A Comparison of Normalization Techniques for Individual Baseline-Free Estimation of Absolute Hypovolemic Status Using a Porcine Model


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection and Feature Extraction
2.1.1. ABVS Dataset
- (1)
- (2)
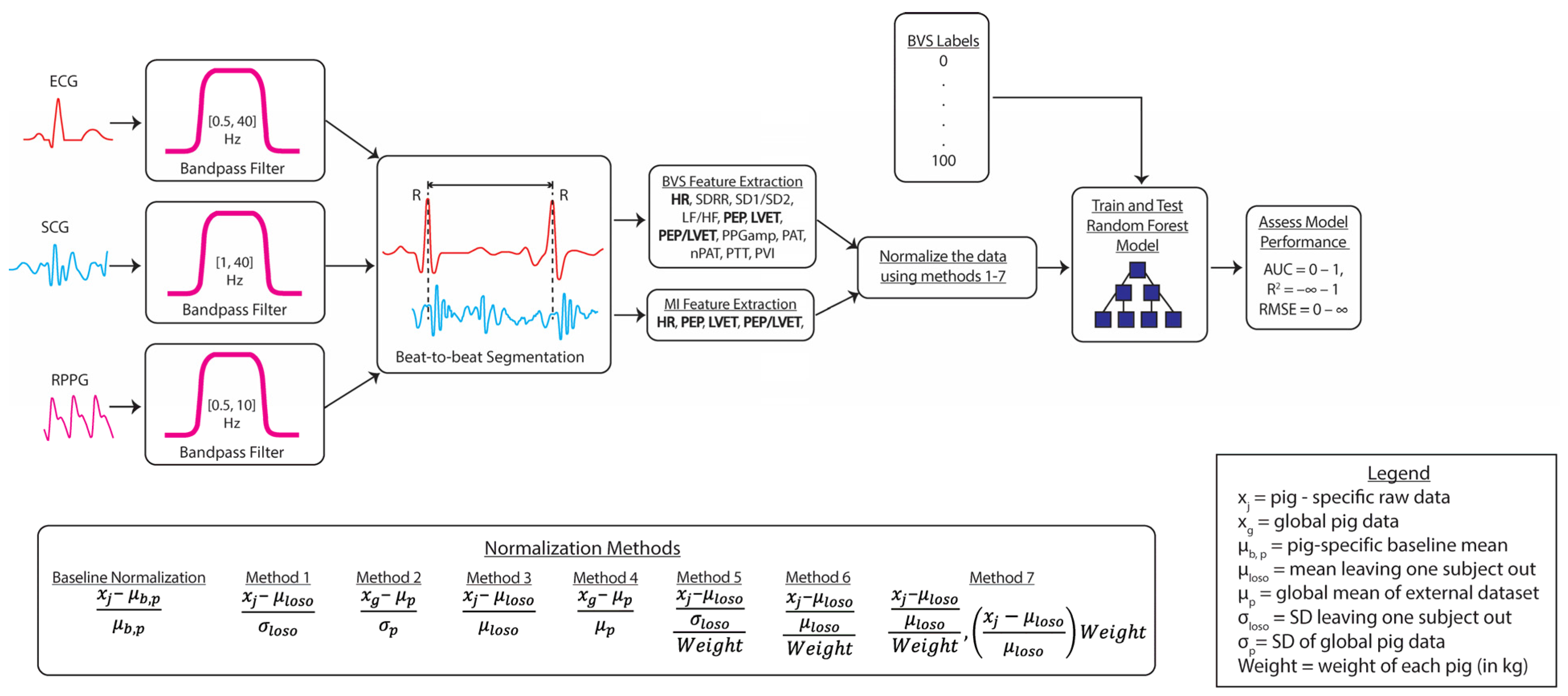
- SCG features: left ventricular ejection time (LVET). Rationale: exhibits strong correlations with measures of ventricular function. Additional information is included in [17];
- (3)
- RPPG features: RPPG amplitude (PPGamp) and pleth variability index (PVI). Rationale: Typically estimates blood pressure, fluid responsiveness, and vascular tone [17];
- (4)
- Cross-domain features: the following features required more than one signal to compute: pre-ejection period (PEP), PEP/LVET, pulse arrival time (PAT), HR-normalized PAT (nPAT), and pulse transit time (PTT). Rationale: (1) exhibits strong correlations with measures of ventricular function (PEP and PEP/LVET) and (2) estimate blood pressure, fluid responsiveness, and vascular tone (PAT, nPAT, and PTT) [17].
2.1.2. Myocardial Infarction Dataset
2.2. Normalization Methods
2.3. Training and Testing the Model
2.3.1. Model Label Assignment
2.3.2. Model Evaluation and Function
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Melendez Rivera, J.G.; Anjum, F. Hypovolemia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Airapetian, N.; Maizel, J.; Slama, M. Diagnosis of Central Hypovolemia in a Spontaneously Breathing Patient. In Intensive Care Medicine; Vincent, J.-L., Ed.; Springer: New York, NY, USA, 2007; pp. 520–530. [Google Scholar]
- Noori, S.; Azhibekov, T.; Lee, B.; Seri, I. 51—Cardiovascular Compromise in the Newborn. In Avery’s Diseases of the Newborn, 10th ed.; Gleason, C.A., Juul, S.E., Eds.; Elsevier: Philadelphia, PA, USA, 2018; pp. 741.e6–767.e6. [Google Scholar]
- Noel-Morgan, J.; Muir, W.W. Anesthesia-Associated Relative Hypovolemia: Mechanisms, Monitoring, and Treatment Considerations. Front. Vet. Sci. 2018, 5, 53. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, S.; Nassar, A.K.; Askari, R. Hypovolemic Shock. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Nuccio, R.P.; Barnes, K.A.; Carter, J.M.; Baker, L.B. Fluid Balance in Team Sport Athletes and the Effect of Hypohydration on Cognitive, Technical, and Physical Performance. Sports Med. 2017, 47, 1951–1982. [Google Scholar] [CrossRef] [PubMed]
- Schlader, Z.J.; Chapman, C.L.; Sarker, S.; Russo, L.; Rideout, T.C.; Parker, M.D.; Johnson, B.D.; Hostler, D. Firefighter Work Duration Influences the Extent of Acute Kidney Injury. Med. Sci. Sports Exerc. 2017, 49, 8. [Google Scholar] [CrossRef] [PubMed]
- Kimball, J.P.; Inan, O.T.; Convertino, V.A.; Cardin, S.; Sawka, M.N. Wearable Sensors and Machine Learning for Hypovolemia Problems in Occupational, Military and Sports Medicine: Physiological Basis, Hardware and Algorithms. Sensors 2022, 22, 442. [Google Scholar] [CrossRef] [PubMed]
- Kreimeier, U. Pathophysiology of fluid imbalance. Crit. Care 2000, 4, S3. [Google Scholar] [CrossRef] [PubMed]
- Hooper, N.; Armstrong, T.J. Hemorrhagic Shock. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Foucher, C.D.; Tubben, R.E. Lactic Acidosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Elhassan, M.G.; Chao, P.W.; Curiel, A. The Conundrum of Volume Status Assessment: Revisiting Current and Future Tools Available for Physicians at the Bedside. Cureus 2021, 13, e15253. [Google Scholar] [CrossRef] [PubMed]
- Quantitative Blood Loss in Obstetric Hemorrhage: ACOG Committee Opinion, Number 794. Obstet. Gynecol. 2019, 134, 6.
- Clifford, C.C. Treating traumatic bleeding in a combat setting. Mil. Med. 2004, 169 (Suppl. 12), 8–10. [Google Scholar] [CrossRef][Green Version]
- Hansen, B. Fluid Overload. Front. Vet. Sci. 2021, 8, 668688. [Google Scholar] [CrossRef]
- Mandal, M. Ideal resuscitation fluid in hypovolemia: The quest is on and miles to go. Int. J. Crit. Illn. Inj. Sci. 2016, 6, 54–55. [Google Scholar] [CrossRef]
- Kimball, J.P.; Zia, J.S.; An, S.; Rolfes, C.; Hahn, J.-O.; Sawka, M.N.; Inan, O.T. Unifying the Estimation of Blood Volume Decompensation Status in a Porcine Model of Relative and Absolute Hypovolemia Via Wearable Sensing. IEEE J. Biomed. Health Inf. 2021, 25, 3351–3360. [Google Scholar] [CrossRef] [PubMed]
- Suresh, M.R.; Chung, K.K.; Schiller, A.M.; Holley, A.B.; Howard, J.T.; Convertino, V.A. Unmasking the Hypovolemic Shock Continuum: The Compensatory Reserve. J. Intensive Care Med. 2019, 34, 696–706. [Google Scholar] [CrossRef]
- Schauer, S.G.; April, M.D.; Arana, A.A.; Maddry, J.K.; Escandon, M.A.; Linscomb, C.D.; Rodriguez, D.C.; Convertino, V.A. Efficacy of the compensatory reserve measurement in an emergency department trauma population. Transfusion 2021, 61 (Suppl. 1), S174–S182. [Google Scholar] [CrossRef] [PubMed]
- Convertino, V.A.; Sawka, M.N. Wearable technology for compensatory reserve to sense hypovolemia. J. Appl. Physiol. 2018, 124, 442–451. [Google Scholar] [CrossRef]
- Schlotman, T.E.; Howard, J.; Suresh, M.; Koons, N.J.; Schiller, A.; Convertino, V. Measures of Compensatory Reserve are More Sensitive and Specific than Heart Rate Variability as Early Predictors of Hemodynamic Decompensation. FASEB J. 2019, 33, 838.9. [Google Scholar] [CrossRef]
- Convertino, V.A.; Hinojosa-Laborde, C.; Muniz, G.W.; Carter, R., 3rd. Integrated Compensatory Responses in a Human Model of Hemorrhage. J. Vis. Exp. 2016, 117. [Google Scholar] [CrossRef]
- Convertino, V.A.; Schauer, S.G.; Weitzel, E.K.; Cardin, S.; Stackle, M.E.; Talley, M.J.; Sawka, M.N.; Inan, O.T. Wearable Sensors Incorporating Compensatory Reserve Measurement for Advancing Physiological Monitoring in Critically Injured Trauma Patients. Sensors 2020, 20, 6413. [Google Scholar] [CrossRef]
- Gupta, J.F.; Arshad, S.H.; Telfer, B.A.; Snider, E.J.; Convertino, V.A. Noninvasive Monitoring of Simulated Hemorrhage and Whole Blood Resuscitation. Biosensors 2022, 12, 1168. [Google Scholar] [CrossRef]
- Gupta, J.F.; Telfer, B.A.; Convertino, V.A. Feature Importance Analysis for Compensatory Reserve to Predict Hemorrhagic Shock. In Proceedings of the 44th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Glasgow, UK, 11–15 July 2022; pp. 1747–1752. [Google Scholar] [CrossRef]
- Bedolla, C.N.; Gonzalez, J.M.; Vega, S.J.; Convertino, V.A.; Snider, E.J. An Explainable Machine-Learning Model for Compensatory Reserve Measurement: Methods for Feature Selection and the Effects of Subject Variability. Bioengineering 2023, 10, 612. [Google Scholar] [CrossRef]
- Heikenfeld, J.; Jajack, A.; Rogers, J.; Gutruf, P.; Tian, L.; Pan, T.; Li, R.; Khine, M.; Kim, J.; Wang, J.; et al. Wearable sensors: Modalities, challenges, and prospects. Lab Chip 2018, 18, 217–248. [Google Scholar] [CrossRef]
- Etemadi, M.; Inan, O.T.; Heller, J.A.; Hersek, S.; Klein, L.; Roy, S. A Wearable Patch to Enable Long-Term Monitoring of Environmental, Activity and Hemodynamics Variables. IEEE Trans. Biomed. Circuits Syst. 2016, 10, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Zia, J.; Kimball, J.; Rolfes, C.; Hahn, J.-O.; Inan, O.T. Enabling the assessment of trauma-induced hemorrhage via smart wearable systems. Sci. Adv. 2020, 6, eabb1708. [Google Scholar] [CrossRef] [PubMed]
- Ali, P.J.M.; Faraj, R.H.; Koya, E. Data normalization and standardization: A technical report. Mach. Learn. Tech. Rep. 2014, 1, 1–6. [Google Scholar]
- Singh, D.; Singh, B. Feature wise normalization: An effective way of normalizing data. Pattern Recognit. 2022, 122, 108307. [Google Scholar] [CrossRef]
- Javaheri, S.H.; Sepehri, M.M.; Teimourpour, B. Chapter 6—Response Modeling in Direct Marketing: A Data Mining-Based Approach for Target Selection. In Data Mining Applications with R; Zhao, Y., Cen, Y., Eds.; Academic Press: Boston, MA, USA, 2014; pp. 153–180. [Google Scholar]
- Ogasawara, E.; Martinez, L.C.; de Oliveira, D.; Zimbrão, G.; Pappa, G.L.; Mattoso, M. Adaptive Normalization: A novel data normalization approach for non-stationary time series. In Proceedings of the 2010 International Joint Conference on Neural Networks (IJCNN), Barcelona, Spain, 18–23 July 2010; pp. 1–8. [Google Scholar] [CrossRef]
- Vricella, L.K.; Louis, J.M.; Chien, E.; Mercer, B.M. Blood volume determination in obese and normal-weight gravidas: The hydroxyethyl starch method. Am. J. Obstet. Gynecol. 2015, 213, 408.e1–408.e6. [Google Scholar] [CrossRef]
- Alba, B.K.; Castellani, J.W.; Charkoudian, N. Cold-induced cutaneous vasoconstriction in humans: Function, dysfunction and the distinctly counterproductive. Exp. Physiol. 2019, 104, 1202–1214. [Google Scholar] [CrossRef]
- Castellani, J.W.; Young, A.J. Human physiological responses to cold exposure: Acute responses and acclimatization to prolonged exposure. Auton. Neurosci. 2016, 196, 63–74. [Google Scholar] [CrossRef]
- Zhao, T.; Zheng, Y.; Wu, Z. Improving computational efficiency of machine learning modeling of nonlinear processes using sensitivity analysis and active learning. Digit. Chem. Eng. 2022, 3, 100027. [Google Scholar] [CrossRef]
- Patil, D.; Wadhvani, R.; Shukla, S.; Gupta, M. Adaptive wind data normalization to improve the performance of forecasting models. Wind. Eng. 2022, 46, 1606–1617. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Sex | CM | CM | CM | F | F | F |
| Age (days) | 150 | 131 | 118 | 118 | 133 | 114 |
| Weight (kg) | 71.4 | 65.4 | 54.5 | 60 | 66.5 | 60.5 |
| HR (bpm) | 84 | 59 | 70 | 67 | 79 | 93 |
| CO (L/min) | 4.5 | 4.2 | 2.9 | 4.3 | 4.9 | 5.8 |
| Est. Blood Volume (L) | 4.6 | 4.3 | 3.5 | 4.3 | 3.3 | 3.3 |
| AoP S/D (mmHg) | 90/45 | 93/52 | 104/56 | 72/32 | 83/34 | 88/49 |
| Normalization Methods | Features | |||||||
|---|---|---|---|---|---|---|---|---|
| HR | PEP | LVET | PEP/LVET | |||||
| ρ | p | ρ | p | ρ | p | ρ | p | |
| Z-Score | 0.90 | 0 | 0.57 | 0 | 0.94 | 0 | 0.57 | 0 |
| Min–Max | 0.90 | 0 | 0.57 | 0 | 0.94 | 0 | 0.57 | 0 |
| Decimal Scaling | 0.90 | 0 | 0.57 | 0 | 0.94 | 0 | 0.57 | 0 |
| Method Name | Features | Method Equation | R2 | AUC | RMSE (%) |
|---|---|---|---|---|---|
| 12-feature model w/IBN | HR, SDRR, SD1/SD2, LF/HF, PEP, LVET, PEP/LVET, PPGamp, PAT, PTT, nPAT, and PVI | 0.86 | 0.89 | 21.20 | |
| 12-feature model w/o IBN | HR, SDRR, SD1/SD2, LF/HF, PEP, LVET, PEP/LVET, PPGamp, PAT, PTT, nPAT, and PVI | 0.91 | 0.89 | 29.02 | |
| 1-feature model w/IBN | PEP/LVET | 0.82 | 0.81 | 22.31 | |
| 1-feature model w/o IBN | PEP/LVET | 0.25 | 0.58 | 40.39 | |
| 2-feature model w/IBN | PEP/LVET, HR | 0.84 | 0.88 | 22.10 | |
| 2-feature model w/o IBN | PEP/LVET, HR | 0.78 | 0.83 | 34.32 | |
| 2-feature model w/IBN | PEP/LVET, SDRR | 0.78 | 0.87 | 23.92 | |
| 2-feature model w/o IBN | PEP/LVET, SDRR | 0.83 | 0.82 | 34.53 | |
| 3-feature model w/IBN | PEP/LVET, HR, and LVET | 0.86 | 0.90 | 21.25 | |
| 3-feature model w/o IBN | PEP/LVET, HR, and LVET | 0.92 | 0.84 | 29.39 | |
| 3-feature model w/IBN | PEP/LVET, SDRR, and LVET | 0.78 | 0.87 | 23.82 | |
| 3-feature model w/o IBN | PEP/LVET, SDRR, and LVET | 0.78 | 0.85 | 35.39 | |
| 4-feature model w/IBN *** | HR, PEP, LVET, and PEP/LVET | 0.90 | 0.92 | 19.47 | |
| 4-feature model w/o IBN | HR, PEP, LVET, and PEP/LVET | 0.81 | 0.85 | 28.96 | |
| 4-feature model w/IBN | HR, SDRR, LVET, and PEP/LVET | 0.80 | 0.89 | 23.07 | |
| 4-feature model w/o IBN | HR, SDRR, LVET, and PEP/LVET | 0.92 | 0.87 | 33.36 | |
| 5-feature model w/IBN | HR, SDRR, PEP, LVET, and PEP/LVET | 0.86 | 0.91 | 21.24 | |
| 5-feature model w/o IBN | HR, SDRR, PEP, LVET, and PEP/LVET | 0.90 | 0.88 | 30.09 | |
| 6-feature model w/IBN | HR, SDRR, SD1/SD2, PEP, LVET, and PEP/LVET | 0.84 | 0.89 | 22.32 | |
| 6-feature model w/o IBN | HR, SDRR, SD1/SD2, PEP, LVET, and PEP/LVET | 0.94 | 0.89 | 28.77 | |
| 7-feature model w/IBN | HR, SDRR, SD1/SD2, LF/HF, PEP, LVET, and PEP/LVET | 0.83 | 0.89 | 22.73 | |
| 7-feature model w/o IBN | HR, SDRR, SD1/SD2, LF/HF, PEP, LVET, and PEP/LVET | 0.91 | 0.89 | 30.22 |
| Method Name | Method Equation | R2 | AUC | RMSE (%) | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | ||
| No normalization | 0.81 | 0.045 | 0.86 | 8.9 × 10−3 | 28.89 | 0.84 | |
| Method 1 | 0.82 | 0.027 | 0.86 | 8.0 × 10−3 | 27.88 | 0.92 | |
| Method 2 | 0.80 | 0.030 | 0.86 | 0.011 | 28.41 | 1.14 | |
| Method 3 | 0.82 | 0.025 | 0.86 | 5.5 × 10−3 | 28.30 | 0.63 | |
| Method 4 | 0.80 | 0.032 | 0.86 | 0.013 | 27.68 | 0.80 | |
| Method 5 | 0.82 | 0.037 | 0.86 | 0.011 | 27.54 | 1.15 | |
| Method 6 | 0.81 | 0.030 | 0.86 | 0.012 | 27.66 | 0.86 | |
| Method 7 | 0.80 | 0.045 | 0.86 | 9.1 × 10−3 | 27.90 | 0.75 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lambert, T.P.; Chan, M.; Sanchez-Perez, J.A.; Nikbakht, M.; Lin, D.J.; Nawar, A.; Bashar, S.K.; Kimball, J.P.; Zia, J.S.; Gazi, A.H.; et al. A Comparison of Normalization Techniques for Individual Baseline-Free Estimation of Absolute Hypovolemic Status Using a Porcine Model. Biosensors 2024, 14, 61. https://doi.org/10.3390/bios14020061
Lambert TP, Chan M, Sanchez-Perez JA, Nikbakht M, Lin DJ, Nawar A, Bashar SK, Kimball JP, Zia JS, Gazi AH, et al. A Comparison of Normalization Techniques for Individual Baseline-Free Estimation of Absolute Hypovolemic Status Using a Porcine Model. Biosensors. 2024; 14(2):61. https://doi.org/10.3390/bios14020061
Chicago/Turabian StyleLambert, Tamara P., Michael Chan, Jesus Antonio Sanchez-Perez, Mohammad Nikbakht, David J. Lin, Afra Nawar, Syed Khairul Bashar, Jacob P. Kimball, Jonathan S. Zia, Asim H. Gazi, and et al. 2024. "A Comparison of Normalization Techniques for Individual Baseline-Free Estimation of Absolute Hypovolemic Status Using a Porcine Model" Biosensors 14, no. 2: 61. https://doi.org/10.3390/bios14020061
APA StyleLambert, T. P., Chan, M., Sanchez-Perez, J. A., Nikbakht, M., Lin, D. J., Nawar, A., Bashar, S. K., Kimball, J. P., Zia, J. S., Gazi, A. H., Cestero, G. I., Corporan, D., Padala, M., Hahn, J.-O., & Inan, O. T. (2024). A Comparison of Normalization Techniques for Individual Baseline-Free Estimation of Absolute Hypovolemic Status Using a Porcine Model. Biosensors, 14(2), 61. https://doi.org/10.3390/bios14020061