RF Remote Blood Glucose Sensor and a Microfluidic Vascular Phantom for Sensor Validation

 ,
, 
 ,
, 

Abstract
:1. Introduction
2. Design and Method
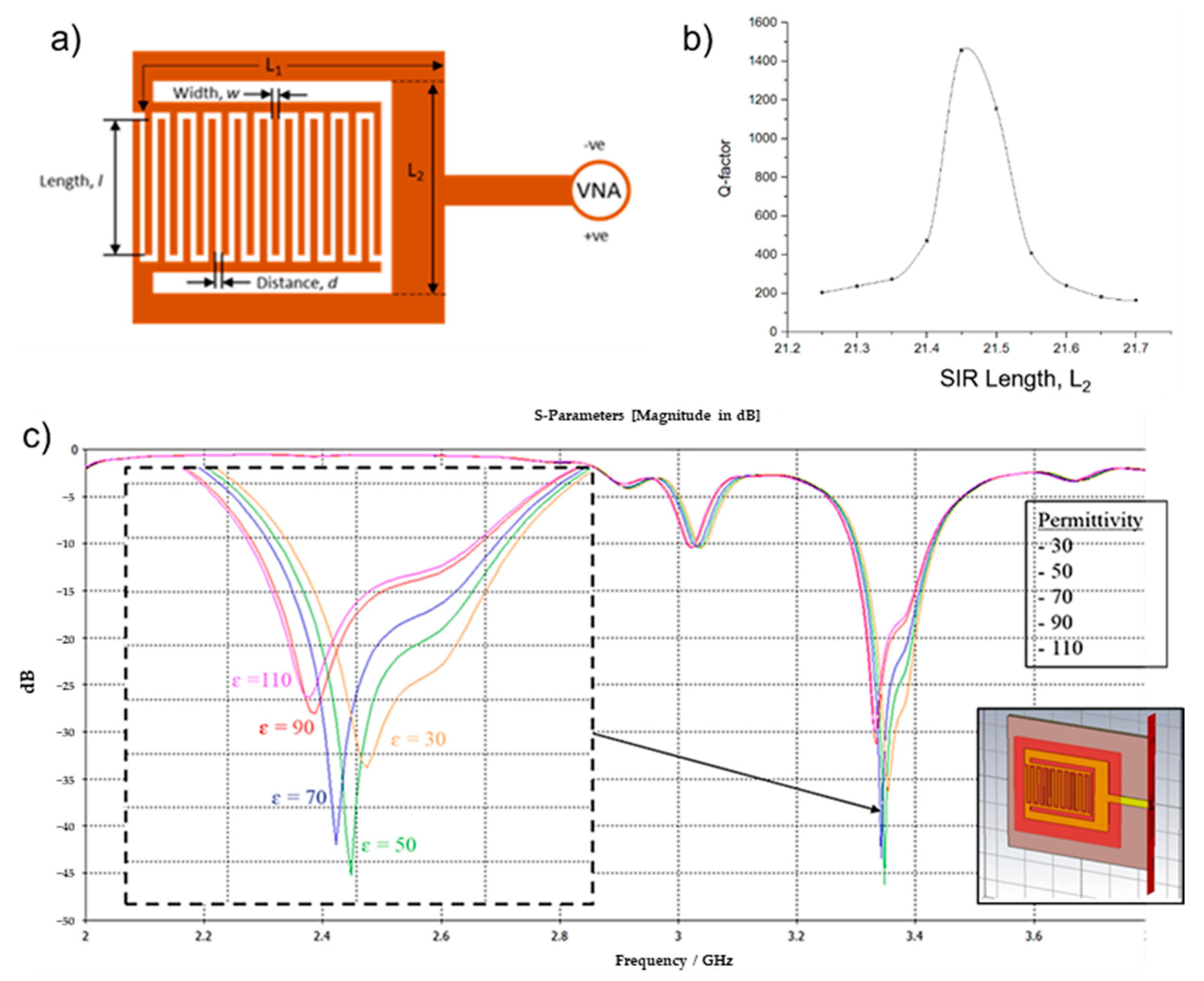
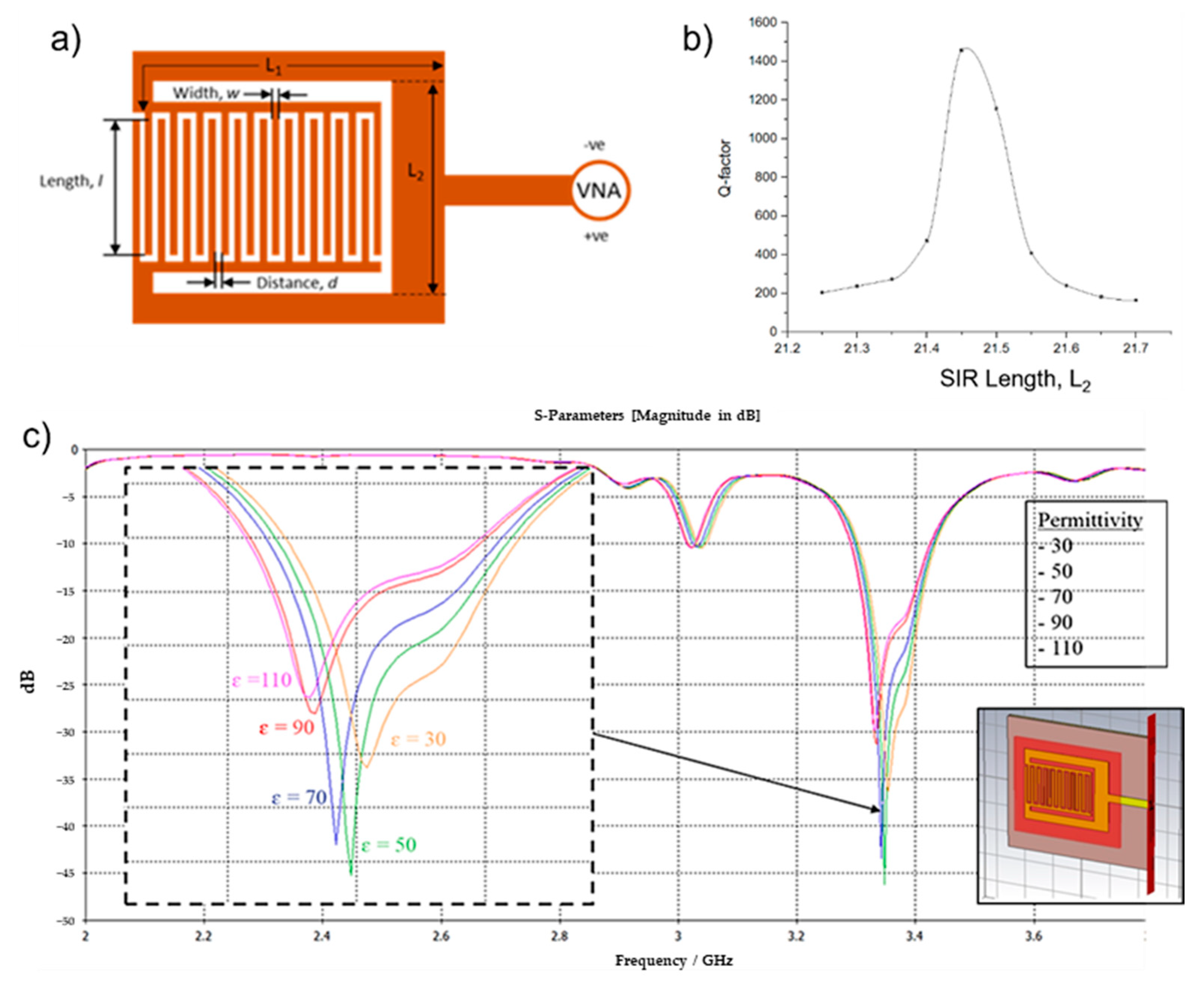
2.1. Stepped Impedance Resonator Sensor
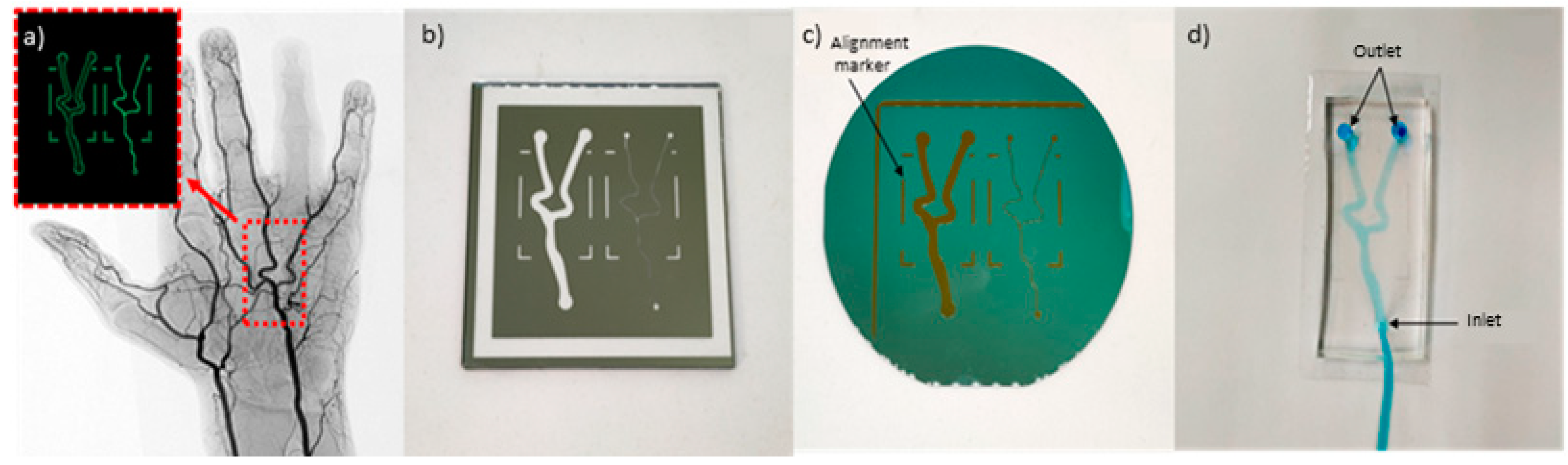
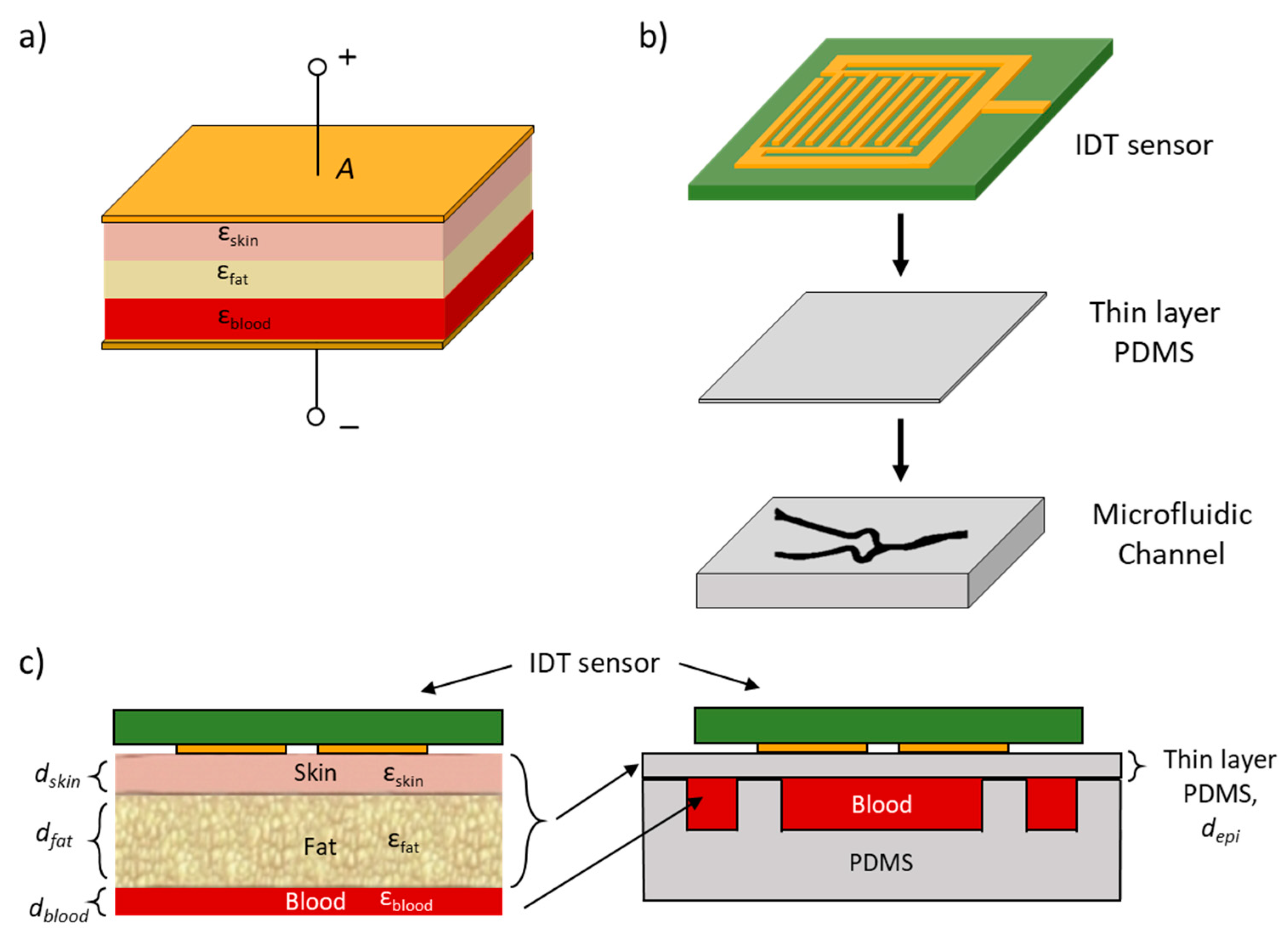
2.2. Microfluidic Vascular Phantom
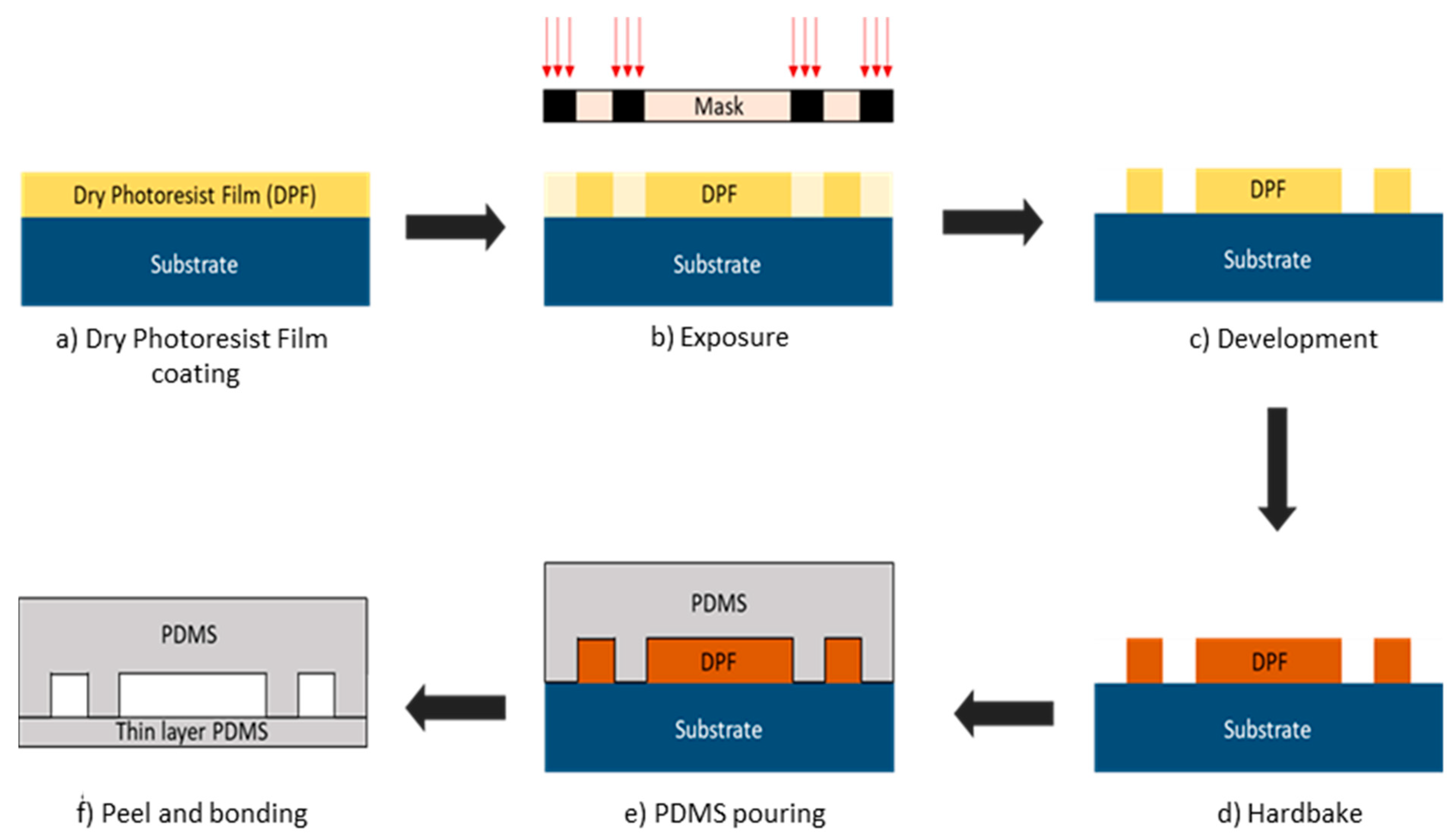
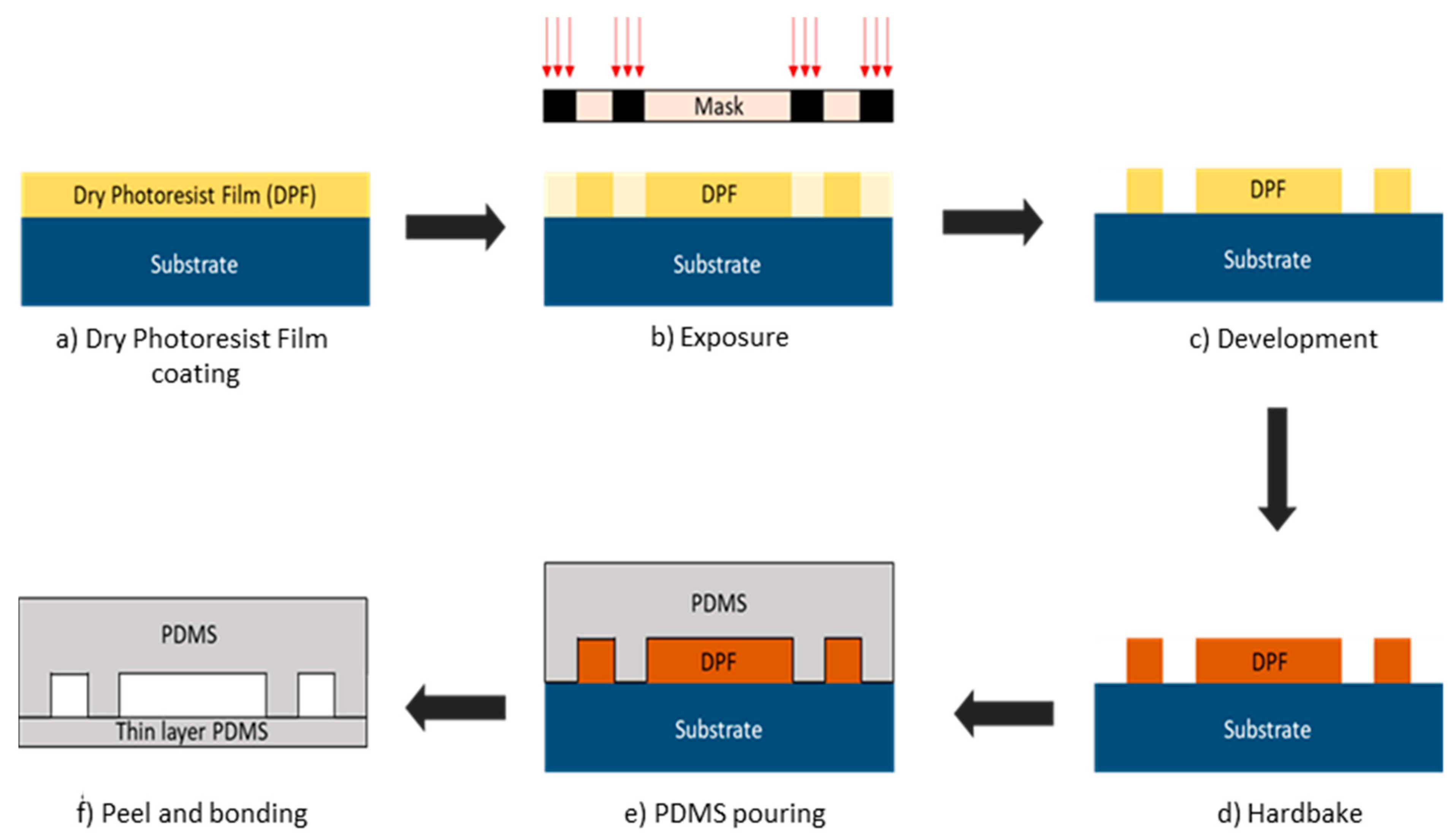
2.3. Microfluidic Fabrication
2.4. Glucose Sample Preparation
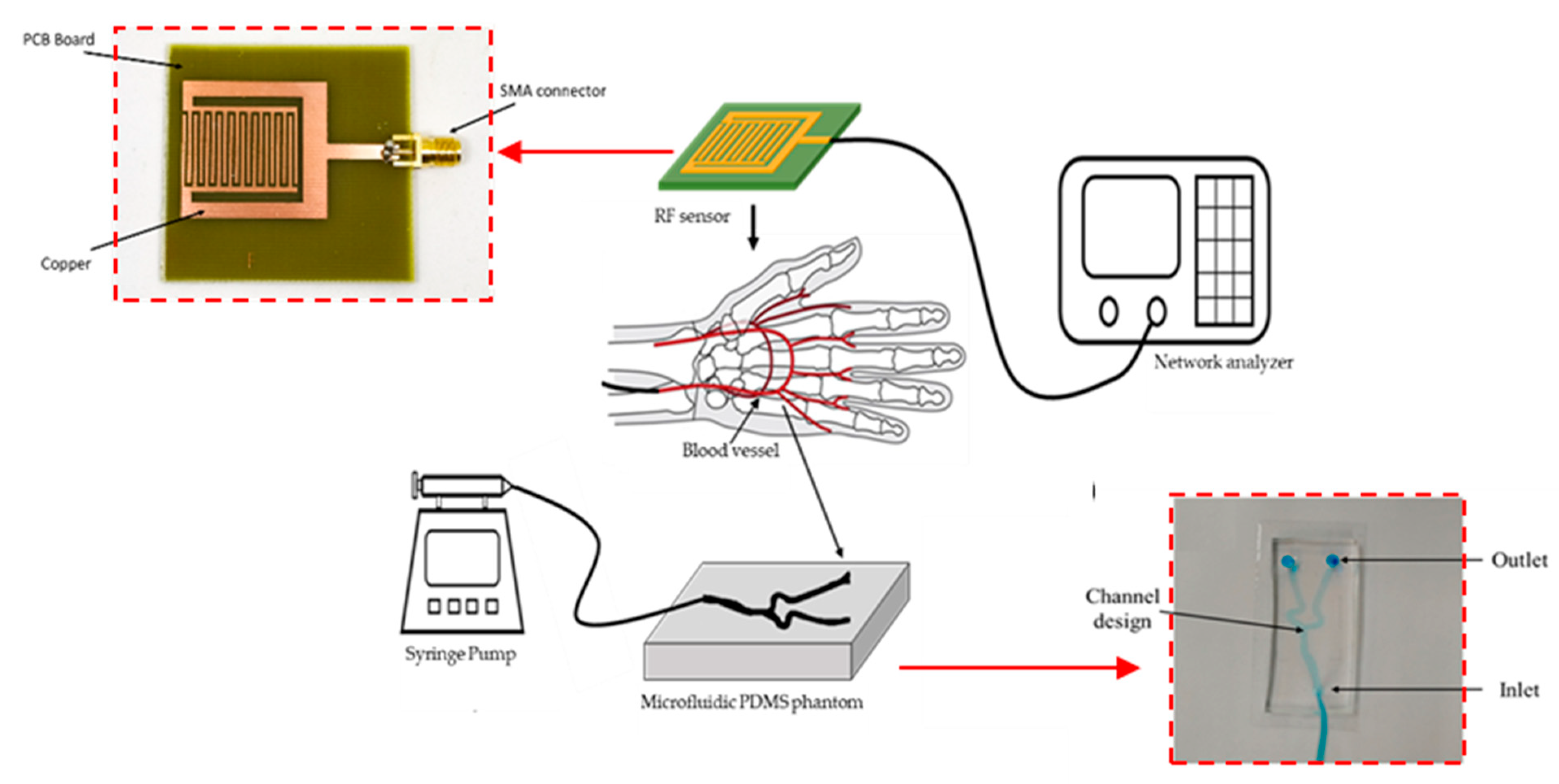
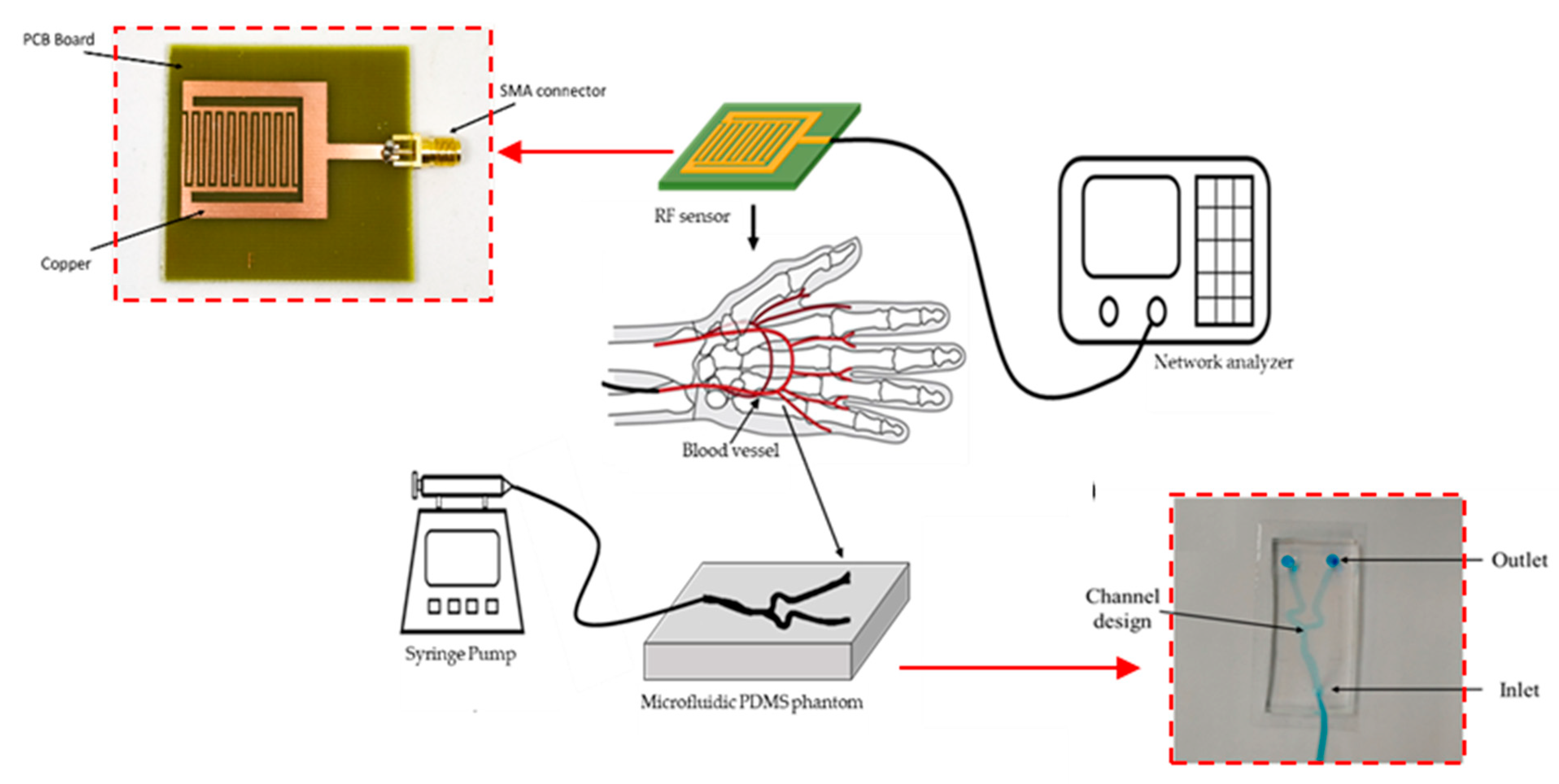
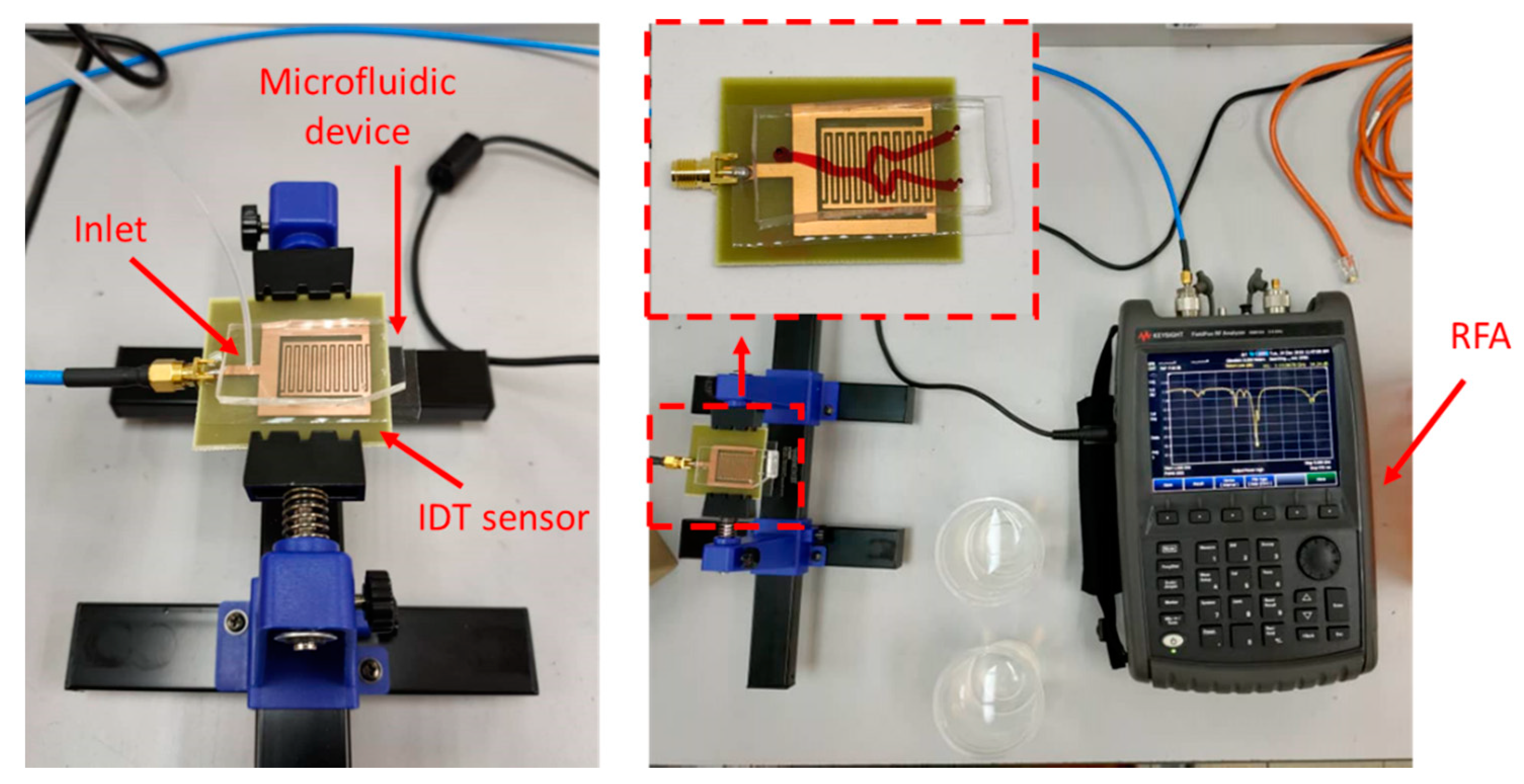
2.5. Experimental Setup
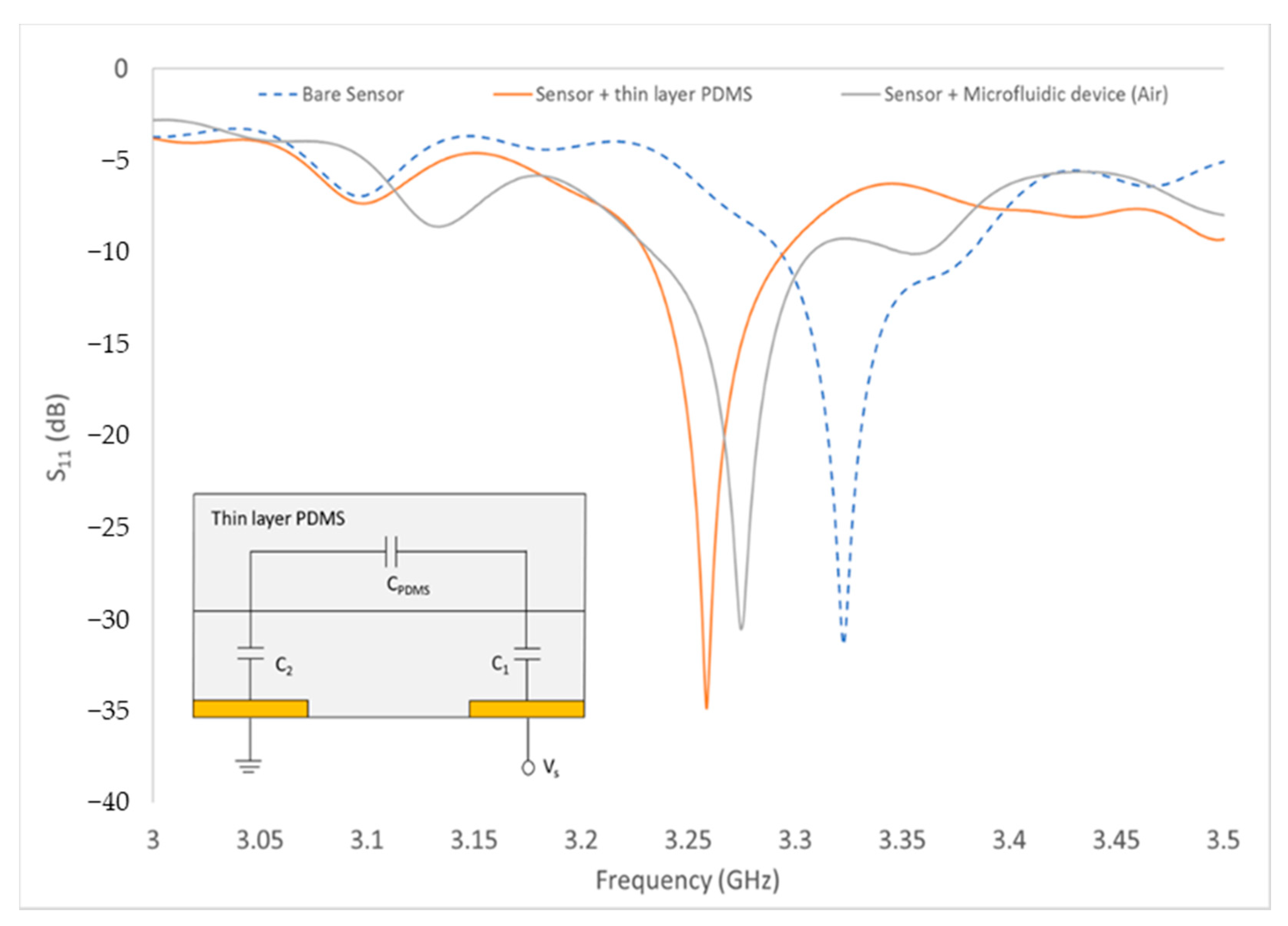
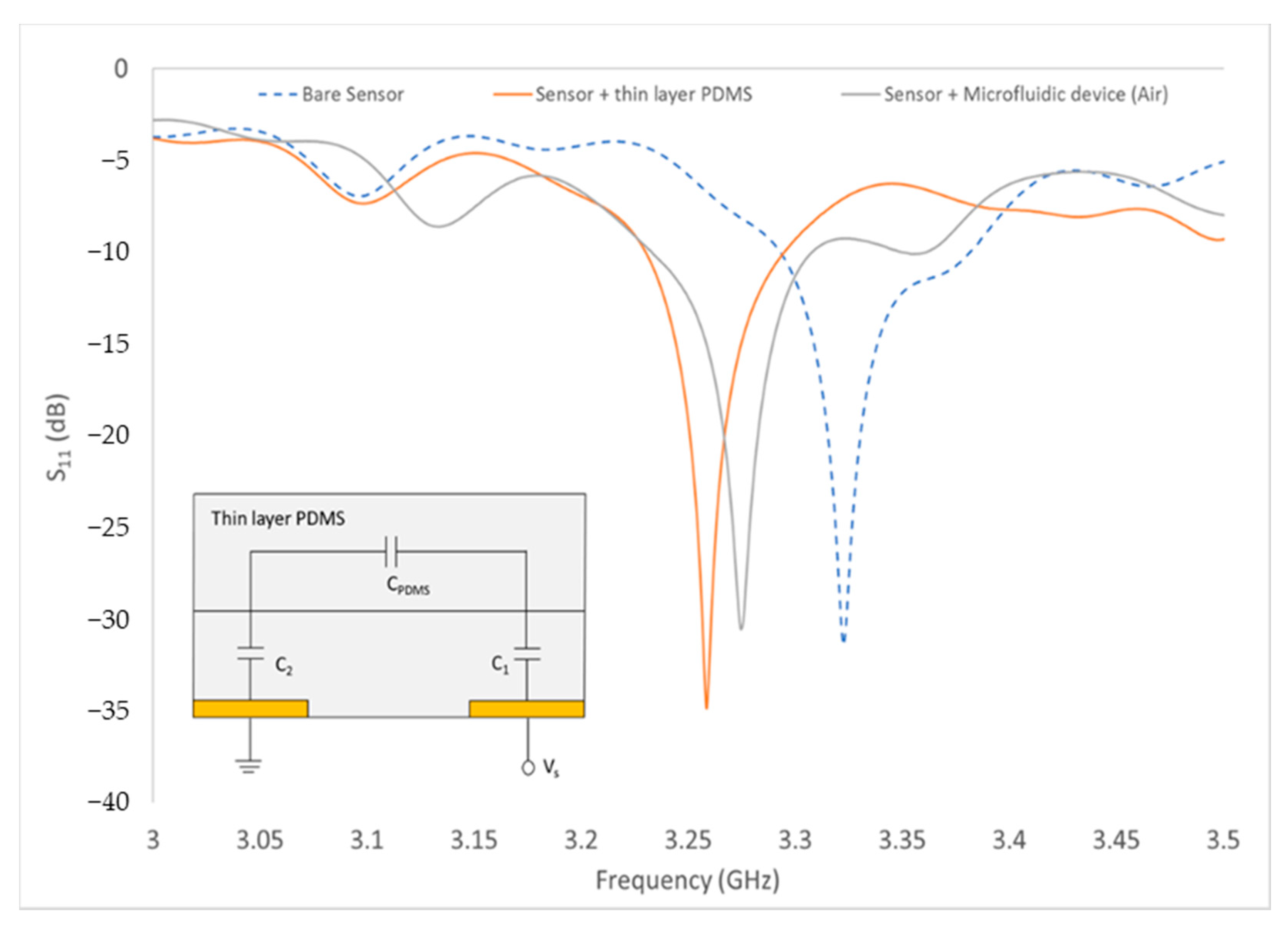
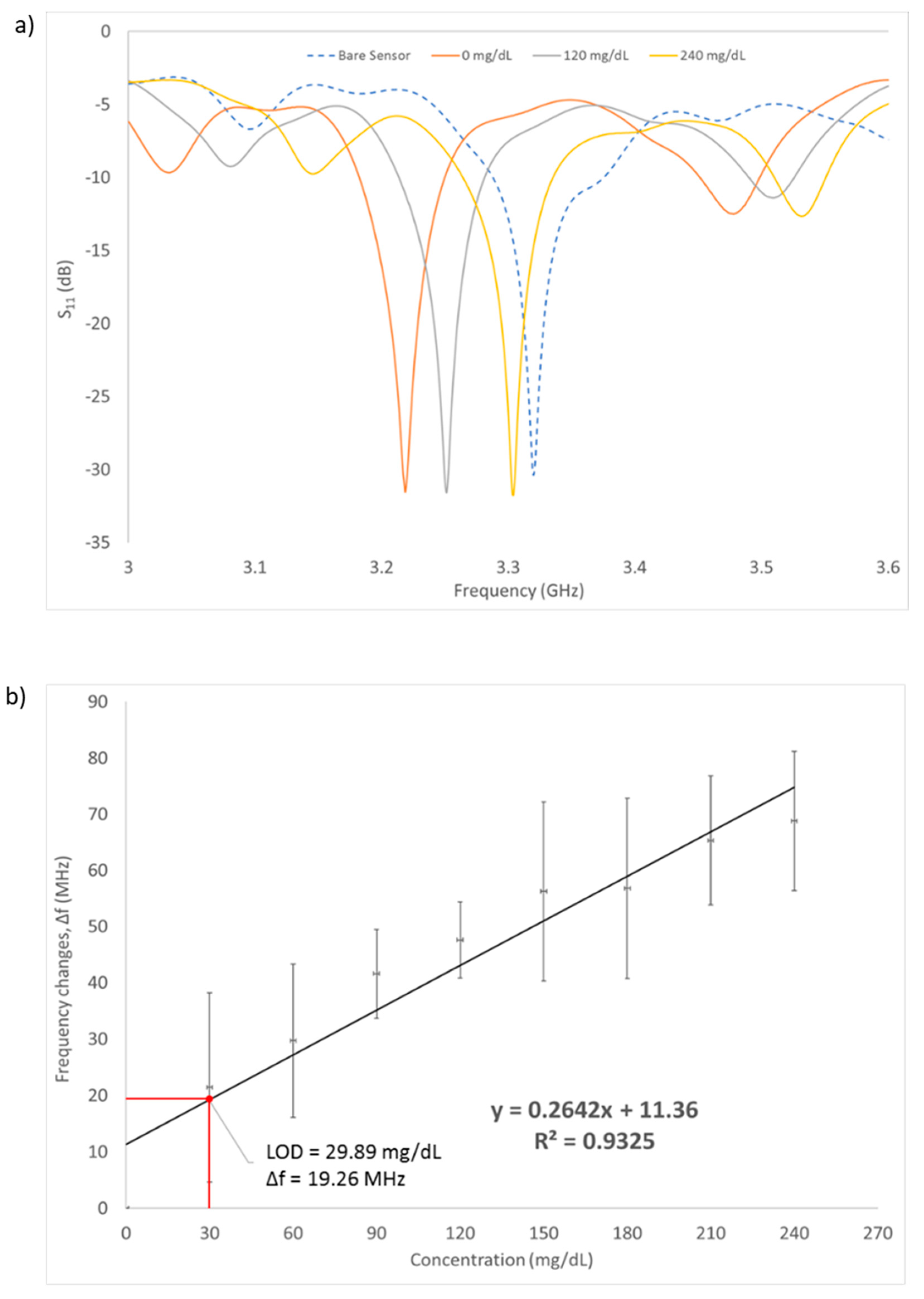
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coster, S.; Gulliford, M.; Seed, P.; Powrie, J.; Swaminathan, R. Monitoring blood glucose control in diabetes mellitus: A systematic review. Health Technol. Assess. 2000, 4, 1–94. [Google Scholar] [CrossRef] [Green Version]
- Abellán-Llobregat, A.; Jeerapan, I.; Bandodkar, A.; Vidal, L.; Canals, A.; Wang, J.; Morallon, E. A stretchable and screen-printed electrochemical sensor for glucose determination in human perspiration. Biosens. Bioelectron. 2017, 91, 885–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topsakal, E.; Karacolak, T.; Moreland, E.C. Glucose-dependent dielectric properties of blood plasma. In Proceedings of the 2011 XXXth URSI General Assembly and Scientific Symposium, Istanbul, Turkey, 13 August 2011; pp. 1–4. [Google Scholar]
- Choi, H.; Naylon, J.; Luzio, S.; Beutler, J.; Birchall, J.; Martin, C.; Porch, A. Design and in vitro interference test of microwave noninvasive blood glucose monitoring sensor. IEEE Trans. Microw. Theory Tech. 2015, 63, 3016–3025. [Google Scholar] [CrossRef] [Green Version]
- Turgul, V.; Kale, I. Characterization of the complex permittivity of glucose/water solutions for noninvasive RF/Microwave blood glucose sensing. In Proceedings of the 2016 IEEE International Instrumentation and Measurement Technology Conference Proceedings, Taipei, Taiwan, 23 May 2016; pp. 1–5. [Google Scholar]
- Gorst, A.; Zavyalova, K.; Mironchev, A. Non-invasive determination of glucose concentration using a near-field sensor. Biosensors 2021, 11, 62. [Google Scholar] [CrossRef] [PubMed]
- Juan, C.G.; Bronchalo, E.; Potelon, B.; Quendo, C.; Sabater-Navarro, J.M. Glucose concentration measurement in human blood plasma solutions with microwave sensors. Sensors 2019, 19, 3779. [Google Scholar] [CrossRef] [Green Version]
- Kitsara, M.; Goustouridis, D.; Chatzandroulis, S.; Chatzichristidi, M.; Raptis, I.; Ganetsos, T.; Igreja, R.; Dias, C. Single chip interdigitated electrode capacitive chemical sensor arrays. Sens. Actuators B Chem. 2007, 127, 186–192. [Google Scholar] [CrossRef]
- Rahman, M.S.B.A.; Mukhopadhyay, S.C.; Yu, P.L. Novel sensors for food inspections. Sens. Transducers 2010, 114, 1–40. [Google Scholar]
- Lei, S.; Deng, C.; Chen, Y.; Li, Y. A novel serial high frequency surface acoustic wave humidity sensor. Sens. Actuators A Phys. 2011, 167, 231–236. [Google Scholar] [CrossRef]
- Bin Yunos, M.F.A.; Nordin, A.N.; Zainuddin, A.; Khan, S. Modeling and development of radio frequency planar interdigital electrode sensors. Bull. Electr. Eng. Inform. 2019, 8, 978–984. [Google Scholar]
- Mishra, S.; Kim, E.-S.; Sharma, P.K.; Wang, Z.-J.; Yang, S.-H.; Kaushik, A.K.; Wang, C.; Li, Y.; Kim, N.-Y. Tailored biofunctionalized biosensor for the label-free sensing of prostate-specific antigen. ACS Appl. Bio Mater. 2020, 3, 7821–7830. [Google Scholar] [CrossRef]
- Adhikari, K.K.; Kim, N.-Y. Ultrahigh-sensitivity mediator-free biosensor based on a microfabricated microwave resonator for the detection of micromolar glucose concentrations. IEEE Trans. Microw. Theory Tech. 2015, 64, 319–327. [Google Scholar] [CrossRef]
- Li, Y.; Yao, Z.; Yue, W.; Zhang, C.; Gao, S.; Wang, C. Reusable, non-invasive, and ultrafast radio frequency biosensor based on optimized integrated passive device fabrication process for quantitative detection of glucose levels. Sensors 2020, 20, 1565. [Google Scholar] [CrossRef] [Green Version]
- Malena, L.; Fiser, O.; Stauffer, P.R.; Drizdal, T.; Vrba, J.; Vrba, D. Feasibility evaluation of metamaterial microwave sensors for non-invasive blood glucose monitoring. Sensors 2021, 21, 6871. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-H.; Kim, C.-S.; Choi, B.-C.; Ham, K.-Y. The correlation of the complex dielectric constant and blood glucose at low frequency. Biosens. Bioelectron. 2003, 19, 321–324. [Google Scholar] [CrossRef]
- Cespedes, F.A. RF Sensing System for Continuous Blood Glucose Monitoring. Ph.D. Thesis, University of South Florida, Tampa Bay, FL, USA, 2017. [Google Scholar]
- Yilmaz, T.; Foster, R.; Hao, Y. Broadband tissue mimicking phantoms and a patch resonator for evaluating noninvasive monitoring of blood glucose levels. IEEE Trans. Antennas Propag. 2014, 62, 3064–3075. [Google Scholar] [CrossRef]
- Coles-Black, J.; Bolton, D.; Chuen, J. Accessing 3D printed vascular phantoms for procedural simulation. Front. Surg. 2021, 7, 158. [Google Scholar] [CrossRef] [PubMed]
- Claudel, J.; Ngo, T.-T.; Kourtiche, D.; Nadi, M. Interdigitated sensor optimization for blood sample analysis. Biosensors 2020, 10, 208. [Google Scholar] [CrossRef]
- Zainuddin, A.A.; Nordin, A.N.; Rahim, R.A.; Ralib, A.A.M.; Khan, S.; Guines, C.; Chatras, M.; Pothier, A. Verification of quartz crystal microbalance array using vector network analyzer and OpenQCM. Indones. J. Electr. Eng. Comput. Sci 2018, 10, 84–93. [Google Scholar] [CrossRef]
- Chomtong, P.; Akkaraekthalin, P. A quad-band bandpass filter using stepped impedance resonators with interdigital capacitors. IEEJ Trans. Electr. Electron. Eng. 2018, 13, 1080–1086. [Google Scholar] [CrossRef]
- Amsüss, R.; Saito, S.; Munro, W. Hybridization of quantum systems: Coupling nitrogen–vacancy (NV) centers in diamond to superconducting circuits. In Quantum Information Processing with Diamond; Elsevier: Amsterdam, The Netherlands, 2014; pp. 264–290. [Google Scholar]
- Fazan, V.P.S.; Borges, C.T.; Da Silva, J.H.; Caetano, A.G.; Filho, O.A.R. Superficial palmar arch: An arterial diameter study. J. Anat. 2004, 204, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Loring, L.A.; Hallisey, M.J. Arteriography and interventional therapy for diseases of the hand. Radiographics 1995, 15, 1299–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, C. Compilation of the Dielectric Properties of Body Tissues at RF and microwave Frequencies. Physics 1996. [Google Scholar] [CrossRef] [Green Version]
- Courson, R.; Cargou, S.; Conédéra, V.; Fouet, M.; Blatché, M.-C.; Serpentini, C.L.; Gué, A.M. Low-cost multilevel microchannel lab on chip: DF-1000 series dry film photoresist as a promising enabler. RSC Adv. 2014, 4, 54847–54853. [Google Scholar] [CrossRef]
- Vrba, J.; Vrba, D. A Microwave metamaterial inspired sensor for non-invasive blood glucose monitoring. Radioengineering 2015, 24, 877–884. [Google Scholar] [CrossRef]
- Klarhöfer, M.; Csapo, B.; Balassy, C.; Szeles, J.; Moser, E. High-resolution blood flow velocity measurements in the human finger. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 2001, 45, 716–719. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, T.; Foster, R.; Hao, Y. Radio-frequency and microwave techniques for non-invasive measurement of blood glucose levels. Diagnostics 2019, 9, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Values |
|---|---|
| Electric Conductivity (S/m) | 3.05 |
| Density (kg/m3) | 1050 |
| Heat Capacity (J/kg/°C) | 3617 |
| Thermal Cond. (W/m/°C) | 0.52 |
| Heat Transfer Rate (mL/min/kg) | 10,000 |
| Parameter | Dielectric Constant, ε | Thickness [mm] |
|---|---|---|
| Skin | 37.50 | 1.5 |
| Fat | 10.70 | 3.0 |
| Blood vessel | 41.90 | 2.5 |
| PDMS | 2.68 | 0.9 |
| Blood Sugar Levels | Blood Glucose Concentration (mg/dL) |
|---|---|
| Hyperglycemia | >200 |
| Normal Glycemia | 72–108 |
| Hypoglycemia | <60 |
| Reference | Sensor | Phantom | Frequency | LOD | Range Glucose Level |
|---|---|---|---|---|---|
| [13] | Dual needle | Hamster tail | 10 kHz | - | 20–500 mg/dL |
| [14] | Dielectric probe | Oil, gelatin, salt, deionized water, detergent | 4–7 GHz | 100 mg/dL | 0–400 mg/dL |
| [15] | Dielectric probe | Oil, gelatin, salt, deionized water, detergent | 0.3–20 GHz | 72 mg/dL | 72–216 mg/dL |
| This work | Stepped impedance resonator | Dual-layer PDMS | 1–5 GHz | 29.89 mg/dL | 0–240 mg/dL |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yunos, M.F.A.M.; Manczak, R.; Guines, C.; Mansor, A.F.M.; Mak, W.C.; Khan, S.; Ramli, N.A.; Pothier, A.; Nordin, A.N. RF Remote Blood Glucose Sensor and a Microfluidic Vascular Phantom for Sensor Validation. Biosensors 2021, 11, 494. https://doi.org/10.3390/bios11120494
Yunos MFAM, Manczak R, Guines C, Mansor AFM, Mak WC, Khan S, Ramli NA, Pothier A, Nordin AN. RF Remote Blood Glucose Sensor and a Microfluidic Vascular Phantom for Sensor Validation. Biosensors. 2021; 11(12):494. https://doi.org/10.3390/bios11120494
Chicago/Turabian StyleYunos, Muhammad Farhan Affendi Mohamad, Rémi Manczak, Cyril Guines, Ahmad Fairuzabadi Mohd Mansor, Wing Cheung Mak, Sheroz Khan, Noor Amalina Ramli, Arnaud Pothier, and Anis Nurashikin Nordin. 2021. "RF Remote Blood Glucose Sensor and a Microfluidic Vascular Phantom for Sensor Validation" Biosensors 11, no. 12: 494. https://doi.org/10.3390/bios11120494
APA StyleYunos, M. F. A. M., Manczak, R., Guines, C., Mansor, A. F. M., Mak, W. C., Khan, S., Ramli, N. A., Pothier, A., & Nordin, A. N. (2021). RF Remote Blood Glucose Sensor and a Microfluidic Vascular Phantom for Sensor Validation. Biosensors, 11(12), 494. https://doi.org/10.3390/bios11120494