
Molecular and Anti-Microbial Resistance (AMR) Profiling of Methicillin-Resistant Staphylococcus aureus (MRSA) from Hospital and Long-Term Care Facilities (LTCF) Environment

 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Detecting Rates of MRSA from LTCFs and Hospitals in Two Cities
2.2. SCCmec PCR Typing for Predicting the Source of the MRSA Strains
2.3. The Detection of Toxin Genes by PCR
2.4. Antimicrobial Susceptibility of the MRSA Strains
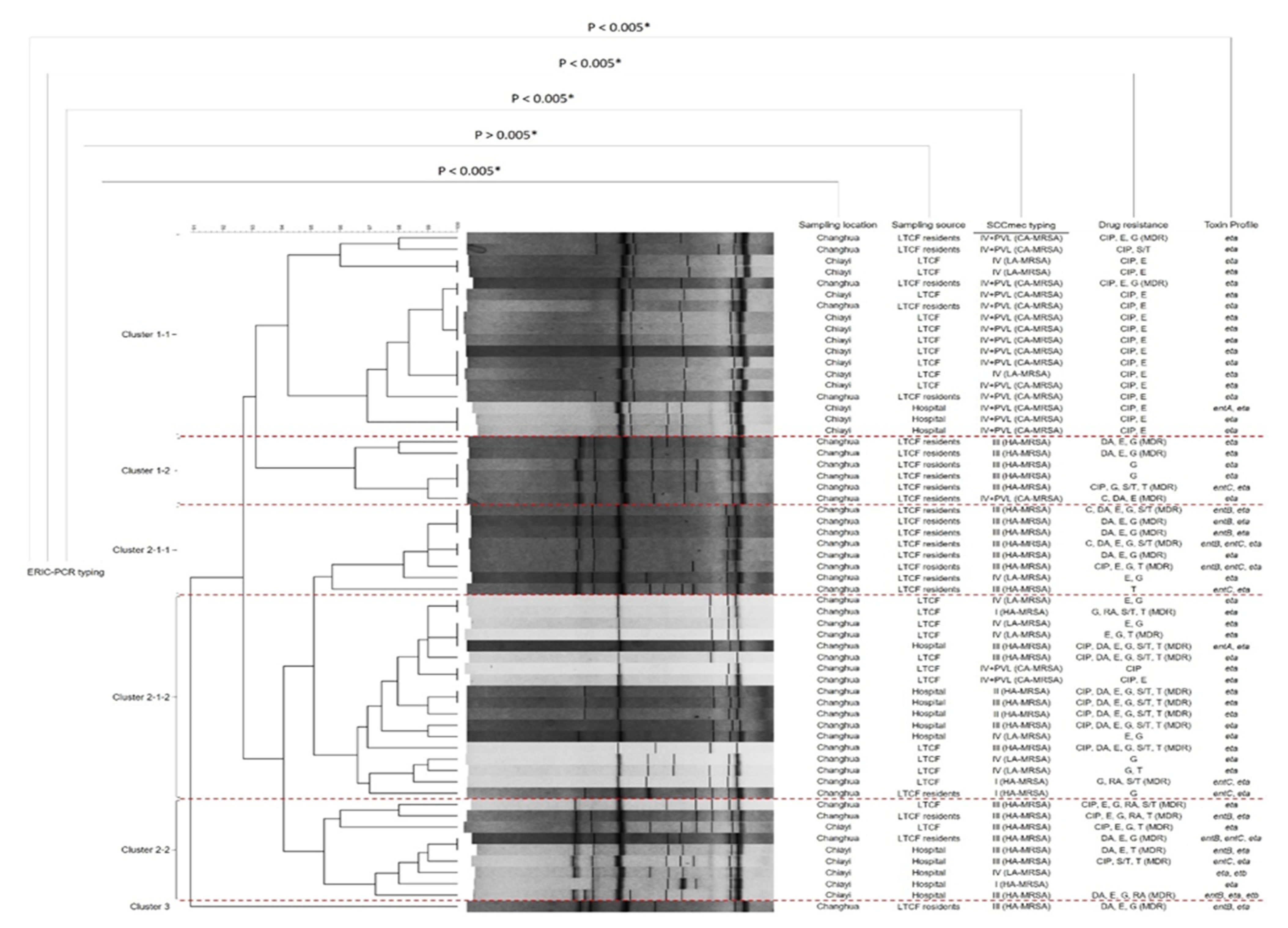
2.5. Genetic Diversity Analysis by ERIC-PCR
3. Discussion
4. Materials and Methods
4.1. Sampling Information and Collection Method
4.2. Isolation Method of MRSA
4.3. PCR Identification of MRSA Strains
4.4. Antibiotic Susceptibility Test
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bonomo, R. Multiple Antibiotic–Resistant Bacteria in Long-Term-Care Facilities: An Emerging Problem in the Practice of Infectious Diseases. Clin. Infect. Dis. 2001, 31, 1414–1422. [Google Scholar] [CrossRef] [Green Version]
- Pai, H.-H. Multidrug resistant bacteria isolated from cockroaches in long-term care facilities and nursing homes. Acta Trop. 2013, 125, 18–22. [Google Scholar] [CrossRef]
- Otto, M. MRSA virulence and spread. Cell. Microbiol. 2012, 14, 1513–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, J. Hospital-associated MRSA and antibiotic resistance—What have we learned from genomics? Int. J. Med. Microbiol. 2013, 303. [Google Scholar] [CrossRef] [PubMed]
- Ge, B.; Mukherjee, S.; Hsu, C.-H.; Davis, J.; Tran, T.; Yang, Q.; Abbott, J.; Ayers, S.; Young, S.; Crarey, E.; et al. MRSA and multidrug-resistant Staphylococcus aureus in U.S. retail meats, 2010–2011. Food Microbiol. 2017, 62, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J. Methicillin-Resistant Staphylococcus aureus in Hospitals and Long-Term Care Facilities: Microbiology, Epidemiology, and Preventive Measures. Infect. Control. Hosp. Epidemiol. 1993, 13, 725–737. [Google Scholar] [CrossRef]
- Pantosti, A.; Sanchini, A.; Monaco, M. Mechanisms of antibiotic resistance in Staphylococcus aureus. Futur. Microbiol. 2007, 2, 323–334. [Google Scholar] [CrossRef]
- Kaito, C.; Saito, Y.; Nagano, G.; Ikuo, M.; Omae, Y.; Hanada, Y.; Han, X.; Kuwahara-Arai, K.; Hishinuma, T.; Baba, T.; et al. Transcription and Translation Products of the Cytolysin Gene psm-mec on the Mobile Genetic Element SCCmec Regulate Staphylococcus aureus Virulence. PLoS Pathog. 2011, 7, e1001267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.; Mwangi, M.; Chung, M.; Milheiriço, C.; De Lencastre, H.; Tomasz, A. The Mechanism of Heterogeneous Beta-Lactam Resistance in MRSA: Key Role of the Stringent Stress Response. PLoS ONE 2014, 9. [Google Scholar] [CrossRef]
- Valsesia, G.; Rossi, M.; Bertschy, S.; Pfyffer, G.E. Emergence of SCCmecType IV and SCCmecType V Methicillin-Resistant Staphylococcus aureus Containing the Panton-Valentine Leukocidin Genes in a Large Academic Teaching Hospital in Central Switzerland: External Invaders or Persisting Circulators? J. Clin. Microbiol. 2010, 48, 720–727. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, J.; Ocampo Rios, A.; Vanegas, J.; Rodriguez, E.; Mediavilla, J.; Chen, L.; Muskus, C.; Vélez, L.; Rojas, C.; Restrepo, A.; et al. CC8 MRSA Strains Harboring SCCmec Type IVc are Predominant in Colombian Hospitals. PLoS ONE 2012, 7, e38576. [Google Scholar] [CrossRef]
- Otto, M. Community-associated MRSA: What makes them special? Int. J. Med. Microbiol. 2013, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chuang, Y.-Y.; Huang, Y.-C. Molecular epidemiology of community-associated meticillin-resistant Staphylococcus aureus in Asia. Lancet Infect. Dis. 2013, 13. [Google Scholar] [CrossRef]
- Chuang, Y.-Y.; Huang, Y.-C. Livestock-associated meticillin-resistant Staphylococcus aureus in Asia: An emerging issue? Int. J. Antimicrob. Agents 2014, 45. [Google Scholar] [CrossRef] [PubMed]
- Goudarzi, M.; Seyedjavadi, S.S.; Nasiri, M.J.; Goudarzi, H.; Nia, R.S.; Dabiri, H. Molecular characteristics of methicillin-resistant Staphylococcus aureus (MRSA) strains isolated from patients with bacteremia based on MLST, SCCmec, spa, and agr locus types analysis. Microb. Pathog. 2017, 104, 328–335. [Google Scholar] [CrossRef]
- Bush, K. Bench-to-bedside review: The role of β-lactamases in antibiotic-resistant Gram-negative infections. Crit. Care 2010, 14, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, A.; Kishony, R. Understanding, predicting and manipulating the genotypic evolution of antibiotic resistance. Nat. Rev. Genet. 2013, 14. [Google Scholar] [CrossRef] [Green Version]
- Wellington, E.M.; Boxall, A.; Cross, P.; Feil, E.; Gaze, W.H.; Hawkey, P.; Johnson-Rollings, A.; Jones, D.; Lee, N.; Otten, W.; et al. The role of the natural environment in the emergence of antibiotic resistance in Gram-negative bacteria. Lancet Infect. Dis. 2013, 13, 155–165. [Google Scholar] [CrossRef]
- Vernel-Pauillac, F.; Nandi, S.; Nicholas, R.A.; Goarant, C. Genotyping as a Tool for Antibiotic Resistance Surveillance of Neisseria gonorrhoeae in New Caledonia: Evidence of a Novel Genotype Associated with Reduced Penicillin Susceptibility. Antimicrob. Agents Chemother. 2008, 52, 3293–3300. [Google Scholar] [CrossRef] [Green Version]
- Köser, C.; Ellington, M.; Cartwright, E.; Gillespie, S.; Brown, N.; Farrington, M.; Holden, M.; Dougan, G.; Bentley, D.; Parkhill, J.; et al. Routine Use of Microbial Whole Genome Sequencing in Diagnostic and Public Health Microbiology. PLoS Pathog. 2012, 8, e1002824. [Google Scholar] [CrossRef] [Green Version]
- Ranjbar, R.; Tabatabaee, A.; Behzadi, P.; Kheiri, R. Enterobacterial Repetitive Intergenic Consensus Polymerase Chain Reaction (ERIC-PCR) Genotyping of Escherichia coli Strains Isolated from Different Animal Stool Specimens. Iran. J. Pathol. 2017, 1212, 25–34. [Google Scholar] [CrossRef]
- Leclercq, R.; Cantón, R.; Brown, D.F.J.; Giske, C.G.; Heisig, P.; MacGowan, A.; Mouton, J.; Nordmann, P.; Rodloff, A.; Rossolini, G.; et al. EUCAST expert rules in antimicrobial susceptibility testing. Clin. Microbiol. Infect. 2011, 24. [Google Scholar] [CrossRef] [Green Version]
- Hsueh, P.-R.; Chen, W.-H.; Luh, K.-T. Relationships between antimicrobial use and antimicrobial resistance in Gram-negative bacteria causing nosocomial infections from 1991–2003 at a university hospital in Taiwan. Int. J. Antimicrob. Agents 2006, 26, 463–472. [Google Scholar] [CrossRef]
- March, A.; Aschbacher, R.; Dhanji, H.; Livermore, D.; Böttcher, A.; Sleghel, F.; Maggi, S.; Noale, M.; Larcher, C.; Woodford, N. Colonization of residents and staff of a long-term-care facility and adjacent acute-care hospital geriatric unit by multiresistant bacteria. Clin. Microbiol. Infect. 2009, 16, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-L.; Ku, S.-C.; Yang, K.-Y.; Fang, W.-F.; Tu, C.-Y.; Chen, C.-W.; Hsu, K.-H.; Fan, W.-C.; Lin, M.-C.; Chen, W.; et al. Antimicrobial drug-resistant microbes associated with hospitalized community-acquired and healthcare-associated pneumonia: A multi-center study in Taiwan. J. Formos. Med. Assoc. 2013, 112, 31–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.-M.; Lai, C.-C.; Chiang, H.; Lu, M.-C.; Wang, L.-F.; Tsai, T.-L.; Kang, M.-Y.; Jan, Y.-N.; Lo, Y.-T.; Ko, W.-C.; et al. Presence of multidrug-resistant organisms in the residents and environments of long-term care facilities in Taiwan. J. Microbiol. Immunol. Infect. 2017, 50. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-Y.; Lai, C.-C.; Chiang, H.; Lu, M.-C.; Wang, L.-F.; Tsai, T.-L.; Kang, M.-Y.; Jan, Y.-N.; Lo, Y.-T.; Ko, W.-C.; et al. Predominance of methicillin-resistant Staphylococcus aureus in the residents and environments of long-term care facilities in Taiwan. J. Microbiol. Immunol. Infect. 2018, 52. [Google Scholar] [CrossRef] [PubMed]
- Phoon, H.Y.; Hussin, H.; Hussain, B.M.; Lim, S.Y.; Woon, J.J.; Er, Y.X.; Thong, K.L. Distribution, genetic diversity and antimicrobial resistance of clinically important bacteria from the environment of a tertiary hospital in Malaysia. J. Glob. Antimicrob. Resist. 2018, 14. [Google Scholar] [CrossRef] [PubMed]
- Tsai, H.-C.; Huang, T.-Y.; Chen, J.-S.; Chen, W.-J.; Lin, C.-Y.; Hsu, B.-M. Acinetobacter baumannii and methicillin-resistant Staphylococcus aureus in long-term care facilities in eastern Taiwan. Tzu. Chi. Med. J. 2019, 31. [Google Scholar] [CrossRef]
- Chen, C.-J.; Huang, Y.-C. New epidemiology of Staphylococcus aureus infection in Asia. Clin. Microbiol. Infect. 2014, 20. [Google Scholar] [CrossRef] [Green Version]
- Faires, M.; Pearl, D.; Ciccotelli, W.; Straus, K.; Zinken, G.; Berke, O.; Reid-Smith, R.; Weese, J. A prospective study to examine the epidemiology of methicillin-resistant Staphylococcus aureus and Clostridium difficile contamination in the general environment of three community hospitals in southern Ontario, Canada. BMC Infect. Dis. 2012, 12, 290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kearney, A.; Kinnevey, P.; Shore, A.; Earls, M.; Poovelikunnel, T.T.; Brennan, G.; Humphreys, H.; Coleman, D.C. The oral cavity revealed as a significant reservoir of Staphylococcus aureus in an acute hospital by extensive patient, healthcare worker and environmental sampling. J. Hosp. Infect. 2020, 105, 389–396. [Google Scholar] [CrossRef] [Green Version]
- Fooladi, A.A.I.; Ashrafi, E.; Tazandareh, S.G.; Koosha, R.Z.; Rad, H.S.; Amin, M.; Soori, M.; Larki, R.A.; Choopani, A.; Hosseini, H.M. The distribution of pathogenic and toxigenic genes among MRSA and MSSA clinical isolates. Microb. Pathog. 2015, 81. [Google Scholar] [CrossRef]
- Ludden, C.; Brennan, G.; Morris, D.; Austin, B.; O’Connell, B.; Cormican, M. Characterization of methicillin-resistant Staphylococcus aureus from residents and the environment in a long-term care facility. Epidemiol. Infect. 2015, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsao, S.-M.; Wang, W.-Y.; Ko, W.-C.; Lu, C.-T.; Liu, C.-Y.; Liao, C.-H.; Chen, Y.-S.; Liu, Y.-C.; Chen, W.-Y.; Jang, T.-N.; et al. Trend in vancomycin susceptibility and correlation with molecular characteristics of methicillin-resistant Staphylococcus aureus causing invasive infections in Taiwan: Results from the Tigecycline in vitro Surveillance in Taiwan (TIST) study, 2006–2010. Diagn. Microbiol. Infect. Dis. 2014, 80. [Google Scholar] [CrossRef]
- Jean, S.-S.; Ko, W.-C.; Hsueh, P.-R. Susceptibility of clinical isolates of meticillin-resistant Staphylococcus aureus and phenotypic non-extended-spectrum β-lactamase-producing Klebsiella pneumoniae to ceftaroline in Taiwan: Results from Antimicrobial Testing Leadership and Surveillance (ATLAS) in 2012–2018 and Surveillance of Multicentre Antimicrobial Resistance in Taiwan (SMART) in 2018–2019. Int. J. Antimicrob. Agents 2020, 56, 106016. [Google Scholar] [CrossRef]
- Tsai, H.-C.; Tao, C.-W.; Hsu, B.-M.; Yang, Y.-Y.; Tseng, Y.-C.; Huang, T.-Y.; Huang, S.-W.; Kuo, Y.-J.; Chen, J.-S. Multidrug-resistance in methicillin-resistant Staphylococcus aureus (MRSA) isolated from a subtropical river contaminated by nearby livestock industries. Ecotoxicol. Environ. Saf. 2020, 200, 110724. [Google Scholar] [CrossRef]
- De Sousa, M.A.; Crisóstomo, M.; Sanches, I.S.; Wu, J.; Fuzhong, J.; Tomasz, A.; de Lencastre, H. Frequent Recovery of a Single Clonal Type of Multidrug-Resistant Staphylococcus aureus from Patients in Two Hospitals in Taiwan and China. J. Clin. Microbiol. 2003, 41, 159–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulon, M.; Haamann, F.; Peters, C.; Schablon, A.; Nienhaus, A. MRSA prevalence in European healthcare settings: A review. BMC Infect. Dis. 2011, 11, 138. [Google Scholar] [CrossRef] [Green Version]
- Mellmann, A.; Weniger, T.; Berssenbrügge, C.; Keckevoet, U.; Friedrich, A.; Harmsen, D.; Grundmann, H. Characterization of Clonal Relatedness among the Natural Population of Staphylococcus aureus Strains by Using spa Sequence Typing and the BURP (Based upon Repeat Patterns) Algorithm. J. Clin. Microbiol. 2008, 46, 2805–2808. [Google Scholar] [CrossRef] [Green Version]
- Nubel, U.; Roumagnac, P.; Feldkamp, M.; Song, J.-H.; Ko, K.S.; Huang, Y.-C.; Coombs, G.; Ip, M.; Westh, H.; Skov, R.; et al. Frequent emergence and limited geographic dispersal of methicillin-resistant Staphylococcus aureus. Proc. Natl. Acad. Sci. USA 2008, 105, 14130–14135. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Liu, J.; Guo, Y.; Zhang, Z. Characterization of Virulence Factors and Genetic Background of Staphylococcus aureus Isolated from Peking University People’s Hospital Between 2005 and 2009. Curr. Microbiol. 2010, 61, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.-M.; Yang, M.-C.; Yang, T.-F.; Lee, P.-L.; Chien, H.-I.; Hsueh, J.-C.; Chang, S.-H.; Hsu, C.-H.; Chien, S.-T. Molecular Characterization of Community- and Healthcare-Associated Methicillin-Resistant Staphylococcus aureus Isolates in Southern Taiwan. Microb. Drug Resist. 2015, 21. [Google Scholar] [CrossRef] [PubMed]
- Candan, E.; Idil, N.; Bilkay, I.S. Usefulness of REP and ERIC-PCR combination for tracking the spread of Staphylococcus aureus strains. Minerva Biotecnol. 2013, 25, 245–250. [Google Scholar]
- Tsai, H.-C.; Chou, M.-Y.; Wu, C.-C.; Wan, M.-T.; Kuo, Y.-J.; Chen, J.-S.; Huang, T.-Y.; Hsu, B.-M. Seasonal Distribution and Genotyping of Antibiotic Resistant Strains of Listeria Innocua Isolated from A River Basin Categorized by ERIC-PCR. Int. J. Environ. Res. Public Health 2018, 15, 1559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Codjoe, F.; Brown, C.; Smith, T.; Miller, K.; Donkor, E. Genetic relatedness in carbapenem-resistant isolates from clinical specimens in Ghana using ERIC-PCR technique. PLoS ONE 2019, 14, e0222168. [Google Scholar] [CrossRef] [PubMed]
- Akindolire, A.; Kumar, A.; Ateba, N. Genetic characterization of antibiotic-resistant Staphylococcus aureus from milk in the North-West Province, South Africa. Saudi J. Biol. Sci. 2015, 25. [Google Scholar] [CrossRef] [Green Version]
- Onyango, L.A.; Dunstan, R.H.; Gottfries, J.; Von Eiff, C.; Roberts, T.K. Effect of Low Temperature on Growth and Ultra-Structure of Staphylococcus spp. PLoS ONE 2012, 7, e29031. [Google Scholar] [CrossRef] [Green Version]
- Azis, N.M.; Pung, H.P.; Rachman, A.R.A.; Nordin, S.A.; Sarchio, S.N.E.; Suhaili, Z.; Desa, M.N.M. A persistent antimicrobial resistance pattern and limited methicil-lin-resistance-associated genotype in a short-term Staphylococcus aureus carriage isolated from a student population. J. Infect. Public Health 2017, 10, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Papadopoulos, P.; Papadopoulos, T.; Angelidis, A.S.; Boukouvala, E.; Zdragas, A.; Papa, A.; Hadjichristodoulou, C.; Sergelidis, D. Prevalence of Staphylococcus aureus and of methicillin-resistant S. aureus (MRSA) along the production chain of dairy products in north-western Greece. Food Microbiol. 2018, 69, 43–50. [Google Scholar] [CrossRef]
- Halaji, M.; Karimi, A.; Shoaei, P.; Nahaei, M.; Khorvash, F.; Ataei, B.; Yaran, M.; Havaei, S.A. Distribution of SCCmec Elements and Presence of Panton-Valentine Leukocidin in Methicillin-Resistant Staphylococcus epidermidis Isolated from Clinical Samples in a University Hospital of Isfahan City, Iran. J. Clin. Diagn. Res. 2017, 11, DC27. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sampling Locations | Sampling Sources | Sample Types | Number (%) |
|---|---|---|---|
| Changhua city | LTCF environment | Moist samples (n = 45) | 10 (22.2%) |
| Arid samples (n = 24) | 0 (0%) | ||
| Total LTCF environment (n = 69) | 10 (14.5%) | ||
| LTCF dwelling medical tubes | Foley catheter-balloons from LTCF residents (n = 30) | 7 (23.3%) | |
| Nasogastric tubes from LTCF residents (n = 15) | 9 (60%) | ||
| Tracheostomy tubes from LTCF residents (n = 18) | 7 (38.9%) | ||
| Total tubes from LTCF residents (n = 63) | 23 (36.5%) | ||
| Total LTCF samples (n = 132) | 33 (25%) | ||
| Hospital environment | Moist samples (n = 20) | 6 (30%) | |
| Arid samples (n = 12) | 0 (0)% | ||
| Outpatient floor (n = 18) | 0 (0%) | ||
| Inpatient floor (n = 7) | 2 (28.6%) | ||
| Ward (used) (n = 7) | 4 (57.1%) | ||
| Total hospital samples (n = 32) | 6 (18.8%) | ||
| Total Changhua city samples (n = 164) | 39 (23.8%) | ||
| Chiayi city | LTCF environment | Mild area (n = 26) | 3 (11.5%) |
| Severe area (n = 24) | 8 (33.3%) | ||
| Moist samples (n = 38) | 7 (18.4%) | ||
| Arid samples (n = 12) | 4 (33.3%) | ||
| Total LTCF samples (n = 50) | 11 (22%) | ||
| Hospital environment | Outpatient building 1F (n = 7) | 1 (14.3%) | |
| Inpatient building 1F (n = 6) | 3 (50%) | ||
| Total building 1F (n = 13) | 4 (30.8%) | ||
| Ward (vacancy) (n = 9) | 1 (11.1%) | ||
| Ward (used) (n = 10) | 3 (30%) | ||
| Total wards (n = 19) | 4 (21.1%) | ||
| Moist samples (n = 16) | 5 (31.3%) | ||
| Arid samples (n = 16) | 3 (18.8%) | ||
| Total hospital samples (n = 32) | 8 (25%) | ||
| Total Chiayi city samples (n = 82) | 19 (23.2%) | ||
| Total Changhua city and Chiayi city samples (n = 246) | 58 (23.6%) | ||
| Sampling Locations | Sampling Sources | SCCmec I | SCCmec II | SCCmec III | SCCmec IV | SCCmec V | PVL | HA-MRSA (I, II, III) | CA-MRSA (IV+PVL, V+PVL) | LA-MRSA (IV, V) |
|---|---|---|---|---|---|---|---|---|---|---|
| Changhua City | LTCF environment (n = 12) | 2 (16.7%) | 0 (0%) | 3 (25%) | 7 (58.3%) | 0 (0%) | 2 (16.7%) | 5 (41.7%) | 2 (16.7%) | 5 (41.7%) |
| Tubes from LTCF residents (n = 23) | 1 (4.3%) | 0 (0%) | 15 (65.2%) | 7 (30.4%) | 0 (0%) | 9 (39.1%) | 16 (69.6%) | 6 (26.1%) | 1 (4.3%) | |
| Total LTCF isolates (n = 35) | 3 (8.6%) | 0 (0%) | 18 (51.4%) | 14 (40%) | 0 (0%) | 11 (31.4%) | 21 (60%) | 8 (22.9%) | 6 (17.1%) | |
| Hospital environment (n = 6) | 0 (0%) | 2 (33.3%) | 3 (50%) | 1 (16.7%) | 0 (0%) | 0 (0%) | 5 (83.3%) | 0 (0%) | 1 (16.7%) | |
| Total Changhua city isolates (n = 41) | 3 (7.3%) | 2 (4.9%) | 21 (51.2%) | 15 (36.6%) | 0 (0%) | 11 (26.8%) | 26 (63.4%) | 8 (19.5%) | 7 (17.1%) | |
| Chiayi City | LTCF environment (n = 11) | 0 (0%) | 0 (0%) | 1 (9.1%) | 10 (90.9%) | 0 (0%) | 7 (63.6%) | 1 (9.1%) | 7 (63.6%) | 3 (27.3%) |
| Hospital environment (n = 8) | 1 (12.5%) | 0 (0%) | 3 (37.5%) | 4 (50%) | 0 (0%) | 6 (75%) | 4 (50%) | 3 (37.5%) | 1 (12.5%) | |
| Total Chiayi city isolates (n = 19) | 1 (5.3%) | 0 (0%) | 4 (21.1%) | 14 (73.7%) | 0 (0%) | 13 (68.4%) | 5 (26.3%) | 10 (52.6%) | 4 (21.1%) | |
| Total Changhua City and Chiayi city isolates (n = 60) | 4 (6.7%) | 2 (3.3%) | 25 (41.7%) | 29 (48.3%) | 0 (0%) | 24 (40%) | 31 (51.7%) | 18 (30%) | 11 (18.3%) | |
| Sampling Locations | Sampling Sources | entA | entB | entC | entD | entE | Eta | etb | tsst-1 |
|---|---|---|---|---|---|---|---|---|---|
| Changhua city | LTCF environment (n = 12) | 0 (0%) | 0 (0%) | 1 (8.3%) | 0 (0%) | 0 (0%) | 12 (100%) | 0 (0%) | 0 (0%) |
| Tubes from LTCF residents (n = 23) | 0 (0%) | 8 (34.8%) | 6 (26.1%) | 0 (0%) | 0 (0%) | 23 (100%) | 0 (0%) | 0 (0%) | |
| Total LTCF isolates (n = 35) | 0 (0%) | 8 (22.9%) | 7 (20%) | 0 (0%) | 0 (0%) | 35 (100%) | 0 (0%) | 0 (0%) | |
| Hospital environment (n = 6) | 1 (16.7%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 6 (100%) | 0 (0%) | 0 (0%) | |
| Total Changhua City isolates (n = 41) | 1 (2.4%) | 8 (19.5%) | 7 (17.1%) | 0 (0%) | 0 (0%) | 41 (100%) | 0 (0%) | 0 (0%) | |
| Chiayi city | LTCF environment (n = 11) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 11 (100%) | 0 (0%) | 0 (0%) |
| Hospital environment (n = 8) | 1 (12.5%) | 2 (25%) | 1 (12.5%) | 0 (0%) | 0 (0%) | 8 (100%) | 2 (25%) | 0 (0%) | |
| Total Chiayi City isolates (n = 19) | 1 (5.3%) | 2 (10.5%) | 1 (5.3%) | 0 (0%) | 0 (0%) | 19 (100%) | 2 (10.5%) | 0 (0%) | |
| Total Changhua city and Chiayi city isolates (n = 60) | 2 (3.3%) | 10 (16.7%) | 8 (13.3%) | 0 (0%) | 0 (0%) | 60 (100%) | 2 (3.3%) | 0 (0%) | |
| Sampling Locations | Sampling Sources | C | CIP | DA | E | G | RA | S/T | T | MDR |
|---|---|---|---|---|---|---|---|---|---|---|
| Changhua city | LTCF environment (n = 12) | 0 (0%) | 5 (41.7%) | 2 (16.7%) | 7 (58.3%) | 10 (83.3%) | 3 (25%) | 5 (41.7%) | 5 (41.7%) | 6 (50%) |
| tubes from LTCF residents (n = 23) | 3 (13.3%) | 8 (34.8%) | 10 (43.5%) | 17 (73.9%) | 18 (78.3%) | 1 (4.3%) | 4 (17.4%) | 4 (17.4%) | 15 (65.2%) | |
| LTCF isolates (n = 35) | 3 (8.6%) | 13 (37.1%) | 12 (34.3%) | 24 (68.6%) | 28 (80%) | 4 (11.4%) | 9 (25.7%) | 9 (25.7%) | 21 (60%) | |
| Hospital environment (n = 6) | 0 (0%) | 5 (83.3%) | 5 (83.3%) | 6 (100%) | 6 (100%) | 0 (0%) | 5 (83.3%) | 5 (83.3%) | 5 (83.3%) | |
| Total Changhua city isolates (n = 41) | 3 (7.3%) | 18 (43.9%) | 17 (41.5%) | 30 (73.2%) | 34 (82.9%) | 4 (9.8%) | 14 (34.1%) | 14 (34.1%) | 26 (63.4%) | |
| Chiayi city | LTCF environment (n = 11) | 0 (0%) | 11 (100%) | 0 (0%) | 11 (100%) | 1 (9.1%) | 0 (0%) | 0 (0%) | 1 (9.1%) | 1 (9.1%) |
| Hospital environment (n = 8) | 0 (0%) | 4 (50%) | 2 (25%) | 5 (62.5%) | 1 (12.5%) | 1 (12.5%) | 1 (12.5%) | 2 (25%) | 3 (37.5%) | |
| Total Chiayi city isolates (n = 19) | 0 (0%) | 15 (78.9%) | 2 (10.5%) | 16 (84.2%) | 2 (10.5%) | 1 (5.3%) | 1 (5.3%) | 3 (15.8%) | 4 (21.1%) | |
| Total Changhua city and Chiayi city isolates (n = 60) | 3 (5%) | 33 (55%) | 19 (31.7%) | 46 (76.7%) | 36 (60%) | 5 (8.3%) | 15 (25%) | 17 (28.3%) | 30 (50%) | |
| Sampling Locations | Changhua City | Chiayi City | Total MDR Strains | |||
|---|---|---|---|---|---|---|
| Sampling Sources | LTCF Environment | Tubes from LTCF Residents | Hospital Environment | LTCF Environment | Hospital Environment | |
| CIP-DA-E-G-S/T-T (6 drugs) | 2 | 5 | 7 | |||
| C-DA-E-G-S/T (5 drugs) | 2 | 4 | ||||
| CIP-E-G-RA-S/T (5 drugs) | 1 | |||||
| CIP-E-G-RA-T (5 drugs) | 1 | |||||
| CIP-E-G-S/T (4 drugs) | 1 | 5 | ||||
| CIP-E-G-T (4 drugs) | 1 | |||||
| CIP-G-S/T-T (4 drugs) | 1 | |||||
| DA-E-G-RA (4 drugs) | 1 | |||||
| G-RA-S/T-T (4 drugs) | 1 | |||||
| C-DA-E (3 drugs) | 1 | 14 | ||||
| CIP-E-G (3 drugs) | 2 | |||||
| CIP-ST-T (3 drugs) | 1 | |||||
| DA-E-G (3 drugs) | 7 | |||||
| DA-E-T (3 drugs) | 1 | |||||
| E-G-T (3 drugs) | 1 | |||||
| G-RA-S/T (3 drugs) | 1 | |||||
| Total strains | 6 | 15 | 5 | 1 | 3 | 30 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, B.-M.; Chen, J.-S.; Lin, I.-C.; Hsu, G.-J.; Koner, S.; Hussain, B.; Huang, S.-W.; Tsai, H.-C. Molecular and Anti-Microbial Resistance (AMR) Profiling of Methicillin-Resistant Staphylococcus aureus (MRSA) from Hospital and Long-Term Care Facilities (LTCF) Environment. Antibiotics 2021, 10, 748. https://doi.org/10.3390/antibiotics10060748
Hsu B-M, Chen J-S, Lin I-C, Hsu G-J, Koner S, Hussain B, Huang S-W, Tsai H-C. Molecular and Anti-Microbial Resistance (AMR) Profiling of Methicillin-Resistant Staphylococcus aureus (MRSA) from Hospital and Long-Term Care Facilities (LTCF) Environment. Antibiotics. 2021; 10(6):748. https://doi.org/10.3390/antibiotics10060748
Chicago/Turabian StyleHsu, Bing-Mu, Jung-Sheng Chen, I-Ching Lin, Gwo-Jong Hsu, Suprokash Koner, Bashir Hussain, Shih-Wei Huang, and Hsin-Chi Tsai. 2021. "Molecular and Anti-Microbial Resistance (AMR) Profiling of Methicillin-Resistant Staphylococcus aureus (MRSA) from Hospital and Long-Term Care Facilities (LTCF) Environment" Antibiotics 10, no. 6: 748. https://doi.org/10.3390/antibiotics10060748
APA StyleHsu, B.-M., Chen, J.-S., Lin, I.-C., Hsu, G.-J., Koner, S., Hussain, B., Huang, S.-W., & Tsai, H.-C. (2021). Molecular and Anti-Microbial Resistance (AMR) Profiling of Methicillin-Resistant Staphylococcus aureus (MRSA) from Hospital and Long-Term Care Facilities (LTCF) Environment. Antibiotics, 10(6), 748. https://doi.org/10.3390/antibiotics10060748