1. Introduction
Open fractures of the lower extremity are common injuries after high-energy trauma. They require urgent surgeries of Altemeier contamination class 3 or 4 depending on the time to surgery. Altemeier contamination classes 3 and 4 correspond to contaminated and septic surgeries, respectively [
1]. Gustilo, in his study, identified the association between certain types of open fractures and the frequency of surgical site infections involving different pathogens [
2]. The Gustilo–Anderson classification of open fractures was used to guide prophylactic and preemptive antibiotic therapy. Infectious complications following open fractures are a common issue, with rates ranging from <1% for grade I open fractures to 30% for grade III fractures [
3,
4,
5,
6].
The severity of infection, Gustilo classification, smoking, diabetes, time to antibiotic therapy initiation, and shorter duration of antibiotic prophylaxis have been identified as risk factors for the occurrence of postoperative infections [
4,
7].
Antibiotic prophylaxis for surgery has proven to be effective in reducing surgical site infections [
4,
8]. Recommendations on this subject are regularly updated to adjust for new specificities of management and the evolution of bacterial resistance.
According to the French recommendations of the Société Française d’Anesthésie Réanimation (SFAR) [
1], antibiotic prophylaxis for open Cauchoix fractures stage II and III, corresponding, respectively, to an open fracture with a skin lesion that presents a high risk of secondary necrosis after suturing and an open fracture with non-suturable skin loss opposite or near the fracture site, regardless of the equipment used, is based on the administration of the amoxicillin/clavulanic acid combination. Clindamycin and gentamicin should be initiated as soon as possible in the case of true allergy to penicillin. The English recommendations are similar to the French recommendations, with the use of either amoxicillin/clavulanic acid or cefuroxime [
9]. As for the American recommendations, antibiotic prophylaxis for open Gustilo fractures stages I and II are based on the administration of cefazolin or clindamycin in the case of proven allergy to penicillin. For open Gustilo stage III fractures, antibiotic prophylaxis is based on the combination of ceftriaxone and vancomycin or aztreonam and vancomycin in the case of allergy to penicillin [
10].
The microorganisms reported in these postoperative infections of open fractures are, depending on the study, staphylococci in proportions varying between 30% and more than 50%, including MRSA (methicillin-resistant
Staphylococcus aureus),
Enterobacter spp. (on average 20–30%),
Pseudomonas spp., and enterococci (56% according to Glass) [
11,
12,
13,
14]. Thus, antibiotic prophylaxis recommendations do not consider the risk of surgical-site infections related to environmental bacteria described in some studies with a water contamination mechanism, in particular with
Pseudomonas spp. [
15,
16].
The rate, as well as the nature and resistance of the microorganisms involved, for surgical site infections (SSI), remain poorly described, and older studies do not reflect the evolution of bacterial distribution and resistance. The aim of this study was to describe the bacterial epidemiology of surgical site infections following an open fracture surgery of the lower limb.
2. Materials and Methods
This study was a monocentric retrospective cohort study based on the analysis of hospital records of patients from a 350-bed non-university hospital in the Ile de France region. In 2018, the department of “Seine et Marne” had a population of 1,412,516 inhabitants, of which 51.6% were women. The age group 24–59 years was more represented (45.8%) [
17]. There are 20 short stay establishments in this department, including 11 public hospitals, with a capacity of 2743 beds [
18]. The inclusion period ranged from 01 January 2012 to 31 December 2020.
The inclusion criteria were any patient who underwent surgery for an open fracture of the lower limb.
All patients operated on for an open fracture of the lower limb with missing data on the occurrence of surgical site infection were excluded.
This study was conducted in accordance with the Declaration of Helsinki and national and institutional standards. The local institutional review board did not waive the requirement for explicit patient consent due to the retrospective, monocentric nature of the study without the use of personal data.
Data on patient characteristics, laboratory tests and treatment outcomes were collected from software used in daily clinical practice (Sillage v19.0.1.2 and CGM Lab channel 1.20. 33,686) and included: age, sex, comorbidities (diabetes, immunodeficiency, peripheral artery disease of the lower limbs), lifestyle habits (smoking), time to surgery, antibiotic prophylaxis adapted to Gustilo’s classification [
2], time to new surgery, time to SSI, and microbiological results.
Antibiotic prophylaxis was prescribed according to the recommendations of the SFAR on the management of fractures [
1]. The duration of antibiotic prophylaxis is generally limited to the operative period, sometimes to 24 h, exceptionally to 48 h, and never beyond. An evaluation of the adequacy of antibiotic prophylaxis was carried out retrospectively by analysis of the medical record.
Surgical site infection was defined according to the criteria established by the center for disease control and prevention (CDC) in 1999, which distinguishes between superficial and deep SSI. Diagnostic criteria include the presence of pus, local inflammatory signs, and microbiological documentation or—simply—the surgeon’s clinical judgment [
19].
Deep infection diagnosis is based on criteria such as purulent drainage from the deep incision, formation of a deep abscess, dehiscence of the fascia either by infection or on reoperation, or deep infection in the presence of a metal implant around the bone. In addition, the diagnosis of deep or superficial infection was also based on radiological evidence and cultures obtained either during a secondary procedure to treat an infection or from exuding wounds [
19].
Antibiotic treatment of SSIs was adjusted according to the antibiotic sensitivity testing between days 5 and 10.
For univariate analysis, categorical variables were analyzed with the chi-square test or Fisher’s exact test. Continuous variables were assessed using the Mann–Whitney/Wilcoxon test and were expressed as the median and interquartile range (IQR). If the missing data were >10%, there was no calculation of relative risk (RR).
Variables with a univariate p-value < 0.050 were included in the multivariate analysis. Statistical analysis was performed using EPI INFO Version 7.2.3.1.
3. Results
A total of 149 patients that were operated on for open fractures of the lower limb were included, of whom 92 (61.7%) were men with a median age of 48.5 (27–62.5) years. The median BMI was 25.2 kg/m2 (21.7–27.8). Among the included patients, 10 (6.7%) were diabetic, and 9 (6%) were immunosuppressed. Smoking was identified in 19 (13%) patients.
The causes of fractures were mainly mechanical falls and motor vehicle accidents (MVA) in 32.3% and 27.6% of cases, respectively. The leg and ankle were the most frequent sites of open fractures in 48.6% and 30.8% of cases.
A total of 10.9% were classified as grade 3 according to the Gustilo classification, and 47.8% were classified as grade 2.
Antibiotic prophylaxis was administered in 85.2% of our population and was compliant in 40.9% of patients. The causes of non-compliance with antibiotic prophylaxis were inadequate duration and timing of prophylaxis, non-compliance of the antibiotic administered. Fourteen (9.4%) patients did not receive antibiotic prophylaxis, and for 8 (5.4%) patients, no information on antibiotic prophylaxis was recorded.
The median time to surgery was less than 1 h (0–24), with a mean time of 9.7 h (standard deviation (SD) 22.4).
In our study population, 19 (12.7%) patients developed a surgical site infection (SSI) according to the Gustilo classification, as follows: 5 patients (26.3%) were classified as Gustilo stage 1, 10 (52.6%) as stage 2, and 4 (21%) as stage 3. The median time to SSI occurrence was 20.5 days (IQR = 11–76). Of these SSIs, 15 patients (88.2%) had deep SSIs and underwent revision surgery with a median delay of 46 days (IQR = 14–78); 2 patients (1.6%) had superficial SSIs.
Table 1 describes the characteristics of patients with open lower limb fractures who had a surgical infection and the factors associated with the occurrence of surgical site infection.
Of the 19 patients with SSI, the sample was polymicrobial in 9 (47.4%) patients. In 9 (47.4%) cases, the samples identified a group 3 enterobacteria, with
Enterobacter cloacae being the main species in 7 (36.9%) cases. Staphylococci were identified in 11 patients, with MSSA (methicillin-susceptible
Staphylococcus aureus) in 9 (47.4%). All
Staphylococcus aureus (SA) were susceptible to methicillin, and all enterobacteria were susceptible to third-generation cephalosporins. In two patients, the samples were rendered sterile.
Table 2 shows the microbiological results of the surgical site infections.
Of all surgical site infections, 10 (58.8%) contained at least one organism resistant to amoxicillin/clavulanic acid. Factors associated with the occurrence of an SSI involving amoxicillin/clavulanic acid-resistant bacteria are shown in
Table 3.
4. Discussion
Our study confirms the high frequency of surgical site infections after open fractures of the lower limb, with an overall rate of 12.7%. This result is higher than that of Li’s study, which found an SSI rate of 9.8% [
20]. This may be related to the larger population size or the exclusion of superficial SSIs in Li’s study. In contrast, our result is closer to those found by Leonidou and Malhotra in their studies with SSI rates of 13.6% and 13%, respectively [
21,
22]. Both studies used the same definition of SSI as in our study.
Regarding risk factors for SSI, our study identified diabetes as the only factor associated with the occurrence of surgical site infections. Although not significant, smoking was more frequently found in patients with surgical site infections. These results may be related to the small size of our population. Other risk factors have been previously identified: male gender, smoking, polytrauma, Gustilo grade III classification, and contaminated wounds [
4,
7,
20].
As in Li’s study [
20], the time between fracture and surgery was not associated with the occurrence of surgical site infections.
Microbiologically, group 3 enterobacteriaceae, including
Enterobacter cloacae, were the most frequently found organisms. This result is similar to that found in the Carsenti-Etesse study [
12]. Our study shows a difference in the type of bacteria depending on the time of infection: SSIs involving group 3 Enterobacteriaceae are very early, at 13 days postoperative, whereas SSIs involving
Staphylococcus aureus occur later, at a median of 52 days. We put forward two explanatory hypotheses: the first is related to the pathophysiological mechanism of the infection involving contamination by telluric germs or bacteria of the digestive flora following a strong inoculum from the trauma. The second hypothesis concerns the lack of microbiological efficacy of antibiotic prophylaxis with amoxicillin/clavulanic acid, which is ineffective against group 3 Enterobacteriaceae or waterborne germs, such as
Pseudomonas. Late MSSA infections could be explained by a secondary mechanism of exogenous wound infection occurring several weeks after surgery and well after antibiotic prophylaxis. This hypothesis is supported by our observation, where surgical site infections with amoxicillin/clavulanic acid-sensitive germs occur after a longer period of time after surgery by exogenous contamination of the scar. Surgical site infections with amoxicillin and clavulanic acid-resistant organisms occur more rapidly after the first operation, possibly due to failure of the initial antibiotic prophylaxis with amoxicillin/clavulanic acid.
Concerning the two patients with sterile samples, two hypotheses were proposed: first, the absence of identification of the germ may be related to the use of an inadequate identification technique; secondly, a previous course of antibiotics could have decapitated the infection resulting in a negative sample. Our study shows, similar to many studies, partial compliance with the recommendations for the administration of antibiotic prophylaxis with an overall compliance rate of 40.9%. However, no association was found between the occurrence of SSI and non-compliance with antibiotic prophylaxis recommendations.
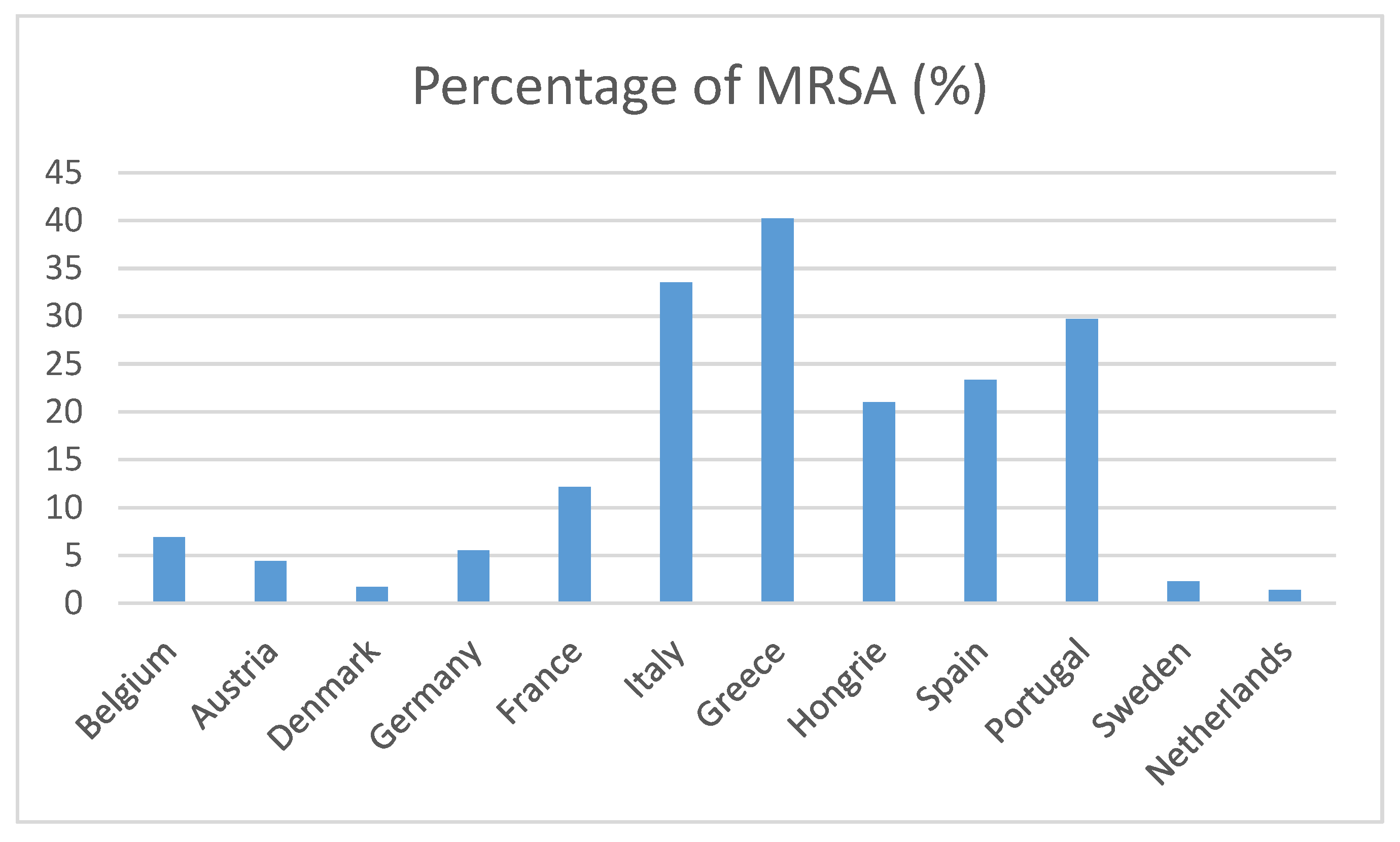
Concerning acquired resistance,
Staphylococcus aureus was always susceptible to methicillin, probably due to the ecology of the study site where methicillin resistance in staphylococci is low, around 15% in France (
Figure 1) [
23]. Cartenssi’s study [
12] reports similar results.
Our study has many limitations. Its monocentric nature leads to a bias related to local epidemiology, which is different according to regions and countries. Our institution is located near the forest of Fontainebleau, where many sports activities at risk of serious trauma, such as horse riding, quad biking, and mountain biking, favor soil contamination. It is likely that centers located in strictly urban areas do not present the same type of trauma.
Our results suggest a failure of the antibiotic prophylaxis strategy with amoxicillin/clavulanate for the prevention of SSI after open limb fractures. These results call for a multicenter prospective cohort study that would allow the confirmation of the results of our study, which would argue in favor of antibiotic prophylaxis with piperacillin-tazobactam in case of land contamination for open fractures.
5. Conclusions
The rate of postoperative infections in all open lower limb fractures was 12.7%. The presence of early SSI due to group 3 Enterobacteriaceae suggests that current antibiotic prophylaxis protocols using amoxicillin/clavulanic acid are not effective in half of the cases, warranting a re-evaluation of the protocols and a discussion on the possible use of piperacillin-tazobactam. Our data calls for prospective multicenter studies.
Author Contributions
Conceptualization, S.D. and A.D.P.; methodology, T.J.Y. and S.D.; validation, all authors, data extraction, S.S.; data curation: A.P. and A.A.; project administration: C.C., A.S., C.N. and C.F.; formal analysis, T.J.Y.; writing—original draft preparation, T.J.Y. and S.D.; writing—review and editing, T.J.Y.; English corrections, M.R.; supervision, S.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the non-interventional and retrospective design of the study. The declaration number of conformity to the reference methodology is 2215880 v 0.
Informed Consent Statement
Patient consent was waived due to the non-interventional retrospective design of the study.
Data Availability Statement
Data is contained within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Martin, C.; Auboyer, C.; Boisson, M.; Dupont, H.; Gauzit, R.; Kitzis, M. Antibioprophylaxis in surgery and interventional medicine (adult patients). Update 2017. Anaesth. Crit. Care Pain Med. 2019, 38, 549–562. [Google Scholar] [CrossRef] [PubMed]
- Gustilo, R.B.; Mendoza, R.M.; Williams, D.N. Problems in the management of type III (severe) open fractures. A new classification of type III open fractures. J. Trauma 1984, 24, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Isaac, S.M.; Woods, A.; Danial, I.N.; Mourkus, H. Antibiotic Prophylaxis in Adults With Open Tibial Fractures: What Is the Evidence for Duration of Administration? A Systematic Review. J. Foot Ankle Surg. 2016, 55, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Kortram, K.; Bezstarosti, H.; Metsemakers, W.J.; Raschke, M.J.; Van Lieshout, E.M.M.; Verhofstad, M.H.J. Risk factors for infectious complications after open fractures; a systematic review and meta-analysis. Int. Orthop. 2017, 45, 1965–1982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papakostidis, C.; Kanakaris, N.K.; Pretel, J.; Faour, O.; Morell, D.J.; Giannoudis, P.V. Prevalence of complications of open tibial shaft fractures stratified as per the Gustilo-Anderson classification. Injury 2011, 42, 1408–1415. [Google Scholar] [CrossRef] [PubMed]
- Ktistakis, I.; Giannoudi, M.; Giannoudis, P.V. Infection rates after open tibial fractures: Are they decreasing? Injury 2014, 45, 1025–1027. [Google Scholar] [CrossRef] [PubMed]
- Ukai, T.; Hamahashi, K.; Uchiyama, Y.; Kobayashi, Y.; Watanabe, M. Retrospective analysis of risk factors for deep infection in lower limb Gustilo–Anderson type III fractures. J. Orthop. Traumatol. 2020, 21, 10. [Google Scholar] [CrossRef] [PubMed]
- Gosselin, R.A.; Roberts, I.; Gillespie, W.J. Antibiotics for preventing infection in open limb fractures. Cochrane Database Syst. Rev. 2004, CD003764. [Google Scholar] [CrossRef] [PubMed]
- Yarrow, J.; Rahman, S.; Marsden, N.; Pallister, I.; Hemington-Gorse, S. Management of open lower limb injuries in South West England and Wales. Ann. R Coll. Surg. Engl. 2015, 97, 35–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garner, M.R.; Sethuraman, S.A.; Schade, M.A.; Boateng, H. Antibiotic Prophylaxis in Open Fractures: Evidence, Evolving Issues, and Recommendations. J. Am. Acad. Orthop. Surg. 2020, 28, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Glass, G.E.; Barrett, S.P.; Sanderson, F.; Pearse, M.F.; Nanchahal, J. The microbiological basis for a revised antibiotic regimen in high-energy tibial fractures: Preventing deep infections by nosocomial organisms. J. Plast. Reconstr. Aesth. Surg. 2011, 64, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Carsenti-Etesse, H.; Doyon, F.; Desplaces, N.; Gagey, O.; Tancrède, C.; Pradier, C.; Dunais, B.; Dellamonica, P. Epidemiology of bacterial infection during management of open leg fractures. Eur. J. Clin. Microbiol. Infect. Dis. 1999, 18, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.N.; Burns, T.C.; Hayda, R.A.; Hospenthal, D.R.; Murray, C.K. Infectious complications of open type III tibial fractures among combat casualties. Clin. Infect. Dis. 2007, 45, 409–415. [Google Scholar] [CrossRef] [PubMed]
- Burns, T.C.; Stinner, D.J.; Mack, A.W.; Potter, B.K.; Beer, R.; Eckel, T.T. Microbiology and injury characteristics in severe open tibia fractures from combat. J. Trauma Acute Care Surg. 2012, 72, 1062–1067. [Google Scholar] [CrossRef] [PubMed]
- Alfonso-Sanchez, J.L.; Martinez, I.M.; Martín-Moreno, J.M.; González, R.S.; et Botía, F. Analyzing the risk factors influencing surgical site infections: The site of environmental factors. Can. J. Surg. 2017, 60, 155–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spagnolo, A.M.; Ottria, G.; Amicizia, D.; Perdelli, F.; Cristina, M.L. Operating theatre quality and prevention of surgical site infections. J. Prev. Med. Hyg. 2013, 54, 131–137. [Google Scholar] [PubMed]
- Available online: https://www.insee.fr/fr/statistiques/2012692#tableau-TCRD_021_tab1_departements (accessed on 23 November 2021).
- Available online: https://www.sanitaire-social.com/annuaire/hopitaux-cliniques/seine-et-marne-77 (accessed on 23 November 2021).
- Mangram, A.J.; Horan, T.C.; Pearson, M.L.; Argent, L.C.; Jarvis, W.R. Guideline for prevention of surgical site infection, 1999. Infect Control Hosp. Epidemiol. 1999, 20, 247–280. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wang, Q.; Lu, Y.; Feng, Q.; He, X.; Li, Z.; Zhang, K. Relationship Between Time to Surgical Debridement and the Incidence of Infection in Patients with Open Tibial Fractures. Orthop. Surg. 2020, 12, 524–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leonidou, A.; Kiraly, Z.; Gality, H.; Apperley, S.; Vanstone, S.; Woods, D.A. The effect of the timing of antibiotics and surgical treatment on infection rates in open long-bone fractures: A 6-year prospective study after a change in policy. Strateg. Trauma Limb Reconstr. 2014, 9, 167–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malhotra, A.K.; Goldberg, S.; Graham, J.; Malhotra, N.R.; Willis, M.C.; Mounasamy, V.; Guilford, K.; Duane, T.M.; Aboutanos, M.B.; Mayglothling, J.; et al. Open extremity fractures: Impact of delay in operative debridement and irrigation. J. Trauma Acute Care Surg. 2014, 76, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://atlas.ecdc.europa.eu/public/index.aspx?Dataset=27&HealthTopic=4) (accessed on 15 September 2021).
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}