
The Inflammation Level and a Microbiological Analysis of the Anophthalmic Cavities of Unilateral Ocular Prosthesis Users: A Blind, Randomized Observational Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Demographics and Clinical Characteristics of IG
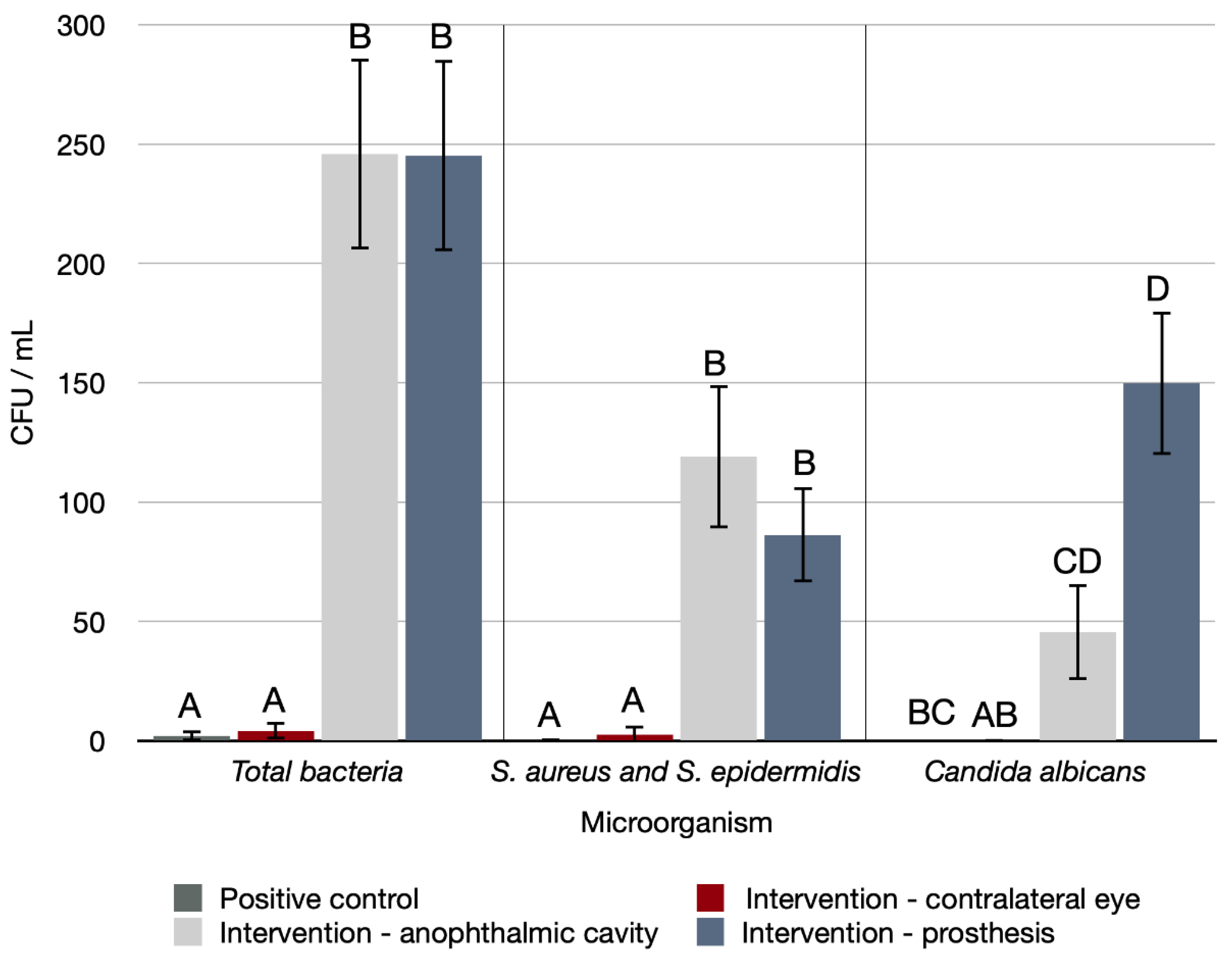
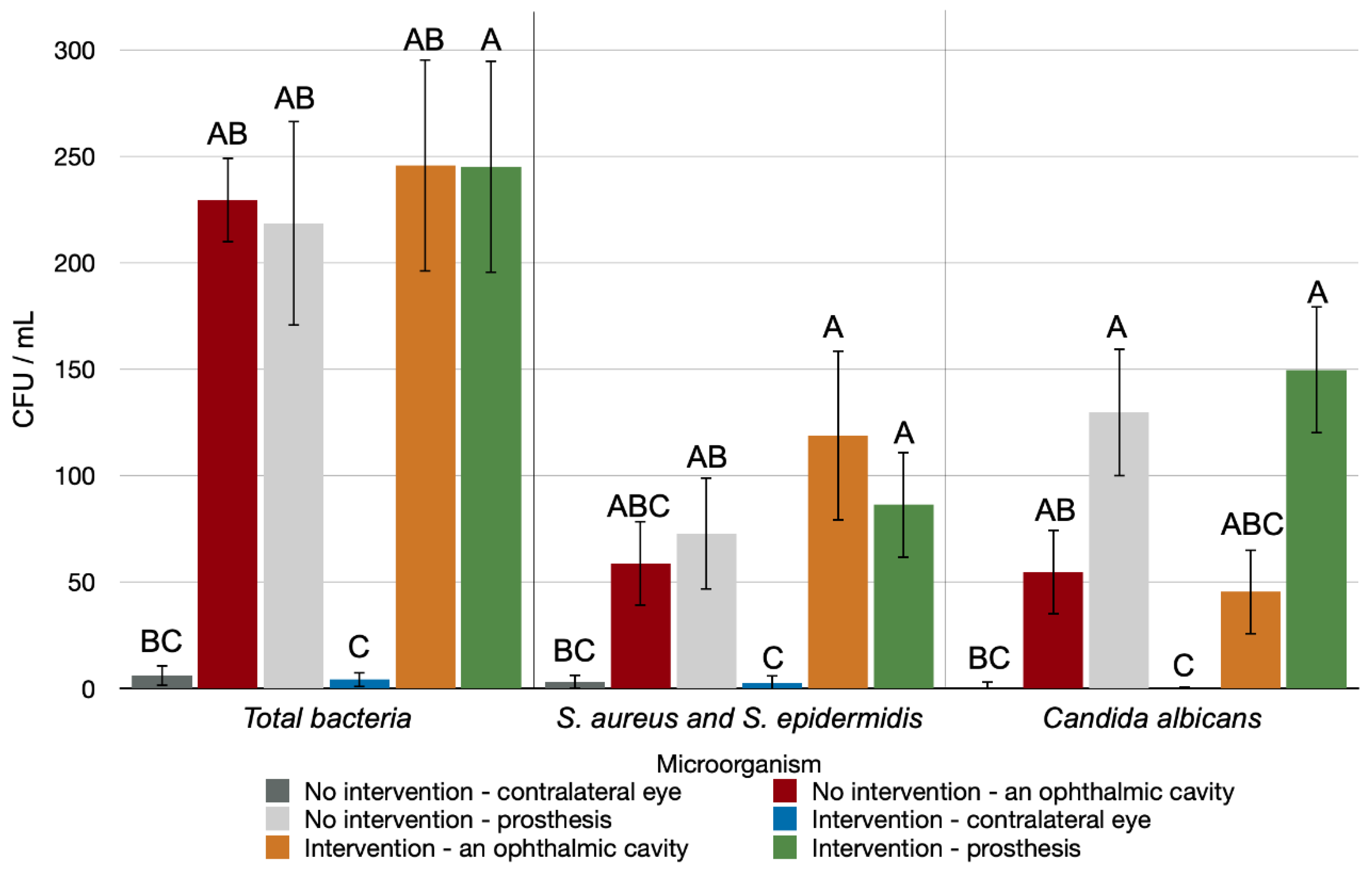
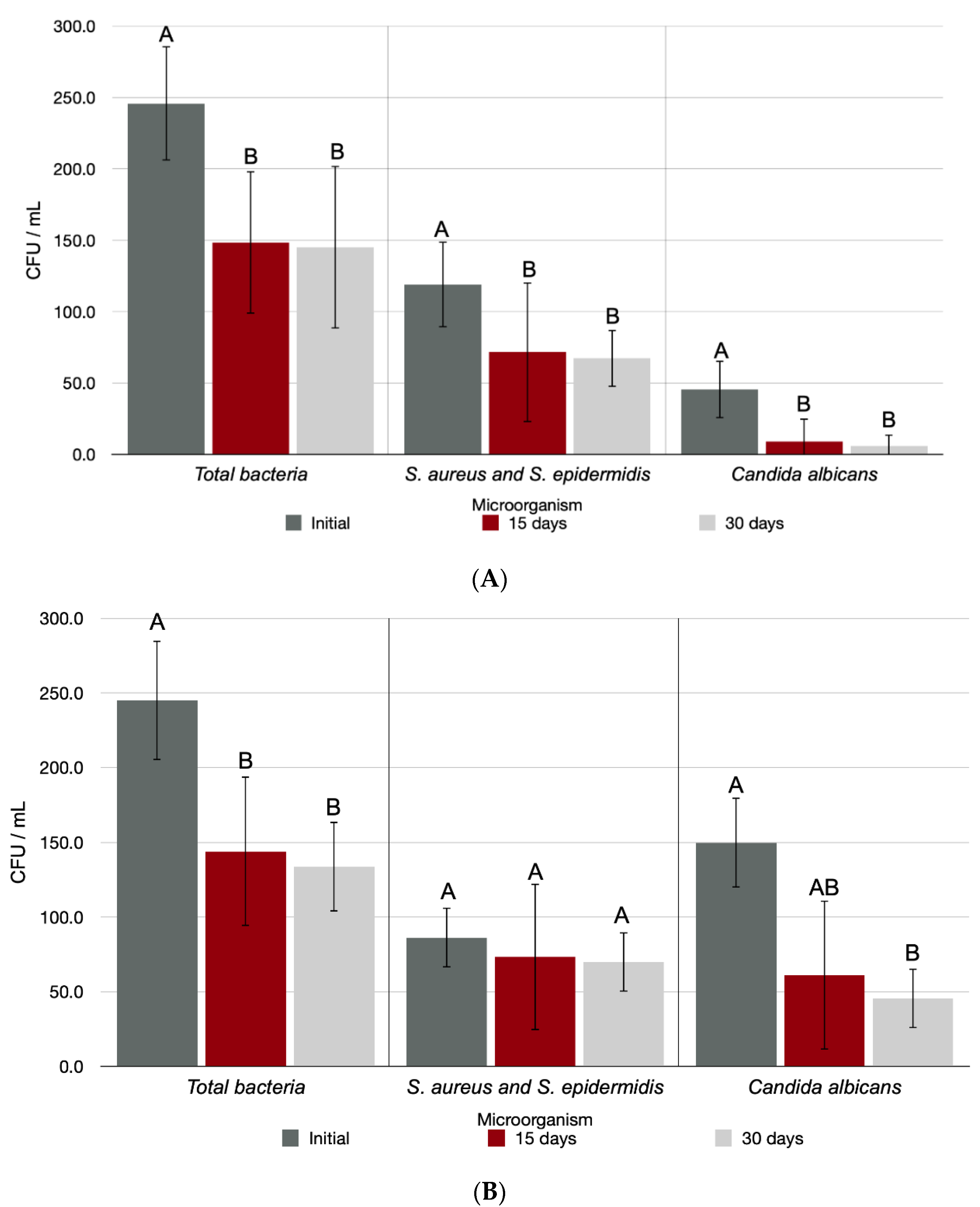
2.2. Microbiological Analysis
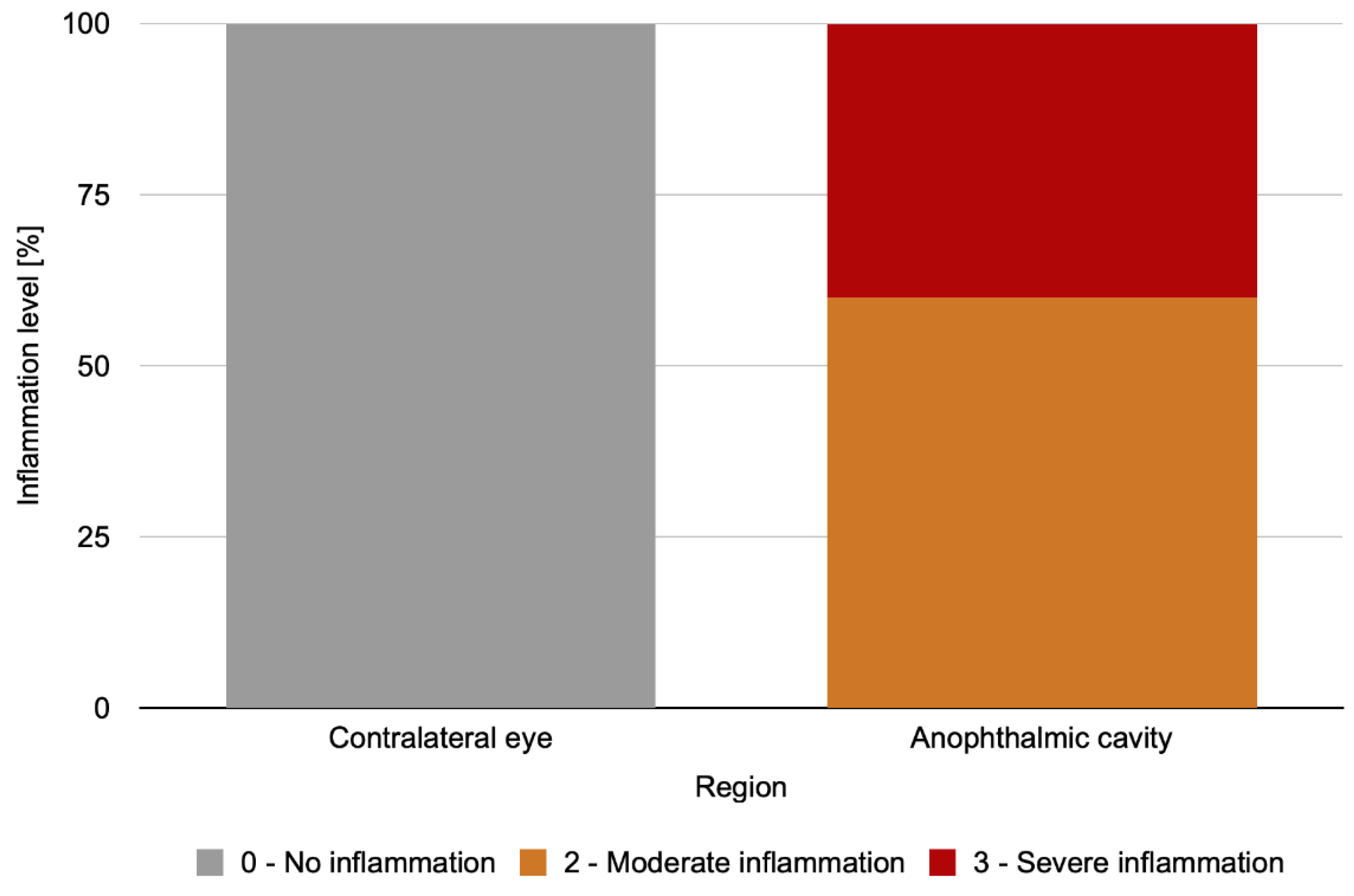
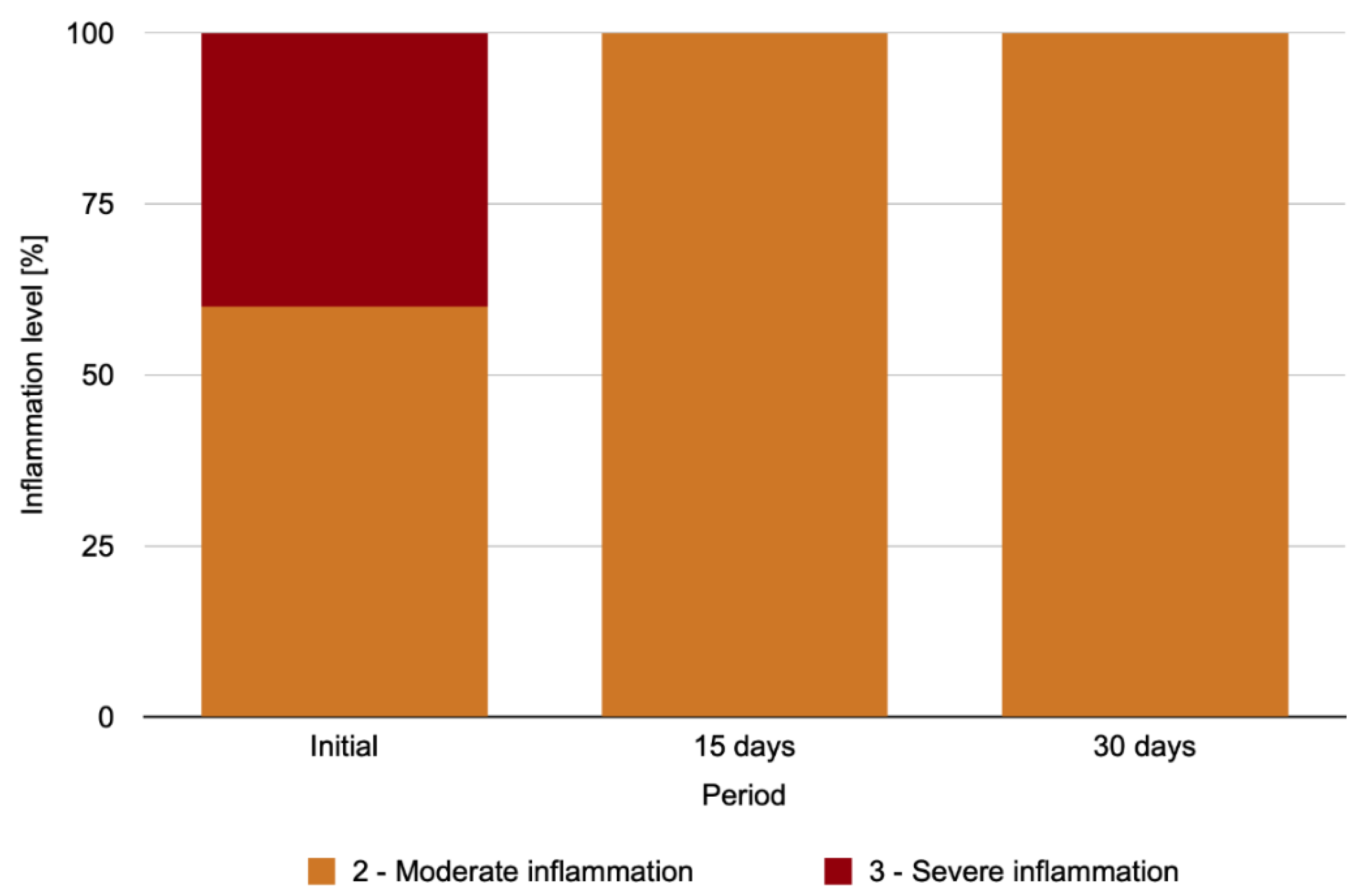
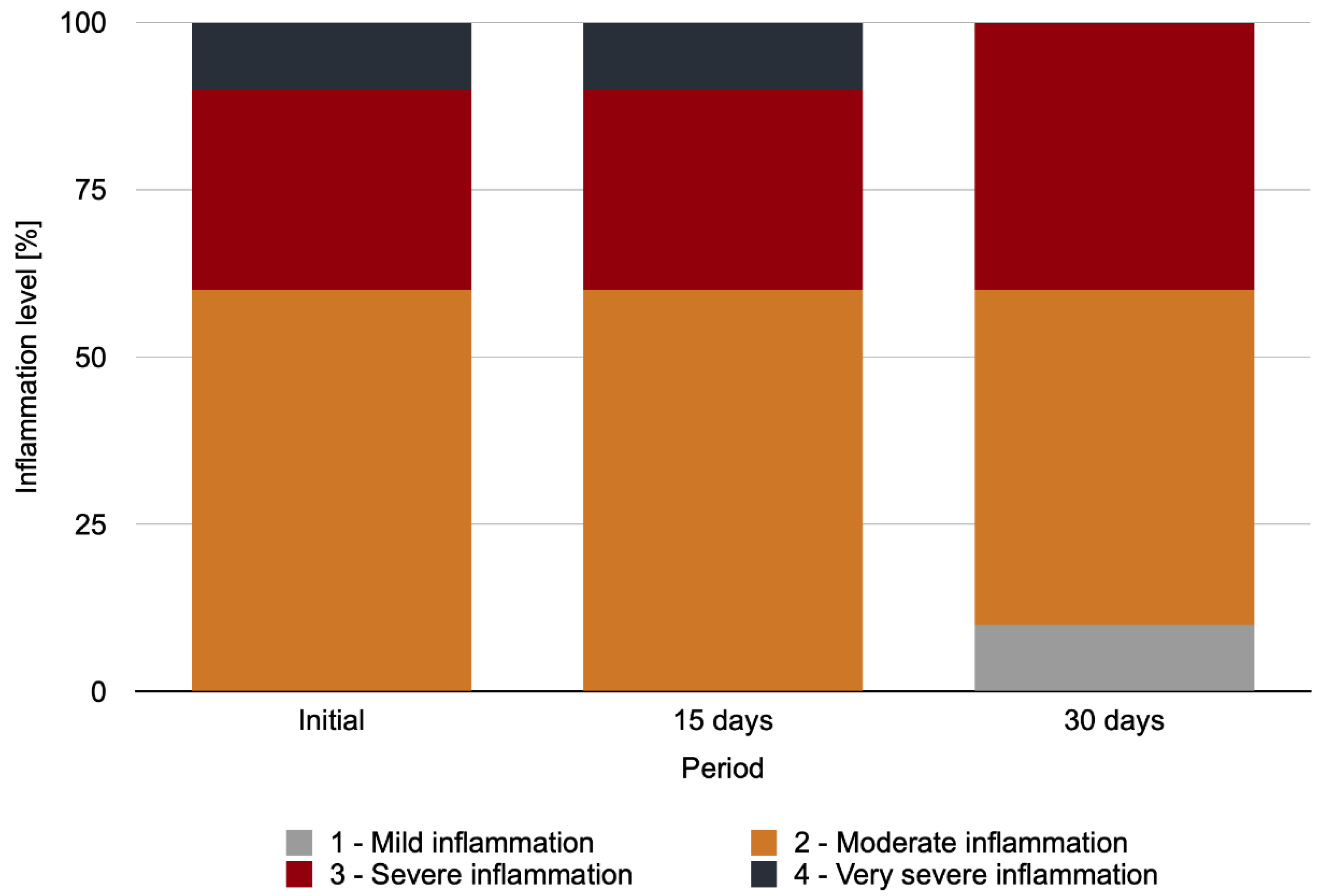
2.3. Level of Clinical Conjunctival Inflammation
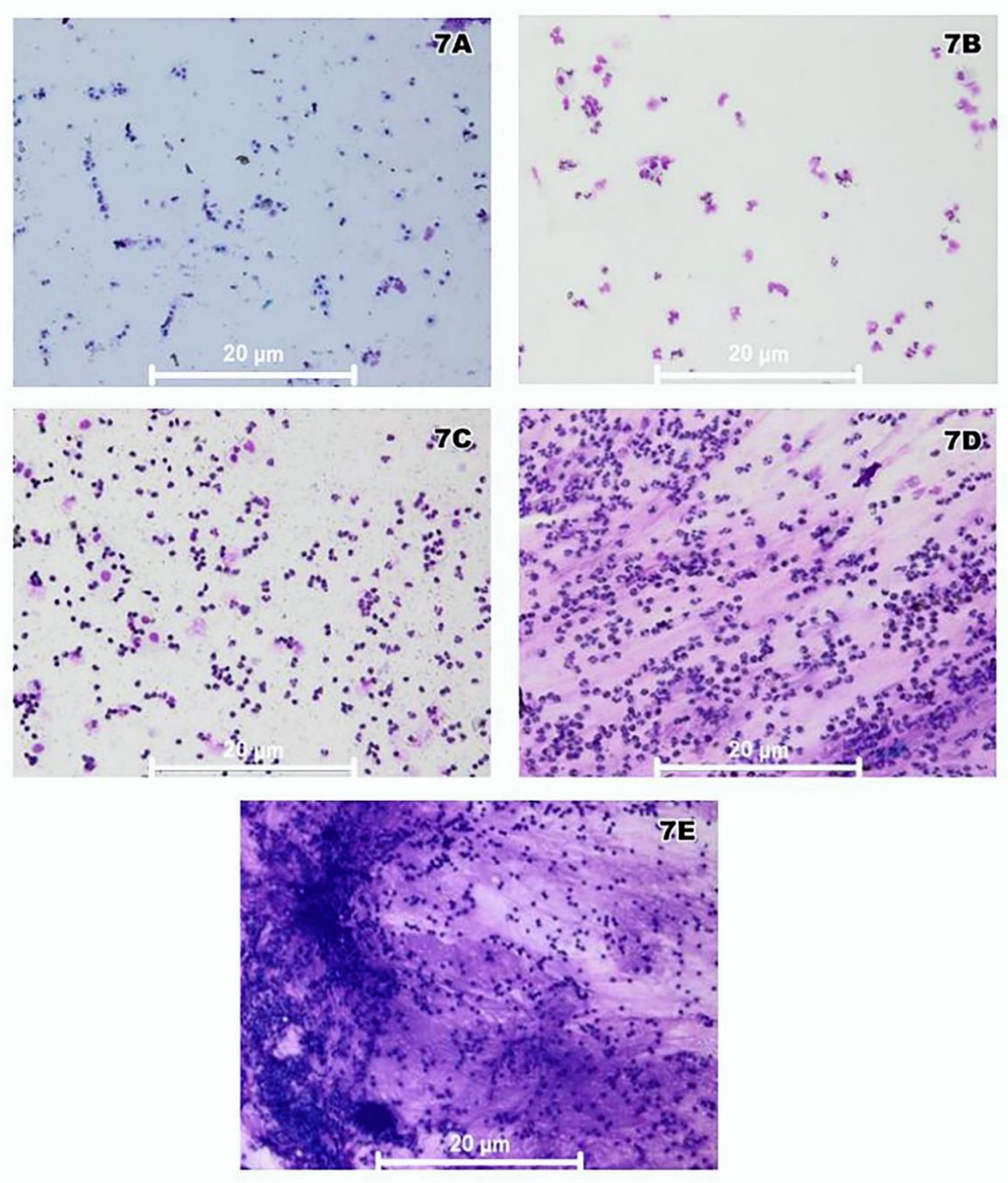
2.4. Conjunctival Smear Cytological Analysis
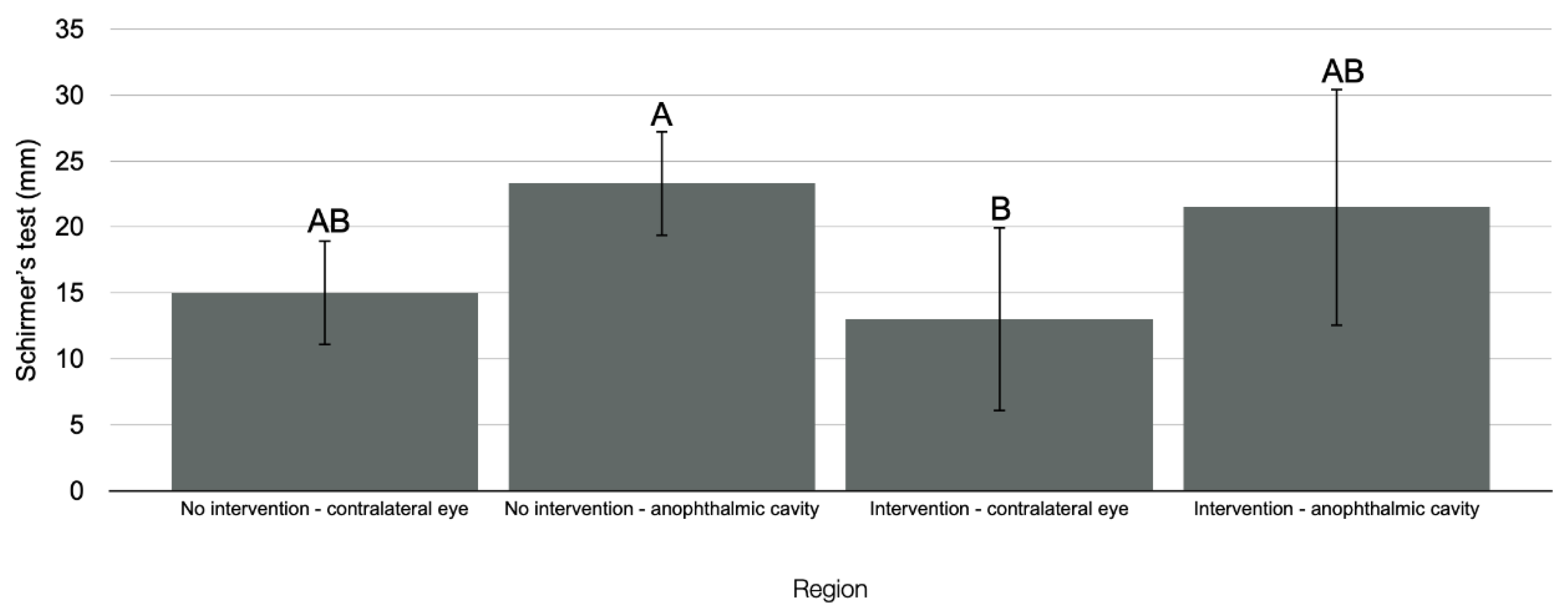
2.5. Tear Production Assessment (Schirmer’s Test)
2.6. Eyelid Sensitivity Assessment
3. Discussion
4. Patients and Methods
4.1. Study Design
4.2. Volunteer Selection
4.3. Demographic Data Collection and Psychosocial Profile
4.4. Microbiological Analysis of Anophthalmic Cavity and Ocular Prosthesis
4.5. Clinical Analysis of Degree of Inflammation
4.6. Analysis of Inflammatory Cells through Conjunctival Exfoliative Cytology
4.7. Tear Production Analysis (Schirmer’s Test)
4.8. Mechanical Sensitivity Assessment
4.9. Ocular-Prosthesis Repolishing
4.10. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goiato, M.C.; Santos, D.M.; Souza, J.F.; Moreno, A.; Pesqueira, A.A. Chromatic stability of acrylic resins of artificial eyes submitted to accelerated aging and polishing. J. Appl. Oral Sci. 2010, 18, 641–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Silva, E.V.F.; Goiato, M.C.; Bonatto, L.D.R.; De Medeiros, R.A.; Santos, D.M.D.; Rangel, E.C.; Oliveira, S.H.P. Toxicity analysis of ocular prosthesis acrylic resin with or without pigment incorporation in human conjunctival cell line. Toxicol. In Vitro 2016, 36, 180–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatamleh, M.M.; Abbariki, M.; Alqudah, N.; Cook, A.E. Survey of ocular prosthetics rehabilitation in the united kingdom, part 1: Anophthalmic patients’ aetiology, opinions, and attitudes. J. Craniofac. Surg. 2017, 28, 1293–1296. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, E.V.; Goiato, M.C.; Dos Santos, D.M.; Bonatto, L.D.; Brito, V.G.; De Oliveira, S.H. Effect of different methods of polymerizing ocular prosthesis acrylic resin on a human conjunctival cell line. J. Prosthet. Dent. 2016, 116, 818–823. [Google Scholar] [CrossRef] [Green Version]
- Goiato, M.C.; Bannwart, L.C.; Haddad, M.F.; Dos Santos, D.M.; Pesqueira, A.A.; Miyahara, G.I. Fabrication techniques for ocular prostheses: An overview. Orbit 2014, 33, 229–233. [Google Scholar] [CrossRef]
- Teughels, W.; Van Assche, N.; Sliepen, I.; Quirynen, M. Effect of material character-istics and/or surface topography on biofilm development. Clin. Oral Implant. Res. 2006, 17, 68–81. [Google Scholar] [CrossRef]
- Andreotti, A.M.; Sousa, C.A.; Goiato, M.C.; Silva, E.V.F.D.; Duque, C.; Moreno, A.; Santoso, D.M.D. In vitro evaluation of microbial adhesion on the different surface roughness of acrylic resin specific for ocular prosthesis. Eur. J. Dent. 2018, 12, 176–183. [Google Scholar] [CrossRef] [Green Version]
- Dayal, Y.; Rao, S.S.; Mahajan, V.M. Comparative study of bacterial and fungal floras of contracted sockets and fellow eyes. Ann. Ophthalmol. 1984, 16, 154–158. [Google Scholar]
- Yoda, I.; Koseki, H.; Tomita, M.; Shida, T.; Horiuchi, H.; Sakoda, H.; Osaki, M. Effect of sur-face roughness of biomaterials on Staphylococcus epidermidis adhesion. BMC Microbiol. 2014, 2, 234. [Google Scholar]
- Odorcic, S.; Haas, W.; Gilmore, M.S.; Dohlman, C.H. Fungal infections after boston type 1 keratoprosthesis implantation: Literature review and in vitro antifungal activity of hypochlorous acid. Cornea 2015, 34, 1599–1605. [Google Scholar] [CrossRef] [Green Version]
- Pine, K.; Sloan, B.; Stewart, J.; Jacobs, R.J. A survey of prosthetic eye wearers to investigate mucoid discharge. Clin. Ophthalmol. 2012, 6, 707–713. [Google Scholar]
- Donshik, P.C.; Ehlers, W.H. The contact lens patient and ocular allergies. Int. Ophthalmol. Clin. 1991, 31, 133–145. [Google Scholar] [CrossRef]
- Chang, W.J.; Tse, D.T.; Rosa, R.H.; Huang, A.; Johnson, T.E.; Schiffman, J. Conjunctival cytology features of giant papillary conjunctivitis associated with ocular prostheses. Ophthalmic Plast. Reconstr. Surg. 2005, 21, 39–45. [Google Scholar] [CrossRef]
- Kenny, S.E.; Tye, C.B.; Johnson, D.A.; Kheirkhah, A. Giant papillary conjunctivitis: A review. Ocul. Surf. 2020, 18, 396–402. [Google Scholar] [CrossRef] [PubMed]
- González-García, M.J.; González-Sáiz, A.; De la Fuente, B.; Morilla-Grasa, A.; Mayo-Iscar, A.; San-José, J.; Feijó, J.; Stern, M.E.; Calonge, M. Exposure to a controlled adverse environment impairs the ocular surface of subjects with minimally symptomatic dry eye. Investig. Ophthalmol. Vis. Sci. 2007, 48, 4026–4032. [Google Scholar] [CrossRef] [Green Version]
- Galor, A.; Kumar, N.; Feuer, W.; Lee, D.J. Environmental factors affect the risk of dry eye syndrome in a United States veteran population. Ophthalmology 2014, 121, 972–973. [Google Scholar] [CrossRef] [PubMed]
- López-Miguel, A.; Tesón, M.; Martín-Montañez, V.; Enríquez-de-Salamanca, A.; Stern, M.E.; Calonge, M.; González-García, M.J. Dry eye exacerbation in patients exposed to desiccating stress under controlled environmental conditions. Am. J. Ophthalmol. 2014, 157, 788–798. [Google Scholar] [CrossRef]
- Glasson, M.J.; Stapleton, F.; Keay, L.; Willcox, M.D. The effect of short term contact lens wear on the tear film and ocular surface characteristics of tolerant and intolerant wearers. Contact Lens Anterior Eye 2006, 29, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Morgan, P.B.; Efron, N. In vivo dehydration of silicone hydrogel contact lenses. Eye Contact Lens 2003, 29, 173–176. [Google Scholar] [CrossRef]
- Maruyama, K.; Yokoi, N.; Takamata, A.; Kinoshita, S. Effect of environmental condi-tions on tear dynamics in soft contact lens wearers. Investig. Ophthalmol. Vis. Sci. 2004, 45, 2563–2568. [Google Scholar] [CrossRef]
- Modugno, A.; Mantelli, F.; Sposato, S.; Moretti, C.; Lambiase, A.; Bonini, S. Ocular pros-theses in the last century: A retrospective analysis of 8018 patients. Eye 2013, 27, 865–870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghislandi, G.M.; Lima, G.C. Comparative study between phenol red thread test and the Schirmer’s test in the diagnosis of dry eyes syndrome. Rev. Bras. Oftalmol. 2016, 75, 438–442. [Google Scholar] [CrossRef] [Green Version]
- Guiotti, A.M.; Da Silva, E.V.F.; Catanoze, I.A.; De Carvalho, K.H.T.; Malavazi, E.M.; Goiato, M.C.; Dos Santos, D.M.; De Almeida, M.T.G. Microbiological analysis of conjunctival secretion in anophthalmic cavity, contralateral eye and ocular prosthesis of patients with maxillofacial abnormalities. Lett. Appl. Microbiol. 2018, 66, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Paranhos, R.M.; Batalhao, C.H.; Semprini, M.; Regalo, S.C.; Ito, I.Y.; De Mattos, M.G. Evaluation of ocular prosthesis biofilm and anophthalmic cavity contamination after use of three cleansing solutions. J. Appl. Oral Sci. 2007, 15, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arciola, C.R.; Campoccia, D.; Speziale, P.; Montanaro, L.; Costerton, J.W. Biofilm for-mation in Staphylococcus implant infections: A review of molecular mechanisms and implications for biofilm-resistant materials. Biomaterials 2012, 33, 5967–5982. [Google Scholar] [CrossRef]
- Bonaque-Gonzalez, S.; Amigo, A.; Rodrıguez-Luna, C. Recommendations for post-adaption care of an ocular prosthesis: A review. Contact Lens Anterior Eye 2015, 38, 397–401. [Google Scholar] [CrossRef]
- Sousa, C.; Teixeira, P.; Oliveira, R. Influence of surface properties on the adhesion of Staphylococcus epidermidis to acrylic and silicone. Int. J. Biomater. 2009, 2009, 718017. [Google Scholar] [CrossRef] [Green Version]
- Fouda, S.M.; Gad, M.M.; Ellakany, P.; Al-Thobity, A.M.; Al-Harbi, F.A.; Virtanen, J.I.; Raustia, A. The effect of nanodiamonds on candida albicans adhesion and surface characteristics of PMMA denture base material—An in vitro study. J. Appl. Oral Sci. 2019, 27, e20180779. [Google Scholar] [CrossRef] [Green Version]
- Moreno, A.; Goiato, M.C.; Dos Santos, D.M.; Haddad, M.F.; Pesqueira, A.A.; Bannwart, L.C. Effect of different disinfectants on the microhardness and roughness of acrylic resins for ocular prosthesis. Gerodontology 2013, 30, 32–39. [Google Scholar] [CrossRef]
- Sarac, O.; Erdener, U.; Irkec, M.; Us, D.; Gungen, Y. Tear eotaxin levels in giant papillary conjunctivitis associated with ocular prosthesis. Ocul. Immunol. Inflamm. 2003, 11, 223–230. [Google Scholar] [CrossRef]
- Da Silva, E.V.F.; Dos Santos, D.M.; Da Rocha Bonatto, L.; Balera Brito, V.G.; De Oliveira, S.H.P.; Goiato, M.C. Influence of preparation and exposure periods of eluates from oc-ular prosthesis acrylic resin in human conjunctival cell line. Iran. Biomed. J. 2019, 23, 78–86. [Google Scholar] [PubMed]
- Luo, Z.D.; Chaplan, S.R.; Higuera, E.S.; Sorkin, L.S.; Stauderman, K.A.; Williams, M.E.; Yaksh, T.L. Upregulation of dorsal root ganglion (alpha)2(delta) calcium channel subunit and its correlation with allodynia in spinal nerve-injured rats. J. Neurosci. 2001, 21, 1868–1875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schultz, C.L.; Kunert, K.S. Interleukin-6 levels in tears of contact lens wearers. J. Interf. Cytokine Res. 2000, 20, 309–310. [Google Scholar] [CrossRef] [PubMed]
- Poyraz, C.; Irkec, M.; Mocan, M.C. Elevated tear interleukin-6 and interleukin-8 levels associated with silicone hydrogel and conventional hydrogel contact lens wear. Eye Contact Lens 2012, 38, 146–149. [Google Scholar] [CrossRef]
- Kallinikos, P.; Morgan, P.; Efron, N. Assessment of stromal keratocytes and tear film inflammatory mediators during extended wear of contact lenses. Cornea 2006, 25, 1–10. [Google Scholar] [CrossRef]
- Staud, R.; Craggs, J.G.; Robinson, M.E.; Perlstein, W.M.; Price, D.D. Brain activity related to temporal summation of cfiber evoked pain. Pain 2007, 129, 130–142. [Google Scholar] [CrossRef] [Green Version]
- Vaccarino, A.L.; Chorney, D.A. Descending modulation of central neural plasticity in the formalin pain test. Brain Res. 1994, 666, 104–108. [Google Scholar] [CrossRef]
- Urban, M.O.; Jiang, M.C.; Gebhart, G.F. Participation of central descending noci-cep-tive facilitatory systems in secondary hyperalgesia produced by mustard oil. Brain Res. 1996, 737, 83–91. [Google Scholar] [CrossRef]
- Yağmur, M.; Ersöz, C.; Ersöz, T.R.; Varinli, S. Brush technique in ocular surface cytology. Diagn. Cytopathol. 1997, 17, 88–89. [Google Scholar] [CrossRef]
- Goiato, M.C.; Dos Santos, D.M.; Bannwart, L.C.; Moreno, A.; Pesqueira, A.A.; Haddad, M.F.; Dos Santos, E.G. Psychosocial impact on anophthalmic patients wearing ocular prosthesis. Int. J. Oral Maxillofac. Surg. 2013, 42, 113–119. [Google Scholar] [CrossRef]
- Santos, J.G.; Brito, J.O.; De Andrade, D.C.; Kaziyama, V.M.; Ferreira, K.A.; Souza, I.; Teixeira, M.J.; Bouhassira, D.; Baptista, A.F. Translation to portuguese and validation of the Douleur Neuropathique 4 questionnaire. J. Pain. 2010, 11, 484–490. [Google Scholar] [CrossRef]
- Nicodemo, D.; Ferreira, L.M. Questionnaire of the psychosocial profile of the patient with anophthalmia with indication of ocular prosthesis. Arq. Bras. Oftalmol. 2006, 69, 463–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, M.L. The eye amputated–consequences of eye amputation with em-phasis on clinical aspects, phantom eye syndrome and quality of life. Acta Ophthalmol. 2010, 88, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Nagay, B.E.; Dini, C.; Cordeiro, J.M.; Ricomini-Filho, A.P.; de Avila, E.D.; Rangel, E.C.; da Cruz, N.C.; Barão, V.A.R. Visible-light-induced photocatalytic and antibacterial activity of TiO2 codoped with nitrogen and bismuth: New perspectives to control implant-biofilm-related diseases. ACS Appl. Mater. Interfaces. 2019, 11, 18186–18202. [Google Scholar] [CrossRef]
- Pine, K.R.; Sloan, B.; Jacobs, R.J. The development of measurement tools for prosthetic eye research. Clin. Exp. Optom. 2013, 96, 32–38. [Google Scholar] [CrossRef] [PubMed]
- An, S.; Raju, I.; Surenkhuu, B.; Kwon, J.E.; Gulati, S.; Karaman, M.; Pradeep, A.; Sinha, S.; Mun, C.; Jain, S. Neutrophil extracellular traps (NETs) contribute to pathological changes of ocular graft-vs.-host disease (oGVHD) dry eye: Implications for novel biomarkers and therapeutic strategies. Ocul. Surf. 2019, 17, 589–614. [Google Scholar] [CrossRef]
- Aragona, P.; Romeo, G.F.; Puzzolo, D.; Micali, A.; Ferreri, G. Impression cytology of the conjunctival epithelium in patients with vernal conjunctivitis. Eye 1996, 10, 82–85. [Google Scholar] [CrossRef]
- Cvenkel, B.; Globocnik, M. Conjunctival scrapings and impression cytology in chronic conjunctivitis. Correlation with microbiology. Eur. J. Ophthalmol. 1997, 7, 19–23. [Google Scholar] [CrossRef]
- Fenga, C.; Aragona, P.; Cacciola, A.; Ferreri, F.; Spatari, G.; Stilo, A.; Spinella, R.; Germanò, D. Ocular dis-comfort and conjunctival alterations in operating room workers. A single-institution pilot study. Int. Arch. Occup. 2001, 74, 123–128. [Google Scholar] [CrossRef]
- Potvin, R.; Makari, S.; Rapuano, C.J. Tear film osmolarity and dry eye disease: A review of the literature. Clin. Ophthalmol. 2015, 9, 2039–2047. [Google Scholar] [CrossRef] [Green Version]
- Stevens, S. Schirmer’s test. Community Eye Health J. 2011, 24, 45. [Google Scholar]
- Fakih, D.; Zhao, Z.; Nicolle, P.; Reboussin, E.; Joubert, F.; Luzu, J.; Labbé, A.; Rostène, W.; Baudouin, C.; Mélik Parsadaniantz, S.; et al. Chronic dry eye induced corneal hypersensitivity, neuroinflammatory responses, and synaptic plasticity in the mouse trigeminal brainstem. J Neuroinflamm. 2019, 16, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, Y.M.; De Araújo Júnior, E.N.S.; Fiedler, L.S.; De Souza, P.R.J.; Silva, L.L.C.P.; Ferreira, D.M.A.O.; Conti, P.C.R.; Bonjardim, L.R. Reproducibility of quantitative sensory testing applied to musculoskeletal orofacial region: Site and sex differences. Eur. J. Pain 2019, 23, 81–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porporatti, A.L.; Costa, Y.M.; Stuginski-Barbosa, J.; Bonjardim, L.R.; Conti, P.C. Effect of topical anaesthesia in patients with persistent dentoalveolar pain disorders: A quan-titative sensory testing evaluation. Arch. Oral Biol. 2015, 60, 973–981. [Google Scholar] [CrossRef]
- Keizer, D.; Van Wijhe, M.; Post, W.J.; Wierda, J.M. Quantifying allodynia in patients suffering from unilateral neuropathic pain using von frey monofilaments. Clin. J. Pain 2007, 23, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Komiyama, O.; Wang, K.; Svensson, P.; Arendt-Nielsen, L.; Kawara, M.; De Laat, A. Ethnic differences regarding sensory, pain, and reflex responses in the trigeminal region. Clin. Neurophysiol. 2009, 120, 384–389. [Google Scholar] [CrossRef]
- Barreto, J.D.O.; De Alencar-Silva, F.J.; Oliveira, V.C.; Silva-Lovato, C.H.; Silva, P.G.; Regis, R.R. The effect of a continuous mechanical polishing protocol on surface roughness, biofilm adhesion, and color stability of acrylic resin artificial teeth. J. Prosthodont. 2019, 28, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Melo, C.B.F.; Feitosa, M.D.; Maia, S.D.B.; Barreto, J.O.; Peixoto, R.F.; Regis, R.R. Effect of a continuous mechanical polishing protocol on the color stainability, microhardness, mass, and surface roughness of denture base acrylic resin. J. Prosthet. Dent. 2020, 21, 796–802. [Google Scholar] [CrossRef]
- Sethi, T.; Kheur, M.; Haylock, C.; Harianawala, H. Fabrication of a custom ocular prosthesis. Middle East Afr. J. Ophthalmol. 2014, 21, 271–274. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Please complete the questionnaire by marking one answer for each number of the four questions below: VOLUNTEER’S INTERVIEW |
| Question 1: Does your pain have one or more of the following characteristics? 1- Burning YES ( ) NO ( ) 2- Painful cold sensation YES ( ) NO ( ) 3- Electric shock YES ( ) NO ( ) |
| Question 2: Is one or more of the following symptoms present in the same area as your pain? 4- Tingling YES ( ) NO ( ) 5- Pins-and-needles feeling YES ( ) NO ( ) 6- Numbness YES ( ) NO ( ) 7- Itching YES ( ) NO ( ) |
| PATIENT EXAMINATION Question 3: Is the pain located in an area where physical examination may reveal one or more of the following characteristics? 8- Hypoesthesia on touch YES ( ) NO ( ) 9- Needle pricking hypoesthesia YES ( ) NO ( ) |
| Question 4: In the painful area, pain may be caused or increased by: 10- Brushing YES ( ) NO ( ) SCORE 0—For each negative item 1—For each positive item Neuropathic pain: Total score from 4/10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Penitente, P.A.; Da Silva, E.V.F.; Goiato, M.C.; Maniçoba, L.L.P.; Brito, V.G.B.; Túrcio, K.H.L.; Rodrigues, A.S.; Nagay, B.E.; Dos Santos, D.M. The Inflammation Level and a Microbiological Analysis of the Anophthalmic Cavities of Unilateral Ocular Prosthesis Users: A Blind, Randomized Observational Study. Antibiotics 2022, 11, 1486. https://doi.org/10.3390/antibiotics11111486
Penitente PA, Da Silva EVF, Goiato MC, Maniçoba LLP, Brito VGB, Túrcio KHL, Rodrigues AS, Nagay BE, Dos Santos DM. The Inflammation Level and a Microbiological Analysis of the Anophthalmic Cavities of Unilateral Ocular Prosthesis Users: A Blind, Randomized Observational Study. Antibiotics. 2022; 11(11):1486. https://doi.org/10.3390/antibiotics11111486
Chicago/Turabian StylePenitente, Paulo Augusto, Emily Vivianne Freitas Da Silva, Marcelo Coelho Goiato, Lorena Louise Pontes Maniçoba, Victor Gustavo Balera Brito, Karina Helga Leal Túrcio, Alana Semenzin Rodrigues, Bruna Egumi Nagay, and Daniela Micheline Dos Santos. 2022. "The Inflammation Level and a Microbiological Analysis of the Anophthalmic Cavities of Unilateral Ocular Prosthesis Users: A Blind, Randomized Observational Study" Antibiotics 11, no. 11: 1486. https://doi.org/10.3390/antibiotics11111486
APA StylePenitente, P. A., Da Silva, E. V. F., Goiato, M. C., Maniçoba, L. L. P., Brito, V. G. B., Túrcio, K. H. L., Rodrigues, A. S., Nagay, B. E., & Dos Santos, D. M. (2022). The Inflammation Level and a Microbiological Analysis of the Anophthalmic Cavities of Unilateral Ocular Prosthesis Users: A Blind, Randomized Observational Study. Antibiotics, 11(11), 1486. https://doi.org/10.3390/antibiotics11111486