
Association between Carbapenem Consumption and Clinical Outcomes in an In-Hospital Setting: Analysis of a Japanese Nationwide Administrative Database in 2020


Abstract
1. Introduction
2. Results
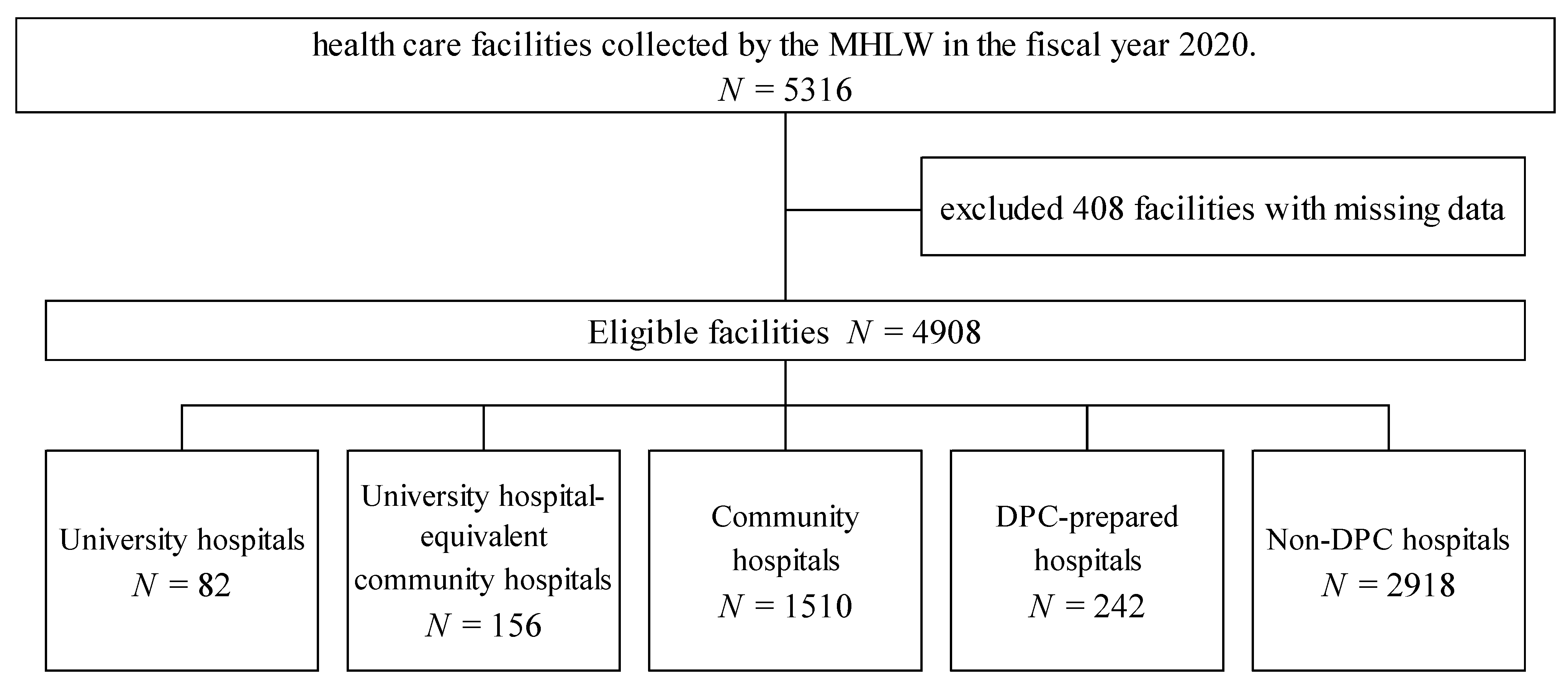
2.1. Characteristics of Hospitals Stratified by Classification of Payment System
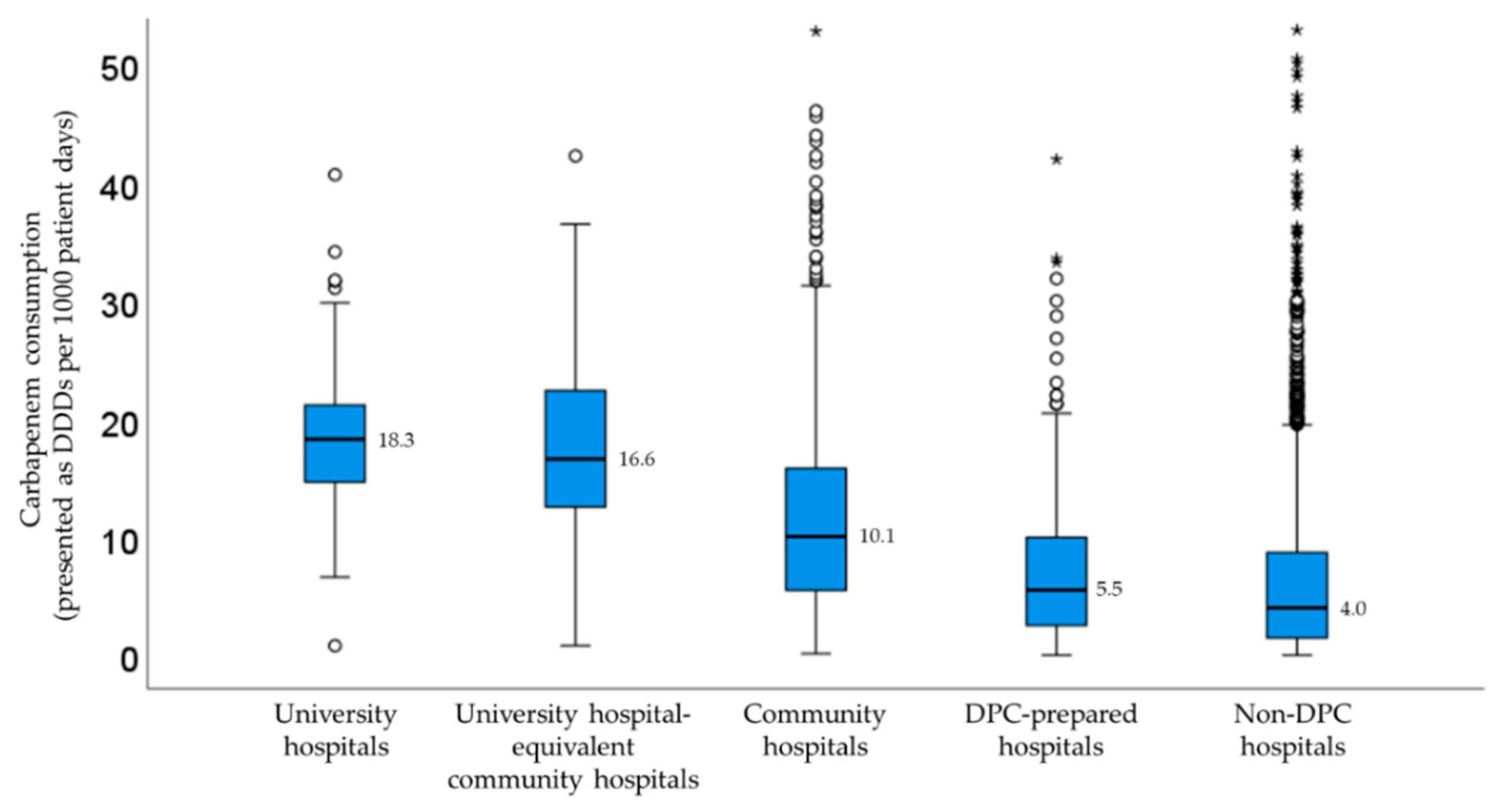
2.2. Correlation Analysis between Carbapenem Consumption and Clinical Outcomes Stratified by Facility Type
2.3. Factors for Carbapenem Consumption Using a Linear Regression Model
3. Discussion
4. Materials and Methods
4.1. Data Sources
4.2. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilson, A.P.R. Sparing carbapenem usage. J. Antimicrob. Chemother. 2017, 72, 2410–2417. [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.S.; Mazuski, J.E.; Bradley, J.S.; Rodvold, K.A.; Goldstein, E.J.C.; Baron, E.J.; O’Neill, P.J.O.; Chow, A.W.; Dellinger, E.P.; Eachempati, S.R.; et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Surg. Infect. 2010, 11, 79–109. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.P.R.; Livermore, D.M.; Otter, J.A.; Warren, R.E.; Jenks, P.; Enoch, D.A.; Newsholme, W.; Oppenheim, B.; Leanord, A.; McNulty, C.; et al. Prevention and control of multi-drug-resistant Gram-negative bacteria: Recommendations from a Joint Working Party. J. Hosp. Infect. 2016, 92, S1–S44. [Google Scholar] [CrossRef] [PubMed]
- Giske, C.G.; Monnet, D.L.; Cars, O.; Carmeli, Y.; ReAct-Action on Antibiotic Resistance. Clinical and economic impact of common multidrug-resistant gram-negative bacilli. Antimicrob. Agents Chemother. 2008, 52, 813–821. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare Japan Nosocomial Infections Surveillance Annual Open Report. Clinical Laboratory Division 2020. Available online: https://janis.mhlw.go.jp/english/report/open_report/2020/3/1/ken_Open_Report_Eng_202000_clsi2012.pdf (accessed on 14 October 2022).
- Oka, K.; Matsumoto, A.; Tetsuka, N.; Morioka, H.; Iguchi, M.; Ishiguro, N.; Nagamori, T.; Takahashi, S.; Saito, N.; Tokuda, K.; et al. Clinical characteristics and treatment outcomes of carbapenem-resistant Enterobacterales infections in Japan. J. Glob. Antimicrob. Resist. 2022, 29, 247–252. [Google Scholar] [CrossRef] [PubMed]
- The Government of Japan: National Action Plan on Antimicrobial Resistance (AMR), 2016–2020. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000120172.html (accessed on 14 October 2022).
- Seah, V.X.F.; Ong, R.Y.L.; Lim, A.S.Y.; Chong, C.Y.; Tan, N.W.H.; Thoon, K.C. Impact of a carbapenem antimicrobial stewardship program on patient outcomes. Antimicrob. Agents Chemother. 2017, 61, e00736-17. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Maeda, M.; Yokoe, T.; Hashiguchi, M.; Togashi, M.; Ishino, K. Impact of the multidisciplinary antimicrobial stewardship team intervention focusing on carbapenem de-escalation: A single-centre and interrupted time series analysis. Int. J. Clin. Pract. 2021, 75, e13693. [Google Scholar] [CrossRef]
- Lau, C.L.; Periyasamy, P.; Saud, M.N.; Robert, S.A.; Gan, L.Y.; Chin, S.Y.; Pau, K.B.; Kong, S.H.; Tajurudin, F.W.; Yin, M.K.; et al. Plethora of antibiotics usage and evaluation of carbapenem prescribing pattern in intensive care units: A single-center experience of Malaysian academic hospital. Antibiotics 2022, 11, 1172. [Google Scholar] [CrossRef]
- Wells, D.A.; Johnson, A.J.; Lukas, J.G.; Mason, D.; Cleveland, K.O.; Bissell, A.; Hobbs, A.L.V. Criteria Restricting Inappropriate Meropenem Empiricism (CRIME): A quasi-experimental carbapenem restriction pilot at a large academic medical centre. Int. J. Antimicrob. Agents 2022, 60, 106661. [Google Scholar] [CrossRef]
- Yamasaki, D.; Tanabe, M.; Muraki, Y.; Kato, G.; Ohmagari, N.; Yagi, T. The first report of Japanese antimicrobial use measured by national database based on health insurance claims data (2011–2013): Comparison with sales data, and trend analysis stratified by antimicrobial category and age group. Infection 2018, 46, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Ebisui, A.; Inose, R.; Kusama, Y.; Koizumi, R.; Kawabe, A.; Ishii, S.; Goto, R.; Ishikane, M.; Yagi, T.; Ohmagari, N.; et al. Trends in antipseudomonal agent use based on the 2006 to 2015 sales data in Japan. Biol. Pharm. Bull. 2021, 44, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Terahara, F.; Nishiura, H. Carbapenem-resistant Pseudomonas aeruginosa and carbapenem use in Japan: An ecological study. J. Int. Med. Res. 2019, 47, 4711–4722. [Google Scholar] [CrossRef] [PubMed]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare, Japan: The Fiscal Year 2018 Revision of Reimbursement of Medical Fees. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000188411.html (accessed on 14 October 2022).
- Maeda, M.; Muraki, Y.; Kosaka, T.; Yamada, T.; Aoki, Y.; Kaku, M.; Kawaguchi, T.; Seki, M.; Tanabe, Y.; Fujita, N.; et al. The first nationwide survey of antimicrobial stewardship programs conducted by the Japanese Society of Chemotherapy. J. Infect. Chemother. 2019, 25, 83–88. [Google Scholar] [CrossRef] [PubMed]
- Maeda, M.; Muraki, Y.; Kosaka, T.; Yamada, T.; Aoki, Y.; Kaku, M.; Seki, M.; Tanabe, Y.; Fujita, N.; Niki, Y.; et al. Impact of health policy on structural requisites for antimicrobial stewardship: A nationwide survey conducted in Japanese hospitals after enforcing the revised reimbursement system for antimicrobial stewardship programs. J. Infect. Chemother. 2021, 27, 1–6. [Google Scholar] [CrossRef]
- Matsuda, S.; Fujimori, K.; Kuwabara, K.; Ishikawa, K.B.; Fushimi, K. Diagnosis procedure combination as an infrastructure for the clinical study. Asian Pac. J. Dis. Manag. 2011, 5, 81–87. [Google Scholar] [CrossRef]
- Hayashida, K.; Murakami, G.; Matsuda, S.; Fushimi, K. History and profile of diagnosis procedure combination (DPC): Development of a real data collection system for acute inpatient care in Japan. J. Epidemiol. 2021, 31, 1–11. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare Health “Survey on Impact Assessment of DPC Introduction: Summary of Statistics”. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000049343.html (accessed on 14 October 2022).
- World Health Organization Anatomical Therapeutic Chemical (ATC) Classification. Available online: https://www.who.int/tools/atc-ddd-toolkit/atc-classification (accessed on 14 October 2022).
- Polk, R.E.; Fox, C.; Mahoney, A.; Letcavage, J.; MacDougall, C. Measurement of adult antibacterial drug use in 130 US hospitals: Comparison of defined daily dose and days of therapy. Clin. Infect. Dis. 2007, 44, 664–670. [Google Scholar] [CrossRef]
- Kuster, S.P.; Ruef, C.; Ledergerber, B.; Hintermann, A.; Deplazes, C.; Neuber, L.; Weber, R. Quantitative antibiotic use in hospitals: Comparison of measurements, literature review, and recommendations for a standard of reporting. Infection 2008, 36, 549–559. [Google Scholar] [CrossRef]
- Gravatt, L.A.H.; Pakyz, A.L. Challenges in measuring antibiotic consumption. Curr. Infect. Dis. Rep. 2013, 15, 559–563. [Google Scholar] [CrossRef]
- Mizuno, K.; Inose, R.; Matsui, Y.; Takata, M.; Yamasaki, D.; Kusama, Y.; Koizumi, R.; Ishikane, M.; Tanabe, M.; Ohge, H.; et al. Search for indexes to evaluate trends in antibiotic use in the sub-prefectural regions using the national database of health insurance claims and specific health checkups of Japan. Antibiotics 2022, 11, 763. [Google Scholar] [CrossRef] [PubMed]
- Kagami, K.; Ishiguro, N.; Yamada, T.; Niinuma, Y.; Iwasaki, S.; Taki, K.; Fukumoto, T.; Hayasaka, K.; Nishida, M.; Sugita, J.; et al. Clinical outcomes of intervention for carbapenems and anti-methicillin-resistant Staphylococcus aureus antibiotics by an antimicrobial stewardship team. Am. J. Infect. Control 2021, 49, 1493–1498. [Google Scholar] [CrossRef] [PubMed]
- Naito, Y.; Maeda, M.; Nagatomo, Y.; Ugajin, K.; Akima, E.; Tanaka, M.; Tokimatsu, I.; Sasaki, T. Impact of the antimicrobial stewardship team intervention focusing on changes in prescribing trends and the rate of carbapenem-resistant P. aeruginosa. Yakugaku Zasshi 2022, 142, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Umemura, T.; Mutoh, Y.; Maeda, M.; Hagihara, M.; Ohta, A.; Mizuno, T.; Kato, H.; Sukawa, M.; Yamada, T.; Ikeda, Y.; et al. Impact of hospital environmental cleaning with a potassium peroxymonosulphate-based environmental disinfectant and antimicrobial stewardship on the reduction of hospital-onset Clostridioides difficile infections. J. Hosp. Infect. 2022, 129, 181–188. [Google Scholar] [CrossRef]
- Tamma, P.D.; Aitken, S.L.; Bonomo, R.A.; Mathers, A.J.; van Duin, D.; Clancy, C.J. Infectious Diseases Society of America guidance on the treatment of AmpC β-lactamase-producing Enterobacterales, carbapenem-resistant Acinetobacter baumannii, and Stenotrophomonas maltophilia infections. Clin. Infect. Dis. 2022, 74, 2089–2114. [Google Scholar] [CrossRef]
- Harris, P.N.A.; Tambyah, P.A.; Lye, D.C.; Mo, Y.; Lee, T.H.; Yilmaz, M.; Alenazi, T.H.; Arabi, Y.; Falcone, M.; Bassetti, M.; et al. MERINO Trial Investigators and the Australasian Society for Infectious Disease Clinical Research Network (ASID-CRN). Effect of Piperacillin-Tazobactam vs. Meropenem on 30-Day Mortality for Patients with E coli or Klebsiella pneumoniae Bloodstream Infection and Ceftriaxone Resistance: A Randomized Clinical Trial. JAMA 2018, 320, 984–994. [Google Scholar]
- Maeda, M.; Muraki, Y.; Anno, Y.; Sawa, A.; Kusama, Y.; Ishikane, M.; Ohmagari, N.; Ohge, H. Development of the predicted and standardized carbapenem usage metric: Analysis of the Japanese Diagnosis Procedure Combination payment system data. J. Infect. Chemother. 2020, 26, 633–635. [Google Scholar] [CrossRef]
- Rhodes, N.J.; Wagner, J.L.; Davis, S.L.; Bosso, J.A.; Goff, D.A.; Rybak, M.J.; Scheetz, M.H.; MAD-ID Research Network. Trends in and predictors of carbapenem consumption across North American hospitals: Results from a multicenter survey by the MAD-ID research network. Antimicrob. Agents Chemother. 2019, 63, e00327-19. [Google Scholar] [CrossRef]
- Wagner, J.L.; Rhodes, N.J.; Scheetz, M.H.; Bosso, J.A.; Goff, D.A.; Rybak, M.J.; Davis, S.L.; MAD-ID Research Network. Opportunities for antimicrobial stewardship among carbapenem-treated patients in 18 North American hospitals. Int. J. Antimicrob. Agents 2020, 55, 105970. [Google Scholar] [CrossRef]
- Maeda, M.; Muraki, Y.; Kosaka, T.; Yamada, T.; Aoki, Y.; Kaku, M.; Seki, M.; Tanabe, Y.; Fujita, N.; Niki, Y.; et al. Essential human resources for antimicrobial stewardship teams in Japan: Estimates from a nationwide survey conducted by the Japanese Society of Chemotherapy. J. Infect. Chemother. 2019, 25, 653–656. [Google Scholar] [CrossRef]
- Maeda, M.; Miyake, T.; Inose, R.; Ueda, S.; Matsugi, K.-I.; Muraki, Y.; Kitahara, T. Bibliometric analysis of pharmacist’s research on antimicrobial stewardship in Japan: An interrupted time series analysis on the implementation of the certification system for infection control pharmacists. J. Pharm. Health Care Sci. 2021, 7, 38. [Google Scholar] [CrossRef]
- van Santen, K.L.; Edwards, J.R.; Webb, A.K.; Pollack, L.A.; O’Leary, E.; Neuhauser, M.M.; Srinivasan, A.; Pollock, D.A. The standardized antimicrobial administration ratio: A new metric for measuring and comparing antibiotic use. Clin. Infect. Dis. 2018, 67, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, O.M.; Polk, R.E. Antimicrobial use metrics and benchmarking to improve stewardship outcomes: Methodology, opportunities, and challenges. Infect. Dis. Clin. N. Am. 2014, 28, 195–214. [Google Scholar] [CrossRef] [PubMed]
- Kagami, K.; Ishiguro, N.; Iwasaki, S.; Usami, T.; Fukumoto, T.; Hayasaka, K.; Oyamada, R.; Watanabe, T.; Nakakubo, S.; Niinuma, Y.; et al. Correlation between antibiotic use and antibiotic resistance: A multicenter study using the Japan Surveillance for Infection Prevention and Healthcare Epidemiology (J-SIPHE) system in Hokkaido, Japan. Am. J. Infect. Control, 2022; in press. [Google Scholar] [CrossRef]
- Endo, A.; Asai, Y.; Tajima, T.; Endo, M.; Akiyama, T.; Matsunaga, N.; Ishioka, H.; Tsuzuki, S.; Ohmagari, N. Temporal trends in microbial detection during the COVID-19 pandemic: Analysis of the Japan surveillance for Infection Prevention and Healthcare Epidemiology (J-SIPHE) database. J. Infect. Chemother. 2022, 29, 98–101. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| University Hospitals (N = 82) | University Hospital-Equivalent Community Hospitals (N = 156) | Community Hospitals (N = 1510) | DPC-Prepared Hospitals (N = 242) | Non-DPC Hospitals (N = 2918) | |
|---|---|---|---|---|---|
| Number of licensed beds | 821 (643–968) | 578 (477–675) | 260 (180–367) | 148 (102–199) | 107 (64–168) |
| Outcome at discharge | |||||
| Cure (%) | 77.17 (71.97–83.85) | 81.24 (77.09–85.71) | 82.66 (76.84–87.04) | 81.80 (72.69–87.62) | 76.83 (62.61–86.21) |
| Remission (%) | 0.23 (0.066–0.406) | 0.13 (0.03–0.56) | 0.06 (0–0.31) | 0.03 (0–0.29) | 0 (0–0.66) |
| Stable disease (%) | 12.54 (5.68–18.03) | 8.08 (3.58–11.60) | 6.15 (2.79–10.89) | 6.37 (2.67–12.28) | 7.05 (2.45–13.55) |
| Exacerbation (%) | 0.063 (0.024–0.13) | 0.03 (0.01–0.13) | 0.12 (0.03–0.32) | 0.40 (0.11–0.84) | 0.63 (0–1.76) |
| Death (%) | 1.43 (1.08–1.795) | 2.57 (2.04–3.19) | 3.62 (2.51–5.12) | 4.41 (2.56–6.75) | 6.87 (2.93–12.22) |
| Others (%) | 8.54 (5.68–10.54) | 7.11 (5.44–8.98) | 5.22 (2.74–7.96) | 2.27 (0.43–6.22) | 0.65 (0–4.37) |
| Readmission within 4 weeks (%) | 14.51 (12.68–16.55) | 12.47 (10.55–14.69) | 9.93 (7.31–12.76) | 8.04 (4.50–12.01) | 5.73 (3.14–9.75) |
| Average length of stay (day) | 12.14 (11.60–12.98) | 11.39 (10.81–12.14) | 12.15 (10.71–13.54) | 12.78 (10.49–15.30) | 14.46 (10.93–18.22) |
| Spearman’s Correlation Coefficient (ρ) | p-Value | |
|---|---|---|
| University hospitals | ||
| Cure rate | −0.068 | 0.541 |
| Rate of readmission within 4 weeks | −0.311 | 0.004 |
| Average length of stay | −0.001 | 0.993 |
| University hospital-equivalent community hospitals | ||
| Cure rate | −0.111 | 0.167 |
| Rate of readmission within 4 weeks | 0.13 | 0.098 |
| Average length of stay | 0.021 | 0.792 |
| Community hospitals | ||
| Cure rate | −0.056 | 0.03 |
| Rate of readmission within 4 weeks | 0.342 | <0.001 |
| Average length of stay | 0.007 | 0.794 |
| DPC-prepared hospitals | ||
| Cure rate | −0.113 | 0.081 |
| Rate of readmission within 4 weeks | 0.483 | <0.001 |
| Average length of stay | −0.014 | 0.829 |
| Non-DPC hospitals | ||
| Cure rate | −0.098 | <0.001 |
| Rate of readmission within 4 weeks | 0.265 | <0.001 |
| Average length of stay | 0.005 | 0.811 |
| Factors | Partial Regression Coefficient (95% Confidence Interval) | p-Value | |
|---|---|---|---|
| Model 1 a (university hospitals) | |||
| MDC 03 (ear, nose, mouth, and throat) | 106.643 | (5.581–207.705) | 0.039 |
| MDC 16 (injuries, burns, poisoning, and toxic effect of drugs) | 133.498 | (22.872–244.124) | 0.019 |
| Constant term | 9.683 | (3.800–15.565) | 0.002 |
| Model 2 b (university hospital-equivalent community hospitals) | |||
| MDC 13 (blood and immunological disorders) | 92.997 | (32.170–153.824) | 0.003 |
| Constant term | 13.930 | (11.352–16.508) | 0.000 |
| Model 3 c (community hospitals) | |||
| Cure rate | 9.955 | (5.687–14.222) | 0.000 |
| Rate of readmission within 4 weeks | 15.361 | (5.878–24.843) | 0.002 |
| Average length of stay | 0.176 | (0.016–0.335) | 0.031 |
| Licensed bed size * | 1.188 | (0.931–1.445) | 0.000 |
| MDC 01 (nervous system) | −4.911 | (−8.368 to −1.454) | 0.005 |
| MDC 04 (respiratory system) | 8.127 | (2.221–14.034) | 0.007 |
| MDC 07 (musculoskeletal system) | −12.784 | (−17.522 to −8.046) | 0.000 |
| MDC 09 (breast) | −16.717 | (−27.749 to −5.685) | 0.003 |
| MDC 10 (endocrine, nutritional, and metabolic system) | −19.321 | (−31.693 to −6.950) | 0.002 |
| MDC 13 (blood and immunological disorders) | 62.499 | (48.049–76.950) | 0.000 |
| MDC 14 (newborn) | −24.892 | (−34.774 to −15.009) | 0.000 |
| MDC 16 (injuries, burns, poisoning, and toxic effect of drugs) | −7.841 | (−13.039 to −2.642) | 0.003 |
| MDC 17 (mental disorders) | −169.432 | (−256.636 to −82.227) | 0.000 |
| Model 4 d (DPC-prepared hospitals) | |||
| Cure rate | 12.344 | (4.946–19.742) | 0.001 |
| Rate of readmission within 4 weeks | 31.157 | (14.330–47.984) | 0.000 |
| MDC 02 (eye) | −10.099 | (−19.786 to −0.413) | 0.041 |
| MDC 04 (respiratory system) | 24.198 | (14.422–33.975) | 0.000 |
| MDC 11 (kidney, urinary tract, and male reproductive system) | 13.260 | (5.408–21.112) | 0.001 |
| MDC 15 (pediatric) | −178.586 | (−302.983 to−54.190) | 0.005 |
| MDC 16 (injuries, burns, poisoning, and toxic effect of drugs) | −9.409 | (−16.880 to −1.938) | 0.014 |
| Model 5 e (non-DPC hospitals) | |||
| Cure rate | 1.890 | (0.283–3.498) | 0.021 |
| Rate of readmission within 4 weeks | 19.484 | (14.966–24.002) | 0.000 |
| MDC 04 (respiratory system) | 16.127 | (13.091–19.162) | 0.000 |
| MDC 05 (circulatory system) | 4.174 | (1.417–6.931) | 0.003 |
| MDC 06 (digestive and hepatobiliary system, and pancreas) | 4.790 | (3.475–6.104) | 0.000 |
| MDC 11 (kidney, urinary tract, and male reproductive system) | 7.595 | (5.144–10.047) | 0.000 |
| MDC 13 (blood and immunological disorders) | 26.154 | (17.447–34.861) | 0.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, K.; Maeda, M.; Ohmagari, N.; Muraki, Y. Association between Carbapenem Consumption and Clinical Outcomes in an In-Hospital Setting: Analysis of a Japanese Nationwide Administrative Database in 2020. Antibiotics 2022, 11, 1807. https://doi.org/10.3390/antibiotics11121807
Yamaguchi K, Maeda M, Ohmagari N, Muraki Y. Association between Carbapenem Consumption and Clinical Outcomes in an In-Hospital Setting: Analysis of a Japanese Nationwide Administrative Database in 2020. Antibiotics. 2022; 11(12):1807. https://doi.org/10.3390/antibiotics11121807
Chicago/Turabian StyleYamaguchi, Kozue, Masayuki Maeda, Norio Ohmagari, and Yuichi Muraki. 2022. "Association between Carbapenem Consumption and Clinical Outcomes in an In-Hospital Setting: Analysis of a Japanese Nationwide Administrative Database in 2020" Antibiotics 11, no. 12: 1807. https://doi.org/10.3390/antibiotics11121807
APA StyleYamaguchi, K., Maeda, M., Ohmagari, N., & Muraki, Y. (2022). Association between Carbapenem Consumption and Clinical Outcomes in an In-Hospital Setting: Analysis of a Japanese Nationwide Administrative Database in 2020. Antibiotics, 11(12), 1807. https://doi.org/10.3390/antibiotics11121807