
Antimicrobial Stewardship during COVID-19 Outbreak: A Retrospective Analysis of Antibiotic Prescriptions in the ICU across COVID-19 Waves
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Primary Outcome
2.3. Secondary Outcomes
2.3.1. Empirical Antibiotic Treatment Appropriateness in the COVID-19 Group
2.3.2. Antimicrobial Resistance in the Overall COVID-19 Group
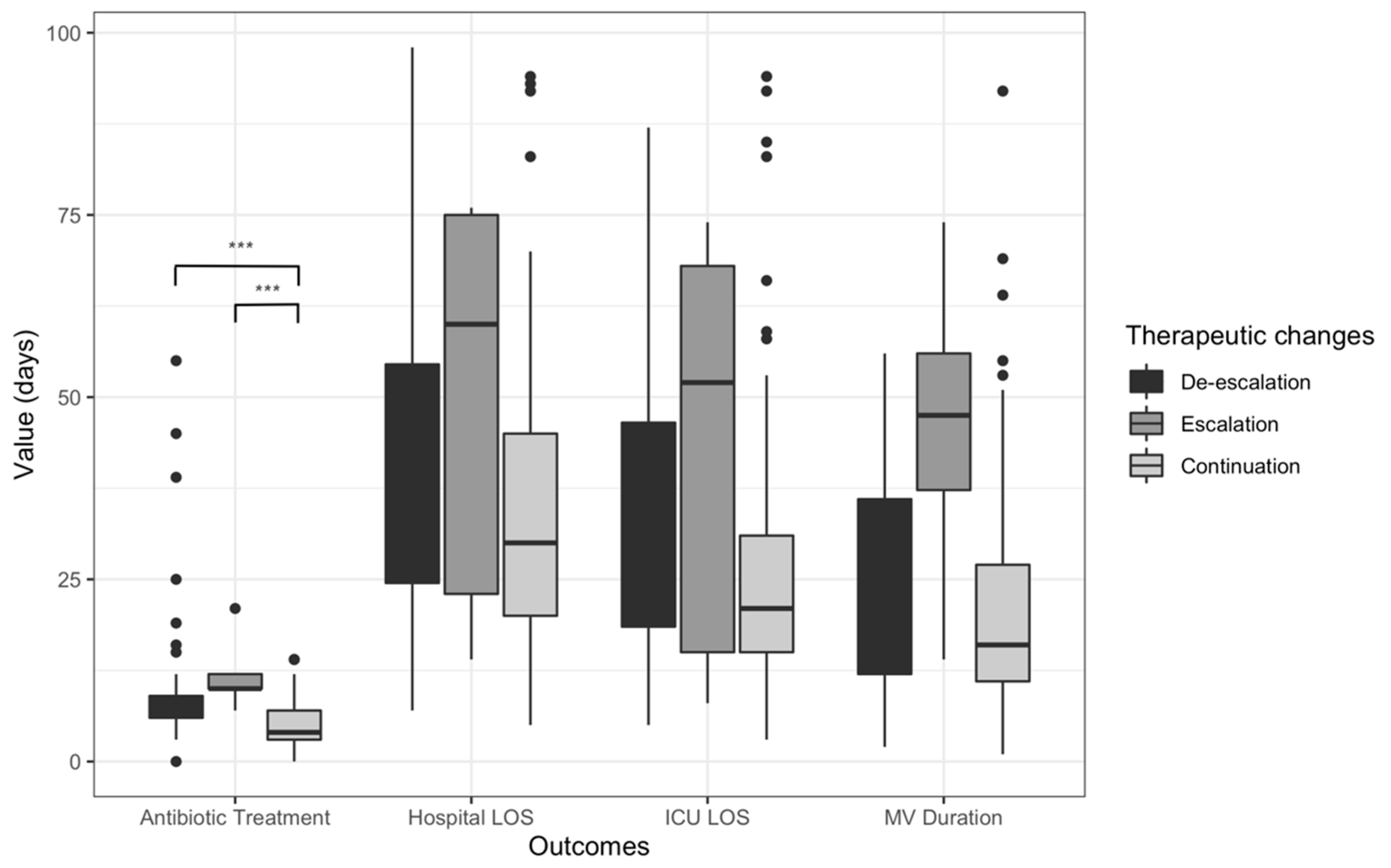
2.3.3. Clinical Outcomes in the COVID-19 Group
2.4. Control Group
3. Discussion
4. Materials and Methods
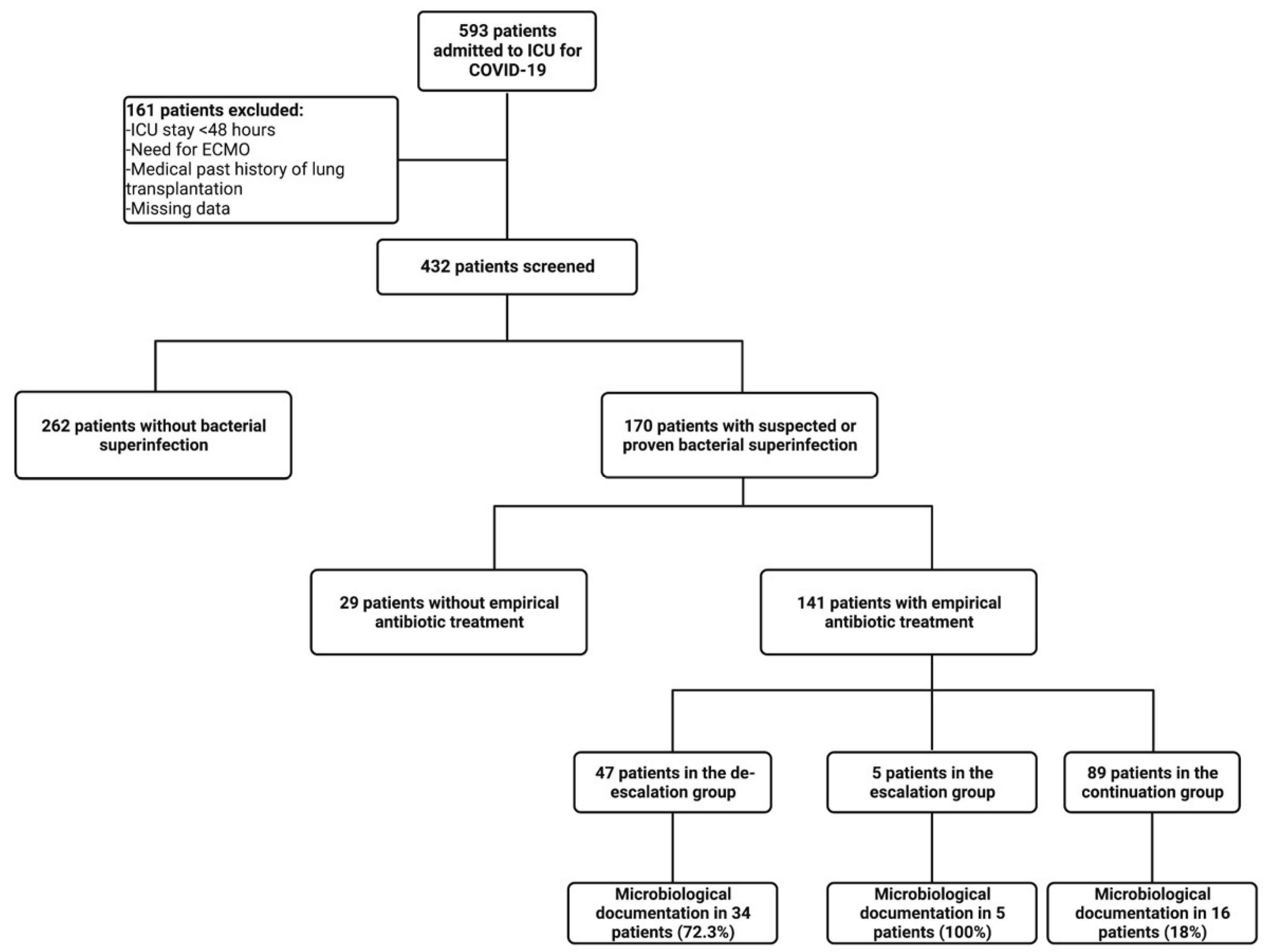
4.1. Study Design and Population
4.2. Extracted Data
4.3. Definitions
4.4. Outcomes
4.5. Control Group
4.6. Ethical Considerations
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amarsy, R.; Trystram, D.; Cambau, E.; Monteil, C.; Fournier, S.; Oliary, J.; Junot, H.; Sabatier, P.; Porcher, R.; Robert, J.; et al. Surging Bloodstream Infections and Antimicrobial Resistance during the First Wave of COVID-19: A Study in a Large Multihospital Institution in the Paris Region. Int. J. Infect. Dis. 2022, 114, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Westblade, L.F.; Simon, M.S.; Satlin, M.J. Bacterial Coinfections in Coronavirus Disease 2019. Trends Microbiol. 2021, 29, 930–941. [Google Scholar] [CrossRef] [PubMed]
- Segala, F.V.; Bavaro, D.F.; Di Gennaro, F.; Salvati, F.; Marotta, C.; Saracino, A.; Murri, R.; Fantoni, M. Impact of SARS-CoV-2 Epidemic on Antimicrobial Resistance: A Literature Review. Viruses 2021, 13, 2110. [Google Scholar] [CrossRef] [PubMed]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider Cytokine Storm Syndromes and Immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Rawson, T.M.; Moore, L.S.P.; Castro-Sanchez, E.; Charani, E.; Davies, F.; Satta, G.; Ellington, M.J.; Holmes, A.H. COVID-19 and the Potential Long-Term Impact on Antimicrobial Resistance. J. Antimicrob. Chemother. 2020, 75, 1681–1684. [Google Scholar] [CrossRef]
- Ferri, M.; Ranucci, E.; Romagnoli, P.; Giaccone, V. Antimicrobial Resistance: A Global Emerging Threat to Public Health Systems. Crit. Rev. Food Sci. Nutr. 2017, 57, 2857–2876. [Google Scholar] [CrossRef]
- Lakbar, I.; Medam, S.; Ronflé, R.; Cassir, N.; Delamarre, L.; Hammad, E.; Lopez, A.; Lepape, A.; Machut, A.; Boucekine, M.; et al. Association between Mortality and Highly Antimicrobial-Resistant Bacteria in Intensive Care Unit-Acquired Pneumonia. Sci. Rep. 2021, 11, 16497. [Google Scholar] [CrossRef]
- Dyar, O.J.; Huttner, B.; Schouten, J.; Pulcini, C. What Is Antimicrobial Stewardship? Clin. Microbiol. Infect. 2017, 23, 793–798. [Google Scholar] [CrossRef] [Green Version]
- Schuts, E.C.; Hulscher, M.E.J.L.; Mouton, J.W.; Verduin, C.M.; Stuart, J.W.T.C.; Overdiek, H.W.P.M.; van der Linden, P.D.; Natsch, S.; Hertogh, C.M.P.M.; Wolfs, T.F.W.; et al. Current Evidence on Hospital Antimicrobial Stewardship Objectives: A Systematic Review and Meta-Analysis. Lancet Infect. Dis. 2016, 16, 847–856. [Google Scholar] [CrossRef]
- Murphy, C.V.; Reed, E.E.; Herman, D.D.; Magrum, B.; Beatty, J.J.; Stevenson, K.B. Antimicrobial Stewardship in the ICU. Semin. Respir. Crit. Care Med. 2022, 43, 131–140. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Sanchis-Gomar, F.; Henry, B.M. Clinical and Demographic Characteristics of Patients Dying from COVID-19 in Italy vs China. J. Med. Virol. 2020, 92, 1759–1760. [Google Scholar] [CrossRef] [PubMed]
- Fried, M.W.; Crawford, J.M.; Mospan, A.R.; Watkins, S.E.; Munoz, B.; Zink, R.C.; Elliott, S.; Burleson, K.; Landis, C.; Reddy, K.R.; et al. Patient Characteristics and Outcomes of 11721 Patients with Coronavirus Disease 2019 (COVID-19) Hospitalized across the United States. Clin. Infect. Dis. 2021, 72, e558–e565. [Google Scholar] [CrossRef] [PubMed]
- Mo, P.; Xing, Y.; Xiao, Y.; Deng, L.; Zhao, Q.; Wang, H.; Xiong, Y.; Cheng, Z.; Gao, S.; Liang, K.; et al. Clinical Characteristics of Refractory Coronavirus Disease 2019 in Wuhan, China. Clin. Infect. Dis. 2021, 73, e4208–e4213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, M.P.; Patel, P.K.; Nori, P. Involving Antimicrobial Stewardship Programs in COVID-19 Response Efforts: All Hands on Deck. Infect. Control Hosp. Epidemiol. 2020, 41, 744–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, T.J.; Davidson, H.C.; Low, J.M.; Basarab, M.; Arnold, A. Antibiotic Usage and Stewardship in Patients with COVID-19: Too Much Antibiotic in Uncharted Waters? J. Infect. Prev. 2021, 22, 119–125. [Google Scholar] [CrossRef]
- Abdela, S.G.; Liesenborghs, L.; Tadese, F.; Abegaz, S.H.; Bayuh, F.B.; Asmamaw, E.A.; Mebrate, T.A.; Mamo, A.E.; Embiale, W.; Hunegnaw, S.; et al. Antibiotic Overuse for COVID-19: Are We Adding Insult to Injury? Am. J. Trop. Med. Hyg. 2021, 105, 1519–1520. [Google Scholar] [CrossRef]
- Meduri, G.U.; Golden, E.; Freire, A.X.; Taylor, E.; Zaman, M.; Carson, S.J.; Gibson, M.; Umberger, R. Methylprednisolone Infusion in Early Severe ARDS. Chest 2007, 131, 954–963. [Google Scholar] [CrossRef] [Green Version]
- Tabah, A.; Cotta, M.O.; Garnacho-Montero, J.; Schouten, J.; Roberts, J.A.; Lipman, J.; Tacey, M.; Timsit, J.-F.; Leone, M.; Zahar, J.R.; et al. A Systematic Review of the Definitions, Determinants, and Clinical Outcomes of Antimicrobial De-Escalation in the Intensive Care Unit. Clin. Infect. Dis. 2016, 62, 1009–1017. [Google Scholar] [CrossRef] [Green Version]
- De Bus, L.; Denys, W.; Catteeuw, J.; Gadeyne, B.; Vermeulen, K.; Boelens, J.; Claeys, G.; De Waele, J.J.; Decruyenaere, J.; Depuydt, P.O. Impact of De-Escalation of β-Lactam Antibiotics on the Emergence of Antibiotic Resistance in ICU Patients: A Retrospective Observational Study. Intensive Care Med. 2016, 42, 1029–1039. [Google Scholar] [CrossRef]
- De Bus, L.; Depuydt, P.; Steen, J.; Dhaese, S.; De Smet, K.; Tabah, A.; Akova, M.; Cotta, M.O.; De Pascale, G.; Dimopoulos, G.; et al. Antimicrobial De-Escalation in the Critically Ill Patient and Assessment of Clinical Cure: The DIANA Study. Intensive Care Med. 2020, 46, 1404–1417. [Google Scholar] [CrossRef]
- For the AZUREA Network Investigators; Leone, M.; Bechis, C.; Baumstarck, K.; Lefrant, J.-Y.; Albanèse, J.; Jaber, S.; Lepape, A.; Constantin, J.-M.; Papazian, L.; et al. De-Escalation versus Continuation of Empirical Antimicrobial Treatment in Severe Sepsis: A Multicenter Non-Blinded Randomized Noninferiority Trial. Intensive Care Med. 2014, 40, 1399–1408. [Google Scholar] [CrossRef] [PubMed]
- Mokart, D.; Slehofer, G.; Lambert, J.; Sannini, A.; Chow-Chine, L.; Brun, J.-P.; Berger, P.; Duran, S.; Faucher, M.; Blache, J.-L.; et al. De-Escalation of Antimicrobial Treatment in Neutropenic Patients with Severe Sepsis: Results from an Observational Study. Intensive Care Med. 2014, 40, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Armand-Lefèvre, L.; Angebault, C.; Barbier, F.; Hamelet, E.; Defrance, G.; Ruppé, E.; Bronchard, R.; Lepeule, R.; Lucet, J.-C.; El Mniai, A.; et al. Emergence of Imipenem-Resistant Gram-Negative Bacilli in Intestinal Flora of Intensive Care Patients. Antimicrob. Agents Chemother. 2013, 57, 1488–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudoignon, E.; Camelena, F.; Leone, M.; Depret, F. What’s New in Antibiotic Stewardship for Pneumonia in ICU? Anaesth. Crit. Care Pain Med. 2022, 41, 101135. [Google Scholar] [CrossRef]
- Lakbar, I.; De Waele, J.J.; Tabah, A.; Einav, S.; Martin-Loeches, I.; Leone, M. Antimicrobial De-Escalation in the ICU: From Recommendations to Level of Evidence. Adv. Ther. 2020, 37, 3083–3096. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Marotta, C.; Amicone, M.; Bavaro, D.F.; Bernaudo, F.; Frisicale, E.M.; Kurotschka, P.K.; Mazzari, A.; Veronese, N.; Murri, R.; et al. Italian Young Doctors’ Knowledge, Attitudes and Practices on Antibiotic Use and Resistance: A National Cross-Sectional Survey. J. Glob. Antimicrob. Resist. 2020, 23, 167–173. [Google Scholar] [CrossRef]
- Leone, M.; Bourgoin, A.; Cambon, S.; Dubuc, M.; Albanèse, J.; Martin, C. Empirical Antimicrobial Therapy of Septic Shock Patients: Adequacy and Impact on the Outcome. Crit. Care Med. 2003, 31, 462–467. [Google Scholar] [CrossRef]
- Tabah, A.; Bassetti, M.; Kollef, M.H.; Zahar, J.-R.; Paiva, J.-A.; Timsit, J.-F.; Roberts, J.A.; Schouten, J.; Giamarellou, H.; Rello, J.; et al. Antimicrobial De-Escalation in Critically Ill Patients: A Position Statement from a Task Force of the European Society of Intensive Care Medicine (ESICM) and European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Critically Ill Patients Study Group (ESGCIP). Intensive Care Med. 2020, 46, 245–265. [Google Scholar] [CrossRef]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the Treatment with β-Lactam Antibiotics in Critically Ill Patients-Guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Société Française d’Anesthésie et Réanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [Green Version]
- Calandra, T.; Cohen, J. The International Sepsis Forum Consensus Conference on Definitions of Infection in the Intensive Care Unit. Crit. Care Med. 2005, 33, 1538–1548. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Crit. Care Med. 2021, 49, e1063–e1143. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.-P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-Resistant, Extensively Drug-Resistant and Pandrug-Resistant Bacteria: An International Expert Proposal for Interim Standard Definitions for Acquired Resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toulouse, E.; Lafont, B.; Granier, S.; Mcgurk, G.; Bazin, J.-E. French Legal Approach to Patient Consent in Clinical Research. Anaesth. Crit. Care Pain Med. 2020, 39, 883–885. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; for the STROBE Initiative. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and Elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (Superinfected Patients) (n= 170) | No Empirical Antibiotic Treatment (n = 29) | Empirical Antibiotic Treatment (n = 141) | ||||
|---|---|---|---|---|---|---|
| De-escalation (n = 47) | Escalation (n = 5) | Continuation (n = 89) | p-Value | |||
| Age | ||||||
| Mean (SD) | 63.3 (12.6) | 63.2 (14.6) | 63.5 (9.51) | 62.6 (7.47) | 63.3 (13.7) | 0.548 |
| Median [IQR] | 66.0 [57.0–72.0] | 68.0 [58.0–74.0] | 63.0 [56.5–69.5] | 65.0 [58.0–68.0] | 67.0 [57.0–74.0] | |
| Gender | ||||||
| F | 46 (27.1%) | 14 (48.3%) | 8 (17.0%) | 1 (20.0%) | 23 (25.8%) | 0.5 |
| H | 124 (72.9%) | 15 (51.7%) | 39 (83.0%) | 4 (80.0%) | 66 (74.2%) | |
| BMI | ||||||
| Mean (SD) | 30.0 (5.84) | 29.9 (6.67) | 30.4 (6.24) | 27.9 (4.76) | 30.0 (5.46) | 0.53 |
| Median [IQR] | 29.0 [26.0–33.4] | 29.0 [26.4–31.5] | 28.9 [26.4–35.0] | 26.8 [26.0–27.0] | 29.3 [26.0–33.1] | |
| Missing | 11 (6.5%) | 2 (6.9%) | 5 (10.6%) | 0 (0%) | 4 (4.5%) | |
| Obesity | ||||||
| 0 | 91 (53.5%) | 17 (58.6%) | 24 (51.1%) | 4 (80.0%) | 46 (51.7%) | 0.473 |
| 1 | 71 (41.8%) | 11 (37.9%) | 18 (38.3%) | 1 (20.0%) | 41 (46.1%) | |
| Missing | 8 (4.7%) | 1 (3.4%) | 5 (10.6%) | 0 (0%) | 2 (2.2%) | |
| Immunosuppression * | ||||||
| 0 | 149 (87.6%) | 26 (89.7%) | 40 (85.1%) | 5 (100%) | 78 (87.6%) | 0.626 |
| 1 | 21 (12.4%) | 3 (10.3%) | 7 (14.9%) | 0 (0%) | 11 (12.4%) | |
| Invasive procedures as outpatients | ||||||
| 0 | 169 (99.4%) | 29 (100%) | 47 (100%) | 5 (100%) | 88 (98.9%) | 0.745 |
| 1 | 1 (0.6%) | 0 (0%) | 0 (0%) | 0 (0%) | 1 (1.1%) | |
| Previous hospitalization < 90 days | ||||||
| 0 | 151 (88.8%) | 26 (89.7%) | 42 (89.4%) | 5 (100%) | 78 (87.6%) | 0.686 |
| 1 | 19 (11.2%) | 3 (10.3%) | 5 (10.6%) | 0 (0%) | 11 (12.4%) | |
| Prior antibiotic course < 90 days | ||||||
| 0 | 124 (72.9%) | 22 (75.9%) | 33 (70.2%) | 4 (80.0%) | 65 (73.0%) | 0.872 |
| 1 | 46 (27.1%) | 7 (24.1%) | 14 (29.8%) | 1 (20.0%) | 24 (27.0%) | |
| Myocardial infarction | ||||||
| 0 | 143 (84.1%) | 23 (79.3%) | 43 (91.5%) | 5 (100%) | 72 (80.9%) | 0.163 |
| 1 | 27 (15.9%) | 6 (20.7%) | 4 (8.5%) | 0 (0%) | 17 (19.1%) | |
| Congestive heart failure | ||||||
| 0 | 165 (97.1%) | 28 (96.6%) | 47 (100%) | 5 (100%) | 85 (95.5%) | 0.3 |
| 1 | 5 (2.9%) | 1 (3.4%) | 0 (0%) | 0 (0%) | 4 (4.5%) | |
| Vascular peripheral disease | ||||||
| 0 | 161 (94.7%) | 27 (93.1%) | 45 (95.7%) | 5 (100%) | 84 (94.4%) | 0.822 |
| 1 | 9 (5.3%) | 2 (6.9%) | 2 (4.3%) | 0 (0%) | 5 (5.6%) | |
| Stroke | ||||||
| 0 | 162 (95.3%) | 29 (100%) | 47 (100%) | 5 (100%) | 81 (91.0%) | 0.0839 |
| 1 | 8 (4.7%) | 0 (0%) | 0 (0%) | 0 (0%) | 8 (9.0%) | |
| Dementia | ||||||
| 0 | 168 (98.8%) | 29 (100%) | 47 (100%) | 4 (80.0%) | 88 (98.9%) | 0.0014 |
| 1 | 2 (1.2%) | 0 (0%) | 0 (0%) | 1 (20.0%) | 1 (1.1%) | |
| Chronic respiratory failure | ||||||
| 0 | 148 (87.1%) | 26 (89.7%) | 41 (87.2%) | 5 (100%) | 76 (85.4%) | 0.639 |
| 1 | 22 (12.9%) | 3 (10.3%) | 6 (12.8%) | 0 (0%) | 13 (14.6%) | |
| Connective tissue disease | ||||||
| 0 | 168 (98.8%) | 29 (100%) | 46 (97.9%) | 5 (100%) | 88 (98.9%) | 0.862 |
| 1 | 2 (1.2%) | 0 (0%) | 1 (2.1%) | 0 (0%) | 1 (1.1%) | |
| Gastric ulcer | ||||||
| 0 | 167 (98.2%) | 28 (96.6%) | 47 (100%) | 5 (100%) | 87 (97.8%) | 0.553 |
| 1 | 3 (1.8%) | 1 (3.4%) | 0 (0%) | 0 (0%) | 2 (2.2%) | |
| Mild liver disease | ||||||
| 0 | 166 (97.6%) | 28 (96.6%) | 46 (97.9%) | 5 (100%) | 87 (97.8%) | 0.944 |
| 1 | 4 (2.4%) | 1 (3.4%) | 1 (2.1%) | 0 (0%) | 2 (2.2%) | |
| Moderate to severe liver disease | ||||||
| 0 | 168 (98.8%) | 29 (100%) | 47 (100%) | 5 (100%) | 87 (97.8%) | 0.553 |
| 1 | 2 (1.2%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (2.2%) | |
| Kidney disease | ||||||
| 0 | 160 (94.1%) | 26 (89.7%) | 45 (95.7%) | 5 (100%) | 84 (94.4%) | 0.822 |
| 1 | 10 (5.9%) | 3 (10.3%) | 2 (4.3%) | 0 (0%) | 5 (5.6%) | |
| Diabetes—without complications | ||||||
| 0 | 118 (69.4%) | 23 (79.3%) | 28 (59.6%) | 4 (80.0%) | 63 (70.8%) | 0.344 |
| 1 | 52 (30.6%) | 6 (20.7%) | 19 (40.4%) | 1 (20.0%) | 26 (29.2%) | |
| Diabetes—with complications | ||||||
| 0 | 164 (96.5%) | 28 (96.6%) | 46 (97.9%) | 5 (100%) | 85 (95.5%) | 0.707 |
| 1 | 6 (3.5%) | 1 (3.4%) | 1 (2.1%) | 0 (0%) | 4 (4.5%) | |
| Solid cancer without metastasis < 5 years | ||||||
| 0 | 148 (87.1%) | 24 (82.8%) | 42 (89.4%) | 5 (100%) | 77 (86.5%) | 0.623 |
| 1 | 22 (12.9%) | 5 (17.2%) | 5 (10.6%) | 0 (0%) | 12 (13.5%) | |
| Solid cancer with metastasis | ||||||
| 0 | 166 (97.6%) | 28 (96.6%) | 46 (97.9%) | 5 (100%) | 87 (97.8%) | 0.944 |
| 1 | 4 (2.4%) | 1 (3.4%) | 1 (2.1%) | 0 (0%) | 2 (2.2%) | |
| Leukemia | ||||||
| 0 | 167 (98.2%) | 29 (100%) | 46 (97.9%) | 5 (100%) | 87 (97.8%) | 0.944 |
| 1 | 3 (1.8%) | 0 (0%) | 1 (2.1%) | 0 (0%) | 2 (2.2%) | |
| Lymphoma | ||||||
| 0 | 167 (98.2%) | 28 (96.6%) | 46 (97.9%) | 5 (100%) | 88 (98.9%) | 0.862 |
| 1 | 3 (1.8%) | 1 (3.4%) | 1 (2.1%) | 0 (0%) | 1 (1.1%) | |
| Hypertension | ||||||
| 0 | 86 (50.6%) | 10 (34.5%) | 24 (51.1%) | 2 (40.0%) | 50 (56.2%) | 0.695 |
| 1 | 84 (49.4%) | 19 (65.5%) | 23 (48.9%) | 3 (60.0%) | 39 (43.8%) | |
| Tobacco consumption | ||||||
| 0 | 126 (74.1%) | 22 (75.9%) | 36 (76.6%) | 4 (80.0%) | 64 (71.9%) | 0.797 |
| 1 | 44 (25.9%) | 7 (24.1%) | 11 (23.4%) | 1 (20.0%) | 25 (28.1%) | |
| COVID-19 wave | ||||||
| wave1 | 30 (17.6%) | 6 (20.7%) | 8 (17.0%) | 0 (0%) | 16 (18.0%) | 0.244 |
| wave2 | 51 (30.0%) | 8 (27.6%) | 17 (36.2%) | 2 (40.0%) | 24 (27.0%) | |
| wave3 | 72 (42.4%) | 13 (44.8%) | 14 (29.8%) | 2 (40.0%) | 43 (48.3%) | |
| wave4 | 17 (10.0%) | 2 (6.9%) | 8 (17.0%) | 1 (20.0%) | 6 (6.7%) | |
| Charlson Score | ||||||
| Mean (SD) | 4.59 (2.28) | 4.79 (2.50) | 4.30 (1.99) | 3.20 (0.837) | 4.76 (2.38) | 0.137 |
| Median [IQR] | 4.00 [3.00–6.00] | 5.00 [3.00–6.00] | 4.00 [3.00–5.00] | 3.00 [3.00–4.00] | 4.00 [3.00–6.00] | |
| SAPS II at ICU admission | ||||||
| Mean (SD) | 41.1 (15.7) | 41.1 (15.6) | 43.9 (14.2) | 29.4 (5.03) | 40.3 (16.6) | 0.0274 |
| Median [IQR] | 38.0 [29.0–49.0] | 39.0 [29.0–50.0] | 41.0 [33.0–50.0] | 29.0 [29.0–31.0] | 36.0 [29.0–46.0] | |
| SOFA at ICU admission | ||||||
| Mean (SD) | 5.09 (2.95) | 4.45 (2.57) | 5.68 (3.07) | 4.00 (1.22) | 5.06 (3.04) | 0.366 |
| Median [IQR] | 4.00 [3.00–8.00] | 3.00 [3.00–6.00] | 4.00 [3.00–8.00] | 4.00 [4.00–5.00] | 4.00 [2.00–8.00] | |
| Prophylactic antibiotic therapy | ||||||
| 0 | 102 (60.0%) | 16 (55.2%) | 25 (53.2%) | 3 (60.0%) | 58 (65.2%) | 0.395 |
| 1 | 68 (40.0%) | 13 (44.8%) | 22 (46.8%) | 2 (40.0%) | 31 (34.8%) | |
| Dexamethasone | ||||||
| 0 | 32 (18.8%) | 6 (20.7%) | 9 (19.1%) | 0 (0%) | 17 (19.1%) | 0.557 |
| 1 | 138 (81.2%) | 23 (79.3%) | 38 (80.9%) | 5 (100%) | 72 (80.9%) | |
| Vasopressors | ||||||
| 0 | 91 (53.5%) | 20 (69.0%) | 14 (29.8%) | 2 (40.0%) | 55 (61.8%) | 0.0016 |
| 1 | 79 (46.5%) | 9 (31.0%) | 33 (70.2%) | 3 (60.0%) | 34 (38.2%) | |
| Mechanical ventilation | ||||||
| 0 | 21 (12.4%) | 6 (20.7%) | 3 (6.4%) | 1 (20.0%) | 11 (12.4%) | 0.442 |
| 1 | 149 (87.6%) | 23 (79.3%) | 44 (93.6%) | 4 (80.0%) | 78 (87.6%) | |
| Meduri corticosteroids protocol ** | ||||||
| 0 | 146 (85.9%) | 27 (93.1%) | 40 (85.1%) | 5 (100%) | 74 (83.1%) | 0.592 |
| 1 | 24 (14.1%) | 2 (6.9%) | 7 (14.9%) | 0 (0%) | 15 (16.9%) | |
| Hydroxychloroquine | ||||||
| 0 | 147 (86.5%) | 21 (72.4%) | 43 (91.5%) | 5 (100%) | 78 (87.6%) | 0.578 |
| 1 | 23 (13.5%) | 8 (27.6%) | 4 (8.5%) | 0 (0%) | 11 (12.4%) | |
| Lopinavir/ritonavir | ||||||
| 0 | 156 (91.8%) | 26 (89.7%) | 43 (91.5%) | 5 (100%) | 82 (92.1%) | 0.796 |
| 1 | 14 (8.2%) | 3 (10.3%) | 4 (8.5%) | 0 (0%) | 7 (7.9%) | |
| Anti-IL1 (Kineret) | ||||||
| 0 | 165 (97.1%) | 29 (100%) | 44 (93.6%) | 5 (100%) | 87 (97.8%) | 0.421 |
| 1 | 5 (2.9%) | 0 (0%) | 3 (6.4%) | 0 (0%) | 2 (2.2%) | |
| Anti-JAK2 (Jakavi) | ||||||
| 0 | 162 (95.3%) | 28 (96.6%) | 43 (91.5%) | 5 (100%) | 86 (96.6%) | 0.369 |
| 1 | 8 (4.7%) | 1 (3.4%) | 4 (8.5%) | 0 (0%) | 3 (3.4%) | |
| Tocilizumab | ||||||
| 0 | 134 (78.8%) | 24 (82.8%) | 35 (74.5%) | 4 (80.0%) | 71 (79.8%) | 0.441 |
| 1 | 4 (2.4%) | 1 (3.4%) | 2 (4.3%) | 0 (0%) | 1 (1.1%) | |
| Missing | 32 (18.8%) | 4 (13.8%) | 10 (21.3%) | 1 (20.0%) | 17 (19.1%) | |
| In-hospital immunosuppressors | ||||||
| 0 | 132 (77.6%) | 26 (89.7%) | 33 (70.2%) | 4 (80.0%) | 69 (77.5%) | 0.368 |
| 1 | 35 (20.6%) | 3 (10.3%) | 13 (27.7%) | 0 (0%) | 19 (21.3%) | |
| Missing | 3 (1.8%) | 0 (0%) | 1 (2.1%) | 1 (20.0%) | 1 (1.1%) | |
| Acquired resistance—Overall *** | ||||||
| 0 | 161 (94.7%) | 29 (100%) | 42 (89.4%) | 4 (80.0%) | 86 (96.6%) | 0.115 |
| 1 | 9 (5.3%) | 0 (0%) | 5 (10.6%) | 1 (20.0%) | 3 (3.4%) | |
| Rectal swab MDR | ||||||
| 0 | 167 (98.2%) | 29 (100%) | 45 (95.7%) | 5 (100%) | 88 (98.9%) | 0.458 |
| 1 | 3 (1.8%) | 0 (0%) | 2 (4.3%) | 0 (0%) | 1 (1.1%) | |
| Acquired resistance in other samples | ||||||
| 0 | 162 (95.3%) | 29 (100%) | 43 (91.5%) | 4 (80.0%) | 86 (96.6%) | 0.173 |
| 1 | 8 (4.7%) | 0 (0%) | 4 (8.5%) | 1 (20.0%) | 3 (3.4%) | |
| Total duration of antibiotic treatment (days) | ||||||
| Mean (SD) | 8.86 (28.5) | 18.6 (67.4) | 10.2 (10.6) | 12.0 (5.34) | 4.82 (3.05) | 0.001 |
| Median [IQR] | 6.00 [3.00–7.00] | 7.00 [6.00–7.00] | 7.00 [6.00–9.00] | 10.0 [10.0–12.0] | 4.00 [3.00–7.00] | |
| Relapse of infection | ||||||
| 0 | 155 (91.2%) | 26 (89.7%) | 41 (87.2%) | 3 (60.0%) | 85 (95.5%) | 0.0095 |
| 1 | 14 (8.2%) | 2 (6.9%) | 6 (12.8%) | 2 (40.0%) | 4 (4.5%) | |
| Missing | 1 (0.6%) | 1 (3.4%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Recurrence of infection | ||||||
| 0 | 143 (84.1%) | 26 (89.7%) | 34 (72.3%) | 2 (40.0%) | 81 (91.0%) | 0.001 |
| 1 | 26 (15.3%) | 2 (6.9%) | 13 (27.7%) | 3 (60.0%) | 8 (9.0%) | |
| Missing | 1 (0.6%) | 1 (3.4%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Mechanical ventilation (days) | ||||||
| Mean (SD) | 21.9 (16.5) | 15.7 (9.77) | 24.4 (15.8) | 45.8 (24.7) | 21.4 (17.1) | 0.0547 |
| Median [IQR] | 17.0 [11.0–30.0] | 13.0 [8.00–19.0] | 20.0 [12.0–36.0] | 47.5 [37.3–56.0] | 16.0 [11.0–27.0] | |
| Missing | 13 (7.6%) | 2 (6.9%) | 2 (4.3%) | 1 (20.0%) | 8 (9.0%) | |
| ICU length of stay (d) | ||||||
| Mean (SD) | 27.7 (19.7) | 18.2 (10.1) | 33.3 (21.9) | 43.4 (30.3) | 26.9 (18.9) | 0.183 |
| Median [IQR] | 21.0 [15.0–35.5] | 15.0 [12.0–19.0] | 25.0 [18.5–46.5] | 52.0 [15.0–68.0] | 21.0 [15.0–31.0] | |
| Hospital length of stay (d) | ||||||
| Mean (SD) | 35.1 (21.3) | 24.3 (12.8) | 43.3 (24.7) | 49.6 (29.3) | 33.4 (19.3) | 0.0562 |
| Median [IQR] | 29.5 [20.0–46.0] | 20.0 [17.0–28.0] | 37.0 [24.5–54.5] | 60.0 [23.0–75.0] | 30.0 [20.0–45.0] | |
| Sepsis to ICU discharge (d) | ||||||
| Mean (SD) | 28.1 (20.3) | 18.6 (10.1) | 34.1 (23.1) | 43.4 (30.9) | 27.1 (19.4) | 0.159 |
| Median [IQR] | 21.0 [15.0–35.5] | 17.0 [12.0–20.0] | 25.0 [18.5–46.5] | 52.0 [15.0–67.0] | 21.0 [15.0–32.0] | |
| Sepsis to hospital discharge (d) | ||||||
| Mean (SD) | 34.7 (23.7) | 22.8 (12.9) | 43.5 (26.3) | 49.4 (29.6) | 33.1 (22.8) | 0.0393 |
| Median [IQR] | 29.0 [19.0–43.8] | 19.0 [14.0–26.0] | 37.0 [25.0–55.5] | 60.0 [23.0–75.0] | 29.0 [18.0–43.0] | |
| Withdrawal or withholding of care | ||||||
| 0 | 156 (91.8%) | 25 (86.2%) | 45 (95.7%) | 5 (100%) | 81 (91.0%) | 0.486 |
| 1 | 14 (8.2%) | 4 (13.8%) | 2 (4.3%) | 0 (0%) | 8 (9.0%) | |
| ICU mortality | ||||||
| 0 | 124 (72.9%) | 17 (58.6%) | 41 (87.2%) | 4 (80.0%) | 62 (69.7%) | 0.0729 |
| 1 | 46 (27.1%) | 12 (41.4%) | 6 (12.8%) | 1 (20.0%) | 27 (30.3%) | |
| In-hospital mortality | ||||||
| 0 | 123 (72.4%) | 17 (58.6%) | 40 (85.1%) | 4 (80.0%) | 62 (69.7%) | 0.136 |
| 1 | 47 (27.6%) | 12 (41.4%) | 7 (14.9%) | 1 (20.0%) | 27 (30.3%) | |
| Day 28 Mortality | ||||||
| 0 | 124 (72.9%) | 17 (58.6%) | 40 (85.1%) | 4 (80.0%) | 63 (70.8%) | 0.174 |
| 1 | 46 (27.1%) | 12 (41.4%) | 7 (14.9%) | 1 (20.0%) | 26 (29.2%) | |
| Day 90 Mortality | ||||||
| 0 | 123 (72.4%) | 17 (58.6%) | 40 (85.1%) | 4 (80.0%) | 62 (69.7%) | 0.136 |
| 1 | 47 (27.6%) | 12 (41.4%) | 7 (14.9%) | 1 (20.0%) | 27 (30.3%) | |
| n (%) | |
|---|---|
| Replacement of an empirical antimicrobial agent with a narrower-spectrum antibiotic | 29/47 (61.7) |
| Stopping one or more components of an empirical combination therapy | 18/47 (38.2) |
| Cases of microbiologically confirmed infection, causative pathogen is covered by concomitant antimicrobial therapy | 5/18 |
| Cases of non-microbiologically confirmed infection | 13/18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lakbar, I.; Delamarre, L.; Curtel, F.; Duclos, G.; Bezulier, K.; Gragueb-Chatti, I.; Martin-Loeches, I.; Forel, J.-M.; Leone, M. Antimicrobial Stewardship during COVID-19 Outbreak: A Retrospective Analysis of Antibiotic Prescriptions in the ICU across COVID-19 Waves. Antibiotics 2022, 11, 1517. https://doi.org/10.3390/antibiotics11111517
Lakbar I, Delamarre L, Curtel F, Duclos G, Bezulier K, Gragueb-Chatti I, Martin-Loeches I, Forel J-M, Leone M. Antimicrobial Stewardship during COVID-19 Outbreak: A Retrospective Analysis of Antibiotic Prescriptions in the ICU across COVID-19 Waves. Antibiotics. 2022; 11(11):1517. https://doi.org/10.3390/antibiotics11111517
Chicago/Turabian StyleLakbar, Ines, Louis Delamarre, Fanny Curtel, Gary Duclos, Karine Bezulier, Ines Gragueb-Chatti, Ignacio Martin-Loeches, Jean-Marie Forel, and Marc Leone. 2022. "Antimicrobial Stewardship during COVID-19 Outbreak: A Retrospective Analysis of Antibiotic Prescriptions in the ICU across COVID-19 Waves" Antibiotics 11, no. 11: 1517. https://doi.org/10.3390/antibiotics11111517