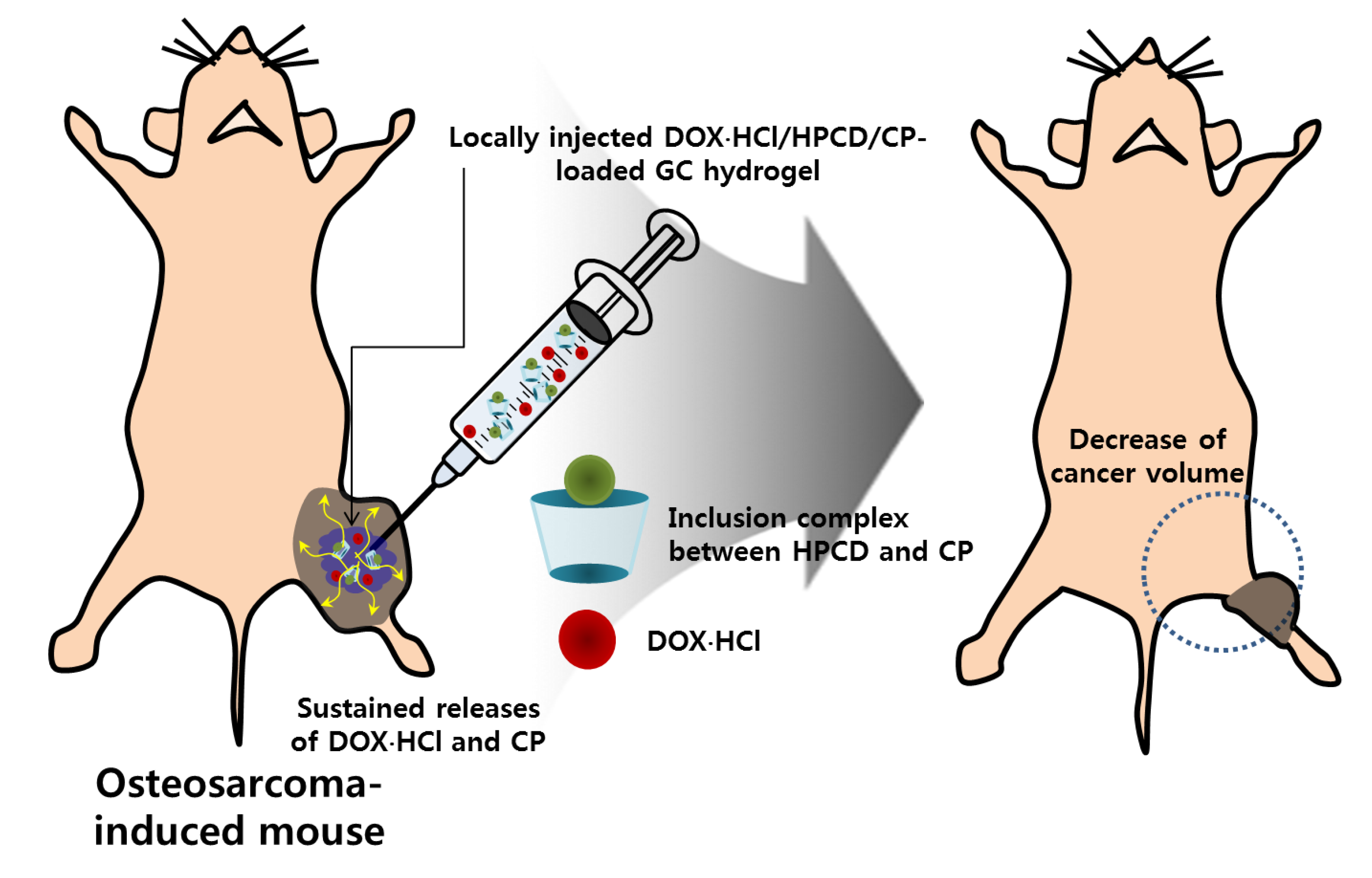
Doxorubicin·Hydrochloride/Cisplatin-Loaded Hydrogel/Nanosized (2-Hydroxypropyl)-Beta-Cyclodextrin Local Drug-Delivery System for Osteosarcoma Treatment In Vivo



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. HP-β-CD ((2-Hydroxypropyl)-Beta-Cyclodextrin) and Cisplatin (CP) Complex (HPCD/CP)
2.3. Preparation of Doxorubicin·Hydrochloride (DOX·HCl) and/or HPCD/CP-Loaded Visible Light-Cured Glycol Chitosan (GC) hydrogel (DOX·HCl-Loaded (GD), CP-Loaded (GHCP) and GDHCP)
2.4. Release Test of DOX·HCl and CP
2.5. In Vitro Cell Viability
2.6. Osteosarcoma (OSA) Animal Model
2.7. Histological Evaluations
2.8. Statistical Analysis
3. Results
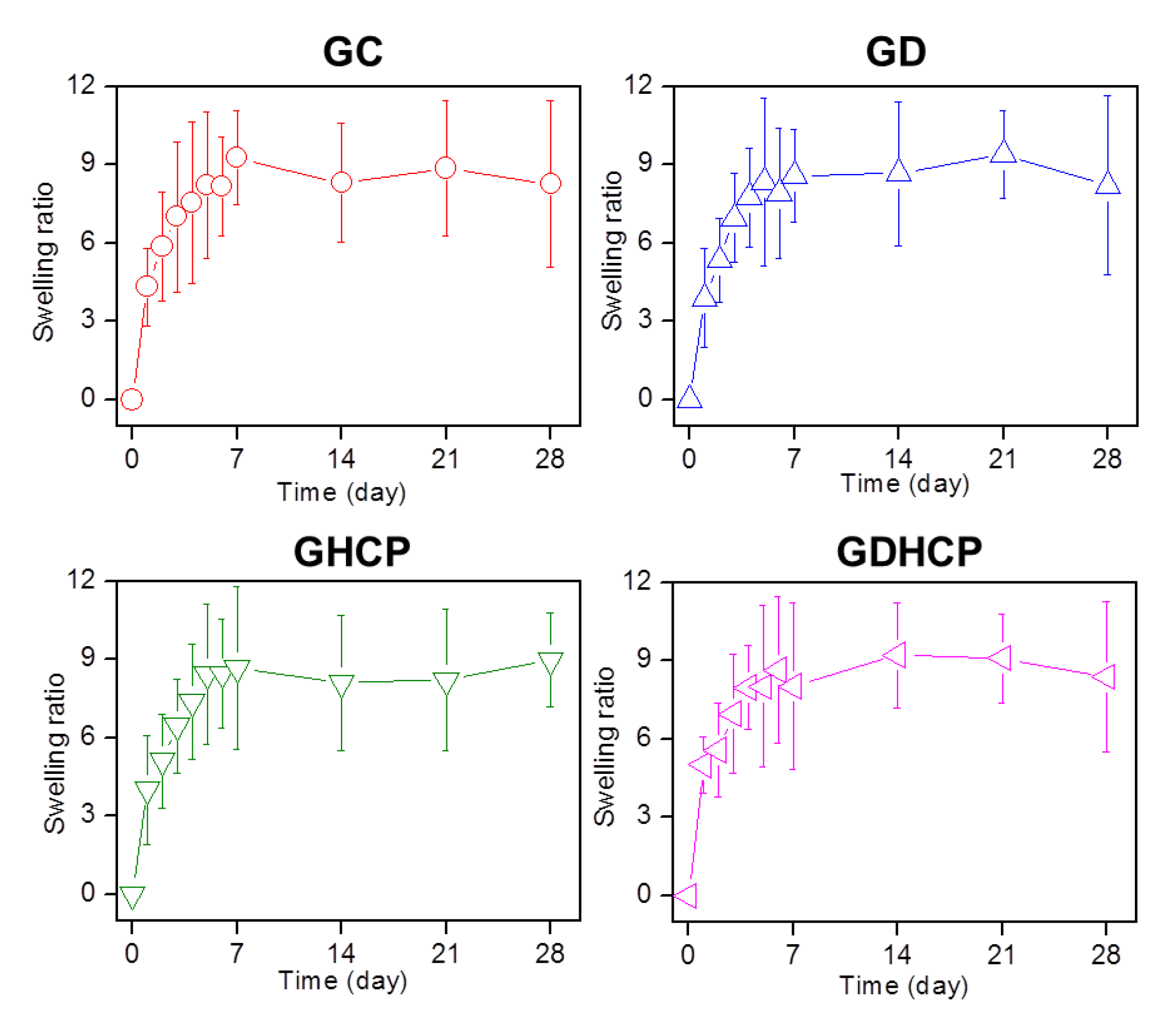
3.1. Swelling Ratio
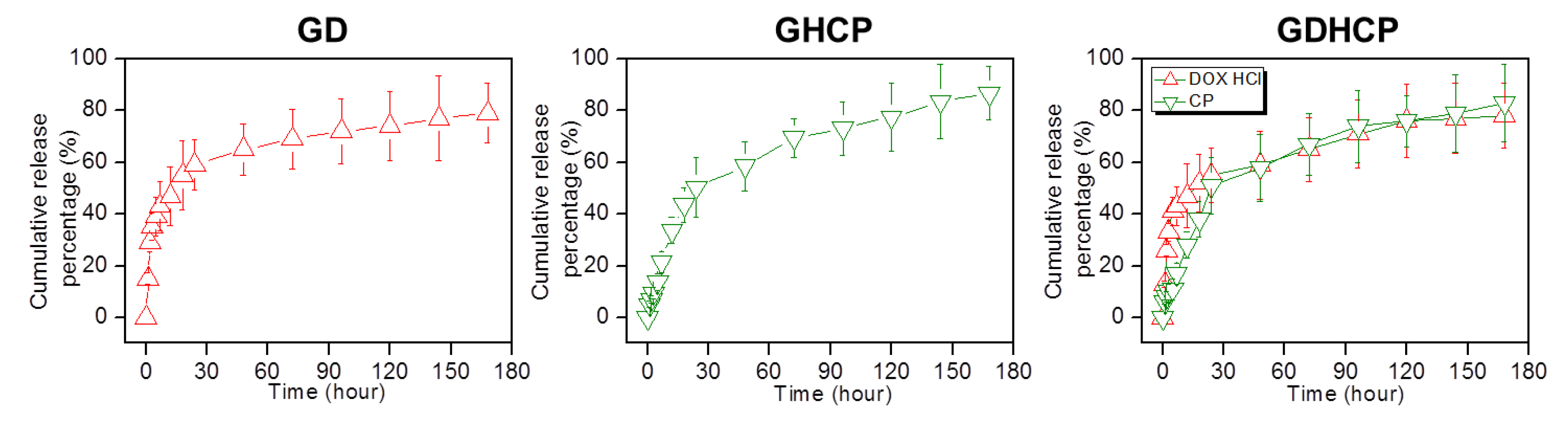
3.2. Release Behavior of DOX·HCl and/or CP
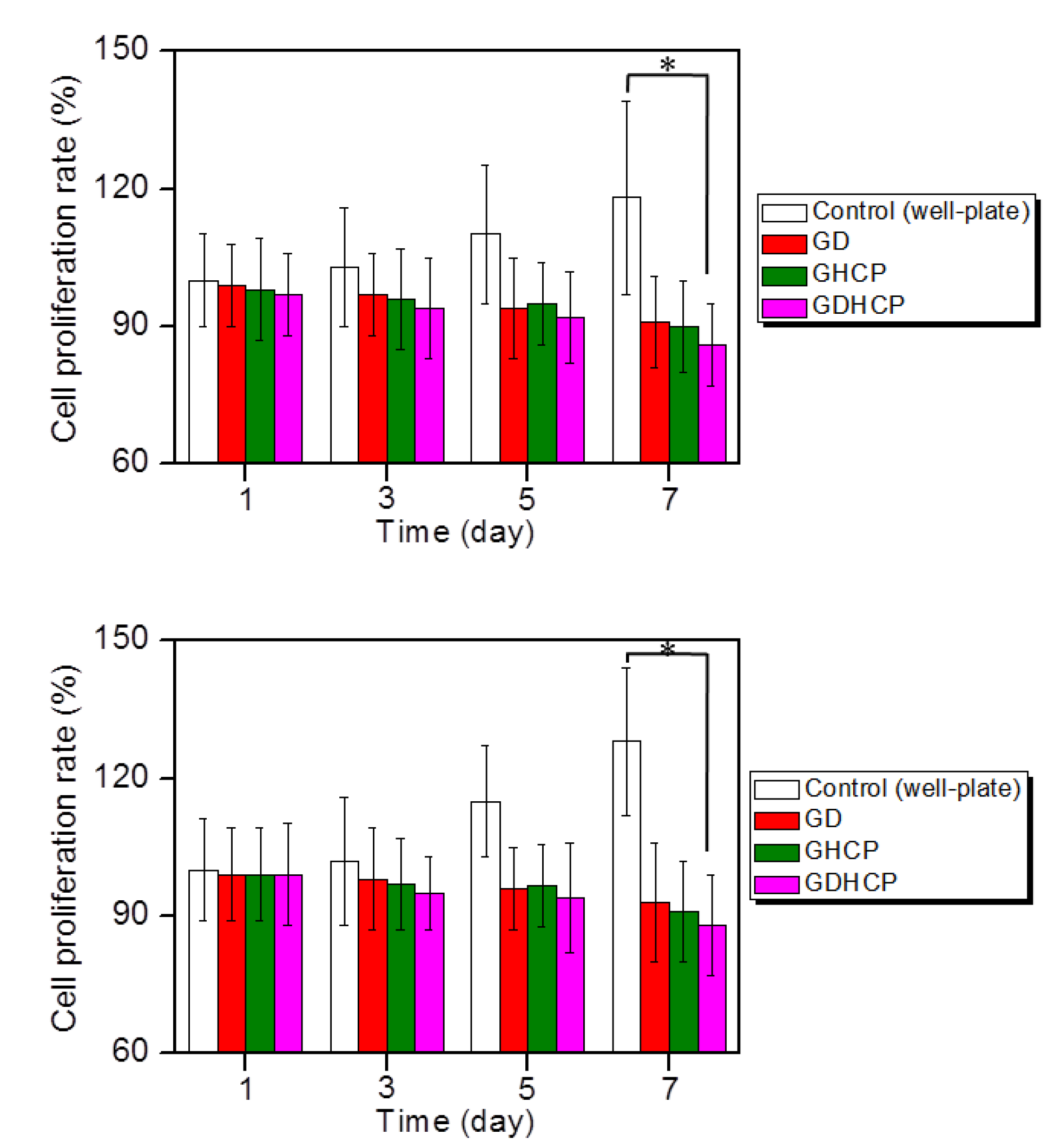
3.3. In Vitro Anticancer Effect
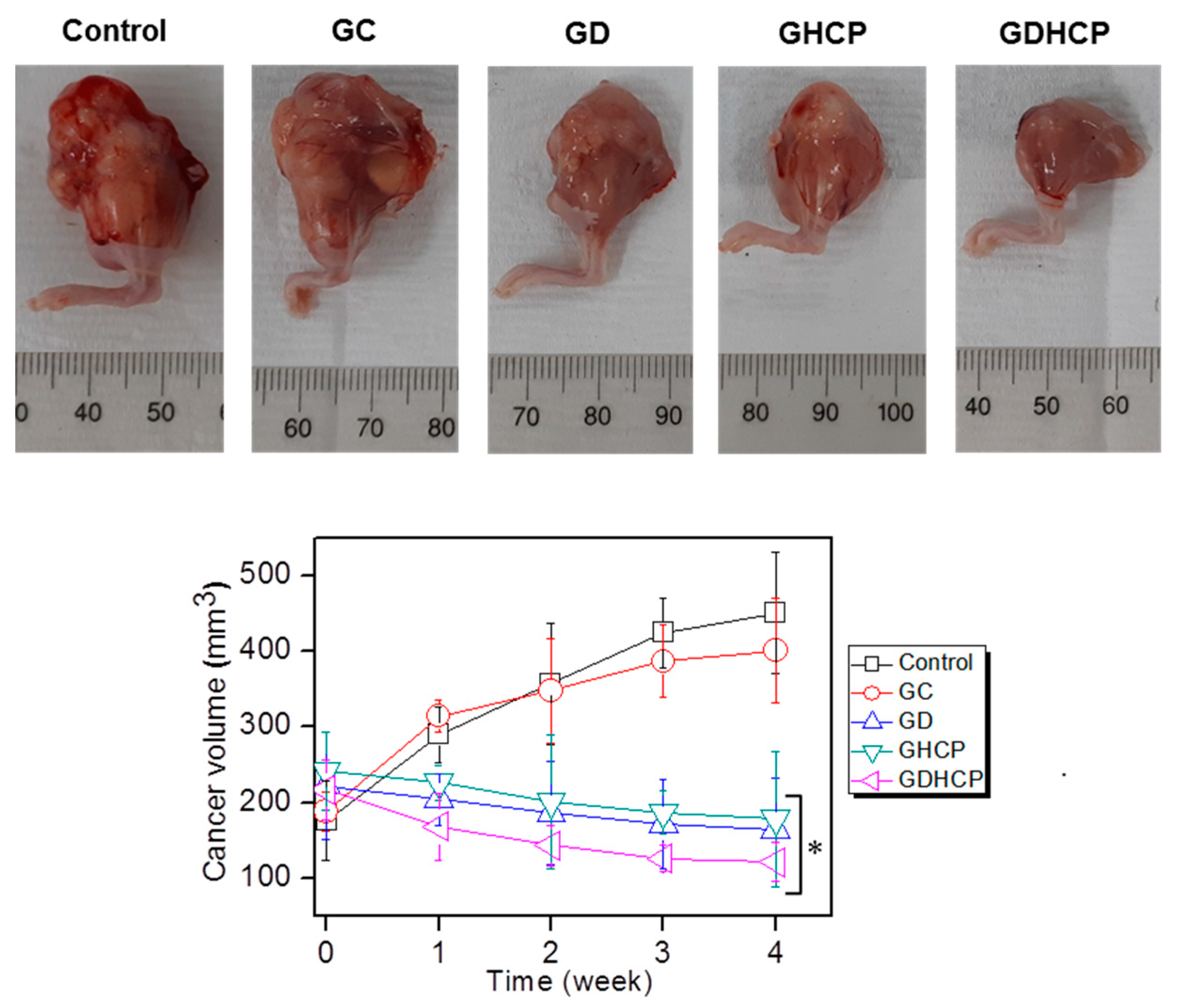
3.4. In Vivo Anticancer Effect
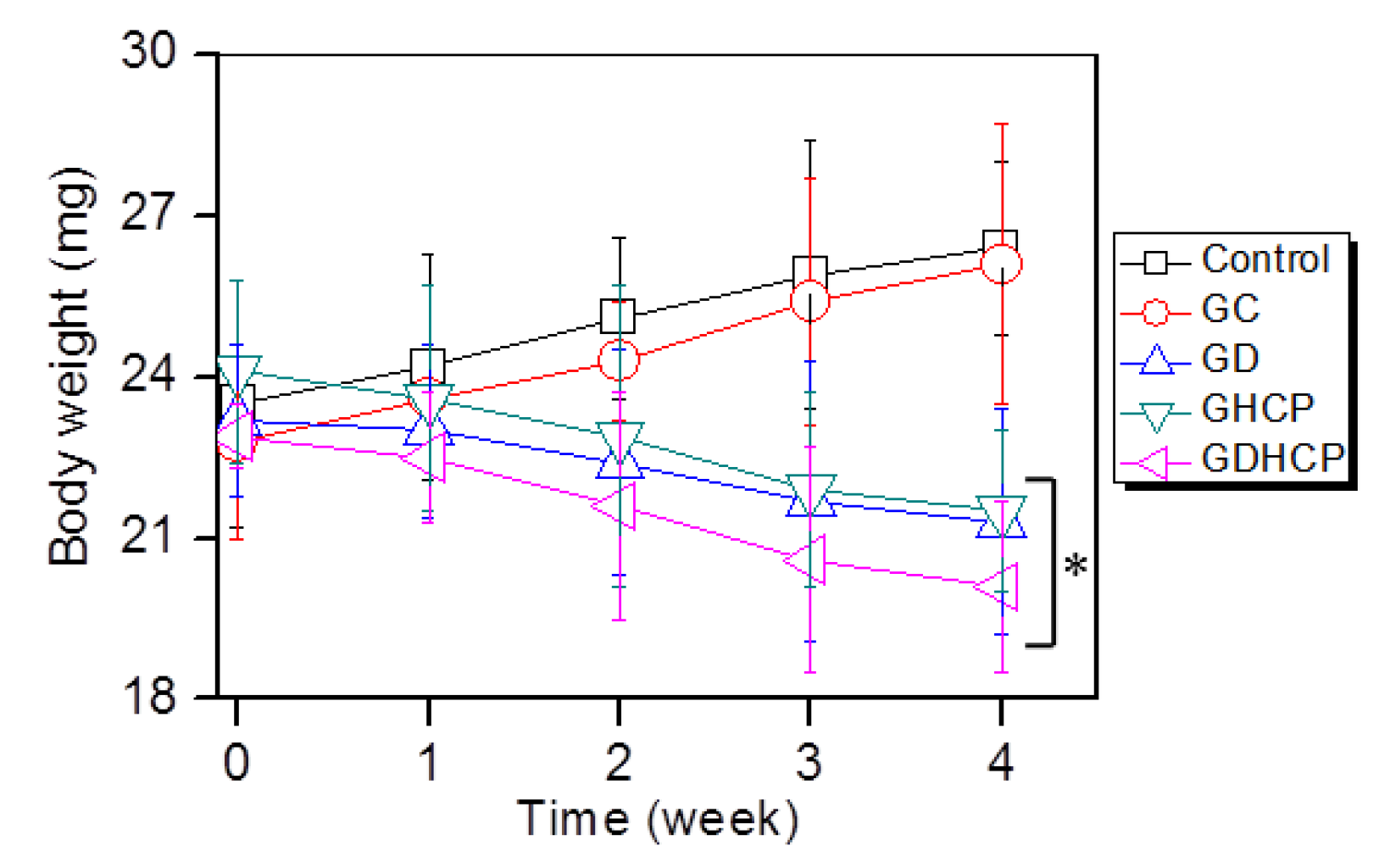
3.5. Body Weight
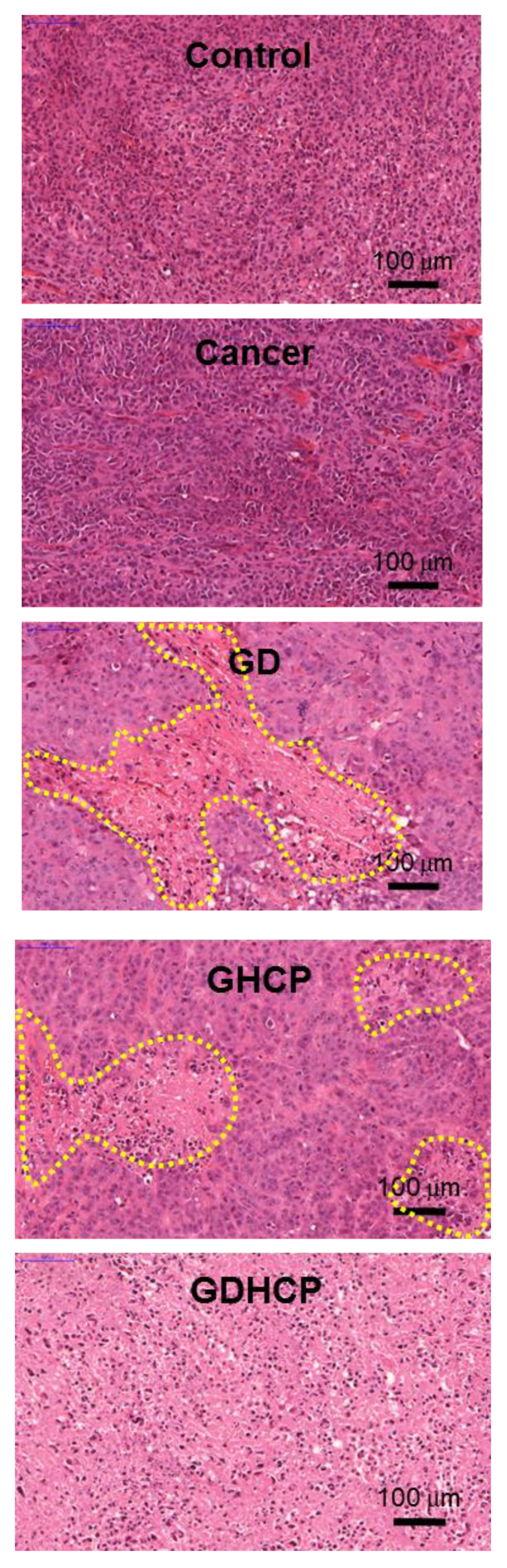
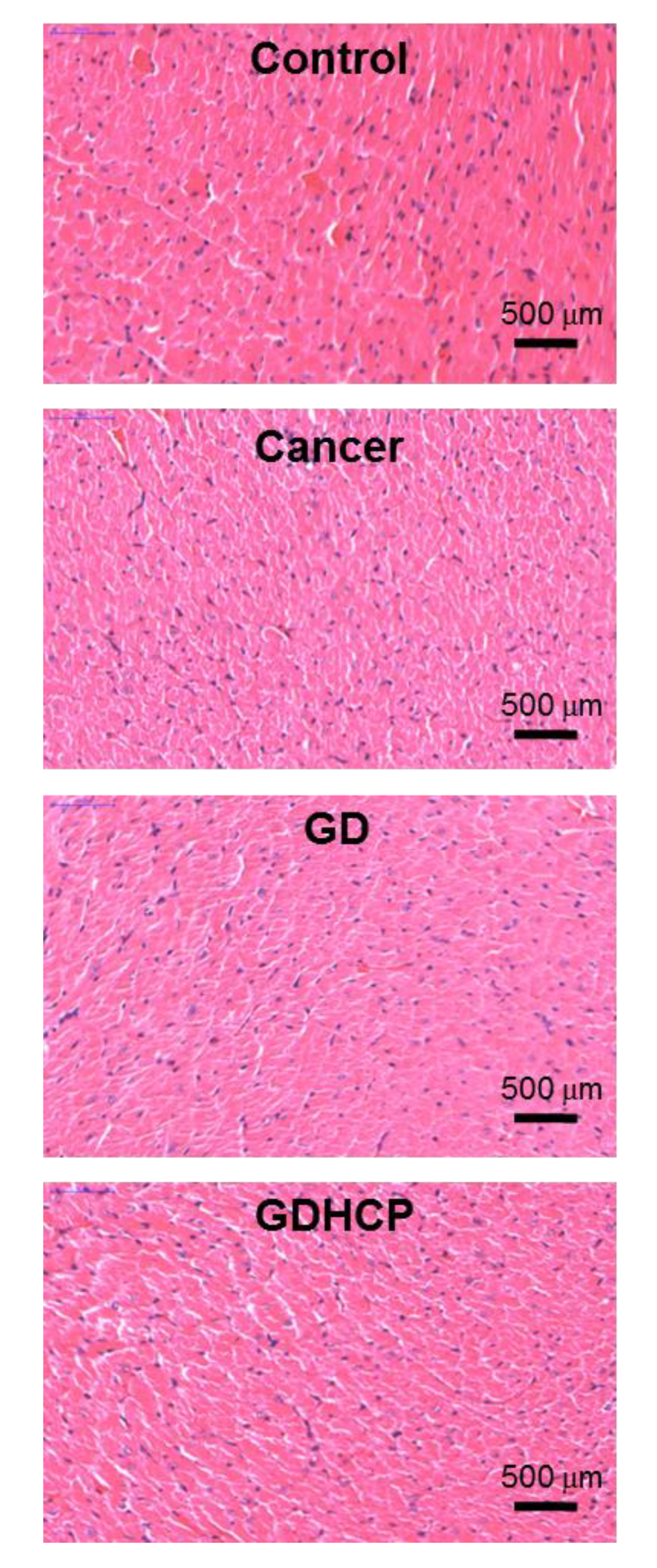
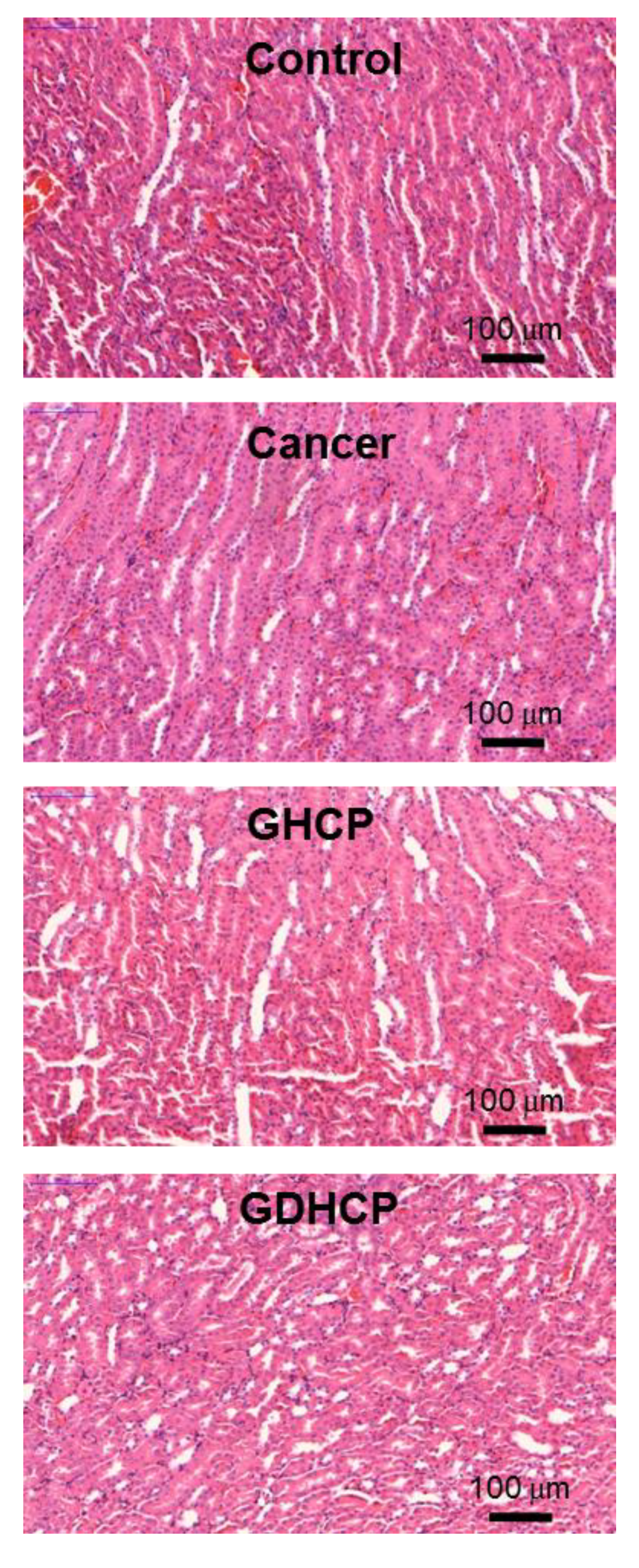
3.6. Histological Evaluations
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current treatment and a collaborative pathway to success. J. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef] [PubMed]
- Ebb, D.; Meyers, P.; Grier, H.; Bernstein, M.; Gorlick, R.; Lipshultz, S.E.; Krailo, M.; Devidas, M.; Barkauskas, D.A.; Siegal, G.P.; et al. Phase II trial of trastuzumab in combination with cytotoxic chemotherapy for treatment of metastatic osteosarcoma with human epidermal growth factor receptor 2 overexpression: A report from the children’s oncology group. J. Clin. Oncol. 2012, 30, 2545–2551. [Google Scholar] [CrossRef] [PubMed]
- Au, K.M.; Satterlee, A.; Min, Y.; Tian, X.; Kim, Y.S.; Caster, J.M.; Zhang, L.; Zhang, T.; Huang, L.; Wang, A.Z. Folate-targeted pH-responsive calcium zoledronate nanoscale metal-organic frameworks: Turning a bone antiresorptove agent into an anticancer therapeutic. Biomaterials 2016, 82, 178–193. [Google Scholar] [CrossRef] [PubMed]
- Wachtel, M.; Schäfer, B.W. Targets for cancer therapy in childhood sarcomas. Cancer Treat. Rev. 2010, 6, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Rainusso, N.; Wang, L.L.; Yustein, J.T. The adolescent and young adult with cancer: State of the art-bone tumors. Curr. Oncol. Rep. 2013, 15, 296–307. [Google Scholar] [CrossRef]
- DeVita, V.T. Principles of Chemotherapy. In Cancer Principles and Practice of Oncology; DeVita, V.T., Hell-man, S., Rosenberg, S.A., Eds.; JB Lippincott Co: Philadelphia, PA, USA, 1993; pp. 276–292. [Google Scholar]
- Chabner, B.A. Clinical Strategies for Cancer Treatment: The Role of Drugs. In Cancer Chemotherapy Principles and Practice; Chabner, B.A., Collins, J.M., Eds.; JB Lippincott Co: Philadelphia, PA, USA, 1990; pp. 1–15. [Google Scholar]
- Chun, R.; Kurzman, I.D.; Couto, C.G.; Klausner, J.; Henry, C.; MacEwen, E.G. Cisplatin and doxorubicin combination chemotherapy for the treatment of canine osteosarcoma: A pilot study. J. Vet. Intern. Med. 2000, 14, 495–498. [Google Scholar] [CrossRef]
- Patra, J.K.; Das, G.; Fraceto, L.F.; Campos, E.V.R.; del Pilar, R.-T.M.; Acosta-Torres, L.S.; Diaz-Torres, L.A.; Grillo, R.; Swamy, M.K.; Sharma, S.; et al. Nano based drug delivery systems: Recent developments and future prospects. J. Nanobiotech. 2018, 16, 71. [Google Scholar] [CrossRef]
- Yoo, Y.; Yoon, S.-J.; Kim, S.Y.; Lee, D.-W.; Um, S.; Hyun, H.; Hong, S.O.; Yang, D.H. A local drug delivery system based on visible light-cured glycol chitosan and doxorubicin⋅hydrochloride for thyroid cancer treatment in vitro and in vivo. Drug Deliv. 2018, 25, 1664–1671. [Google Scholar] [CrossRef]
- Hyun, H.; Park, M.H.; Lim, W.; Kim, S.Y.; Jo, D.; Jung, J.S.; Jo, G.; Um, S.; Lee, D.-W.; Yang, D.H. Injectable visible light-cured glycol chitosan hydrogels with controlled release of anticancer drugs for local cancer therapy in vivo: A feasible study. Artf. Cells Nanomed. Biotech. 2018, 46, 874–882. [Google Scholar] [CrossRef]
- Hyun, H.; Park, M.H.; Jo, G.; Kim, S.Y.; Chun, H.J.; Yang, D.H. Photo-cured glycol chitosan hydrogel for ovarian cancer drug delivery. Mar. Drugs 2019, 17, 41. [Google Scholar] [CrossRef]
- Yang, D.H.; Kim, H.J.; Kim, J.K.; Chun, H.J.; Park, K.S. Preparation of redox-sensitive β-CD-based nanoparticles with controlled release of curcumin for improved therapeutic effect on liver cancer in vitro. J. Ind. Eng. Chem. 2017, 45, 156–163. [Google Scholar] [CrossRef]
- Hyun, H.; Lee, S.; Lim, W.; Jo, D.; Jung, J.S.; Jo, G.; Kim, S.Y.; Lee, D.-W.; Um, S.; Yang, D.H.; et al. Engineered beta-cyclodextrin-based carrier for targeted doxorubicin delivery in breast cancer therapy in vivo. J. Ind. Eng. Chem. 2019, 70, 145–151. [Google Scholar] [CrossRef]
- Balaji, A.; Pandey, V.P.; Srinath, M.S.; Manavalan, R. Synthesis and characterization studies of cisplatin/hydroxypropyl-β-cyclodextrin complex. Pharmacologyoniline 2009, 1, 1135–1143. [Google Scholar]
- Desandes, E. Survival from adolescent cancer. Cancer Treat. Rev. 2007, 33, 69–615. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Sun, W.; Wang, H.; Zuo, D.; Hua, Y.; Cai, Z. Research progress on the multidrug resistance mechanisms of osteosarcoma chemotherapy and reversal. Tumor Biol. 2015, 36, 1329–1338. [Google Scholar] [CrossRef]
- Nedelcu, T.; Kubista, B.; Koller, A.; Sulzbacher, I.; Mosberger, I.; Arrich, F.; Trieb, K.; Kotz, R.; Toma, C.D. Livin and Bcl-2 expression in high-grade osteosarcoma. J. Cancer Res. Clin. Oncol. 2008, 134, 237–244. [Google Scholar] [CrossRef]
- Youlden, D.R.; Cramb, S.M.; Dunn, N.A.; Muller, J.M.; Pyke, C.M.; Baade, P.D. The descriptive epidemiology of female breast cancer: An international comparison of screening, incidence, survival and mortality. Cancer Epidemiol. 2012, 36, 212–216. [Google Scholar] [CrossRef]
- Wang, L.; WeiGuo, W.; Ze, R.; Zhou, D. The effective combination therapy against human osteosarcoma: Doxorubicin plus curcumin co-encapsulated lipid-coated polymeric nanoparticulate drug delivery system. Drug Deliv. 2016, 23, 3200–3208. [Google Scholar] [CrossRef]
- Buondonno, I.; Gazzano, E.; Jean, S.R.; Audrito, V.; Kopecka, J.; Fanelli, M.; Salaroglio, I.C.; Costamagna, C.; Roato, I.; Mungo, E.; et al. Mitochondria-targeted doxorubicin: A new therapeutic strategy against doxorubicin-resistant osteosarcoma. Mol. Cancer Ther. 2016, 15, 2640–2652. [Google Scholar] [CrossRef]
- Siu, P.; Sun, L.; Zhou, D.S.; Zhang, P.; Wang, Y.H.; Li, D.; Li, Q.H.; Feng, R.J. Development of alendronate-conjugated poly(lactic-co-glycolic acid)-dextran nanoparticles for active targeting of cisplatin in osteosarcoma. Sci. Rep. 2015, 5, 17387. [Google Scholar]
- Van Leeuwen, B.L.; Kamps, W.A.; Jansen, H.W.B.; Hoekstra, H.J. The effect of chemotherapy on the growing skeleton. Cancer Treat. Rev. 2000, 26, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Ostrovidov, S.; Annabi, N.; Seidi, A.; Ramalingam, M.; Dehghani, F.; Kaji, H.; Khademhosseini, A. Controlled release of drugs from gradient hydrogels for high throughput analysis of cell-drug interactions. Anal. Chem. 2012, 84, 1302–1309. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhang, B. Doxorubicin induces cardiotoxicity through upregulation of death receptors mediated apoptosis in cardiomyocytes. Sci. Rep. 2017, 7, 44735. [Google Scholar] [CrossRef] [PubMed]
- Zagar, T.M.; Cardinale, D.M.; Marks, L.B. Breast cancer therapy-associated cardiovascular disease. Nat. Rev. Clin. Oncol. 2016, 13, 172–184. [Google Scholar] [CrossRef]
- Yao, X.; Panichpisal, K.; Kurtzman, N.; Nugent, K. Cisplatin nephrotoxicity: A review. Am. J. Med. Sci. 2007, 334, 115–124. [Google Scholar] [CrossRef]
- Miller, R.P.; Tadagavadi, R.K.; Ramesh, G.; Reeves, W.B. Mechanisms of cisplatin nephrotoxicity. Toxins 2010, 2, 2490–2518. [Google Scholar] [CrossRef]









© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, S.J.; Moon, Y.J.; Chun, H.J.; Yang, D.H. Doxorubicin·Hydrochloride/Cisplatin-Loaded Hydrogel/Nanosized (2-Hydroxypropyl)-Beta-Cyclodextrin Local Drug-Delivery System for Osteosarcoma Treatment In Vivo . Nanomaterials 2019, 9, 1652. https://doi.org/10.3390/nano9121652
Yoon SJ, Moon YJ, Chun HJ, Yang DH. Doxorubicin·Hydrochloride/Cisplatin-Loaded Hydrogel/Nanosized (2-Hydroxypropyl)-Beta-Cyclodextrin Local Drug-Delivery System for Osteosarcoma Treatment In Vivo . Nanomaterials. 2019; 9(12):1652. https://doi.org/10.3390/nano9121652
Chicago/Turabian StyleYoon, Sun Jung, Young Jae Moon, Heung Jae Chun, and Dae Hyeok Yang. 2019. "Doxorubicin·Hydrochloride/Cisplatin-Loaded Hydrogel/Nanosized (2-Hydroxypropyl)-Beta-Cyclodextrin Local Drug-Delivery System for Osteosarcoma Treatment In Vivo " Nanomaterials 9, no. 12: 1652. https://doi.org/10.3390/nano9121652
APA StyleYoon, S. J., Moon, Y. J., Chun, H. J., & Yang, D. H. (2019). Doxorubicin·Hydrochloride/Cisplatin-Loaded Hydrogel/Nanosized (2-Hydroxypropyl)-Beta-Cyclodextrin Local Drug-Delivery System for Osteosarcoma Treatment In Vivo . Nanomaterials, 9(12), 1652. https://doi.org/10.3390/nano9121652