A Nanoparticle-Based Immunoassay on Facemasks for Evaluating Neutrophilic Airway Inflammation in COPD Patients

 , , , , , , , , ,
, , , , , , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Reagents
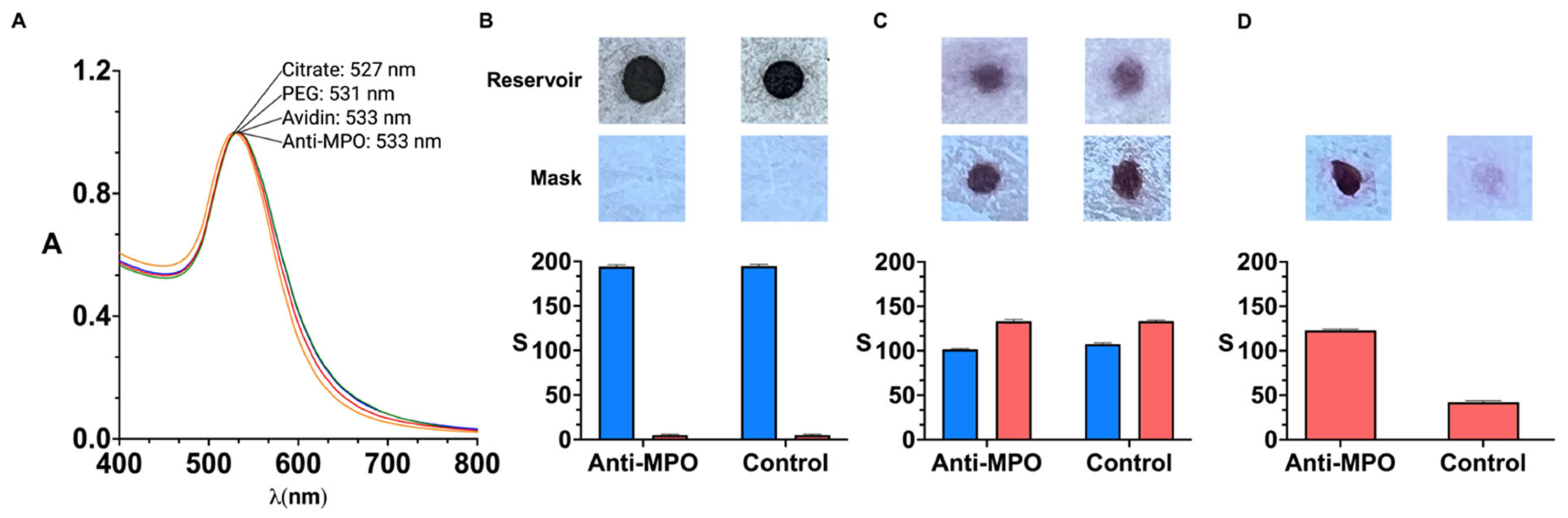
2.2. Antibody-Coated Nanoparticles
2.3. Manufacturing of Nanoparticle Reservoirs
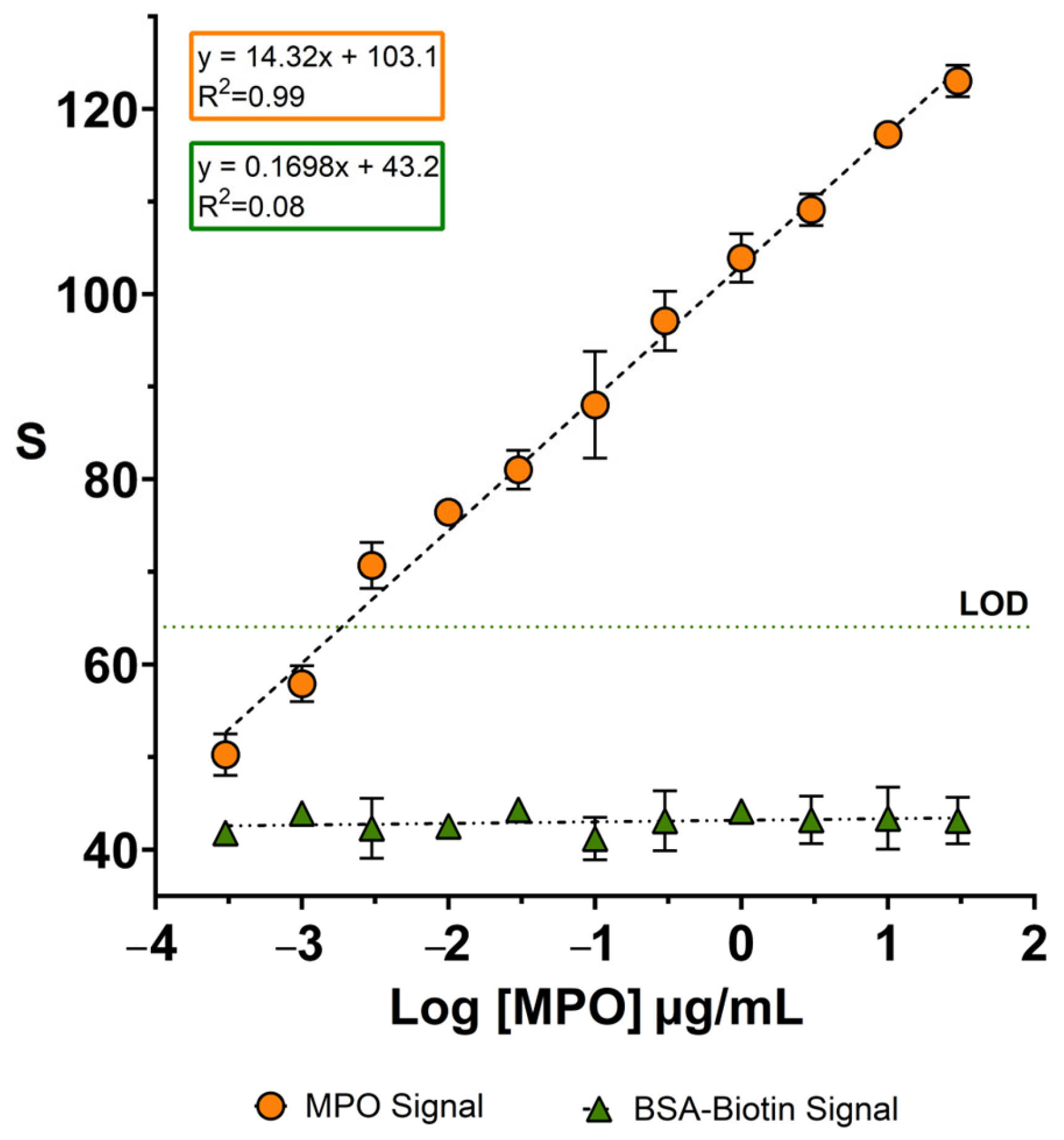
2.4. Calibration Experiments
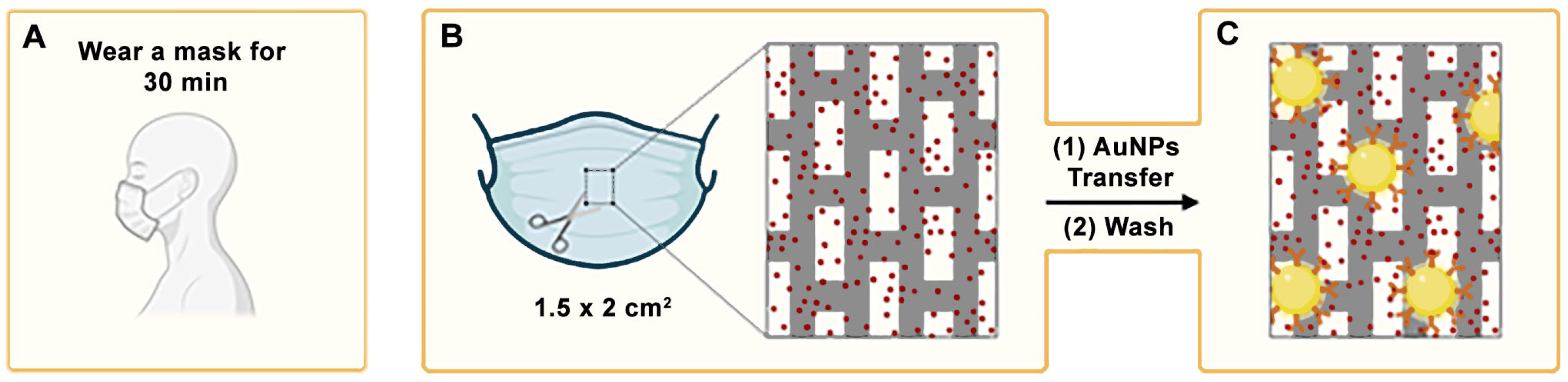
2.5. Analysis of Facemasks Worn by Patients
2.6. Study Design
2.7. Ethics Declarations
2.8. Inclusion and Exclusion Criteria
2.9. Clinical Data Collection
2.10. Statistical Analyses
2.11. Data Availability
3. Results and Discussion
4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COPD | Chronic obstructive pulmonary disease |
| MPO | Myeloperoxidase |
| PEG | Poly(ethyleneglycol) |
| LOD | Limit of detection |
| Sulfo-NHS | N-Hydroxysulfosuccinimide sodium salt |
| S | Colorimetric signal |
| Abs | Absorbance |
| BSA | Bovine serum albumin |
| PBS | Phosphate-buffered saline |
| SH-PEG-COOH | Poly(ethylene glycol) 2-mercaptoethyl ether acetic acid |
| EDC | 1-etil-3-(3-dimetilaminopropil)carbodiimida |
| PSS | Poly(4-styrenesulfonate) sodium salt |
| SD | Standard deviation |
| IQR | Interquartile ranges |
| LSPR | Localized surface plasmon resonance |
| NIR | Near-infrared |
| GOLD | Global Initiative for Chronic Obstructive Lung Disease |
| COPD-E | Chronic obstructive pulmonary disease patients with exacerbations |
| COPD-NE | Chronic obstructive pulmonary disease patients without exacerbations |
| WBC | White blood cell |
| BMI | Body mass index |
| DLCO | Diffusion Capacity of Carbon Monoxide |
| FEV1 | Forced expiratory volume in 1 s |
| FVC | Forced Vital Capacity |
| mMRC | Modified Medical Research Council |
| NA | Not assessed |
| PA | Pseudomonas aeruginosa |
References
- Boers, E.; Barrett, M.; Su, J.G.; Benjafield, A.V.; Sinha, S.; Kaye, L.; Zar, H.J.; Vuong, V.; Tellez, D.; Gondalia, R.; et al. Global Burden of Chronic Obstructive Pulmonary Disease Through 2050. JAMA Netw. Open 2023, 6, e2346598. [Google Scholar] [CrossRef] [PubMed]
- Gernez, Y.; Tirouvanziam, R.; Chanez, P. Neutrophils in Chronic Inflammatory Airway Diseases: Can We Target Them and How? Eur. Respir. J. 2010, 35, 467–469. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.J.; Sapey, E.; Stockley, R. Neutrophil Phenotypes in Chronic Lung Disease. Expert. Rev. Respir. Med. 2019, 13, 951–967. [Google Scholar] [CrossRef]
- Woodhead, M.; Blasi, F.; Ewig, S.; Garau, J.; Huchon, G.; Ieven, M.; Ortqvist, A.; Schaberg, T.; Torres, A.; van der Heijden, G.; et al. Guidelines for the Management of Adult Lower Respiratory Tract Infections—Full Version. Clin. Microbiol. Infect. 2011, 17, E1–E59. [Google Scholar] [CrossRef]
- 2024 GOLD Report. Available online: https://goldcopd.org/2024-gold-report/ (accessed on 21 October 2024).
- Wedzicha, J.A.; Seemungal, T.A. COPD Exacerbations: Defining Their Cause and Prevention. Lancet 2007, 370, 786–796. [Google Scholar] [CrossRef]
- Soler-Cataluña, J.J.; Martínez-García, M.A.; Román Sánchez, P.; Salcedo, E.; Navarro, M.; Ochando, R. Severe Acute Exacerbations and Mortality in Patients with Chronic Obstructive Pulmonary Disease. Thorax 2005, 60, 925–931. [Google Scholar] [CrossRef]
- Zhu, A.; Ge, D.; Zhang, J.; Teng, Y.; Yuan, C.; Huang, M.; Adcock, I.M.; Barnes, P.J.; Yao, X. Sputum Myeloperoxidase in Chronic Obstructive Pulmonary Disease. Eur. J. Med. Res. 2014, 19, 12. [Google Scholar] [CrossRef]
- Romero, P.V.; Rodríguez, B.; Martínez, S.; Cañizares, R.; Sepúlveda, D.; Manresa, F. Analysis of Oxidative Stress in Exhaled Breath Condensate From Patients With Severe Pulmonary Infections. Arch. Bronconeumol. 2006, 42, 113–119. [Google Scholar] [CrossRef]
- Tateosian, N.L.; Costa, M.J.; Guerrieri, D.; Barro, A.; Mazzei, J.A.; Eduardo Chuluyan, H. Inflammatory Mediators in Exhaled Breath Condensate of Healthy Donors and Exacerbated COPD Patients. Cytokine 2012, 58, 361–367. [Google Scholar] [CrossRef]
- Bayley, D.L.; Abusriwil, H.; Ahmad, A.; Stockley, R.A. Validation of Assays for Inflammatory Mediators in Exhaled Breath Condensate. Eur. Respir. J. 2008, 31, 943–948. [Google Scholar] [CrossRef]
- Davis, M.D.; Montpetit, A.; Hunt, J. Exhaled Breath Condensate: An Overview. Immunol. Allergy Clin. North. Am. 2012, 32, 363–375. [Google Scholar] [CrossRef]
- Chow, S.; Yates, D.H.; Thomas, P.S. Reproducibility of Exhaled Breath Condensate Markers. Eur. Respir. J. 2008, 32, 1124–1126. [Google Scholar] [CrossRef] [PubMed]
- Vaquer, A.; Adrover-Jaume, C.; Clemente, A.; Iglesias, A.; López, M.; Martínez, R.; Roig, I.M.; Cosío, B.G.; de la Rica, R. Immunosensors Made of Polymer-Infused Porous Paper for the Non-Invasive Detection of Airways Cytokines Trapped by Porous Face Masks. Sens. Actuators B Chem. 2023, 379, 133233. [Google Scholar] [CrossRef]
- Delgado-Cano, D.; Clemente, A.; Adrover-Jaume, C.; Vaquer, A.; López, M.; Martínez, R.; Roig, I.M.; Iglesias, A.; Cosío, B.G.; Rica, R. de la Facemask Analyses for the Non-Invasive Detection of Chronic and Acute P. Aeruginosa Lung Infections Using Nanoparticle-Based Immunoassays. Analyst 2023, 148, 4837–4843. [Google Scholar] [CrossRef]
- Vaquer, A.; Alba-Patiño, A.; Adrover-Jaume, C.; Russell, S.M.; Aranda, M.; Borges, M.; Mena, J.; Del Castillo, A.; Socias, A.; Martín, L.; et al. Nanoparticle Transfer Biosensors for the Non-Invasive Detection of SARS-CoV-2 Antigens Trapped in Surgical Face Masks. Sens. Actuators B Chem. 2021, 345, 130347. [Google Scholar] [CrossRef]
- Xue, Q.; Kan, X.; Pan, Z.; Li, Z.; Pan, W.; Zhou, F.; Duan, X. An Intelligent Face Mask Integrated with High Density Conductive Nanowire Array for Directly Exhaled Coronavirus Aerosols Screening. Biosens. Bioelectron. 2021, 186, 113286. [Google Scholar] [CrossRef]
- Kim, J.-H.; Marcus, C.; Ono, R.; Sadat, D.; Mirzazadeh, A.; Jens, M.; Fernandez, S.; Zheng, S.; Durak, T.; Dagdeviren, C. A Conformable Sensory Face Mask for Decoding Biological and Environmental Signals. Nat. Electron. 2022, 5, 794–807. [Google Scholar] [CrossRef]
- Zhang, K.; Li, Z.; Zhang, J.; Zhao, D.; Pi, Y.; Shi, Y.; Wang, R.; Chen, P.; Li, C.; Chen, G.; et al. Biodegradable Smart Face Masks for Machine Learning-Assisted Chronic Respiratory Disease Diagnosis. ACS Sens. 2022, 7, 3135–3143. [Google Scholar] [CrossRef]
- Alba-Patiño, A.; Adrover-Jaume, C.; de la Rica, R. Nanoparticle Reservoirs for Paper-Only Immunosensors. ACS Sens. 2020, 5, 147–153. [Google Scholar] [CrossRef]
- Clemente, A.; Alba-Patiño, A.; Rojo-Molinero, E.; Russell, S.M.; Borges, M.; Oliver, A.; de la Rica, R. Rapid Detection of Pseudomonas Aeruginosa Biofilms via Enzymatic Liquefaction of Respiratory Samples. ACS Sens. 2020, 5, 3956–3963. [Google Scholar] [CrossRef]
- Anthonisen, N.R.; Manfreda, J.; Warren, C.P.; Hershfield, E.S.; Harding, G.K.; Nelson, N.A. Antibiotic Therapy in Exacerbations of Chronic Obstructive Pulmonary Disease. Ann. Intern. Med. 1987, 106, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Murray, P.R.; Washington, J.A. Microscopic and Baceriologic Analysis of Expectorated Sputum. Mayo Clin. Proc. 1975, 50, 339–344. [Google Scholar] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. Available online: https://goldcopd.org/ (accessed on 19 September 2024).
- Casanova, C.; Marin, J.M.; Martinez-Gonzalez, C.; de Lucas-Ramos, P.; Mir-Viladrich, I.; Cosio, B.; Peces-Barba, G.; Solanes-García, I.; Agüero, R.; Feu-Collado, N.; et al. Differential Effect of Modified Medical Research Council Dyspnea, COPD Assessment Test, and Clinical COPD Questionnaire for Symptoms Evaluation Within the New GOLD Staging and Mortality in COPD. Chest 2015, 148, 159–168. [Google Scholar] [CrossRef]
- de la Escosura-Muñiz, A.; Parolo, C.; Merkoçi, A. Immunosensing Using Nanoparticles. Mater. Today 2010, 13, 24–34. [Google Scholar] [CrossRef]
- Manson, J.; Kumar, D.; Meenan, B.J.; Dixon, D. Polyethylene Glycol Functionalized Gold Nanoparticles: The Influence of Capping Density on Stability in Various Media. Gold. Bull. 2011, 44, 99–105. [Google Scholar] [CrossRef]
- Rahme, K.; Chen, L.; Hobbs, R.G.; Morris, M.A.; O’Driscoll, C.; Holmes, J.D. PEGylated Gold Nanoparticles: Polymer Quantification as a Function of PEG Lengths and Nanoparticle Dimensions. RSC Adv. 2013, 3, 6085–6094. [Google Scholar] [CrossRef]
- Aaron, S.D.; Angel, J.B.; Lunau, M.; Wright, K.; Fex, C.; Le Saux, N.; Dales, R.E. Granulocyte Inflammatory Markers and Airway Infection during Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2001, 163, 349–355. [Google Scholar] [CrossRef]
- Bathoorn, E.; Liesker, J.J.W.; Postma, D.S.; Koëter, G.H.; van der Toorn, M.; van der Heide, S.; Ross, H.A.; van Oosterhout, A.J.M.; Kerstjens, H.A.M. Change in Inflammation in Out-Patient COPD Patients from Stable Phase to a Subsequent Exacerbation. Int. J. Chron. Obs. Pulmon. Dis. 2009, 4, 101–109. [Google Scholar] [CrossRef]
- Mulvanny, A.; Pattwell, C.; Beech, A.; Southworth, T.; Singh, D. Validation of Sputum Biomarker Immunoassays and Cytokine Expression Profiles in COPD. Biomedicines 2022, 10, 1949. [Google Scholar] [CrossRef]
- Gutiérrez-Capitán, M.; Sanchís, A.; Carvalho, E.O.; Baldi, A.; Vilaplana, L.; Cardoso, V.F.; Calleja, Á.; Wei, M.; de la Rica, R.; Hoyo, J.; et al. Engineering a Point-of-Care Paper-Microfluidic Electrochemical Device Applied to the Multiplexed Quantitative Detection of Biomarkers in Sputum. ACS Sens. 2023, 8, 3032–3042. [Google Scholar] [CrossRef]
- Iwamoto, H.; Gao, J.; Koskela, J.; Kinnula, V.; Kobayashi, H.; Laitinen, T.; Mazur, W. Differences in Plasma and Sputum Biomarkers between COPD and COPD-Asthma Overlap. Eur. Respir. J. 2014, 43, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Jiang, E.; Fu, Y.; Wang, Y.; Ying, L.; Li, W. The Role and Clinical Significance of Myeloperoxidase (MPO) and TNF-α in Prognostic Evaluation of T-COPD. BMC Pulm. Med. 2025, 25, 192. [Google Scholar] [CrossRef] [PubMed]
- Holz, O.; Müller, M.; Carstensen, S.; Olin, A.-C.; Hohlfeld, J.M. Inflammatory Cytokines Can Be Monitored in Exhaled Breath Particles Following Segmental and Inhalation Endotoxin Challenge in Healthy Volunteers. Sci. Rep. 2022, 12, 5620. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Deng, N.; Chen, Q.; Yu, H.; Ding, X.; Hu, S.; Nie, H. Application of Inflammatory Markers in Induced Sputum in Stable Chronic Obstructive Pulmonary Disease Patients with Positive Bronchodilation Tests. Curr. Med. Sci. 2019, 39, 560–567. [Google Scholar] [CrossRef]
- Liu, B.; Lu, L. Amperometric Sandwich Immunoassay for Determination of Myeloperoxidase by Using Gold Nanoparticles Encapsulated in Graphitized Mesoporous Carbon. Microchim. Acta 2019, 186, 262. [Google Scholar] [CrossRef]
- Miravitlles, M.; Kruesmann, F.; Haverstock, D.; Perroncel, R.; Choudhri, S.H.; Arvis, P. Sputum Colour and Bacteria in Chronic Bronchitis Exacerbations: A Pooled Analysis. Eur. Respir. J. 2012, 39, 1354–1360. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| COPD-E | COPD-NE | Control | p-Value | |
|---|---|---|---|---|
| Total patients | 8 | 14 | 21 | |
| Age, mean ± SD | 72.7 ± 7.3 | 69.2 ± 4.7 | 41.4 ± 5.5 | <0.0001 * |
| Sex, n (%) | 0.15 | |||
| Male | 7 (87.5) | 8 (57.1) | 10 (47.6) | |
| Female | 1 (12.5) | 6 (42.8) | 11 (52.4) | |
| Active smoking, n (%) | 0.001 * | |||
| Yes | 1 (12.5) | 5 (35.7) | 5 (23.8) | |
| No # | 7 (87.5) | 9 (64.3) | 5 (23.8) | |
| Never smoker | 0 | 0 | 11 (52.4) | |
| Smoking index (pack–years), median (IQR) | 50 (50–80) | 47.5 (40–71.2) | 1.4 (0.7–4) | <0.0001 * |
| BMI (kg/m2), mean ± SD | 24.5 ± 5 | 27.3 ± 4.7 | 24.7 ± 4.5 | 0.3775 |
| Dyspnea level (mMRC scale), median (IQR) | 3 (2.2–3) | 2 (2–3) | NA | 0.3528 |
| Airflow limitation severity (GOLD), n (%) | 0.6613 | |||
| GOLD 2 | 1 (12.5) | 4 (28.5) | NA | |
| GOLD 3 | 3 (37.5) | 4 (28.5) | NA | |
| GOLD 4 | 3 (37.5) | 4 (28.5) | NA | |
| Lung function, mean ± SD | ||||
| FVCpost (% predicted) | 78.8 ± 20.6 | 67.7 ± 26.8 | 100.4 ± 15.1 | 0.0003 * |
| FEV1post (% predicted) | 34.8 ± 15.3 | 41 ± 17.9 | 104.8 ± 13.7 | <0.0001 * |
| FEV1/FVCpost | 32.7 ± 9.4 | 40.1 ± 9.2 | 83.7 ± 4.6 | <0.0001 * |
| DLCO (% predicted) | 46.8 ± 32.3 | 36.7 ± 10.7 | 92.2 ± 12.6 | <0.0001 * |
| PaO2 (mmHg) | 66 (66–66) | 66.5 (45–79) | NA | 0.8473 |
| PaCO2 (mmHg) | 51 (43–59) | 45 (44–50) | NA | 0.6415 |
| Laboratory values, mean ± SD | ||||
| WBC (·109/L) | 10 ± 4.5 | 9.7 ± 2.6 | 5.9 ± 1.1 | <0.0001 * |
| Neutrophils (·109/L) | 7.2 ± 4.9 | 6.6 ± 2.3 | 3.2 ± 0.6 | <0.0001 * |
| Neutrophils (%) | 68.6 ± 15.6 | 68 ± 9.4 | 53.9 ± 9.2 | 0.0004 * |
| Eosinophils (·109/L) | 0.1 ± 0.2 | 0.2 ± 0.1 | 0.1 ± 0.07 | 0.4870 |
| Eosinophils (%) | 2.2 ± 2.5 | 2.2 ± 1.8 | 2.6 ± 1.5 | 0.8045 |
| C-reactive protein (mg/dL) | 0.09 ± 0.07 | 1.4 ± 2.1 | 0.1 ± 0.1 | 0.1492 |
| Allergies, n (%) | 0 | 3 (21.4) | 7 (33.3) | 0.7041 |
| Bronchiectasis, n (%) | 1 (12.5) | 5 (35.7) | 0 | 0.3512 |
| PA colonization, n (%) | 1 (12.5) | 4 (28.5) | NA | 0.6130 |
| Other pathogen colonization, n (%) | 2 (25) | 3 (21.4) | NA | >0.9999 |
| MPO levels, mean ± SD | 172.7 ± 8.6 | 125.8 ± 4.2 | 72 ± 7.5 | <0.0001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mestre, B.; Toledo-Pons, N.; Vaquer, A.; Tejada, S.; Clemente, A.; Iglesias, A.; López, M.; Engonga, R.; Perelló, S.; Cosío, B.G.; et al. A Nanoparticle-Based Immunoassay on Facemasks for Evaluating Neutrophilic Airway Inflammation in COPD Patients. Biosensors 2025, 15, 323. https://doi.org/10.3390/bios15050323
Mestre B, Toledo-Pons N, Vaquer A, Tejada S, Clemente A, Iglesias A, López M, Engonga R, Perelló S, Cosío BG, et al. A Nanoparticle-Based Immunoassay on Facemasks for Evaluating Neutrophilic Airway Inflammation in COPD Patients. Biosensors. 2025; 15(5):323. https://doi.org/10.3390/bios15050323
Chicago/Turabian StyleMestre, Bartomeu, Nuria Toledo-Pons, Andreu Vaquer, Sofia Tejada, Antonio Clemente, Amanda Iglesias, Meritxell López, Ruth Engonga, Sabina Perelló, Borja G. Cosío, and et al. 2025. "A Nanoparticle-Based Immunoassay on Facemasks for Evaluating Neutrophilic Airway Inflammation in COPD Patients" Biosensors 15, no. 5: 323. https://doi.org/10.3390/bios15050323
APA StyleMestre, B., Toledo-Pons, N., Vaquer, A., Tejada, S., Clemente, A., Iglesias, A., López, M., Engonga, R., Perelló, S., Cosío, B. G., & de la Rica, R. (2025). A Nanoparticle-Based Immunoassay on Facemasks for Evaluating Neutrophilic Airway Inflammation in COPD Patients. Biosensors, 15(5), 323. https://doi.org/10.3390/bios15050323