) |
| [92] | Retrospective observational March-April 2020 Multicenter, UK | 224 | Hospitalized Both critical/non-critical | PCT > 0.5 ng/mL in 16.5% of patients PCT associated with increased risk of death (p = 0.0004) |
| [93] | Retrospective observational March-June 2020 Multicenter, Spain | 777 | Critical ICU patients | PCT 0.64 (0.17–1.44) ng/mL in non-survivors compared to 0.23 (0.11–0.60) ng/mi in survivors, p < 0.01 |
| [95] | Observational Single-center, Netherlands | 66 | Critical ICU patients | PCT > 1.00 ng/mL at admission rule in secondary bacterial infection PCT < 0.25 ng/mL at admission rule out secondary bacterial infection |
| [96] | Retrospective observational March-June 2020 Single-center, UK | 65 | Critical ICU patients | PCT rise in 81.5% of patients PCT rise in 97% of patients with confirmed VAT/VAP and/or BSI |
| [97] | Retrospective observational March-October 2020 Single-center, Germany | 99 | Hospitalized Both critical/non-critical | PCT of patients with secondary bacterial infection 0.4 ng/mL versus 0.1 of those without, p = 0.016 cut-off 0.55 ng/mL: sensitivity 91%, specificity 81% for bacterial infection |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kyriazopoulou, E.; Giamarellos-Bourboulis, E.J. Antimicrobial Stewardship Using Biomarkers: Accumulating Evidence for the Critically Ill. Antibiotics 2022, 11, 367. https://doi.org/10.3390/antibiotics11030367
Kyriazopoulou E, Giamarellos-Bourboulis EJ. Antimicrobial Stewardship Using Biomarkers: Accumulating Evidence for the Critically Ill. Antibiotics. 2022; 11(3):367. https://doi.org/10.3390/antibiotics11030367
Chicago/Turabian StyleKyriazopoulou, Evdoxia, and Evangelos J. Giamarellos-Bourboulis. 2022. "Antimicrobial Stewardship Using Biomarkers: Accumulating Evidence for the Critically Ill" Antibiotics 11, no. 3: 367. https://doi.org/10.3390/antibiotics11030367
APA StyleKyriazopoulou, E., & Giamarellos-Bourboulis, E. J. (2022). Antimicrobial Stewardship Using Biomarkers: Accumulating Evidence for the Critically Ill. Antibiotics, 11(3), 367. https://doi.org/10.3390/antibiotics11030367