
Does the Use of Local Antibiotics Affect Clinical Outcome of Patients with Fracture-Related Infection?

 , , , and
, , , and
Abstract
1. Introduction
1.1. Background
1.2. Rationale
1.3. Research Questions
2. Results
2.1. Patient Population
2.2. Type of Local Antibiotics
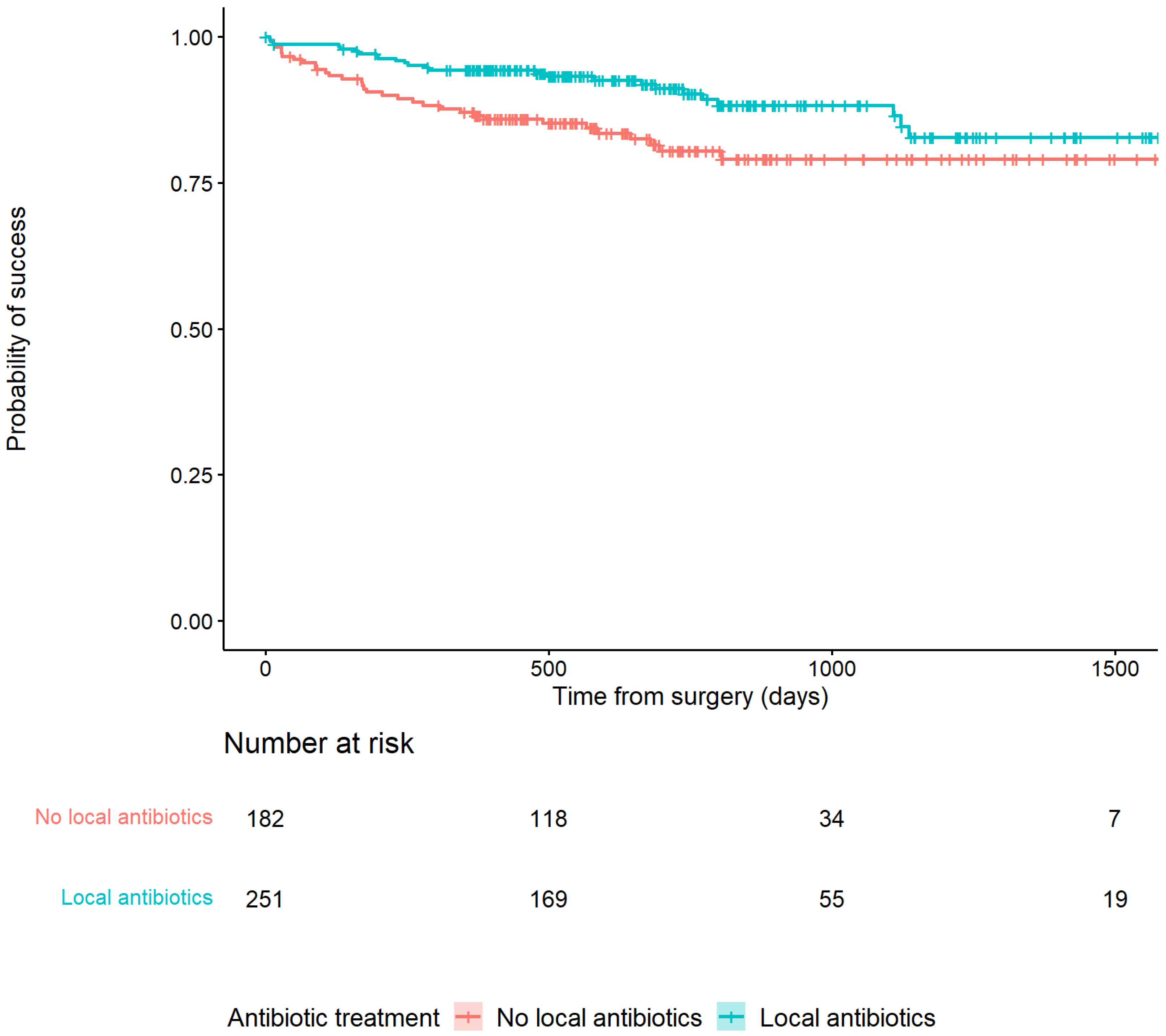
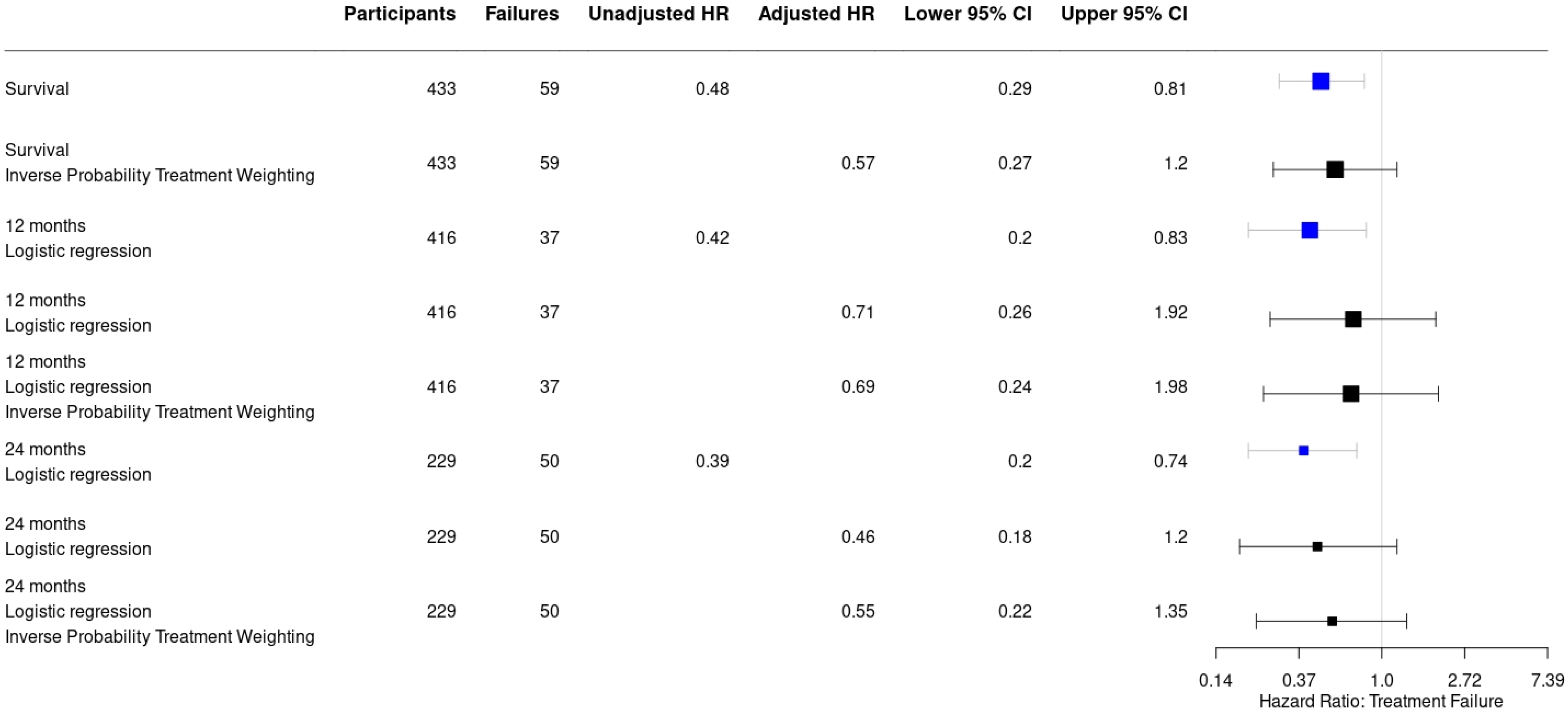
2.3. Application of Antibiotic-Loaded Carriers in Relation to Outcome
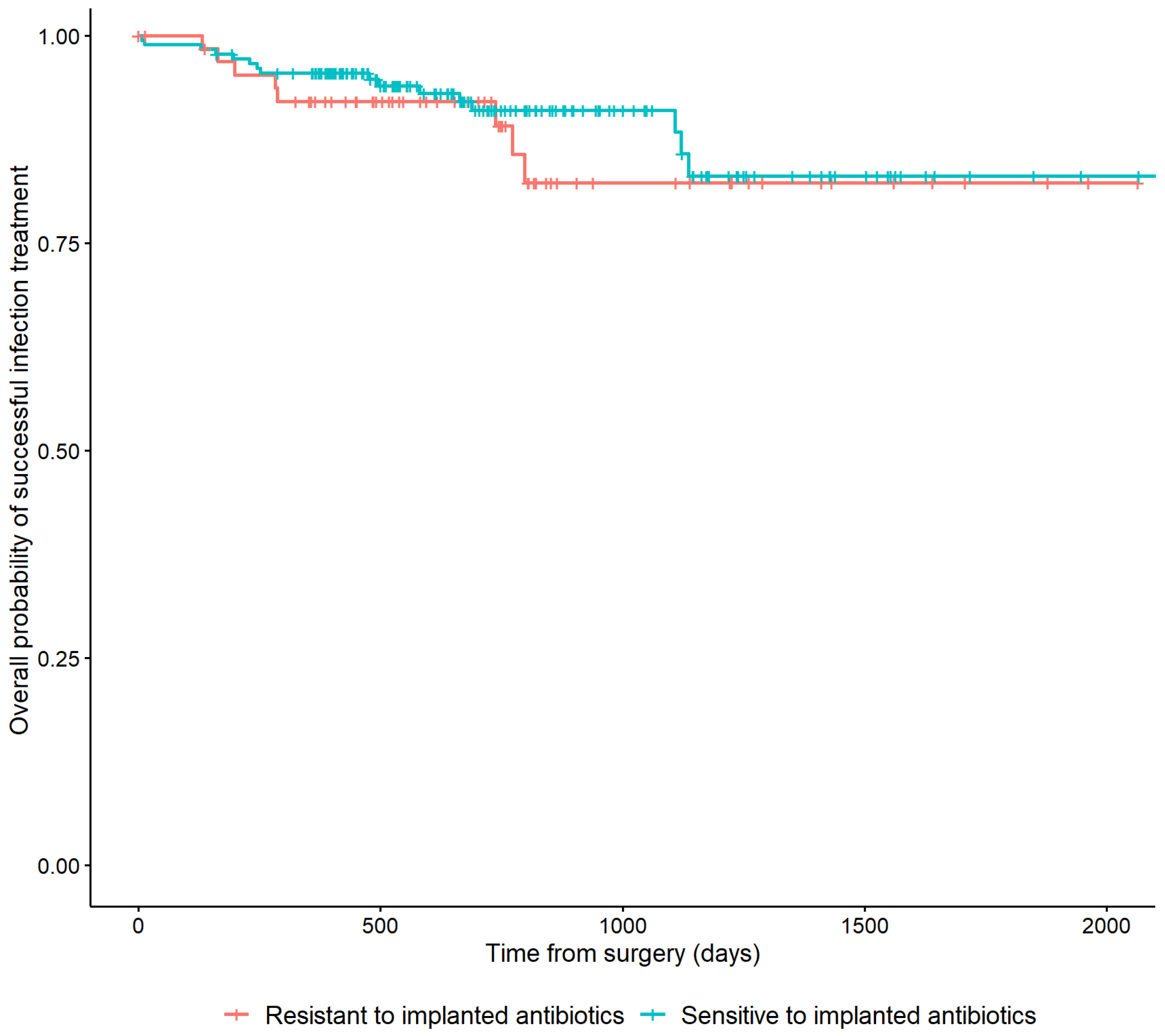
2.4. Bacterial Resistance to Local Antibiotics in Relation to Outcome
3. Discussion
3.1. Application of Local Antibiotics Related to Outcome
3.2. Susceptibility to Local Antibiotics Related to Outcome
3.3. Limitations
4. Materials and Methods
4.1. Study Design
4.2. Study Population
4.3. Surgical and Antibiotic Treatment
4.4. Clinical Outcome
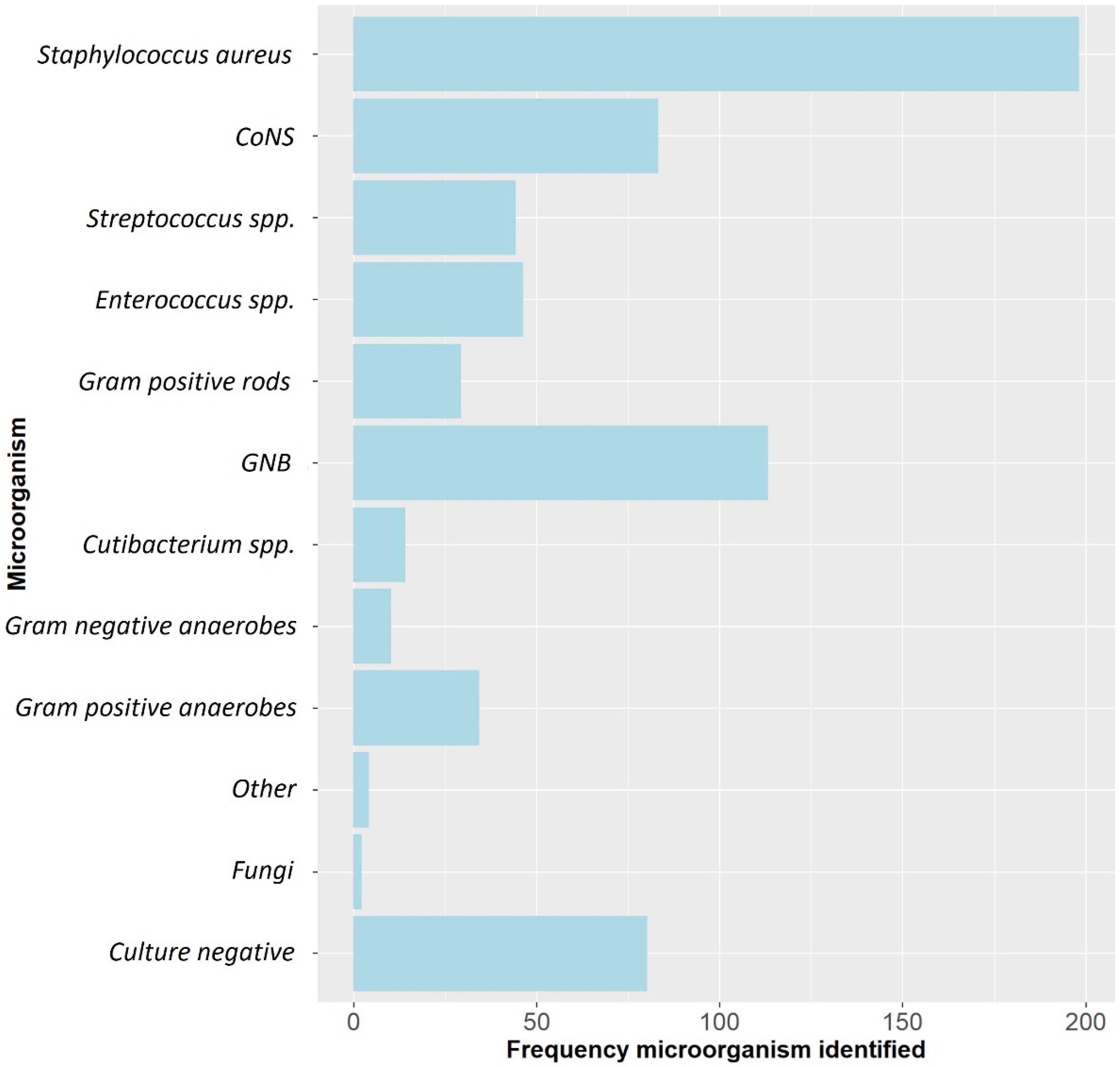
4.5. Causative Pathogens and Local Antibiotics
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iliaens, J.; Onsea, J.; Hoekstra, H.; Nijs, S.; Peetermans, W.E.; Metsemakers, W.J. Fracture-related infection in long bone fractures: A comprehensive analysis of the economic impact and influence on quality of life. Injury 2021, 52, 3344–3349. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Morgenstern, M.; Senneville, E.; Borens, O.; Govaert, G.A.; Onsea, J.; Depypere, M.; Richards, R.G.; Trampuz, A.; Verhofstad, M.H.; et al. General treatment principles for fracture-related infection: Recommendations from an international expert group. Arch. Orthop. Trauma Surg. 2020, 140, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Metsemakers, W.J.; Kuehl, R.; Moriarty, T.F.; Richards, R.G.; Verhofstad, M.H.; Borens, O.; Kates, S.; Morgenstern, M. Infection after fracture fixation: Current surgical and microbiological concepts. Injury 2018, 49, 511–522. [Google Scholar] [CrossRef]
- Baecker, H.; Frieler, S.; Schildhauer, T.A.; Gessmann, J.; Hanusrichter, Y. Fracture-related infections in traumatology: Current standards and new developments in diagnostics and treatment. Orthopade 2020, 49, 702–709. [Google Scholar] [CrossRef]
- Iliadis, A.D.; Shivji, F.; Debuka, E.; Trompeter, A.; Narayan, B.; Heidari, N. Current concepts in the prevention, diagnosis and treatment of fracture-related infection (FRI). Eur. J. Orthop. Surg. Traumatol. 2021, 31, 957–966. [Google Scholar] [CrossRef]
- Metsemakers, W.J.; Fragomen, A.T.; Moriarty, T.F.; Morgenstern, M.; Egol, K.A.; Zalavras, C.; Obremskey, W.T.; Raschke, M.; McNally, M.A. Evidence-Based Recommendations for Local Antimicrobial Strategies and Dead Space Management in Fracture-Related Infection. J. Orthop. Trauma 2020, 34, 18–29. [Google Scholar] [CrossRef]
- Wassif, R.K.; Elkayal, M.; Shamma, R.N.; Elkheshen, S.A. Recent advances in the local antibiotics delivery systems for management of osteomyelitis. Drug Deliv. 2021, 28, 2392–2414. [Google Scholar] [CrossRef] [PubMed]
- Cobb, L.H.; McCabe, E.M.; Priddy, L.B. Therapeutics and delivery vehicles for local treatment of osteomyelitis. J. Orthop. Res. 2020, 38, 2091–2103. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, J.; Diefenbeck, M.; McNally, M. Ceramic Biocomposites as Biodegradable Antibiotic Carriers in the Treatment of Bone Infections. J. Bone Jt. Infect. 2017, 2, 38–51. [Google Scholar] [CrossRef]
- ter Boo, G.J.; Grijpma, D.W.; Moriarty, T.F.; Richards, R.G.; Eglin, D. Antimicrobial delivery systems for local infection prophylaxis in orthopedic- and trauma surgery. Biomaterials 2015, 52, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Carver, D.C.; Kuehn, S.B.; Weinlein, J.C. Role of Systemic and Local Antibiotics in the Treatment of Open Fractures. Orthop. Clin. N. Am. 2017, 48, 137–153. [Google Scholar] [CrossRef]
- Masters, E.A.; Trombetta, R.P.; de Mesy Bentley, K.L.; Boyce, B.F.; Gill, A.L.; Gill, S.R.; Nishitani, K.; Ishikawa, M.; Morita, Y.; Ito, H.; et al. Evolving concepts in bone infection: Redefining “biofilm”, “acute vs. chronic osteomyelitis”, “the immune proteome” and “local antibiotic therapy”. Bone Res. 2019, 7, 20. [Google Scholar] [CrossRef] [PubMed]
- Muir, R.; Birnie, C.; Hyder-Wilson, R.; Ferguson, J.; McNally, M.A. Does local implantation of gentamicin impair renal function in patients undergoing surgery for chronic bone infection? Int. J. Res. Orthop. 2021, 7, 438–443. [Google Scholar] [CrossRef]
- McLaren, A.C. Alternative materials to acrylic bone cement for delivery of depot antibiotics in orthopaedic infections. Clin. Orthop. Relat. Res. 2004, 427, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Morgenstern, M.; Vallejo, A.; McNally, M.A.; Moriarty, T.F.; Ferguson, J.Y.; Nijs, S.; Metsemakers, W.J. The effect of local antibiotic prophylaxis when treating open limb fractures: A systematic review and meta-analysis. Bone Jt. Res. 2018, 7, 447–456. [Google Scholar] [CrossRef]
- Pinto, D.; Manjunatha, K.; Savur, A.D.; Ahmed, N.R.; Mallya, S.; Ramya, V. Comparative study of the efficacy of gentamicin-coated intramedullary interlocking nail versus regular intramedullary interlocking nail in Gustilo type I and II open tibia fractures. Chin. J. Traumatol. 2019, 22, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.; Fuchs, T.; Jenks, M.; Fleetwood, K.; Franz, D.; Iff, J.; Raschke, M. Systematic review and meta-analysis of the additional benefit of local prophylactic antibiotic therapy for infection rates in open tibia fractures treated with intramedullary nailing. Int. Orthop. 2014, 38, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.D.; Li-Bland, E.A.; Wild, L.M.; Schemitsch, E.H. A prospective, randomized clinical trial comparing an antibiotic-impregnated bioabsorbable bone substitute with standard antibiotic-impregnated cement beads in the treatment of chronic osteomyelitis and infected nonunion. J. Orthop. Trauma 2010, 24, 483–490. [Google Scholar] [CrossRef]
- McNally, M.A.; Ferguson, J.Y.; Scarborough, M.; Ramsden, A.; Stubbs, D.A.; Atkins, B.L. Mid- to long-term results of single-stage surgery for patients with chronic osteomyelitis using a bioabsorbable gentamicin-loaded ceramic carrier. Bone Jt. J. 2022, 104-B, 1095–1100. [Google Scholar] [CrossRef]
- Zhou, C.H.; Ren, Y.; Ali, A.; Meng, X.Q.; Zhang, H.A.; Fang, J.; Qin, C.H. Single-stage treatment of chronic localized tibial osteomyelitis with local debridement and antibiotic-loaded calcium sulfate implantation: A retrospective study of 42 patients. J. Orthop. Surg. Res. 2020, 15, 201. [Google Scholar] [CrossRef] [PubMed]
- Gitelis, S.; Brebach, G.T. The treatment of chronic osteomyelitis with a biodegradable antibiotic-impregnated implant. J. Orthop. Surg. 2002, 10, 53–60. [Google Scholar] [CrossRef]
- Zhang, H.A.; Zhou, C.H.; Meng, X.Q.; Fang, J.; Qin, C.H. Intramedullary reaming and irrigation and antibiotic-loaded calcium sulfate implantation for the treatment of infection after intramedullary nailing: A retrospective study of 19 cases. BMC Musculoskelet Disord. 2020, 21, 710. [Google Scholar] [CrossRef]
- Ferguson, J.Y.; Dudareva, M.; Riley, N.D.; Stubbs, D.; Atkins, B.L.; McNally, M.A. The use of a biodegradable antibiotic-loaded calcium sulphate carrier containing tobramycin for the treatment of chronic osteomyelitis: A series of 195 cases. Bone Jt. J. 2014, 96, 829–836. [Google Scholar] [CrossRef]
- Patzakis, M.J.; Mazur, K.; Wilkins, J.; Sherman, R.; Holtom, P. Septopal beads and autogenous bone grafting for bone defects in patients with chronic osteomyelitis. Clin. Orthop. Relat. Res. 1993, 295, 112–118. [Google Scholar] [CrossRef]
- Calhoun, J.H.; Henry, S.L.; Anger, D.M.; Cobos, J.A.; Mader, J.T. The treatment of infected nonunions with gentamicin-polymethylmethacrylate antibiotic beads. Clin. Orthop. Relat. Res. 1993, 295, 23–27. [Google Scholar] [CrossRef]
- Romanò, C.L.; Logoluso, N.; Meani, E.; Romanò, D.; De Vecchi, E.; Vassena, C.; Drago, L. A comparative study of the use of bioactive glass S53P4 and antibiotic-loaded calcium-based bone substitutes in the treatment of chronic osteomyelitis: A retrospective comparative study. Bone Jt. J. 2014, 96, 845–850. [Google Scholar] [CrossRef]
- Chang, W.; Colangeli, M.; Colangeli, S.; Di Bella, C.; Gozzi, E.; Donati, D. Adult osteomyelitis: Debridement versus debridement plus Osteoset T pellets. Acta Orthop. Belg. 2007, 73, 238–243. [Google Scholar]
- McKee, M.D.; Wild, L.M.; Schemitsch, E.H.; Waddell, J.P. The use of an antibiotic-impregnated, osteoconductive, bioabsorbable bone substitute in the treatment of infected long bone defects: Early results of a prospective trial. J. Orthop. Trauma 2002, 16, 622–627. [Google Scholar] [CrossRef]
- Patel, P.; Iliadis, A.D.; Vris, A.; Heidari, N.; Trompeter, A. Intramedullary application of local antibiotic bullets for the treatment of long bone fracture related infection. Eur. J. Orthop. Surg. Traumatol. 2022. [Google Scholar] [CrossRef]
- Hake, M.E.; Young, H.; Hak, D.J.; Stahel, P.F.; Hammerberg, E.M.; Mauffrey, C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury 2015, 46, 1447–1456. [Google Scholar] [CrossRef]
- Palmer, M.P.; Altman, D.T.; Altman, G.T.; Sewecke, J.J.; Ehrlich, G.D.; Hu, F.Z.; Nistico, L.; Melton-Kreft, R.; Gause, T.M., III; Costerton, J.W. Can we trust intraoperative culture results in nonunions? J. Orthop. Trauma 2014, 28, 384–390. [Google Scholar] [CrossRef]
- Malchau, K.S.; Tillander, J.; Zaborowska, M.; Hoffman, M.; Lasa, I.; Thomsen, P.; Malchau, H.; Rolfson, O.; Trobos, M. Biofilm properties in relation to treatment outcome in patients with first-time periprosthetic hip or knee joint infection. J. Orthop. Translat. 2021, 30, 31–40. [Google Scholar] [CrossRef]
- Scott, C.P.; Higham, P.A.; Dumbleton, J.H. Effectiveness of bone cement containing tobramycin. An in vitro susceptibility study of 99 organisms found in infected joint arthroplasty. J. Bone Jt. Surg. Br. 1999, 81, 440–443. [Google Scholar] [CrossRef]
- Stravinskas, M.; Horstmann, P.; Ferguson, J.; Hettwer, W.; Nilsson, M.; Tarasevicius, S.; Petersen, M.M.; McNally, M.A.; Lidgren, L. Pharmacokinetics of gentamicin eluted from a regenerating bone graft substitute: In vitro and clinical release studies. Bone Jt. Res. 2016, 5, 427–435. [Google Scholar] [CrossRef]
- Badha, V.; Moore, R.; Heffernan, J.; Castaneda, P.; McLaren, A.; Overstreet, D. Determination of Tobramycin and Vancomycin Exposure Required to Eradicate Biofilms on Muscle and Bone Tissue In Vitro. J. Bone Jt. Infect. 2019, 4, 1–9. [Google Scholar] [CrossRef]
- Willenegger, H.; Roth, B. Treatment tactics and late results in early infection following osteosynthesis. Unfallchirurgie 1986, 12, 241–246. [Google Scholar] [CrossRef]
- Lazzarini, L.; Mader, J.T.; Calhoun, J.H. Osteomyelitis in long bones. J. Bone Jt. Surg. Am. 2004, 86, 2305–2318. [Google Scholar] [CrossRef]
- Cierny, G., 3rd; DiPasquale, D. Treatment of chronic infection. J. Am. Acad. Orthop. Surg. 2006, 14, S105–S110. [Google Scholar] [CrossRef]
- McNally, M.; Corrigan, R.; Sliepen, J.; Dudareva, M.; Rentenaar, R.; IJpma, F.; Atkins, B.L.; Wouthuyzen-Bakker, M.; Govaert, G. What factors affect outcome in the treatment of fracture-related infection? Antibiotics 2022, 11, 946. [Google Scholar] [CrossRef]
- Bakhtiari, I.G.; Vles, G.; Busch, S.M.; Frommelt, L.; Gehrke, T.; Salber, J.; Citak, M. Septic Failure After One-Stage Exchange for Prosthetic Joint Infection of the Hip: Microbiological Implications. J. Arthroplast. 2022, 37, 373–378. [Google Scholar] [CrossRef]
- Zhou, C.H.; Ren, Y.; Song, H.J.; Ali, A.A.; Meng, X.Q.; Xu, L.; Zhang, H.A.; Fang, J.; Qin, C.H. One-stage debridement and bone transport versus first-stage debridement and second-stage bone transport for the management of lower limb post-traumatic osteomyelitis. J. Orthop. Translat. 2021, 28, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Pesch, S.; Hanschen, M.; Greve, F.; Zyskowski, M.; Seidl, F.; Kirchhoff, C.; Biberthaler, P.; Huber-Wagner, S. Treatment of fracture-related infection of the lower extremity with antibiotic-eluting ceramic bone substitutes: Case series of 35 patients and literature review. Infection 2020, 48, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Pincher, B.; Fenton, C.; Jeyapalan, R.; Barlow, G.; Sharma, H.K. A systematic review of the single-stage treatment of chronic osteomyelitis. J. Orthop. Surg. Res. 2019, 14, 393. [Google Scholar] [CrossRef] [PubMed]
- Fleiter, N.; Walter, G.; Bösebeck, H.; Vogt, S.; Büchner, H.; Hirschberger, W.; Hoffmann, R. Clinical use and safety of a novel gentamicin-releasing resorbable bone graft substitute in the treatment of osteomyelitis/osteitis. Bone Jt. Res. 2014, 3, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Badie, A.A.; Arafa, M.S. One-stage surgery for adult chronic osteomyelitis: Concomitant use of antibiotic-loaded calcium sulphate and bone marrow aspirate. Int. Orthop. 2019, 43, 1061–1070. [Google Scholar] [CrossRef] [PubMed]
- Zalavras, C.G.; Patzakis, M.J.; Holtom, P. Local antibiotic therapy in the treatment of open fractures and osteomyelitis. Clin. Orthop. Relat. Res. 2004, 427, 86–93. [Google Scholar] [CrossRef]
- van Raaij, T.M.; Visser, L.E.; Vulto, A.G.; Verhaar, J.A. Acute renal failure after local gentamicin treatment in an infected total knee arthroplasty. J. Arthroplast. 2002, 17, 948–950. [Google Scholar] [CrossRef]
- Ruppen, C.; Hemphill, A.; Sendi, P. In vitro activity of gentamicin as an adjunct to penicillin against biofilm group B Streptococcus. J. Antimicrob. Chemother. 2017, 72, 444–447. [Google Scholar] [CrossRef]
- Corrigan, R.A.; Sliepen, J.; Rentenaar, R.J.; IJpma, F.F.A.; Hietbrink, F.; Atkins, B.L.; Dudareva, M.; Govaert, G.A.M.; McNally, M.A.; Wouthuyzen-Bakker, M. The Effect of Guideline based Antimicrobial Therapy on the outcome of Fracture-Related Infections (EAT FRI Study). Clin. Microbiol. Infect. 2022. submitted. [Google Scholar]
- Metsemakers, W.J.; Morgenstern, M.; McNally, M.A.; Moriarty, T.F.; McFadyen, I.; Scarborough, M.; Athanasou, N.A.; Ochsner, P.E.; Kuehl, R.; Raschke, M.; et al. Fracture-related infection: A consensus on definition from an international expert group. Injury 2018, 49, 505–510. [Google Scholar] [CrossRef]
- Govaert, G.A.; Kuehl, R.; Atkins, B.L.; Trampuz, A.; Morgenstern, M.; Obremskey, W.T.; Verhofstad, M.H.; McNally, M.A.; Metsemakers, W.J. Diagnosing Fracture-Related Infection: Current Concepts and Recommendations. J. Orthop. Trauma 2020, 34, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Depypere, M.; Kuehl, R.; Metsemakers, W.J.; Senneville, E.; McNally, M.A.; Obremskey, W.T.; Zimmerli, W.; Atkins, B.L.; Trampuz, A. Recommendations for Systemic Antimicrobial Therapy in Fracture-Related Infection: A Consensus from an International Expert Group. J. Orthop. Trauma 2020, 34, 30–41. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Govaert, G.; Dudareva, M.; Morgenstern, M.; Metsemakers, W.J. Definition and diagnosis of fracture-related infection. EFORT Open Rev. 2020, 5, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Dudareva, M.; Barrett, L.; Figtree, M.; Scarborough, M.; Watanabe, M.; Newnham, R.; Wallis, R.; Oakley, S.; Kendrick, B.; Stubbs, D.; et al. Sonication versus Tissue Sampling for Diagnosis of Prosthetic Joint and Other Orthopedic Device-Related Infections. J. Clin. Microbiol. 2018, 56, e00688-18. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort (n = 433) | Local Antibiotics Group (n = 251) | No Local Antibiotics Group (n = 182) | p-Value | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Sex (male) | 318 (73.4) | 191 (76.1) | 127 (69.8) | 0.142 |
| Age (years): median (P25–P75) | 50.6 (36.3–62.0) | 50.0 (37.0–62.0) | 51.5 (33.0–63.0) | 0.750 |
| BMI (kg/m2): median (P25–P75) | 27.0 (23.3–30.4) | 27.7 (23.5–31.0) | 26.3 (23.1–29.7) | 0.068 |
| Smoker (yes) | 112 (25.9) | 56 (22.3) | 56 (30.8) | 0.047 * |
| Diabetes (yes) | 47 (10.9) | 28 |(11.2) | 19 (10.4) | 0.813 |
| Immunosuppressives | 17(3.9) | 9 (3.6) | 8 (4.4) | 0.668 |
| Renal function (eGFR) | 0.114 | |||
| Normal (≥90 mL/min/1.73 m2) | 310 (71.6) | 178 (70.9) | 132 (72.5) | |
| Impaired (<90 mL/min/1.73 m2) | 115 (26.6) | 71 (28.3) | 44 (24.2) | |
| Not determined | 8 (1.8) | 2 (0.8) | 6 (3.3) | |
| Fracture characteristics (Location) | ||||
| Humerus | 20 (4.6) | 11 (4.4) | 9 (4.9) | 0.783 |
| Forearm | 26 (6.0) | 16 (6.4) | 10 (5.5) | 0.704 |
| Femur | 94 (21.7) | 65 (25.9) | 29 (15.9) | 0.013 * |
| Tibia | 219 (50.6) | 130 (51.8) | 89 (48.9) | 0.552 |
| Tibia and fibula | 6 (1.4) | 6 (2.4) | 0 (0) | 0.042 * |
| Fibula | 13 (3.0) | 12 (4.8) | 1 (0.5) | 0.011 * |
| Pelvis | 26 (6.0) | 4 (1.6) | 22 (12.1) | <0.001 * |
| Clavicle | 6 (1.4) | 0 (0) | 6 (3.3) | 0.005 * |
| Tibia and talus | 1 (0.2) | 1 (0.4) | 0 (0) | 1.000 |
| Calcaneus | 11 (2.5) | 4 (1.6) | 7 (3.8) | 0.215 |
| Midfoot | 3 (0.7) | 1 (0.4) | 2 (1.1) | 0.575 |
| Foot (crush) | 5 (1.2) | 0 (0) | 5 (2.7) | 0.013 * |
| Sternum | 1 (0.2) | 0 (0) | 1 (0.5) | 0.420 |
| Patella | 2 (0.5) | 1 (0.4) | 1 (0.5) | 1.000 |
| Fracture healed at time of surgery | <0.001 * | |||
| Yes | 190 (43.9) | 163 (64.8) | 27 (14.8) | |
| No | 243 (56.1) | 88 (35.1) | 155 (85.2) | |
| Time to onset of infection (weeks): median (P25–P75) | 44.0 (6.0–356.0) | 125.0 (39.0–806.0) | 6.5 (3.0–38.0) | <0.001 * |
| Surgical approach | <0.001 * | |||
| DAIR | 139 (32.1) | 22 (8.8) | 117 (64.3) | <0.001 * |
| Exchange to new internal fixation | 24 (5.6) | 10 (4.0) | 14 (7.7) | 0.096 |
| Fixation removed | 95 (21.9) | 73 (29.1) | 22 (12.1) | <0.001 * |
| Exchange to external fixation | 68 (15.7) | 51 (20.3) | 17 (9.3) | 0.002 * |
| Internal fixation | 1 (0.2) | 0 (0) | 1 (0.5) | 0.420 |
| No fixation used | 106 (24.5) | 95 (37.8) | 11 (6.0) | <0.001 * |
| Soft tissue status | 0.012 * | |||
| Direct closure possible | 300 | 162 (64.5) | 138 (75.8) | |
| Direct closure not possible (SSG, local/free flap) | 133 | 89 (35.5) | 44 (24.2) | |
| Microbiology | ||||
| Monomicrobial | 199 (46.0) | 123 (49.0) | 76 (41.8) | 0.144 |
| Polymicrobial | 154 (35.6) | 65 (25.9) | 89 (48.9) | <0.001 * |
| Culture negative | 80 (18.5) | 63 (25.1) | 17 (9.3) | <0.001 * |
| Characteristics | n | Recurrence of Infection n (%) | HR | 95% CI | |
|---|---|---|---|---|---|
| Yes | No | ||||
| Antibiotic loaded carrier used (all time points) | 433 | ||||
| Yes | 251 | 25 (10.0) | 226 (90.0) | 0.48 | 0.29–0.81 * |
| No | 182 | 34 (18.7) | 148 (81.3) | ||
| Susceptible to local antibiotics | 244 | ||||
| Yes | 16 (9.0) | 162 (91.0) | 0.75 | 0.32–1.74 | |
| No | 8 (12.1) | 58 (87.9) | |||
| Antibiotic-loaded carrier bioabsorbable | 251 | ||||
| Yes | 16 (7.5) | 197 (92.5) | - | - | |
| No | 9 (23.7) | 29 (76.3) | |||
| Antimicrobial Agents | n (%) | Susceptible to Local Antibiotics | Recurrence of Infection | |
|---|---|---|---|---|
| No n = 66 (%) | Yes n = 178 (%) | n = 58 (%) | ||
| Gentamicin | 221 (51.9) | 64 (29.0) | 157 (71.0) | 22 (10.0) |
| Gentamicin and Vancomycin | 11 (2.6) | 1 (9.1) | 10 (90.9) | 1 (9.1) |
| Gentamicin and Clindamycin | 3 (0.7) | 1 (33.3) | 2 (66.7) | 1 (33.3) |
| Gentamicin and Tobramycin | 6 (1.4) | 0 (0) | 6 (100) | 0 (0) |
| Gentamicin and Vancomycin and Colistin | 1 (0.2) | 0 (0) | 1 (100) | 0 (0) |
| Vancomycin | 2 (0.5) | 0 (0) | 2 (1.1) | 0 (0) |
| None | 182 (43.0) | - | - | 34 (18.7) |
| Antibiotic Carriers | n (%) |
|---|---|
| Cerament G | 147 (58.6) |
| Cerament V | 1 (0.4) |
| Herafill G | 11 (4.4) |
| Osteoset T | 2 (0.8) |
| PMMA | 38 (15.1) |
| Cerament G + Herafill | 42 (16.7) |
| Cerament G + Herafill + Cerament V | 2 (0.8) |
| Cerament G + Osteoset T | 8 (3.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sliepen, J.; Corrigan, R.A.; Dudareva, M.; Wouthuyzen-Bakker, M.; Rentenaar, R.J.; Atkins, B.L.; Govaert, G.A.M.; McNally, M.A.; IJpma, F.F.A. Does the Use of Local Antibiotics Affect Clinical Outcome of Patients with Fracture-Related Infection? Antibiotics 2022, 11, 1330. https://doi.org/10.3390/antibiotics11101330
Sliepen J, Corrigan RA, Dudareva M, Wouthuyzen-Bakker M, Rentenaar RJ, Atkins BL, Govaert GAM, McNally MA, IJpma FFA. Does the Use of Local Antibiotics Affect Clinical Outcome of Patients with Fracture-Related Infection? Antibiotics. 2022; 11(10):1330. https://doi.org/10.3390/antibiotics11101330
Chicago/Turabian StyleSliepen, Jonathan, Ruth A. Corrigan, Maria Dudareva, Marjan Wouthuyzen-Bakker, Rob J. Rentenaar, Bridget L. Atkins, Geertje A. M. Govaert, Martin A. McNally, and Frank F. A. IJpma. 2022. "Does the Use of Local Antibiotics Affect Clinical Outcome of Patients with Fracture-Related Infection?" Antibiotics 11, no. 10: 1330. https://doi.org/10.3390/antibiotics11101330
APA StyleSliepen, J., Corrigan, R. A., Dudareva, M., Wouthuyzen-Bakker, M., Rentenaar, R. J., Atkins, B. L., Govaert, G. A. M., McNally, M. A., & IJpma, F. F. A. (2022). Does the Use of Local Antibiotics Affect Clinical Outcome of Patients with Fracture-Related Infection? Antibiotics, 11(10), 1330. https://doi.org/10.3390/antibiotics11101330