
Antimicrobial Susceptibility Patterns and Resistance Trends of Staphylococcus aureus and Coagulase-Negative Staphylococci Strains Isolated from Ocular Infections


 , , , ,
, , , ,  ,
,  , , and
, , and
Abstract
1. Introduction
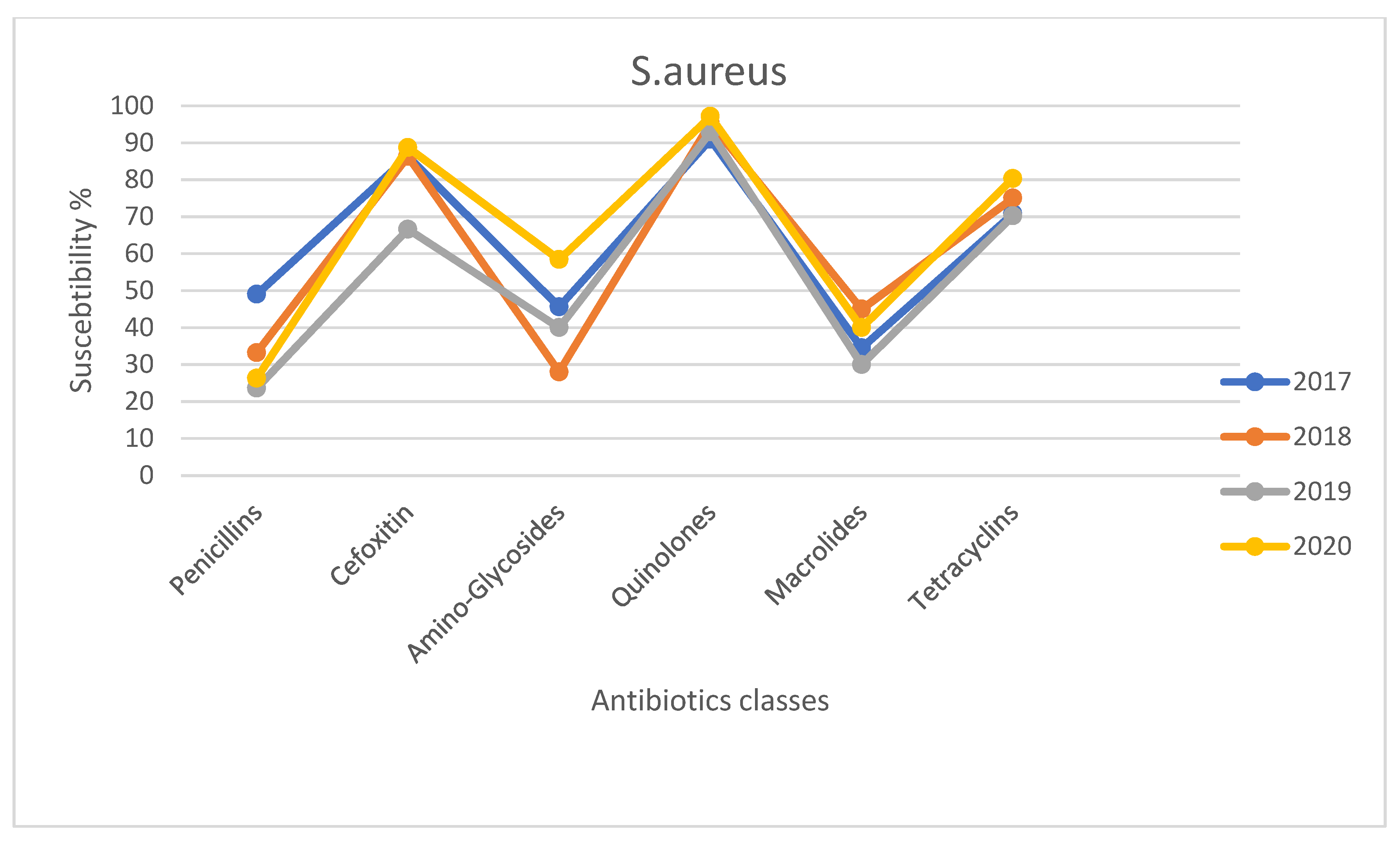
2. Results
3. Discussion
4. Materials and Methods
4.1. Sample Collection
4.2. Bacterial Isolation and Identification
4.3. Antibiotic Susceptibility Test
4.4. Statistical Analysis
4.5. Ethical Consideration Statement.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pleyer, U.; Baatz, H. Antibacterial protection of the ocular surface. Ophthalmologica 1997, 211 (Suppl. 1), 2–8. [Google Scholar] [CrossRef]
- Rose, G.E. Lacrimal drainage surgery in a patient with dry eyes. Dev. Ophthalmol. 2008, 41, 127–137. [Google Scholar] [CrossRef]
- Meyer, D.R. Lacrimal disease and surgery. Curr. Opin. Ophthalmol. 1993, 4, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, F.; Folliero, V.; Santella, B.; Franci, G.; Foglia, F.; Trotta, M.C.; Della Rocca, M.T.; Avitabile, T.; Gagliano, C.; Galdiero, M. Prevalence and Antibiotic Resistance Patterns of Ocular Bacterial Strains Isolated from Pediatric Patients in University Hospital of Campania “Luigi Vanvitelli,” Naples, Italy. Int. J. Microbiol. 2020, 2020, 8847812. [Google Scholar] [CrossRef]
- Klotz, S.A.; Penn, C.C.; Negvesky, G.J.; Butrus, S.I. Fungal and parasitic infections of the eye. Clin. Microbiol. Rev. 2000, 13, 662–685. [Google Scholar] [CrossRef]
- Teweldemedhin, M.; Gebreyesus, H.; Atsbaha, A.H.; Asgedom, S.W.; Saravanan, M. Bacterial profile of ocular infections: A systematic review. BMC ophthalmology 2017, 17, 212. [Google Scholar] [CrossRef]
- O’Callaghan, R.J. The Pathogenesis of Staphylococcus aureus Eye Infections. Pathogens 2018, 7, 9. [Google Scholar] [CrossRef]
- Becker, K.; Heilmann, C.; Peters, G. Coagulase-negative staphylococci. Clin. Microbiol. Rev. 2014, 27, 870–926. [Google Scholar] [CrossRef] [PubMed]
- Getahun, E.; Gelaw, B.; Assefa, A.; Assefa, Y.; Amsalu, A. Bacterial pathogens associated with external ocular infections alongside eminent proportion of multidrug resistant isolates at the University of Gondar Hospital, northwest Ethiopia. BMC Ophthalmol. 2017, 17, 151. [Google Scholar] [CrossRef]
- Schechter, B.A.; Sheppard, J.D.; Sanfilippo, C.M.; DeCory, H.H.; Asbell, P.A. An Evaluation of Staphylococci from Ocular Surface Infections Treated Empirically with Topical Besifloxacin: Antibiotic Resistance, Molecular Characteristics, and Clinical Outcomes. Ophthalmol. Ther. 2020, 9, 159–173. [Google Scholar] [CrossRef] [PubMed]
- Baum, J.; Barza, M. The evolution of antibiotic therapy for bacterial conjunctivitis and keratitis: 1970–2000. Cornea 2000, 19, 659–672. [Google Scholar] [CrossRef]
- Steinert, R.F. Current therapy for bacterial keratitis and bacterial conjunctivitis. Am. J. Ophthalmol. 1991, 112, 10S–14S. [Google Scholar] [PubMed]
- Thomas, R.K.; Melton, R.; Asbell, P.A. Antibiotic resistance among ocular pathogens: Current trends from the ARMOR surveillance study (2009–2016). Clin. Optom. (Auckl.) 2019, 11, 15–26. [Google Scholar] [CrossRef]
- Franci, G.; Falanga, A.; Zannella, C.; Folliero, V.; Martora, F.; Galdiero, M.; Galdiero, S.; Morelli, G.; Galdiero, M. Infectivity inhibition by overlapping synthetic peptides derived from the gH/gL heterodimer of herpes simplex virus type 1. J. Pept. Sci. 2017, 23, 311–319. [Google Scholar] [CrossRef]
- Bertino, J.S., Jr. Impact of antibiotic resistance in the management of ocular infections: The role of current and future antibiotics. Clin. Ophthalmol. (Auckl. N. Z.) 2009, 3, 507–521. [Google Scholar] [CrossRef]
- Watson, S.; Cabrera-Aguas, M.; Khoo, P. Common eye infections. Aust Prescr 2018, 41, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Grzybowski, A.; Brona, P.; Kim, S.J. Microbial flora and resistance in ophthalmology: A review. Graefe’s Arch. Clin. Exp. Ophthalmol. 2017, 255, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Monda, V.; Valenzano, A.; Monda, M. Modifications of Activity of Autonomic Nervous System, and Resting Energy Expenditure in Women Using Hormone-Replacement Therapy. Biol. Med. 2016, 8. [Google Scholar] [CrossRef]
- Singh, M.; Zannella, C.; Folliero, V.; Di Girolamo, R.; Bajardi, F.; Chianese, A.; Altucci, L.; Damasco, A.; Del Sorbo, M.R.; Imperatore, C.; et al. Combating Actions of Green 2D-Materials on Gram Positive and Negative Bacteria and Enveloped Viruses. Front. Bioeng. Biotechnol. 2020, 8, 569967. [Google Scholar] [CrossRef] [PubMed]
- Courtright, P.; West, S.K. Contribution of sex-linked biology and gender roles to disparities with trachoma. Emerg. Infect. Dis. 2004, 10, 2012–2016. [Google Scholar] [CrossRef]
- Aziz, B.; Tawfik, C. Prevalence of dry eye disease among healthy Egyptian population. J. Egypt. Ophthalmol. Soc. 2020, 113, 133–141. [Google Scholar] [CrossRef]
- Schaumberg, D.A.; Uchino, M.; Christen, W.G.; Semba, R.D.; Buring, J.E.; Li, J.Z. Patient Reported Differences in Dry Eye Disease between Men and Women: Impact, Management, and Patient Satisfaction. PLoS ONE 2013, 8, e76121. [Google Scholar] [CrossRef] [PubMed]
- Franci, G.; Crudele, V.; Della Rocca, M.T.; Melardo, C.; Chianese, A.; Finamore, E.; Bencivenga, F.; Astorri, R.; Vitiello, M.; Galdiero, E.; et al. Epstein-Barr Virus Seroprevalence and Primary Infection at the University Hospital Luigi Vanvitelli of Naples from 2007 to 2017. Intervirology 2019, 62, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Farrand, K.F.; Fridman, M.; Stillman, I.Ö.; Schaumberg, D.A. Prevalence of Diagnosed Dry Eye Disease in the United States Among Adults Aged 18 Years and Older. Am. J. Ophthalmol. 2017, 182, 90–98. [Google Scholar] [CrossRef]
- Teweldemedhin, M.; Saravanan, M.; Gebreyesus, A.; Gebreegziabiher, D. Ocular bacterial infections at Quiha Ophthalmic Hospital, Northern Ethiopia: An evaluation according to the risk factors and the antimicrobial susceptibility of bacterial isolates. BMC Infect. Diseases 2017, 17, 207. [Google Scholar] [CrossRef]
- Lorenzo, D. Chloramphenicol Resurrected: A Journey from Antibiotic Resistance in Eye Infections to Biofilm and Ocular Microbiota. Microorganisms 2019, 7, 278. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Gender | n (%) | p-Value |
|---|---|---|
| Male | 155 (48.1%) | - |
| Female | 167 (51.9%) | - |
| Age (Years) by Categories | n (%) | p-Value |
| 0–30 years old | 26 (8.0%) | - |
| 31–60 years old | 81 (25.2%) | - |
| 61–90 years old | 215 (66.8%) | <0.05 * |
| Antimicrobial Agent | % CoNS | % S. aureus | p-Value |
|---|---|---|---|
| Ampicillin | 61.7 | 23.7 | <0.05 * |
| Amoxicillin-Clavulanic Acid | 61.7 | 23.7 | <0.05 * |
| Cefoxitin | 61.7 | 23.7 | <0.05 * |
| Gentamycin | 72.8 | 41.7 | 0.05 * |
| Tobramycin | 72.8 | 41.7 | 0.05 * |
| Clindamycin | 87.5 | 56.0 | <0.05 * |
| Erythromycin | 81.9 | 45.8 | 0.001 * |
| Tetracycline | 58.5 | 28.6 | <0.05 * |
| Ciprofloxacin | 84.2 | 47.6 | <0.05 * |
| Moxifloxacin | 84.2 | 47.6 | <0.05 * |
| Neomycin | 72.8 | 41.7 | 0.05 * |
| Chloramphenicol | 0 | 0 | - |
| Trimethoprim Sulfamethoxazole | 0 | 0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrillo, F.; Pignataro, D.; Di Lella, F.M.; Reibaldi, M.; Fallico, M.; Castellino, N.; Parisi, G.; Trotta, M.C.; D’Amico, M.; Santella, B.; et al. Antimicrobial Susceptibility Patterns and Resistance Trends of Staphylococcus aureus and Coagulase-Negative Staphylococci Strains Isolated from Ocular Infections. Antibiotics 2021, 10, 527. https://doi.org/10.3390/antibiotics10050527
Petrillo F, Pignataro D, Di Lella FM, Reibaldi M, Fallico M, Castellino N, Parisi G, Trotta MC, D’Amico M, Santella B, et al. Antimicrobial Susceptibility Patterns and Resistance Trends of Staphylococcus aureus and Coagulase-Negative Staphylococci Strains Isolated from Ocular Infections. Antibiotics. 2021; 10(5):527. https://doi.org/10.3390/antibiotics10050527
Chicago/Turabian StylePetrillo, Francesco, Danilo Pignataro, Federica Maria Di Lella, Michele Reibaldi, Matteo Fallico, Niccolò Castellino, Guglielmo Parisi, Maria Consiglia Trotta, Michele D’Amico, Biagio Santella, and et al. 2021. "Antimicrobial Susceptibility Patterns and Resistance Trends of Staphylococcus aureus and Coagulase-Negative Staphylococci Strains Isolated from Ocular Infections" Antibiotics 10, no. 5: 527. https://doi.org/10.3390/antibiotics10050527
APA StylePetrillo, F., Pignataro, D., Di Lella, F. M., Reibaldi, M., Fallico, M., Castellino, N., Parisi, G., Trotta, M. C., D’Amico, M., Santella, B., Folliero, V., Della Rocca, M. T., Rinaldi, M., Franci, G., Avitabile, T., Galdiero, M., & Boccia, G. (2021). Antimicrobial Susceptibility Patterns and Resistance Trends of Staphylococcus aureus and Coagulase-Negative Staphylococci Strains Isolated from Ocular Infections. Antibiotics, 10(5), 527. https://doi.org/10.3390/antibiotics10050527