
Antibacterial Effects of Modified Implant Abutment Surfaces for the Prevention of Peri-Implantitis—A Systematic Review


Abstract
:1. Introduction:
2. Material and Methods:
- C (Case): Prevention of peri-implantitis through antibacterial implant-abutment coatings
- A (Assay or laboratory procedure): analyzing antibacterial activity and cytotoxicity
- P (Predicate/reference standard): abutment material without coating
- O (Outcome): cell viability, bacterial death
2.1. Eligibility Criteria
2.2. Information Sources and Search
2.2.1. Electronic Search
2.2.2. Search Strategy
PubMed
Cochrane Central Register of Controlled Trials
2.3. Risk of Bias Assessment
3. Results
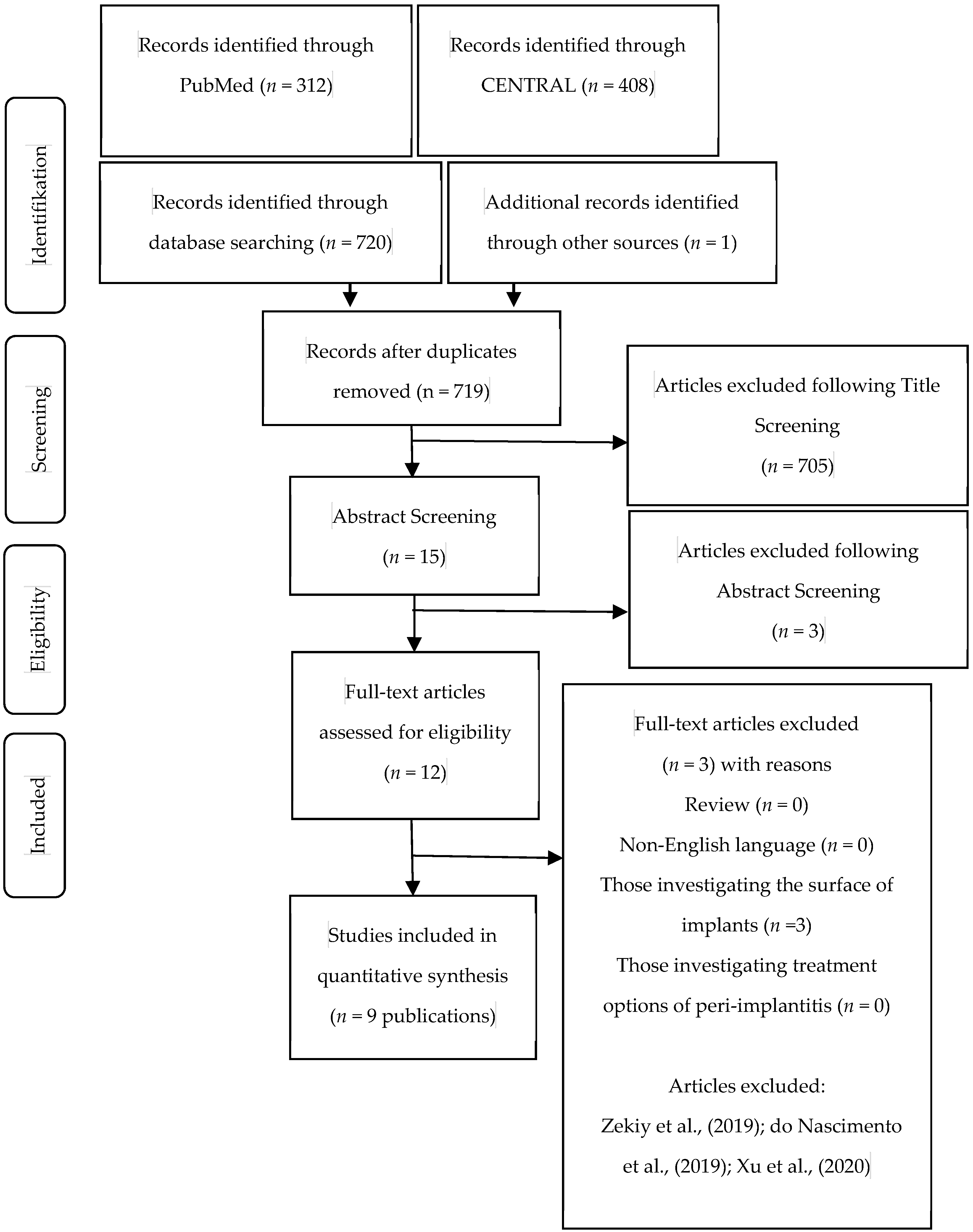
3.1. Study Selection
3.2. Risk of Bias Assessment (RoB)
3.3. Study Characteristics
3.3.1. Abutment Surface Modification
3.3.2. Control Groups
3.3.3. Antibacterial Properties of Investigated Implant Abutment Surfaces
In Vitro Studies
In Vivo Studies
3.3.4. Influence of Implant Abutment Coating on the Behavior of Examined Cells
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S158–S171. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis--a review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindhe, J.; Meyle, J.; Group D of the European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khammissa, R.A.; Feller, L.; Meyerov, R.; Lemmer, J. Peri-implant mucositis and peri-implantitis: Clinical and histopathological characteristics and treatment. S. Afr. Dent. J. 2012, 67, 122, 124–126. [Google Scholar]
- Guo, T.; Gulati, K.; Arora, H.; Han, P.; Fournier, B.; Ivanovski, S. Race to invade: Understanding soft tissue integration at the transmucosal region of titanium dental implants. Dent. Mater. 2021, 37, 816–831. [Google Scholar] [CrossRef]
- Zheng, Z.; Ao, X.; Xie, P.; Jiang, F.; Chen, W. The biological width around implant. J. Prosthodont. Res. 2021, 65, 11–18. [Google Scholar] [CrossRef]
- Sanz, M.; Chapple, I.L.; On Behalf of Working Group 1 of the VIII European Workshop on Periodontology. Clinical research on peri-implant diseases: Consensus report of Working Group 4. J. Clin. Periodontol. 2012, 39 (Suppl. 12), 202–206. [Google Scholar] [CrossRef]
- Furst, M.M.; Salvi, G.E.; Lang, N.P.; Persson, G.R. Bacterial colonization immediately after installation on oral titanium implants. Clin. Oral Implants Res. 2007, 18, 501–508. [Google Scholar] [CrossRef]
- Persson, G.R.; Renvert, S. Cluster of bacteria associated with peri-implantitis. Clin. Implants Dent. Relat. Res. 2014, 16, 783–793. [Google Scholar] [CrossRef]
- Kheur, S.; Singh, N.; Bodas, D.; Rauch, J.Y.; Jambhekar, S.; Kheur, M.; Rajwade, J. Nanoscale silver depositions inhibit microbial colonization and improve biocompatibility of titanium abutments. Colloids Surf. B Biointerfaces 2017, 159, 151–158. [Google Scholar] [CrossRef]
- Cardoso, M.; Sangalli, J.; Koga-Ito, C.Y.; Ferreira, L.L.; da Silva Sobrinho, A.S.; Nogueira, L., Jr. Abutment Coating with Diamond-Like Carbon Films to Reduce Implant-Abutment Bacterial Leakage. J. Periodontol. 2016, 87, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Fröjd, V.; Linderbäck, P.; Wennerberg, A.; Chávez de Paz, L.; Svensäter, G.; Davies, J.R. Effect of nanoporous TiO2 coating and anodized Ca2+ modification of titanium surfaces on early microbial biofilm formation. BMC Oral Health 2011, 11, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odatsu, T.; Kuroshima, S.; Sato, M.; Takase, K.; Valanezhad, A.; Naito, M.; Sawase, T. Antibacterial Properties of Nano-Ag Coating on Healing Abutment: An In Vitro and Clinical Study. Antibiot. (Basel) 2020, 9, 347. [Google Scholar] [CrossRef]
- Huacho, P.M.M.; Nogueira, M.N.M.; Basso, F.G.; Jafelicci Junior, M.; Francisconi, R.S.; Spolidorio, D.M.P. Analyses of Biofilm on Implant Abutment Surfaces Coating with Diamond-Like Carbon and Biocompatibility. Braz. Dent. J. 2017, 28, 317–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunello, G.; Brun, P.; Gardin, C.; Ferroni, L.; Bressan, E.; Meneghello, R.; Zavan, B.; Sivolella, S. Biocompatibility and antibacterial properties of zirconium nitride coating on titanium abutments: An in vitro study. PLoS ONE 2018, 13, e0199591. [Google Scholar] [CrossRef]
- Xing, R.; Witsø, I.L.; Jugowiec, D.; Tiainen, H.; Shabestari, M.; Lyngstadaas, S.P.; Lönn-Stensrud, J.; Haugen, H.J. Antibacterial effect of doxycycline-coated dental abutment surfaces. Biomed. Mater. 2015, 10, 055003. [Google Scholar] [CrossRef]
- Visai, L.; Rimondini, L.; Giordano, C.; Del Curto, B.; Sbarra, M.S.; Franchini, R.; Della Valle, C.; Chiesa, R. Electrochemical surface modification of titanium for implant abutments can affect oral bacteria contamination. J. Appl. BioMater. Biomech 2008, 6, 170–177. [Google Scholar]
- Almohandes, A.; Abrahamsson, I.; Dahlén, G.; Berglundh, T. Effect of biofilm formation on implant abutments with an anti-bacterial coating: A pre-clinical in vivo study. Clin. Oral Implants Res. 2021, 32, 756–766. [Google Scholar] [CrossRef]
- Grossner-Schreiber, B.; Griepentrog, M.; Haustein, I.; Muller, W.D.; Lange, K.P.; Briedigkeit, H.; Gobel, U.B. Plaque formation on surface modified dental implants. An in vitro study. Clin. Oral Implants Res. 2001, 12, 543–551. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Christenson, R.H.; Committee on Evidence Based Laboratory Medicine of the International Federation for Clinical Chemistry Laboratory Medicine. Evidence-based laboratory medicine—a guide for critical evaluation of in vitro laboratory testing. Ann. Clin. Biochem. 2007, 44, 111–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Sterne, J.A.C.; Savovic, J.; Page, M.J.; Hróbjartsson, A.; Boutron, I.; Reeves, B.; Eldridge, S. A revised tool for assessing risk of bias in randomized trials. Cochrane Database Syst. Rev. 2016, 10, 29–31. [Google Scholar]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Handbook for Conducting a Literature-Based Health Assessment Using OHAT Approach for Systematic Review and Evidence Integration. 2019. Available online: https://ntp.niehs.nih.gov/ntp/ohat/pubs/handbookmarch2019_508.pdf (accessed on 11 October 2021).
- Abdullah, H.; Sorrell, C. Titanium Dioxide (TiO2) Films by Anodic Oxidation in Phosphoric Acid. Adv. Mater. Res. 2012, 545, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Calvert, K.L.; Desai, T.; Webster, T.J. Advances in calcium phosphate coatings--anodic spark deposition: A review. Front. Biosci. 2014, 19, 475–489. [Google Scholar] [CrossRef] [Green Version]
- Alcazar, J.C.; Salas, M.M.; Conde, M.C.; Chisini, L.A.; Demarco, F.F.; Tarquinio, S.B.; Carreno, N.L. Electrochemical Cathodic Polarization, a Simplified Method That Can Modified and Increase the Biological Activity of Titanium Surfaces: A Systematic Review. PLoS ONE 2016, 11, e0155231. [Google Scholar] [CrossRef] [Green Version]
- Walter, M.S.; Frank, M.J.; Satue, M.; Monjo, M.; Ronold, H.J.; Lyngstadaas, S.P.; Haugen, H.J. Bioactive implant surface with electrochemically bound doxycycline promotes bone formation markers in vitro and in vivo. Dent. Mater. 2014, 30, 200–214. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.K.; Lin, Y.S.; Chen, Y.J.; Chu, H. A review of photocatalysts prepared by sol-gel method for VOCs removal. Int. J. Mol. Sci. 2010, 11, 2336–2361. [Google Scholar] [CrossRef]
- Rane, A.V.; Kanny, K.; Abitha, V.K.; Thomas, S. Chapter 5—Methods for Synthesis of Nanoparticles and Fabrication of Nanocomposites. In Synthesis of Inorganic Nanomaterials; Mohan Bhagyaraj, S., Oluwafemi, O.S., Kalarikkal, N., Thomas, S., Eds.; Woodhead Publishing: Cambridge, UK, 2018; pp. 121–139. [Google Scholar]
- Tran, L.; Tam, D.N.H.; Elshafay, A.; Dang, T.; Hirayama, K.; Huy, N.T. Quality assessment tools used in systematic reviews of in vitro studies: A systematic review. BMC Med. Res. Methodol. 2021, 21, 101. [Google Scholar] [CrossRef]
- Roony, A. Extending a Risk-of-Bias Approach to Address In Vitro Studies. In National Toxicology Program Office of Health Assessment and Translation; Environmental Protection Agency (EPA): Washington, DC, USA, 2015. Available online: https://ofmpub.epa.gov/eims/eimscomm.getfile? (accessed on 11 October 2021).
- Dickersin, K.; Chan, S.; Chalmers, T.C.; Sacks, H.S.; Smith, H., Jr. Publication bias and clinical trials. Control. Clin. Trials 1987, 8, 343–353. [Google Scholar] [CrossRef]
- Saito, T.; Iwase, T.; Horie, J.; Morioka, T. Mode of photocatalytic bactericidal action of powdered semiconductor TiO2 on mutans streptococci. J. Photochem. Photobiol. B 1992, 14, 369–379. [Google Scholar] [CrossRef]
- Arango-Santander, S.; Pelaez-Vargas, A.; Freitas, S.C.; Garcia, C. A novel approach to create an antibacterial surface using titanium dioxide and a combination of dip-pen nanolithography and soft lithography. Sci. Rep. 2018, 8, 15818. [Google Scholar] [CrossRef]
- Pantaroto, H.N.; Ricomini-Filho, A.P.; Bertolini, M.M.; Dias da Silva, J.H.; Azevedo Neto, N.F.; Sukotjo, C.; Rangel, E.C.; Barao, V.A.R. Antibacterial photocatalytic activity of different crystalline TiO2 phases in oral multispecies biofilm. Dent. Mater. 2018, 34, e182–e195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marciano, F.R.; Lima-Oliveira, D.A.; Da-Silva, N.S.; Diniz, A.V.; Corat, E.J.; Trava-Airoldi, V.J. Antibacterial activity of DLC films containing TiO2 nanoparticles. J. Colloid Interface Sci. 2009, 340, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.J.; Tsai, M.T.; Shieh, T.M.; Huang, H.L.; Hsu, J.T.; Ko, Y.C.; Fuh, L.J. In vitro antibacterial activity and cytocompatibility of bismuth doped micro-arc oxidized titanium. J. Biomater. Appl. 2013, 27, 553–563. [Google Scholar] [CrossRef] [PubMed]
- Nagay, B.E.; Dini, C.; Cordeiro, J.M.; Ricomini-Filho, A.P.; de Avila, E.D.; Rangel, E.C.; da Cruz, N.C.; Barao, V.A.R. Visible-Light-Induced Photocatalytic and Antibacterial Activity of TiO2 Codoped with Nitrogen and Bismuth: New Perspectives to Control Implant-Biofilm-Related Diseases. ACS Appl. Mater. Interfaces 2019, 11, 18186–18202. [Google Scholar] [CrossRef]
- Pascale, D.; Gordon, J.; Lamster, I.; Mann, P.; Seiger, M.; Arndt, W. Concentration of doxycycline in human gingival fluid. J. Clin. Periodontol. 1986, 13, 841–844. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.M.; Walker, C.B.; Murphy, J.C.; Goodson, J.M.; Socransky, S.S. Concentration of tetracycline in human gingival fluid after single doses. J. Clin. Periodontol. 1981, 8, 117–121. [Google Scholar] [CrossRef]
- Lavda, M.; Clausnitzer, C.E.; Walters, J.D. Distribution of systemic ciprofloxacin and doxycycline to gingiva and gingival crevicular fluid. J. Periodontol. 2004, 75, 1663–1667. [Google Scholar] [CrossRef]
- Zetner, K.; Rothmueller, G. Treatment of periodontal pockets with doxycycline in beagles. Vet. Ther. 2002, 3, 441–452. [Google Scholar]
- Tomasi, C.; Koutouzis, T.; Wennstrom, J.L. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets. J. Periodontol. 2008, 79, 431–439. [Google Scholar] [CrossRef]
- Tomasi, C.; Wennstrom, J.L. Locally delivered doxycycline as an adjunct to mechanical debridement at retreatment of periodontal pockets: Outcome at furcation sites. J. Periodontol. 2011, 82, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Lang, N.P.; Cortellini, P.; Suvan, J.E.; Eickholz, P.; Fourmousis, I.; Topoll, H.; Vangsted, T.; Wallkamm, B. Effects of a single topical doxycycline administration adjunctive to mechanical debridement in patients with persistent/recurrent periodontitis but acceptable oral hygiene during supportive periodontal therapy. J. Clin. Periodontol. 2012, 39, 475–482. [Google Scholar] [CrossRef] [PubMed]
- van Winkelhoff, A.J. Antibiotics in the treatment of peri-implantitis. Eur. J. Oral Implantol. 2012, 5, S43–S50. [Google Scholar] [PubMed]
- Roy, R.K.; Lee, K.R. Biomedical applications of diamond-like carbon coatings: A review. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 83, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Pinault, M.; Pfefferle, L.D.; Elimelech, M. Single-walled carbon nanotubes exhibit strong antimicrobial activity. Langmuir 2007, 23, 8670–8673. [Google Scholar] [CrossRef]
- Soininen, A.; Tiainen, V.M.; Konttinen, Y.T.; van der Mei, H.C.; Busscher, H.J.; Sharma, P.K. Bacterial adhesion to diamond-like carbon as compared to stainless steel. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 90, 882–885. [Google Scholar] [CrossRef]
- Franci, G.; Falanga, A.; Galdiero, S.; Palomba, L.; Rai, M.; Morelli, G.; Galdiero, M. Silver nanoparticles as potential antibacterial agents. Molecules 2015, 20, 8856–8874. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Castañón, G.A.; Niño-Martínez, N.; Martínez-Gutierrez, F. Synthesis and antibacterial activity of silver nanoparticles with different sizes. J. Nanoparticle Res. 2008, 10, 1343–1348. [Google Scholar] [CrossRef]
- Monteiro, D.R.; Gorup, L.F.; Silva, S.; Negri, M.; de Camargo, E.R.; Oliveira, R.; Barbosa, D.B.; Henriques, M. Silver colloidal nanoparticles: Antifungal effect against adhered cells and biofilms of Candida albicans and Candida glabrata. Biofouling 2011, 27, 711–719. [Google Scholar] [CrossRef]
- Salleh, A.; Naomi, R.; Utami, N.D.; Mohammad, A.W.; Mahmoudi, E.; Mustafa, N.; Fauzi, M.B. The Potential of Silver Nanoparticles for Antiviral and Antibacterial Applications: A Mechanism of Action. Nanomaterials 2020, 10, 1566. [Google Scholar] [CrossRef]
- Yin, I.X.; Zhang, J.; Zhao, I.S.; Mei, M.L.; Li, Q.; Chu, C.H. The Antibacterial Mechanism of Silver Nanoparticles and Its Application in Dentistry. Int. J. Nanomed. 2020, 15, 2555–2562. [Google Scholar] [CrossRef] [Green Version]
- Marambio-Jones, C.; Hoek, E.M.V. A review of the antibacterial effects of silver nanomaterials and potential implications for human health and the environment. J. Nanoparticle Res. 2010, 12, 1531–1551. [Google Scholar] [CrossRef]
- Groessner-Schreiber, B.; Hannig, M.; Duck, A.; Griepentrog, M.; Wenderoth, D.F. Do different implant surfaces exposed in the oral cavity of humans show different biofilm compositions and activities? Eur. J. Oral Sci. 2004, 112, 516–522. [Google Scholar] [CrossRef]
- Ji, M.K.; Park, S.W.; Lee, K.; Kang, I.C.; Yun, K.D.; Kim, H.S.; Lim, H.P. Evaluation of antibacterial activity and osteoblast-like cell viability of TiN, ZrN and (Ti1-xZrx)N coating on titanium. J. Adv. Prosthodont. 2015, 7, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Piattelli, M.; Vrespa, G.; Caputi, S.; Piattelli, A. Bacterial adhesion on titanium nitride-coated and uncoated implants: An in vivo human study. J. Oral Implantol. 2003, 29, 80–85. [Google Scholar] [CrossRef]
- Rehman, A.; Hu, J.; Ott, S.J.; Grossner-Schreiber, B. Microbial community composition on modified dental implant surfaces: An in vivo study. Int. J. Oral Maxillofac. Implants 2012, 27, 811–819. [Google Scholar]
- Sakka, S.; Baroudi, K.; Nassani, M.Z. Factors associated with early and late failure of dental implants. J. Investig. Clin. Dent. 2012, 3, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Shimabukuro, M. Antibacterial Property and Biocompatibility of Silver, Copper, and Zinc in Titanium Dioxide Layers Incorporated by One-Step Micro-Arc Oxidation: A Review. Antibiotics 2020, 9, 716. [Google Scholar] [CrossRef] [PubMed]
- Vargas-Reus, M.A.; Memarzadeh, K.; Huang, J.; Ren, G.G.; Allaker, R.P. Antimicrobial activity of nanoparticulate metal oxides against peri-implantitis pathogens. Int. J. Antimicrob. Agents 2012, 40, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Abdulkareem, E.H.; Memarzadeh, K.; Allaker, R.P.; Huang, J.; Pratten, J.; Spratt, D. Anti-biofilm activity of zinc oxide and hydroxyapatite nanoparticles as dental implant coating materials. J. Dent. 2015, 43, 1462–1469. [Google Scholar] [CrossRef] [PubMed]
- Luo, Q.; Cao, H.; Wang, L.; Ma, X.; Liu, X. ZnO@ZnS nanorod-array coated titanium: Good to fibroblasts but bad to bacteria. J. Colloid Interface Sci. 2020, 579, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fan, H.; Zhang, F.; Zhao, S.; Liu, Y.; Xu, Y.; Wu, R.; Li, D.; Yang, Y.; Liao, L.; et al. Antibacterial Properties of Bilayer Biomimetic Nano-ZnO for Dental Implants. ACS Biomater. Sci. Eng. 2020, 6, 1880–1886. [Google Scholar] [CrossRef]
- Yin, S.; Sun, N.; Jiang, F.; Lu, Y.; Yang, G.; Wu, X.; Lin, S.; Zhang, W.; Jiang, X. The Translation from In Vitro Bioactive Ion Concentration Screening to In Vivo Application for Preventing Peri-implantitis. ACS Appl. Mater. Interfaces 2021, 13, 5782–5794. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Inclusion criteria |
|
| Exclusion criteria |
|
| Author (Year) [10,11,12,13,14,15,16,17,18] | Study Design | Abutment Coating | Control Group | Cells Used | Bacteria Used | Test Procedure | Influence of Abutment Coating on Cell Behaviour | Influence of Abutment Coating on Bacteria | Missing or Unclear Information |
|---|---|---|---|---|---|---|---|---|---|
| Visai et al., (2008) [17] | In vitro and in vivo | Electrochemical surface modification of titanium by Anodic Spark Deposition technique (ASD), performed in a calcium phosphate enriched solution | Grade 2 titanium | MG63—human osteosarcoma cell lines and L929—murine fibroblasts | Streptococcus mutans, Streptococcus salivarius and Streptococcus sanguis | Surface microstrucutral characterization; in vitro metabloic cell activity with Alamar blue Solution; Bacterial adhesion and growth inhibition by couting Colony Forming Units/cm2; in vivo: customized appliances with samples on 8 volunteers measuring bacteria density after 24 h with SEM | Metabolic activity showed no differences between the groups; Cell number of MG63 cells on ASD treated sample statistically significant higher compared to negative control | After 24 hr of incubation, the results of antibacterial activity were greater on AB than on Ti samples (p < 0.05) following this trend: S. salivarius > S. sanguis > S. mutans; After 3 hr of incubation, bacterial attachment was consistently reduced on ASD samples than on Ti samples for all tested strains (p < 0.05). The amount of biofilm formation was lower, on average, in the non-treated titanium than in the ASD sample | - |
| Fröjd et al., (2011) [12] | In vitro | Sol-gel treatment to create a nanoporous TiO2 coat (SG), heat-treated in a similar way to the sol-gel treated discs (HT), or anodically oxidized and calcium treated (OC) | Grade 4 pure titanium | - | Streptococcus sanguinis and Actinomyces naeslundii | Assay for bacterial adhesion and early biofilm formation | - | No differences in the overall biofilm biovolume between the four surfaces were detected | - |
| Almohandes et al., (2021) [18] | Pre-clinical in vivo study in dogs | Titanium-bismuth-gallium (Ti-Bi-Ga) coating by physical vapour deposition (PVD) | Titanium Uni abutment (Astra Tech Implant SystemTM, Dentsply Implants IH AB) | - | Microbiological samples were collected and analyzed | 2 months after implantation, ligatures were placed around implants and plaque formation was allowed until the end of the experimen; ligatures were removed after 4 weeks; Radiographs and microbiological samples were obtained from each implant site during the plaque formation period. Biopsies were obtained 8 months after abutment connection and prepared for histological analysis. | Ti-Bi-Ga coating did not influence the host response in the adjacent peri-implant mucosa. | Ti-Bi-Ga coating did not prevent biofilm formation | Titanium Ggade was missing. (According to Astra Tech Implant System; Dentsply Sirona: Ti6Al4V Grad 5) |
| Xing et al., (2015) [16] | In vitro | Doxycycline coating by cathodic polarization and polarization time of 1 h and 5 h and current density of 1 and 5 mA cm−2 | Titanium–zirconium coin-shaped samples machined (M); and machined, acid-etched (MA) Control 1: cathodic polarization with Doxy at 1 mA cm−2 for 1 h; control 2: cathodic polarization with Doxy at 5 mA cm−2 for 3 h. | - | Staphylococcus epidermidis | Biofilm and planktonic growth assays using Staphylococcus epidermidis | - | Initial bacteriostatic property from the burst release of Doxy within 24 h, and a long-term antibacterial potential for at least 2 weeks. A higher amount of Doxy on the surface can be obtained by increasing polarization time from 1h to 5h and current density from 1 to 5 mA cm−2. | |
| Cardoso et al., (2016) [11] | In vitro | Diamond-like carbon (DLC) films (pure DLC and DLC with embedded silver nanoparticles [Ag-DLC]) were deposited on the abutment bases by plasma-enhanced chemical vapor deposition (PECVD) | Titanium abutments | - | Enterococcus faecalis | Indirect (or reverse) technique was used to assess bacterial leakage from internal and external hexagon implant-abutment connections; inner part of the implant was inoculated with 1 μL E. faecalis suspension (106 colony-forming units [CFU]/mL); After inoculation, the abutments were screw-retained to the implants with a torque of 20 Ncm. The quantity of inoculum was determined in a pilot study, in which the authors observed that >1 μL promoted leakage to the external side. | - | Percentage of bacterial leakage was 16.09% for EH implants and 80.71% for IH implants (p < 0.0001). Although the DLC film reduced the absolute percentage of leakage, there were no statistically significant differences between the two types of implants (p = 0.253 for EH implants and p = 0.535 for IH implants). | Abutment Material. The pictures show a titanium abutments but without specific caption |
| Huacho et al., (2017) [14] | In vitro | Diamond-like carbon (DLC) | Titanium | HaCat cells | Escherichia coli | Biocompatibility testing of DLC was performed by colorimetric analysis of methylthiazol tetrazolium (MTT); Bacterial Adhesion Test, Antimicrobial Test | Biocompatible, with mild cytotoxicity | DLC has no antimicrobial properties and does not interfere with bacterial adhesion when tested against Escherichia coli | The method for coating surfaces with DLC was not mentioned. |
| Kheur et al., (2017) [10] | In vitro | Etched and non-etched Ti discs were coated with silver using a DC plasma sputter coating instrument for 1, 2, 3 and 5 min | Grade 5 titanium discs | Human gingival fibroblast | Staphylococcus aureus, Streptococcus mutans, Pseudomonas aeruginosa | Bacterial adhesion assay; Cytotoxicity against HGF cells was assessed by MTT assay; Cell morphology by phase contrast microscopy | In comparison to the titanium control, a reduction (20%) in cell viability was observed insilver-deposited titanium abutment. For unetched-Ag coated samples; Ti-Ag(2), Ti-Ag(3) and Ti-Ag(5), although a reduction in viability was noted, the difference was not statistically significant. Similar reductions were noted in the case of etched Ag-coated samples; Ti-EAg(2), Ti-E-Ag(3). However, in a case of Ti-E-Ag(5), only 60% cell viability was observed; this decrease being statistically significant (p < 0.05) as compared to other time-points. Overall, at 72 h the toxicity of the specimens was in the order, Ti-E-Ag(5) > Ti-Ag(5) > Ti-EAg(3) > Ti-Ag(3) > Ti-E-Ag(2) > Ti-Ag(2) | In case of S. mutans and P. aeruginosa, the viable count reduced drastically after 6 h in all silver deposited abutments viz., Ti-Ag(1), Ti-Ag(2), Ti-Ag(3) and Ti- Ag(5). In the case of S. aureus, cells remained viable after contact with Ti-Ag(1) for 6 h. However, in a case of Ti-Ag(2), Ti-Ag(3) and Ti-Ag(5), the decrease in cell viability post 6 h contact was significant. | Antibacterial activity of etched titanium discs with silver coating was not mentioned. |
| Brunello et al., (2018) [15] | In vitro | Anodized, coated with titanium nitride, or coated with zirconium nitride. Anodization (Anodic oxidation) was performed with current of 2.2 A, voltage of 8 V in 5% phosphoric solution for 10 min. Coating was applied by PVD | Uncoated machined Ti disks | Human gingival fibroblasts | Streptococcus salivarius, S. sanguinis, S. mutans, S. sobrinus, and S. oralis | MTT Assay for proliferation analyzes of cells incubated directly on the discs; morphological analyzes with SEM; Hemolyses Test, Ames Test; RNA extraction and first-strand cDNA synthesis; Real-time PCR; Bacterial strains and biofilm quantification, indirect Immunfluorscence | No differences in proliferation between the samples. None of the samples were hemolytic; no mutagenic activity was revealed for any of the surfaces tested; The genes considered were talin, alpha-actinin, vinculin, zyxin, paxillin, vitronectin, focal adhesion kinase (FAK), and collagen type I, all involved in cell adhesion. Good mRNA relative expression levels were found on all the surfaces examined, but the highest gene expression values were observed on the ZrN-treated disks, HGF adhered on all disks; no difference in Vinculin expression; | The percentage of dead bacteria was higher in the biofilms grown on the TiN- and ZrN-coated disks than on the uncoated disks | - |
| Odatsu et al., (2020) [13] | In vitro and clinical study | Microwave assistant nanosilver coating on pure titanium | Pure titanium | Human gingival fibroblasts | Staphylococcus aureus | Immunfluorescence of actin filaments; number of attached cells, MTS assay for assessment of proliferation; Measuring colony forming units; Plaque covered area of abutments in vivo after 28 days | No statistically significant difference between control and nano-Ag coating regarding cell number and proliferation | Prevention of plaque accumulation by the nano-Ag coating. | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jennes, M.-E.; Naumann, M.; Peroz, S.; Beuer, F.; Schmidt, F. Antibacterial Effects of Modified Implant Abutment Surfaces for the Prevention of Peri-Implantitis—A Systematic Review. Antibiotics 2021, 10, 1350. https://doi.org/10.3390/antibiotics10111350
Jennes M-E, Naumann M, Peroz S, Beuer F, Schmidt F. Antibacterial Effects of Modified Implant Abutment Surfaces for the Prevention of Peri-Implantitis—A Systematic Review. Antibiotics. 2021; 10(11):1350. https://doi.org/10.3390/antibiotics10111350
Chicago/Turabian StyleJennes, Marie-Elise, Michael Naumann, Simon Peroz, Florian Beuer, and Franziska Schmidt. 2021. "Antibacterial Effects of Modified Implant Abutment Surfaces for the Prevention of Peri-Implantitis—A Systematic Review" Antibiotics 10, no. 11: 1350. https://doi.org/10.3390/antibiotics10111350
APA StyleJennes, M.-E., Naumann, M., Peroz, S., Beuer, F., & Schmidt, F. (2021). Antibacterial Effects of Modified Implant Abutment Surfaces for the Prevention of Peri-Implantitis—A Systematic Review. Antibiotics, 10(11), 1350. https://doi.org/10.3390/antibiotics10111350