1. Introduction
Lower respiratory tract infections (LRTIs) are the most common infections in humans. It is estimated that 2.74 million deaths worldwide occur each year due to LRTIs [
1]. The commonest LRTIs are acute bronchitis, acute trachea bronchitis, chronic bronchitis, and pneumonia, which account for 4.4% of all hospital admissions and are associated with high morbidity, mortality, and excessive health costs [
2,
3,
4]. The incidence and related mortality due to LRTIs can be influenced by several factors, including age, gender, season, the type of population at risk, but mainly to antibiotic therapy, the distribution of causative agents, and the prevalence of antimicrobial resistance [
5,
6]. The microbial aetiology of LRTIs and their susceptibility profile to antibiotics varies in different geographic regions [
7,
8]. The most common bacterial agents of LRTIs are Gram-positive bacteria such as
Staphylococcus aureus and
Enterococcus spp., and Gram-negative bacteria such as
Pseudomonas spp.,
Acinetobacter spp.,
Klebsiella pneumoniae, and
Haemophilus influenzae [
9,
10,
11,
12].
Due to the severity of these infections, there is an urgent need to adopt empirical antimicrobial treatment, before receiving the result on bacterial aetiology and antimicrobial susceptibility patterns [
13,
14]. Unfortunately, the ongoing spread of extended-spectrum β-lactamases and carbapenems has begun to limit the clinical effectiveness of β-lactam agents. This trend is presumably due to the empirical administration of antibacterial therapy [
15,
16]. The situation is further complicated by the emergence of multi-resistant pathogens, such as
Klebsiella pneumoniae carbapenemase and
Haemophilus influenzae 𝛽-lactamase [
17,
18]. Therefore, current knowledge of bacterial etiology and their antimicrobial susceptibility pattern would help to choose the antimicrobial therapy for bacterial LRTIs, to limit the development of antimicrobial resistance and reduce overall management costs [
19,
20,
21]. The aim of this study was to describe the prevalence and patterns of antimicrobial sensitivity of microorganisms isolated from respiratory samples of patients with LRTIs, admitted to the San Giovanni di Dio e Ruggi d’Aragona Hospital (Salerno, Italy), to improve treatment protocols.
3. Discussion
The aim of the study was to determine the prevalence of microorganisms responsible to LRTIs in our hospital and their susceptibility profile to antibiotics. From 2015 to 2019, 7038 sputum and bronchoaspirate samples were analyzed, among them 2753 (39.1%) produced a significant growth of microorganisms on culture media, with a higher incidence in bronchoaspirate samples compared to sputum (52.7% vs. 25.1%). Recently published articles show similar incidence rates to ours [
22,
23,
24].
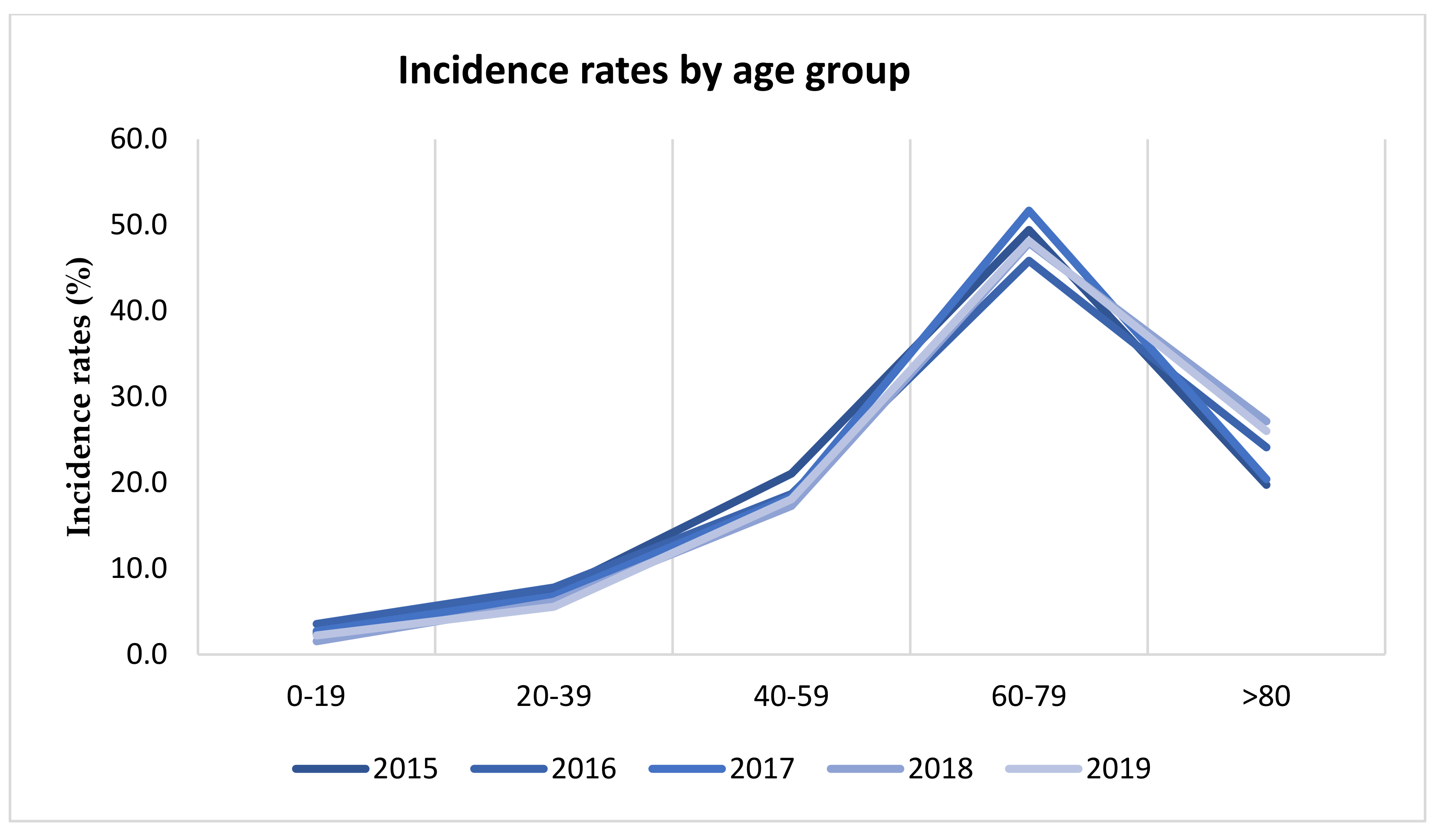
LRTIs were more common in males than females (67.1% vs. 32.9%). Male prevalence of LRTI may be due to some associated risk factors for respiratory tract infection such as smoking, alcohol consumption and COPD [
12,
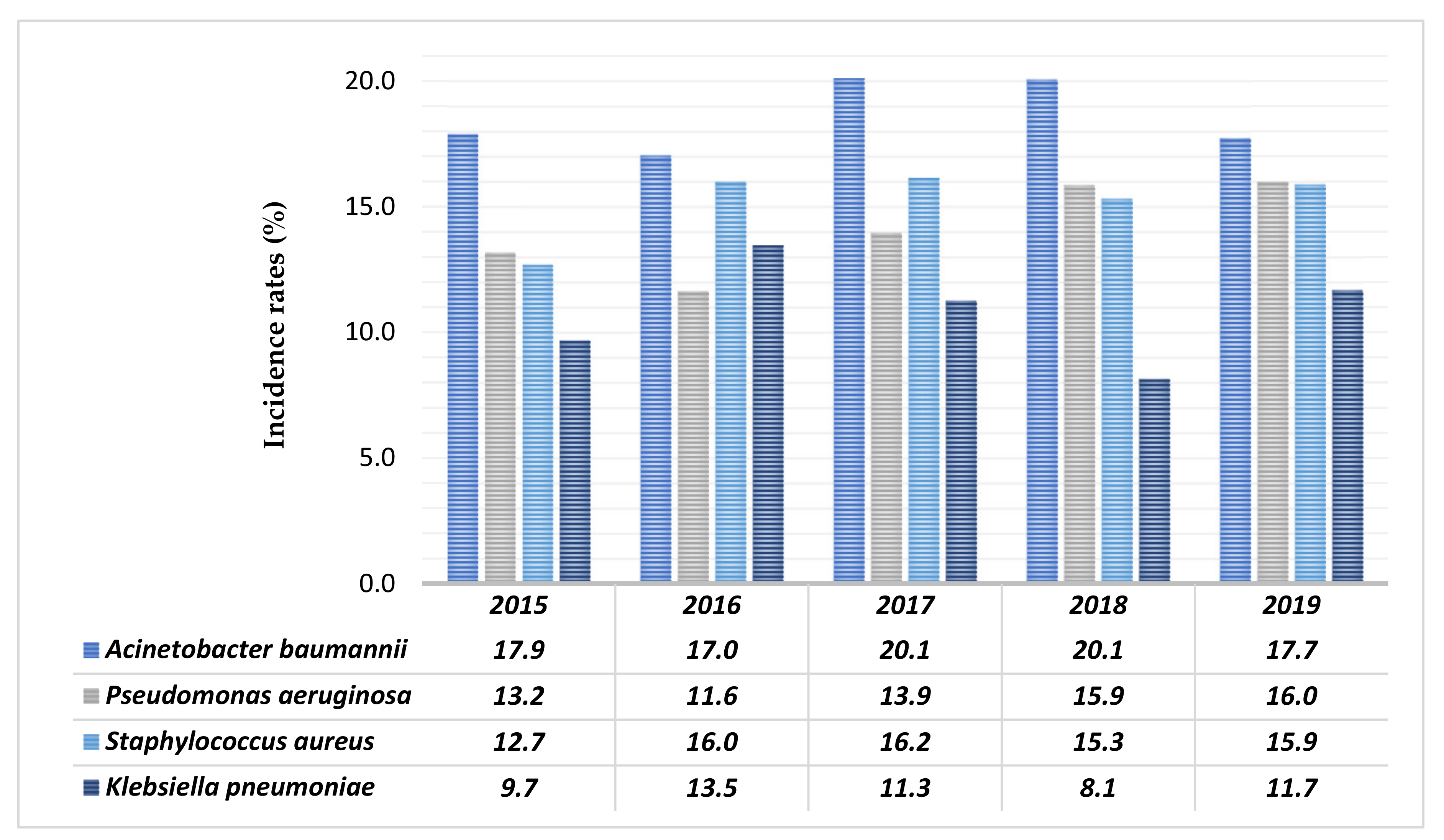
25]. Age range distribution showed that the incidence of LTRIs increases rapidly with increasing age, with a maximum incidence between 60 and 79 years. Among 4278 pathogenic microorganism isolates, 72.5% were Gram-negative bacteria, 24.5% were Gram-positive bacteria, and 3.0% were
Candida spp. In similar studies, Gram-negative bacteria represented the species most commonly isolated from samples by patients of lower respiratory tract infections [
26,
27]. In the current investigation, monomicrobial growth was found in 74.7% of the cases, whereas 25.3% were polymicrobial, and identification of the polymicrobial infection is very important for treatment strategies. In another study, monomicrobial growth was found in 80% of cases, whereas 20% were polymicrobial [
28]. The major microorganisms causing LRTI were
Acinetobacter baumannii,
Staphylococcus aureus,
Pseudomonas aeruginosa, and
Klebsiella pneumoniae. This observation is similar to other studies, such that of Christopher Aye Egbe et al., in which the most frequent mixed infection was caused by
Klebsiella spp. and
Pseudomonas spp. [
12,
24,
29].
Antimicrobial susceptibility test performed on
Acinetobacter baumannii isolates showed that Colistin was the most effective (nearly 100% sensitivity) and Amoxicillin/Clavulanic acid, Cefotaxime, Oxacillin, Ciprofloxacin, Ertapenem, Gentamicin, Imipenem, and Trimethoprim/Sulfamethoxazole were the least effective ones (98–100% resistance). The causes may be due to the high propensity of this species to easily acquire resistance genes and the ability to persist and multiply in a hospital setting. The high rates of resistance to first-line antimicrobial drugs shown by
A. baumannii isolate highlight the need to find new effective molecules to counter this threat [
30,
31,
32,
33,
34].
Pseudomonas aeruginosa was the second commonest organism among Gram-negative bacteria isolated. In the case of
P. aeruginosa, Gentamycin, Amikacin, and Colistin were the most effective antibiotics (less to 20% resistance), contrary to Piperacillin/Tazobactam and Ciprofloxacin that was the least effective (40–50% resistance). The antibiotic resistance rates shown in
P. aeruginosa are similar to results shown by a study by Yayan J. et al. [
35]
The most species isolated of Gram-positive was
Staphylococcus aureus. This species was found to be mostly resistant against Penicillin G and medium resistant to Oxacillin, followed by Macrolides, Lincosamides and Fluoroquinolones class. The antibiotics more efficient against
S. aureus were Gentamicin, Tetracycline, Tigecycline, Teicoplanin, Vancomycin, and Linezolid, with a rate of resistance less to 10%. Oxacillin, Vancomycin, and Teicoplanin showed very low resistance rates, but a worrying increasing trend over the years of study. This event may have been caused by the increase in Oxacillin-resistant
S. aureus MRSA, which are treated with Vancomycin and Teicoplanin; consequently, an increase in resistance to the latter has been observed. The same event has been documented in other articles [
36,
37,
38,
39,
40].
Among Gram-negative bacteria, in terms of frequency,
P. aeruginosa was followed by
Klebsiella pneumoniae. This species was mostly resistant to Penicillin, Cephalosporins, and Fluoroquinolones class (above 70%). Moreover, in this case, the most efficient antibiotic was Colistin, with resistance rates higher than 10%, while the Carbapenems, Aminoglycosides and Tetracyclines class have higher resistances, around 45%. In a study by Ahmed et al.,
K. pneumoniae showed similar resistance rates, except for Piperacillin/Tazobactam, with a reported resistance rate of 18.2%, lower than that shown in our study (73.3%) [
41]. This difference could be due to a different empirical antimicrobial treatment and a different geographic region, as described by Prestinaci et al. [
42]. Very recent reports indicated Gram-negative bacteria were the major microorganisms involved in LRTIs [
12,
43] and were reported to increase resistance to Carbapenems and Fluoroquinolones for
K. pneumoniae. Another hand, among Gram-positive,
S. aureus was the main bacteria isolated reported and showed high susceptibility to Vancomycin and Linezolid, findings are the same as observed in our study. According to a recent WHO report on the epidemiology of infectious diseases, LRTI tops the list in developing countries [
44]. This study reveals the incidence of the main pathogens responsible for LRTI and their resistance to the most commonly used antibiotics in hospital settings [
45,
46]. The results show high rates of resistance by the most commonly isolated bacteria. Resistance to Fluoroquinolones and 3rd generation Cephalosporins is rapidly emerging [
47]. This may be due to irrational drug abuse and the resulting mutation of pathogenic microorganisms [
48,
49].
4. Materials and Methods
4.1. Samples Collection
The present retrospective study was conducted in the Microbiology department of University Hospital “San Giovanni di Dio e Ruggi d’Aragona” in the period between January 2015 and December 2019.
Sputum and bronchial aspiration samples from patients with suspected lower respiratory tract infection (LRTI) were analyzed. A total of 7038 samples were collected from patients of all age and gender groups.
4.2. Identification and Antimicrobial Susceptibility Testing
The samples were collected in sterile containers and immediately transported to the bacteriology laboratory and were processed further. Only those samples with an adequate amount of sputum were accepted. Those that contained an inadequate amount of sputum for analysis or that contained only saliva were excluded.
Sputum specimen for bacteriological culture was subjected to Gram-staining and examined microscopically. In microscopic examination sputum smear containing less than 10 squamous epithelial cells and more than 25 leucocytes or pus cells per low power, field confirmed the reliability of the specimen, indicating that it was not contaminated with saliva. The samples of sputum which were very thick and mucoid were first homogenized with commercially available sputasol containing 0.01% dithiothreitol and were incubated at 37 °C for 30 min for complete homogenization of sputum.
All samples were immediately plated on Chocolate agar, blood agar, MacConkey, and Sabouraud Glucose agar medium (Oxoid, Hampshire, UK), and were incubated at 37 °C. The Chocolate agar was incubated at 37 °C in a 5% CO2 atmosphere. After 18–36 h of incubation, each plate was examined, and bacterial identification and antimicrobial susceptibility test were performed.
Sputum or bronchoaspirate showing less than 104 CFU/ml by semiquantitative culture were regarded as commensal or contaminant and were excluded. The bacterial identification and antimicrobial susceptibility test were performed utilizing a Vitek 2 (bioMerieux, Marcy l’Etoile, France), using an identification card (ID-GN for Gram-Negative, ID-GP for Gram-positive, YST for yeast) and the AST-659 (for Staphylococci), AST-658 (for Enterococci and S. agalactiae), AST-ST03 (for Pneumococci), AST-379 (for Enterobacteriaceae), and AST-397 (for GN non-fermenters) susceptibility cards, according to the manufacturer’s instructions. The results of antimicrobial susceptibility were interpreted as “susceptible”, “resistant”, or “intermediate” according to EUCAST guidelines. The Quality Control process encompasses the annual service and certification of the instrument by bioMérieux and the Quality Control of each lot of Gram-negative (GN), Gram-positive (GP) cards using four strains: Enterococcus ATCC 700,327 and Staphylococcus aureus ATCC 29,213 for GP; Enterobacter ATCC 700,323 and Klebsiella oxytoca ATCC 700,324 for GN.
The following antibiotics were included in the present study: amikacin (AMK), amoxicillin/clavulanic acid (AMC), azithromycin (AZM), cefepime (FEP), cefotaxime (CTX), ceftazidime (CAZ), ciprofloxacin (CIP), clarithromycin (CLR), colistin (COL), ertapenem (ETP), erythromycin (ERY), gentamicin (GEN), imipenem (IPM), levofloxacin (LVX), linezolid (LNZ), meropenem (MEM), moxifloxacin (MFX), oxacillin (OXA), piperacillin/tazobactam (TZP), teicoplanin (TEC), tigecycline (TCG), vancomycin (VAN).
4.3. Ethical Consideration Statement
Ethical approval by the Human Research Ethics Committee was not requested. The present study used laboratory management data, collected from a database. This is a retrospective study and not directly associated with patients.
4.4. Statistical Analysis
Demographic data of patients, including age, gender, isolated strain(s), and drug sensitivity results, were used for the analysis. The crude incidence and age- and sex-standardized incidence were calculated. The chi-framework test was used to compare the differences in the incidence of bacteria in hospitalized patients and the differences among antibiotic sensitivities over the range of years considered in the study. A chi-square test was used to verify the possible associations between the categorical variables, while the Cochran–Armitage trend test was used to verify the existence of a trend, the existence of a trend was checked only for antibiotics that showed statistically significant differences in the distribution of resistance during the years under consideration, an alpha equal to 5% was considered for both tests, therefore those associations that had a p-value < 0.05 were considered statistically significant. The IBM Statistical Package for Social Sciences Version 22.00 (SPSS Inc., Chicago, IL, USA) was used for data analysis.


 ,
, 








{kind=link}
{kind=link}