
Fecal Carriage and Epidemiology of Extended-Spectrum Beta-Lactamase/Carbapenemases Producing Enterobacterales Isolates in Bulgarian Hospitals

 , and
, and 
Abstract
1. Introduction
2. Material and Methods
2.1. Bacterial Isolates
2.2. Phenotypic ESBL and Carbapenemases Detection
2.3. Molecular-Genetic Beta-Lactamase Identification
2.4. Conjugation Experiments and Replicon Typing
2.5. ERIC and MLST Typing
3. Results
3.1. Bacterial Isolates
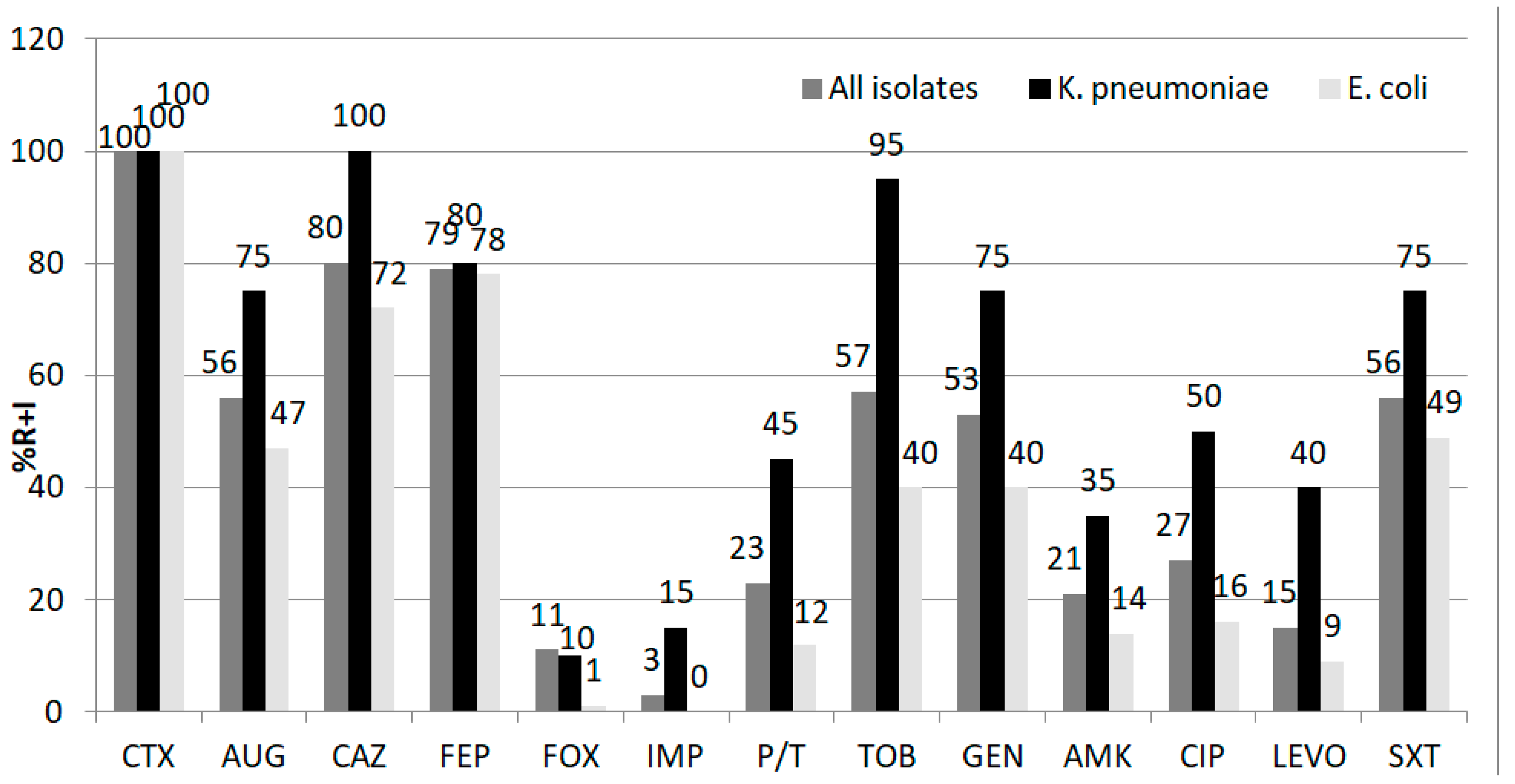
3.2. Antimicrobial Susceptibility Testing
3.3. Phenotypic ESBL and Carbapenemases Detection
3.4. Molecular-Genetic Beta-Lactamase Identification
3.5. Isoelectric Focusing and Bioassay
3.6. Conjugation Experiments and Replicon Typing
3.7. MLST and ERIC Typing
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Davin-Regli, A.; Lavigne, J.P.; Pagès, J.M. Enterobacter spp.: Update on Taxonomy, Clinical Aspects, and Emerging Antimicrobial Resistance. Clin. Microbiol. Rev. 2019, 32, e00002-19. [Google Scholar] [CrossRef]
- Bush, K.; Patricia, A. Bradford Epidemiology of β-Lactamase-Producing Pathogens. Clin. Microbiol. Rev. 2020, 33, e00047-19. [Google Scholar] [CrossRef]
- Wyres, K.L.; Lam, M.M.C.; Holt, K.E. Population genomics of Klebsiella pneumoniae. Nat. Rev. Microbiol. 2020, 18, 344–359. [Google Scholar] [CrossRef]
- Peirano, G.; Pitout, J. Extended-Spectrum β-Lactamase-Producing Enterobacteriaceae: Update on Molecular Epidemiology and Treatment Options. Drugs 2019, 79, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
- Bonomo, R.A. β-Lactamases: A Focus on Current Challenges. Cold Spring Harb. Perspect. Med. 2017, 7, a025239. [Google Scholar] [CrossRef] [PubMed]
- Nordmann, P.; Poirel, L. Epidemiology and Diagnostics of Carbapenem Resistance in Gram-negative Bacteria. Clin. Infect. Dis. 2019, 69 (Suppl. 7), S521–S528. [Google Scholar] [CrossRef] [PubMed]
- Partridge, S.R.; Kwong, S.M.; Firth, N.; Jensen, S.O. Mobile Genetic Elements Associated with Antimicrobial Resistance. Clin. Microbiol. Rev. 2018, 31, e00088-17. [Google Scholar] [CrossRef] [PubMed]
- Woerther, P.L.; Burdet, C.; Chachaty, E.; Andremont, A. Trends in human fecal carriage of extended-spectrum β-lactamases in the community: Toward the globalization of CTX-M. Clin. Microbiol. Rev. 2013, 26, 744–758. [Google Scholar] [CrossRef] [PubMed]
- Thaden, J.T.; Fowler, V.G.; Sexton, D.J.; Anderson, D.J. Increasing Incidence of Extended-Spectrum β-Lactamase-Producing Escherichia coli in Community Hospitals throughout the Southeastern United States. Infect. Control Hosp. Epidemiol. 2016, 37, 49–54. [Google Scholar] [CrossRef]
- Karanika, S.; Karantanos, T.; Arvanitis, M.; Grigoras, C.; Mylonakis, E. Fecal Colonization With Extended-spectrum Beta-lactamase-Producing Enterobacteriaceae and Risk Factors among Healthy Individuals: A Systematic Review and Metaanalysis. Clin. Infect. Dis. 2016, 63, 310–318. [Google Scholar] [CrossRef]
- Jolivet, S.; Vaillant, L.; Poncin, T.; Lolom, I.; Gaudonnet, Y.; Rondinaud, E.; Bendjelloul, G.; Lomont, A.; Lucet, J.C.; Armand-Lefèvre, L. Prevalence of carriage of extended-spectrum β-lactamase-producing enterobacteria and associated factors in a French hospital. Clin. Microbiol. Infect. 2018, 24, 1311–1314. [Google Scholar] [CrossRef]
- Jarlier, V.; Nicolas, M.H.; Fournier, G.; Philippon, A. Extended broad-spectrum beta-lactamases conferring transferable resistance to newer beta-lactam agents in Enterobacteriaceae: Hospital prevalence and susceptibility patterns. Rev. Infect. Dis. 1988, 10, 867–878. [Google Scholar] [CrossRef]
- Markovska, R.; Stoeva, T.; Schneider, I.; Boyanova, L.; Popova, V.; Dacheva, D.; Kaneva, R.; Bauernfeind, A.; Mitev, V.; Mitov, I. Clonal dissemination of multilocus sequence type ST15 KPC-2-producing Klebsiella pneumoniae in Bulgaria. APMIS 2015, 123, 887–894. [Google Scholar] [CrossRef]
- Poirel, L.; Walsh, T.R.; Cuvillier, V.; Nordmann, P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 2011, 70, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Rasheed, J.K.; Kitchel, B.; Zhu, W.; Anderson, K.F.; Clark, N.C.; Ferraro, M.J.; Savard, P.; Humphries, R.M.; Kallen, A.J.; Limbago, B.M. New Delhi metallo-β-lactamase-producing Enterobacteriaceae, United States. Emerg. Infect. Dis. 2013, 19, 870–878. [Google Scholar] [CrossRef] [PubMed]
- Carattoli, A.; Bertini, A.; Villa, L.; Falbo, V.; Hopkins, K.L.; Threlfall, E.J. Identification of plasmids by PCR-based replicon typing. J. Microbiol. Methods 2005, 63, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Clermont, O.; Bonacorsi, S.; Bingen, E. Rapid and simple detection of the Escherichia coli phylogenetic group. Appl. Environ. Microbiol. 2000, 66, 4555–4558. [Google Scholar] [CrossRef] [PubMed]
- Wirth, T.; Falush, D.; Lan, R.; Colles, F.; Mensa, P.; Wieler, L.H.; Karch, H.; Reeves, P.R.; Maiden, M.C.; Ochman, H.; et al. Sex and virulence in Escherichia coli: An evolutionary perspective. Mol. Microbiol. 2006, 60, 1136–1151. [Google Scholar] [CrossRef]
- Clermont, O.; Dhanji, H.; Upton, M.; Gibreel, T.; Fox, A.; Boyd, D.; Mulvey, M.R.; Nordmann, P.; Ruppé, E.; Sarthou, J.L.; et al. Rapid detection of the O25b-ST131 clone of Escherichia coli encompassing the CTX-M-15-producing strains. J. Antimicrob. Chemother. 2009, 64, 274–277. [Google Scholar] [CrossRef]
- Aires-de-Sousa, M.; Lopes, E.; Gonçalves, M.L.; Pereira, A.L.; Machado E Costa, A.; de Lencastre, H.; Poirel, L. Intestinal carriage of extended-spectrum beta-lactamase-producing Enterobacteriaceae at admission in a Portuguese hospital. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 783–790. [Google Scholar] [CrossRef]
- Pilmis, B.; Cattoir, V.; Lecointe, D.; Limelette, A.; Grall, I.; Mizrahi, A.; Marcade, G.; Poilane, I.; Guillard, T.; Bourgeois Nicolaos, N.; et al. Carriage of ESBL-producing Enterobacteriaceae in French hospitals: The PORTABLSE study. J. Hosp. Infect. 2018, 98, 247–252. [Google Scholar] [CrossRef]
- Schoevaerdts, D.; Verroken, A.; Huang, T.D.; Frennet, M.; Berhin, C.; Jamart, J.; Bogaerts, P.; Swine, C.; Glupczynski, Y. Multidrug-resistant bacteria colonization amongst patients newly admitted to a geriatric unit: A prospective cohort study. J. Infect. 2012, 65, 109–118. [Google Scholar] [CrossRef]
- Otter, J.A.; Natale, A.; Batra, R.; Tosas Auguet, O.; Dyakova, E.; Goldenberg, S.D.; Edgeworth, J.D. Individual- and community-level risk factors for ESBL Enterobacteriaceae colonization identified by universal admission screening in London. Clin. Microbiol. Infect. 2019, 25, 1259–1265. [Google Scholar] [CrossRef]
- Díaz-Agero Pérez, C.; López-Fresneña, N.; Rincon Carlavilla, A.L.; Hernandez Garcia, M.; Ruiz-Garbajosa, P.; Aranaz-Andrés, J.M.; Maechler, F.; Gastmeier, P.; Bonten, M.J.M.; Canton, R. Local prevalence of extended-spectrum beta-lactamase (ESBL) producing Enterobacteriaceae intestinal carriers at admission and co-expression of ESBL and OXA-48 carbapenemase in Klebsiella pneumoniae: A prevalence survey in a Spanish University Hospital. BMJ Open 2019, 9, e024879. [Google Scholar] [CrossRef] [PubMed]
- Platteel, T.N.; Leverstein-van Hall, M.A.; Cohen Stuart, J.W.; Thijsen, S.F.; Mascini, E.M.; van Hees, B.C.; Scharringa, J.; Fluit, A.C.; Bonten, M.J. Predicting carriage with extended-spectrum beta-lactamase-producing bacteria at hospital admission: A cross-sectional study. Clin. Microbiol. Infect. 2015, 21, 141–146. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Titelman, E.; Hasan, C.M.; Iversen, A.; Naucler, P.; Kais, M.; Kalin, M.; Giske, C.G. Faecal carriage of extended-spec-trum beta-lactamase-producing Enterobacteriaceae is common 12 months after infection and is related to strain factors. Clin. Microbiol. Infect. 2014, 20, O508–O515. [Google Scholar] [CrossRef] [PubMed]
- Markovska, R.; Schneider, I.; Ivanova, D.; Mitov, I.; Bauernfeind, A. Predominance of IncL/M and IncF plasmid types among CTX-M-ESBL-producing Escherichia coli and Klebsiella pneumoniae in Bulgarian hospitals. APMIS 2014, 122, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, F.S.; Assous, M.V.; Bdolah-Abram, T.; Lachish, T.; Yinnon, A.M.; Wiener-Well, Y. Duration of carriage of carbapenem-resistant Enterobacteriaceae following hospital discharge. Am. J. Infect. Control 2013, 41, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Machado, E.; Ramos, H.; Peixe, L.; Novais, Â. Expansion of ESBL-producing Klebsiella pneumoniae in hospitalized patients: A successful story of international clones (ST15, ST147, ST336) and epidemic plasmids (IncR, IncFIIK). Int. J. Med. Microbiol. 2014, 304, 1100–1108. [Google Scholar] [CrossRef]
- Wang, J.T.; Wu, U.I.; Lauderdale, T.L.; Chen, M.C.; Li, S.Y.; Hsu, L.Y.; Chang, S.C. Carbapenem-nonsusceptible Enterobacteriaceae in Taiwan. PLoS ONE 2015, 10, e0121668. [Google Scholar] [CrossRef] [PubMed]
- Esteban-Cantos, A.; Aracil, B.; Bautista, V.; Ortega, A.; Lara, N.; Saez, D.; Fernández-Romero, S.; Pérez-Vázquez, M.; Navarro, F.; Grundmann, H.; et al. The Carbapenemase-Producing Klebsiella pneumoniae Population Is Distinct and More Clonal than the Carbapenem-Susceptible Population. Antimicrob. Agents Chemother. 2017, 61, e02520-16. [Google Scholar] [CrossRef] [PubMed]
- Ríos, E.; López, M.C.; Rodríguez-Avial, I.; Culebras, E.; Picazo, J.J. Detection of Escherichia coli ST131 clonal complex (ST705) and Klebsiella pneumoniae ST15 among faecal carriage of extended-spectrum β-lactamase- and carbapenemase-producing Enterobacteriaceae. J. Med. Microbiol. 2017, 66, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Markovska, R.; Stoeva, T.; Boyanova, L.; Stankova, P.; Schneider, I.; Keuleyan, E.; Mihova, K.; Murdjeva, M.; Sredkova, M.; Lesseva, M.; et al. Multicentre investigation of carbapenemase-producing Klebsiella pneumoniae and Escherichia coli in Bulgarian hospitals—Interregional spread of ST11 NDM-1-producing K. pneumoniae. Infect. Genet. Evol. 2019, 69, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Markovska, R.; Stoeva, T.; Boyanova, L.; Stankova, P.; Pencheva, D.; Keuleyan, E.; Murjeva, M.; Sredkova, M.; Ivanova, D.; Lazarova, G.; et al. Dissemination of successful international clone ST15 and clonal complex 17 among Bulgarian CTX-M-15 producing K. pneumoniae isolates. Diagn. Microbiol. Infect. Dis. 2017, 89, 310–313. [Google Scholar] [CrossRef]
- Banerjee, R.; Johnston, B.; Lohse, C.; Porter, S.B.; Clabots, C.; Johnson, J.R. Escherichia coli sequence type 131 is a dominant, antimicrobial-resistant clonal group associated with healthcare and elderly hosts. Infect. Control Hosp. Epidemiol. 2013, 34, 361–369. [Google Scholar] [CrossRef]
- Mathers, A.J.; Peirano, G.; Pitout, J.D. The role of epidemic resistance plasmids and international high-risk clones in the spread of multidrug-resistant Enterobacteriaceae. Clin. Microbiol. Rev. 2015, 28, 565–591. [Google Scholar] [CrossRef] [PubMed]
- Hilty, M.; Betsch, B.Y.; Bogli-Stuber, K.; Heiniger, N.; Stadler, M.; Kuffer, M.; Kronenberg, A.; Rohrer, C.; Aebi, S.; Endimiani, A.; et al. Transmission dynamics of extended-spectrum ß-lactamase-producing Enterobacteriaceae in the tertiary care hospital and the household setting. Clin. Infect. Dis. 2012, 55, 967–975. [Google Scholar] [CrossRef]
- Rogers, B.A.; Sidjabat, H.E.; Paterson, D.L. Escherichia coli O25b-ST131: A pandemic, multiresistant, community-associated strain. J. Antimicrob. Chemother. 2011, 66, 1–14. [Google Scholar] [CrossRef]
- Overdevest, I.; Haverkate, M.; Veenemans, J.; Hendriks, Y.; Verhulst, C.; Mulders, A.; Couprie, W.; Bootsma, M.; Johnson, J.; Kluytmans, J. Prolonged colonisation with Escherichia coli O25:ST131 versus other extended-spectrum beta-lactamase-producing E. coli in a long-term care facility with high endemic level of rectal colonisation, the Netherlands, 2013 to 2014. Euro Surveill. 2016, 21, 30376. [Google Scholar] [CrossRef]
- Doumith, M.; Day, M.; Ciesielczuk, H.; Hope, R.; Underwood, A.; Reynolds, R.; Wain, J.; Livermore, D.; Woodford, N. Rapid identification of major Escherichia coli sequence types causing urinary tract and bloodstream infections. J. Clin. Microbiol. 2015, 53, 160–166. [Google Scholar] [CrossRef]
- Hertz, F.; Nielsen, J.; Schønning, K.; Littauer, P.; Knudsen, J.; Løbner-Olesen, A.; Frimodt-Møller, N. Population structure of drug-susceptible,-resistant and ESBL-producing Escherichia coli from community-acquired urinary tract. BMC Microbiol. 2016, 16, 63. [Google Scholar]
- Poirel, L.; Savov, E.; Nazli, A.; Trifonova, A.; Todorova, I.; Gergova, I.; Nordmann, P. Outbreak caused by NDM-1- and RmtB-producing Escherichia coli in Bulgaria. Antimicrob. Agents Chemother. 2014, 58, 2472–2474. [Google Scholar] [CrossRef] [PubMed]
- Roy Chowdhury, P.; McKinnon, J.; Liu, M.; Djordjevic, S.P. Multidrug Resistant Uropathogenic Escherichia coli ST405 With a Novel, Composite IS26 Transposon in a Unique Chromosomal Location. Front. Microbiol. 2019, 9, 3212. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| ESBL. Species | CTX-M-3 Number H/PA | CTX-M-15 Number H/PA | KPC-2 + CTX-M-15 Number H/PA | CTX-M-14 Number H/PA | CTX-M-1 Number H/PA | SHV-12 Number H/PA |
|---|---|---|---|---|---|---|
| K. pneumoniae n = 20 | 4/2 | 11/0 | 3/0 | |||
| E. coli n = 68 | 9/18 | 6/22 | 0/1 | 8/3 | 0/1 | |
| E. cloacae complex n = 5. | 1/0 | 2/1. | ||||
| K. aerogenes n = 2 | 2/0 | |||||
| C. freundii n = 1 | 1/0 | |||||
| S. sonnei n = 2 | 0/2 | |||||
| Total n = 98 | 16/22 | 20/23 | 3/0 | 0/1 | 8/3 | 1/1 |
| Patients, Type | ESBL | MLST Types | Phenotype of Transconjugants | Replicon Type |
|---|---|---|---|---|
| Hospitalized (14) | CTX-M-3 (4) | ST17(4) | CTX,TOB.GEN.AMI,SXT(2) | L/M(2) |
| CTX-M-15 (7) | ST15(5) * | - | ||
| ST340(1) ST16(1) | - | |||
| KPC-2+CTX-M-15 (3) | ST15(3) | IMP,MER,PIP/TAZ (2) | FIA,FIIAs (2) | |
| At admission (6) | CTX-M-3 (2) | ST37(2) | CTX, GEN (2) | L/M(2) |
| CTX-M-15 (4) | ST215(1) ST359(1) ST873(2) | CTX,CAZ,TOB,GEN,TET CTX,CAZ,TOB,GEN,CIP - | F (1) NT (1) |
| ESBL | ERIC | MLST | Phylogroup | Phenotype of Transconjugants | Replicon Type | |
|---|---|---|---|---|---|---|
| Isolates from HP n = 23 | CTX-M-3 n = 9 | f(5) | ST131 * | A | CTX (2) | I1(2) |
| b(1) | ST 38 | D | CTX (1) | I1(1) | ||
| uni(3) | ND | A | CTX,TOB,GEN,AMI.SXT(1) CTX, SXT (1) | L/M(1) I1(1) | ||
| CTX-M-14 n = 8 | c(2) | ST 43 | A | - | ||
| a(4) | ST 95 | B2 | CTX(2) | F(2) | ||
| b(2) | ST 38 | D | - | |||
| CTX-M-15 n = 6 | f(3) | ST131 | B2 | CTX,CAZ,TOB,GEN,TET(2) | FIA,F(2) | |
| d(2) | ST405 | D | CTX,CAZ,TOB,TET,SXT(1) | FIA,F(1) | ||
| l(1) | ST316 | A | - | |||
| Isoaltes from PA n = 45 | SHV-12 n = 1 | f(1) | ST131 | B2 | - | |
| CTX-M-1 n = 1 | f(1) | ST131 | B2 | - | ||
| CTX-M-3 n = 18 | f(5) ** | ST131 | B2 | CTX(2) CTX,TOB,GEN,AMI(1) CTX,TOB,GEN,SXT,CHL(1) | I1(2) L/M(1) FIIAs(1) | |
| l(3) | ST316 | A | CTX(1) | I1(1) | ||
| b(2) | ST 38 | D | CTX(1) | I1(1) | ||
| m(2) | ST676 | B2 | CTX,GEN(1) | L/M(1) | ||
| a(1) | ST 95 | B2 | CTX(1) | I1(1) | ||
| t(3) | ST 517 | B1 | CTX,GEN(1) | L/M(1) | ||
| uni(2) | ND | A(2) | CTX(2) | I1(2) | ||
| CTX-M-14 n = 3 | a(1) | ST 95 | B2 | CTX(1) | F(1) | |
| f(1) | ST131 | B2 | CTX(1) | F(1) | ||
| m(1) | ST676 | B2 | ||||
| CTX-M-15 n = 22 | f(5) | ST131 | B2 | |||
| l(3) | ST316 | A | CTX,CAZ(2) CTX,CAZ,SXT(1) | F(3) | ||
| a(1) | ST 95 | B2 | ||||
| m(2) | ST676 | B2 | CTX,CAZ(1) | F(1) | ||
| n(2) | ST540 | A | CTX,CAZ(1) | NT(1) | ||
| b(3) | ST38 | D | CTX,CAZ(1) | NT(1) | ||
| uni (6) | ND | A(5),B1(1) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Markovska, R.; Stankova, P.; Stoeva, T.; Ivanova, D.; Pencheva, D.; Kaneva, R.; Boyanova, L. Fecal Carriage and Epidemiology of Extended-Spectrum Beta-Lactamase/Carbapenemases Producing Enterobacterales Isolates in Bulgarian Hospitals. Antibiotics 2021, 10, 747. https://doi.org/10.3390/antibiotics10060747
Markovska R, Stankova P, Stoeva T, Ivanova D, Pencheva D, Kaneva R, Boyanova L. Fecal Carriage and Epidemiology of Extended-Spectrum Beta-Lactamase/Carbapenemases Producing Enterobacterales Isolates in Bulgarian Hospitals. Antibiotics. 2021; 10(6):747. https://doi.org/10.3390/antibiotics10060747
Chicago/Turabian StyleMarkovska, Rumyana, Petya Stankova, Temenuga Stoeva, Dobrinka Ivanova, Daniela Pencheva, Radka Kaneva, and Lyudmila Boyanova. 2021. "Fecal Carriage and Epidemiology of Extended-Spectrum Beta-Lactamase/Carbapenemases Producing Enterobacterales Isolates in Bulgarian Hospitals" Antibiotics 10, no. 6: 747. https://doi.org/10.3390/antibiotics10060747
APA StyleMarkovska, R., Stankova, P., Stoeva, T., Ivanova, D., Pencheva, D., Kaneva, R., & Boyanova, L. (2021). Fecal Carriage and Epidemiology of Extended-Spectrum Beta-Lactamase/Carbapenemases Producing Enterobacterales Isolates in Bulgarian Hospitals. Antibiotics, 10(6), 747. https://doi.org/10.3390/antibiotics10060747