Influence of Gait Speed on Inter-Joint Coordination in People with and Without Parkinson’s Disease

 ,
,  , , and
, , and 
Abstract
1. Introduction
2. Methods
2.1. Study Overview and Ethics
2.2. Participants
2.3. Data Collection
2.4. Walking Protocol
2.5. Data Processing
2.6. Joint Angle Extraction and Event Detection
2.7. Joint Excursion Calculation
2.8. Coordination and Coordination Variability Calculations
2.9. Statistical Analysis
3. Results
3.1. Results of ANCOVA for Impact of Gait Speed on Hip–Knee Coordination (MARP) and Hip–Knee Coordination Variability (DP), by Group
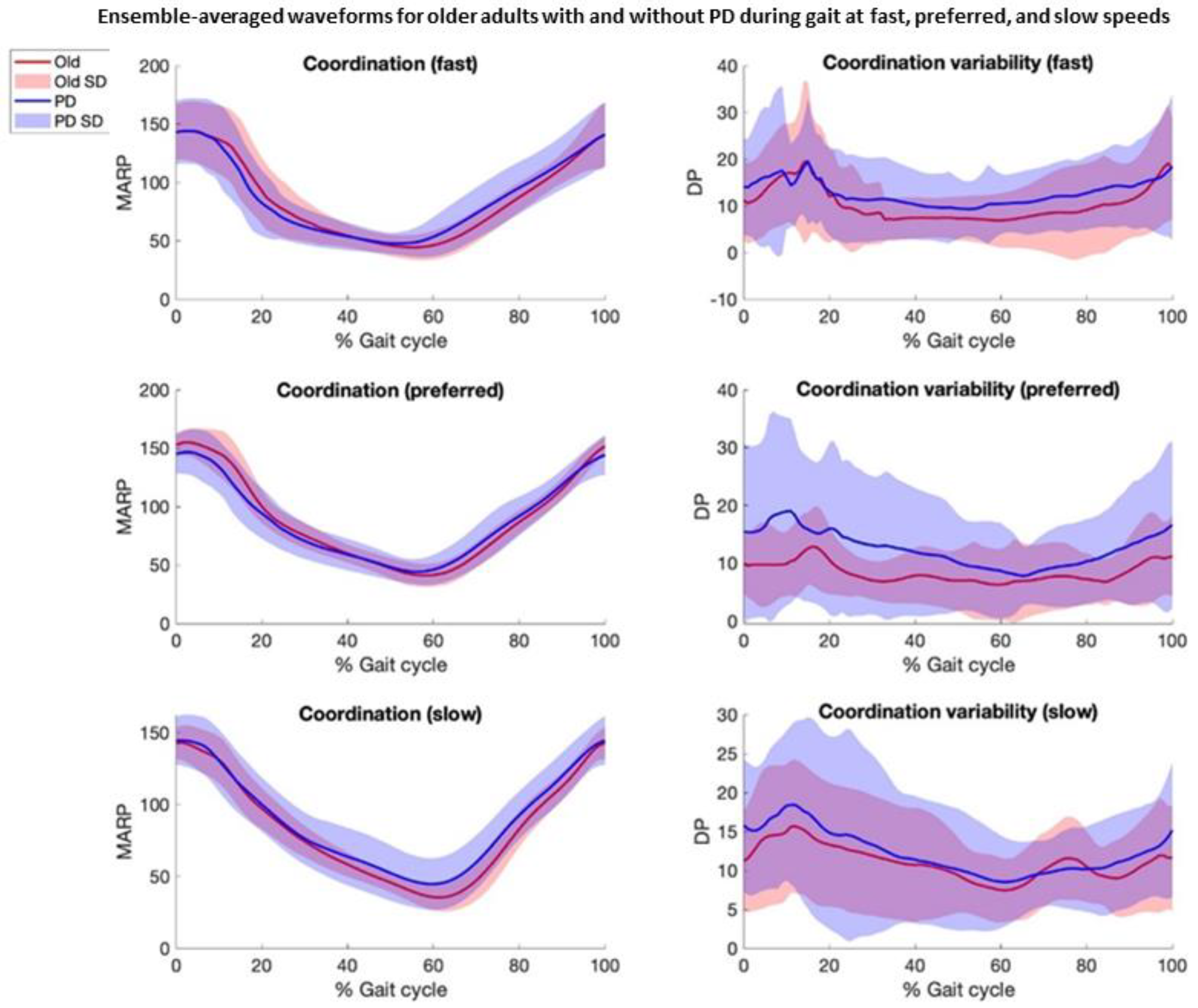
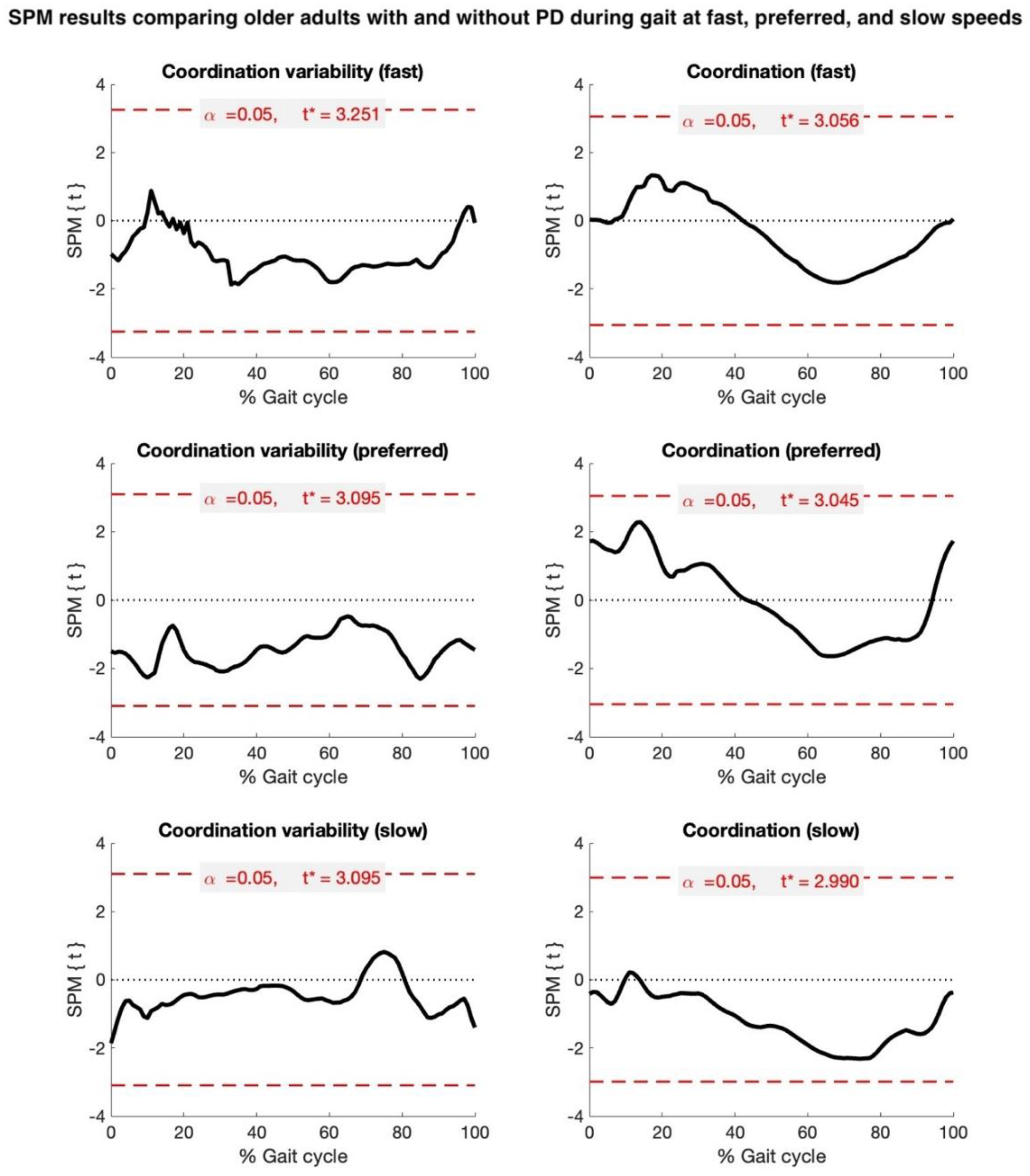
3.2. Analyses for Hip–Knee Coordination (MARP) and Hip–Knee Coordination Variability (DP)
3.3. Results of ANCOVA for Impact of Gait Speed on Hip and Knee Joint Excursion, by Group
4. Discussion
4.1. Gait Speed Does Not Significantly Influence Coordination Variability, Independent of Clinical Status
4.2. Joint Excursion During Gait Does Not Differ Between HOAs and pwPD
4.3. Clinical Implications
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef]
- Creaby, M.W.; Cole, M.H. Gait characteristics and falls in Parkinson’s disease: A systematic review and meta-analysis. Park. Relat. Disord. 2018, 57, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Allen, N.E.; Schwarzel, A.K.; Canning, C.G. Recurrent Falls in Parkinson’s Disease: A Systematic Review. Park. Dis. 2013, 2013, 906274. [Google Scholar] [CrossRef]
- Rahman, S.; Griffin, H.J.; Quinn, N.P.; Jahanshahi, M. Quality of life in Parkinson’s disease: The relative importance of the symptoms. Mov. Disord. 2008, 23, 1428–1434. [Google Scholar] [CrossRef] [PubMed]
- van de Port, I.; Kwakkel, G.; Lindeman, E. Community ambulation in patients with chronic stroke: How is it related to gait speed? J. Rehabil. Med. 2008, 40, 23–27. [Google Scholar] [CrossRef]
- Sanders, J.B.; Bremmer, M.A.; Comijs, H.C.; van de Ven, P.M.; Deeg, D.J.; Beekman, A.T. Gait Speed and processing speed as clinical markers for geriatric health outcomes. Am. J. Geriatr. Psychiatry 2017, 25, 374–385. [Google Scholar] [CrossRef]
- von der Recke, F.; Warmerdam, E.; Hansen, C.; Romijnders, R.; Maetzler, W. Reduced Range of Gait Speed: A Parkinson’s Disease-Specific Symptom? J. Park. Dis. 2023, 13, 197–202. [Google Scholar] [CrossRef]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.W.; Keller, A.; et al. Long-term unsupervised mobility assessment in movement disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Atrsaei, A.; Corrà, M.F.; Dadashi, F.; Vila-Chã, N.; Maia, L.; Mariani, B.; Maetzler, W.; Aminian, K. Gait speed in clinical and daily living assessments in Parkinson’s disease patients: Performance versus capacity. npj Park. Dis. 2021, 7, 24. [Google Scholar] [CrossRef]
- Zanardi, A.P.J.; da Silva, E.S.; Costa, R.R.; Passos-Monteiro, E.; dos Santos, I.O.; Kruel, L.F.M.; Peyré-Tartaruga, L.A. Gait parameters of Parkinson’s disease compared with healthy controls: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 752. [Google Scholar] [CrossRef] [PubMed]
- Van Emmerik, R.E.; Hamill, J.; McDermott, W.J. Variability and Coordinative Function in Human Gait. Quest 2005, 57, 102–123. [Google Scholar] [CrossRef]
- Krasovsky, T.; Levin, M.F. Review: Toward a Better Understanding of Coordination in Healthy and Poststroke Gait. Neurorehabilit. Neural Repair 2010, 24, 213–224. [Google Scholar] [CrossRef]
- Hamill, J.; Palmer, C.; Van Emmerik, R.E.A. Coordinative variability and overuse injury. BMC Sports Sci. Med. Rehabil. 2012, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- Stergiou, N.; Harbourne, R.T.; Cavanaugh, J.T. Optimal movement variability: A new theoretical perspective for neurologic physical therapy. J. Neurol. Phys. Ther. 2006, 30, 120–129. [Google Scholar] [CrossRef]
- Lukšys, D.; Jatužis, D.; Jonaitis, G.; Griškevičius, J. Application of continuous relative phase analysis for differentiation of gait in neurodegenerative disease. Biomed. Signal Process. Control. 2021, 67, 102558. [Google Scholar] [CrossRef]
- Hubble, R.P.; Naughton, G.A.; Silburn, P.A.; Cole, M.H. Wearable sensor use for assessing standing balance and walking stability in people with Parkinson’s disease: A systematic review. PLoS ONE 2015, 10, e0123705. [Google Scholar] [CrossRef]
- Zhao, H.; Cao, J.; Xie, J.; Liao, W.-H.; Lei, Y.; Cao, H.; Qu, Q.; Bowen, C. Wearable sensors and features for diagnosis of neurodegenerative diseases: A systematic review. Digit. Health 2023, 9, 20552076231173569. [Google Scholar] [CrossRef]
- Piau, A.; Mattek, N.; Crissey, R.; Beattie, Z.; Dodge, H.; Kaye, J. When Will My Patient Fall? Sensor-Based In-Home Walking Speed Identifies Future Falls in Older Adults. J. Gerontol. Ser. A 2020, 75, 968–973. [Google Scholar] [CrossRef]
- Saegner, K.; Romijnders, R.; Hansen, C.; Holder, J.; Warmerdam, E.; Maetzler, W. Inter-joint coordination with and without dopaminergic medication in Parkinson’s disease: A case-control study. J. Neuroeng. Rehabil. 2024, 21, 118. [Google Scholar] [CrossRef]
- Warmerdam, E.; Romijnders, R.; Geritz, J.; Elshehabi, M.; Maetzler, C.; Otto, J.C.; Reimer, M.; Stuerner, K.; Baron, R.; Paschen, S.; et al. Proposed mobility assessments with simultaneous full-body inertial measurement units and optical motion capture in healthy adults and neurological patients for future validation studies: Study protocol. Sensors 2021, 21, 5833. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Dixon, P.C.; Loh, J.J.; Michaud-Paquette, Y.; Pearsall, D.J. biomechZoo: An open-source toolbox for the processing, analysis, and visualization of biomechanical movement data. Comput. Methods Programs Biomed. 2017, 140, 1–10. [Google Scholar] [CrossRef]
- Schepers, M.; Giuberti, M.; Bellusci, G. Xsens MVN: Consistent tracking of human motion using inertial sensing. Xsens Technol. 2018, 1, 1–8. [Google Scholar]
- Valenti, R.G.; Dryanovski, I.; Xiao, J. Keeping a good attitude: A quaternion-based orientation filter for IMUs and MARGs. Sensors 2015, 15, 19302–19330. [Google Scholar] [CrossRef] [PubMed]
- Grood, E.S.; Suntay, W.J. A Joint Coordinate System for the clinical description of three-dimensional motions: Application to the knee. J. Biomech. Eng. 1983, 105, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Fadillioglu, C.; Stetter, B.J.; Ringhof, S.; Krafft, F.C.; Sell, S.; Stein, T. Automated gait event detection for a variety of locomotion tasks using a novel gyroscope-based algorithm. Gait Posture 2020, 81, 102–108. [Google Scholar] [CrossRef]
- Burgess-Limerick, R.; Abernethy, B.; Neal, R.J. Relative phase quantifies interjoint coordination. J. Biomech. 1993, 26, 91–94. [Google Scholar] [CrossRef]
- Lamb, P.F.; Stöckl, M. On the use of continuous relative phase: Review of current approaches and outline for a new standard. Clin. Biomech. 2014, 29, 484–493. [Google Scholar] [CrossRef]
- Stergiou, N. Innovative Analyses of Human Movement: Analytical Tools for Human Movement Research; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Kang, H.G.; Dingwell, J.B. Effects of walking speed, strength and range of motion on gait stability in healthy older adults. J. Biomech. 2008, 41, 2899–2905. [Google Scholar] [CrossRef] [PubMed]
- Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Common and distinct behavior among stride length, gait variability, and fractal-like scaling. Chaos Interdiscip. J. Nonlinear Sci. 2009, 19, 026113. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Age [Years] | Height [cm] | Weight [cm] | MOCA | SPPB | Slow [m/s] (# of Steps) | Preferred [m/s] (# of Steps) | Fast [m/s] (# of Steps) | |
|---|---|---|---|---|---|---|---|---|
| PD n = 24 10 ♀, 16 ♂ | 65 ± 9 | 174 ± 9 | 81 ± 16 | 24 ± 3 | 9.1 ± 2.1 | 0.65 ± 0.17 5 ± 2 | 0.97 ± 0.18 3 ± 1 | 1.19 ± 0.34 3 ± 1 |
| OA n = 19 11 ♀, 8 ♂ | 71 ± 7 | 173 ± 9 | 77 ± 17 | 25 ± 4 | 10.4 ± 1.7 | 0.67 ± 0.17 5 ± 1 | 1.07 ± 0.21 3 ± 1 | 1.45 ± 0.27 3 ± 1 |
| Gait Speed | Hip Joint Excursion | Knee Joint Excursion | ||
|---|---|---|---|---|
| Older Adults | pwPD | Older Adults | pwPD | |
| Slow | 34.6 (7.4) | 30.2 (7.4) | 59.6 (8.1) | 53.4 (8.4) |
| Preferred | 40.5 (7.6) | 34.5 (7.3) | 65.2 (8.6) | 55.3 (9.2) |
| Fast | 45.2 (7.6) | 39.5 (10.5) | 62.6 (9.7) | 55.5 (9.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ippersiel, P.; Dixon, P.C.; Warmerdam, E.; Romijnders, R.; Maetzler, W.; Hansen, C. Influence of Gait Speed on Inter-Joint Coordination in People with and Without Parkinson’s Disease. Biosensors 2025, 15, 367. https://doi.org/10.3390/bios15060367
Ippersiel P, Dixon PC, Warmerdam E, Romijnders R, Maetzler W, Hansen C. Influence of Gait Speed on Inter-Joint Coordination in People with and Without Parkinson’s Disease. Biosensors. 2025; 15(6):367. https://doi.org/10.3390/bios15060367
Chicago/Turabian StyleIppersiel, Patrick, Philippe C. Dixon, Elke Warmerdam, Robbin Romijnders, Walter Maetzler, and Clint Hansen. 2025. "Influence of Gait Speed on Inter-Joint Coordination in People with and Without Parkinson’s Disease" Biosensors 15, no. 6: 367. https://doi.org/10.3390/bios15060367
APA StyleIppersiel, P., Dixon, P. C., Warmerdam, E., Romijnders, R., Maetzler, W., & Hansen, C. (2025). Influence of Gait Speed on Inter-Joint Coordination in People with and Without Parkinson’s Disease. Biosensors, 15(6), 367. https://doi.org/10.3390/bios15060367