
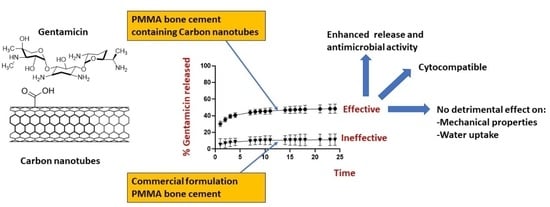
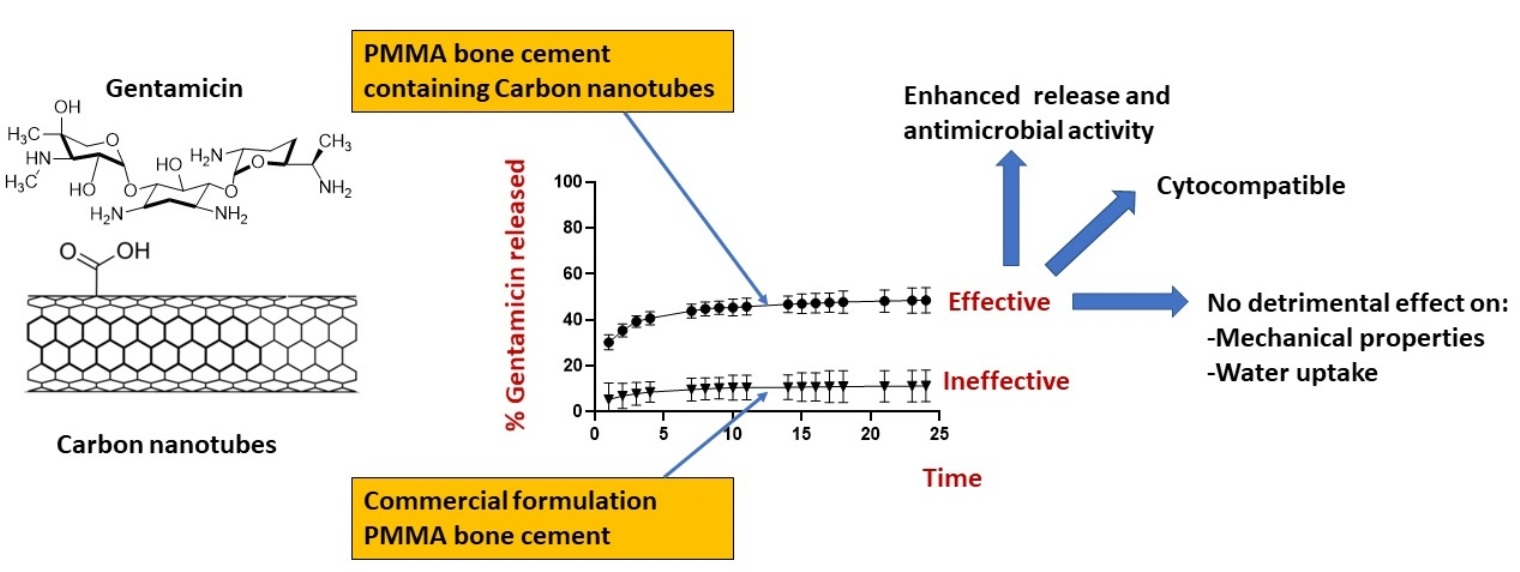
Antimicrobial PMMA Bone Cement Containing Long Releasing Multi-Walled Carbon Nanotubes


Abstract
1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Preparation of Gentamicin-Loaded CNT
2.3. Characterization for CNT and Gentamicin-Loaded CNTs
- Transmission electron microscope (TEM)
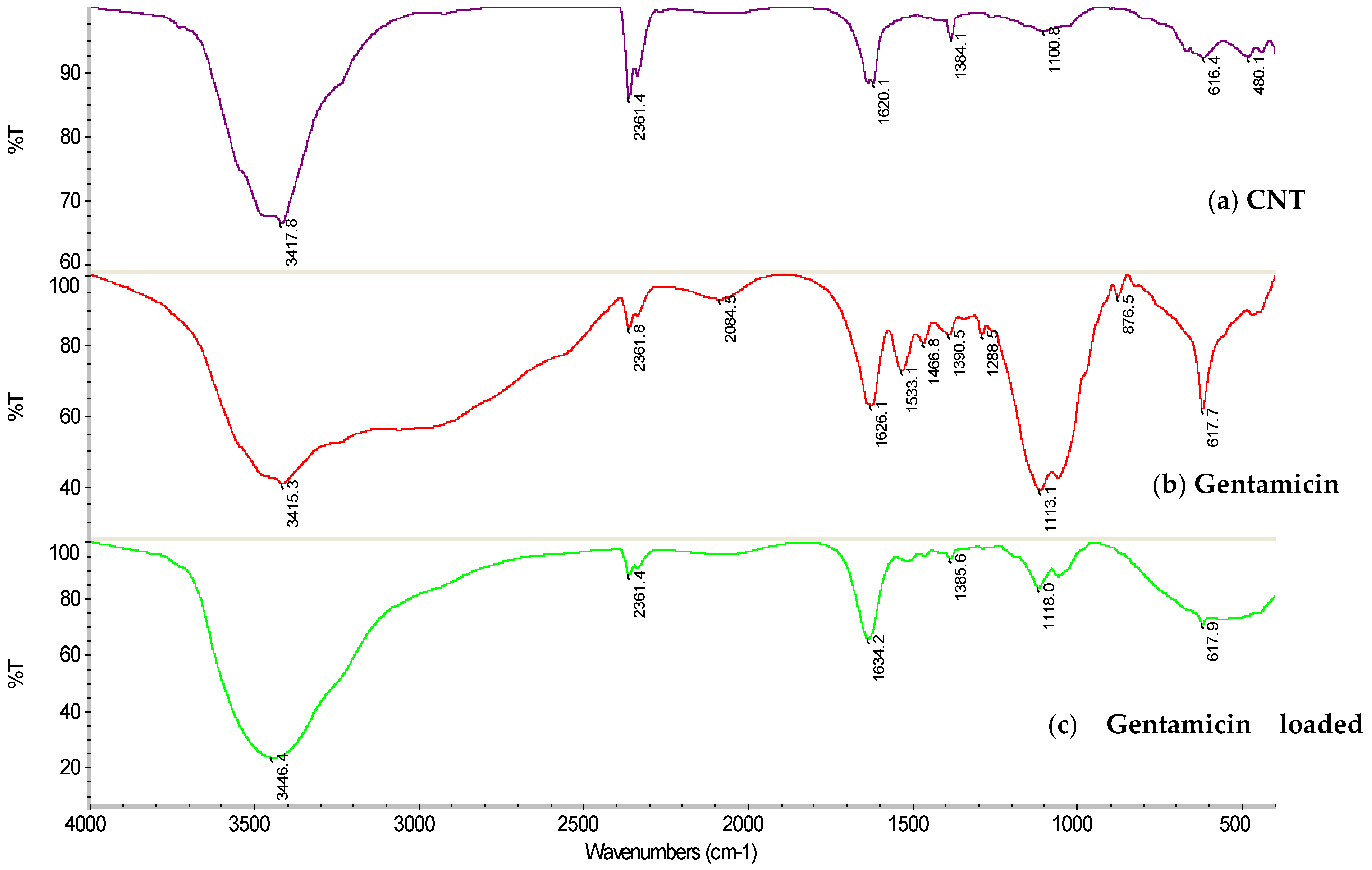
- Fourier-transformed infrared (FTIR)
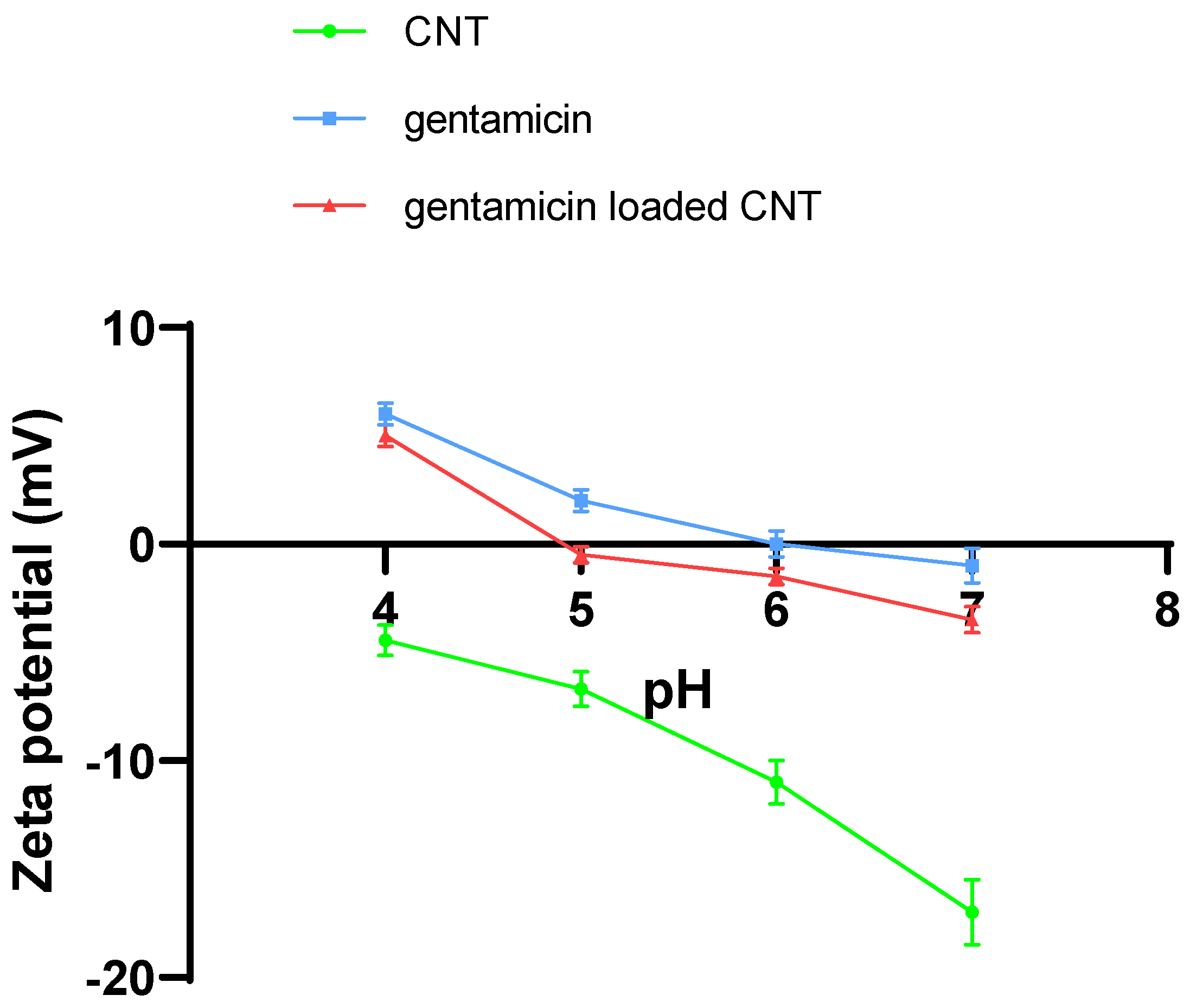
- Zeta potential measurements
2.4. Bone Cement Preparation
2.5. Gentamicin Release Quantification
2.6. Mechanical Testing
2.7. Water Uptake Testing
2.8. Agar Diffusion Assay
2.9. Cytotoxicity Analysis
- In vitro differentiation of HDFs
- MTT Assay
- LDH (lactate dehydrogenase) measurement
- Detection of calcium deposits (mineralization)
2.10. Statistical Analysis
3. Results
3.1. Characterization of CNT and Gentamicin-Loaded CNT
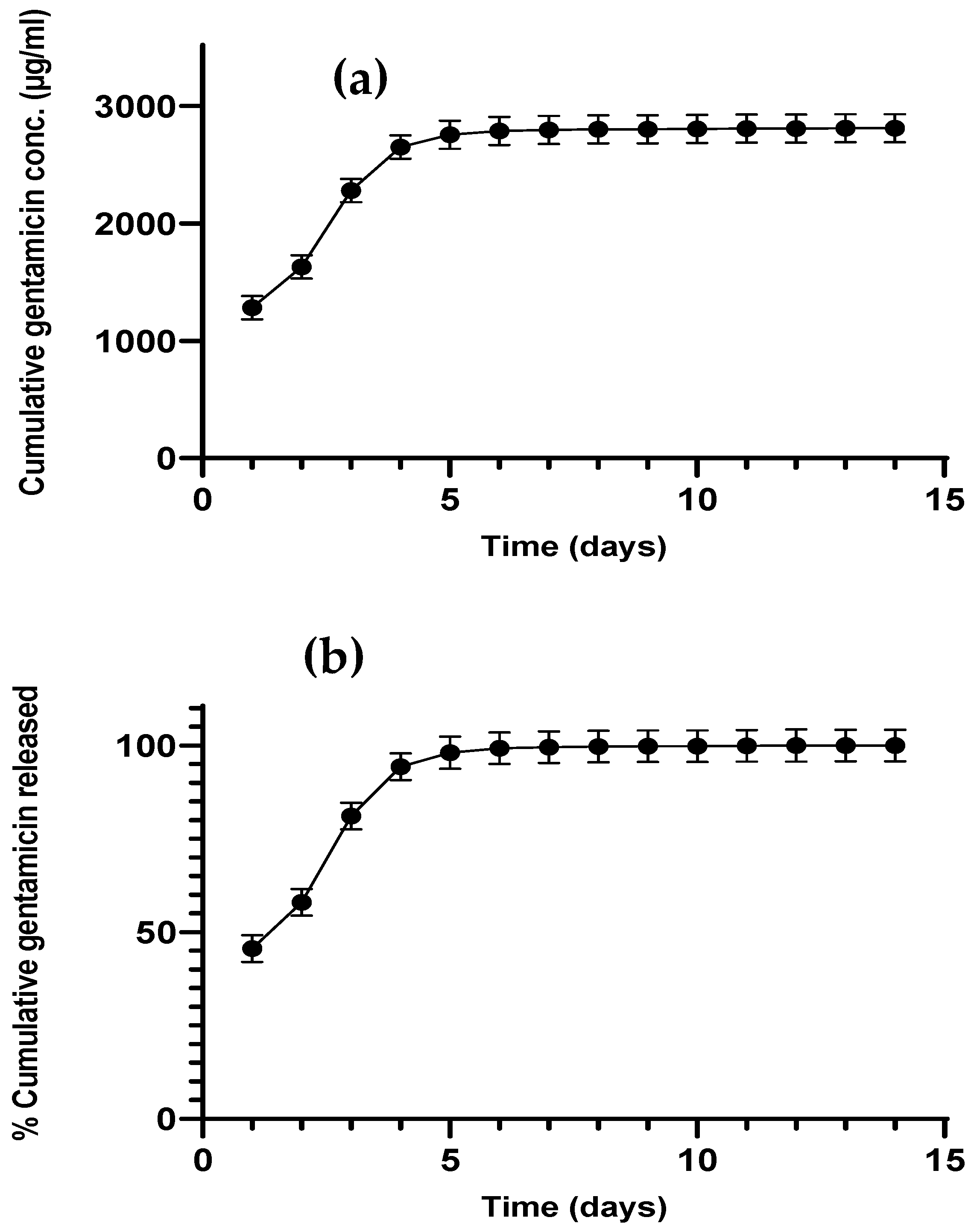
3.2. Gentamicin Release from CNTs
3.3. Gentamicin Release from Bone Cement
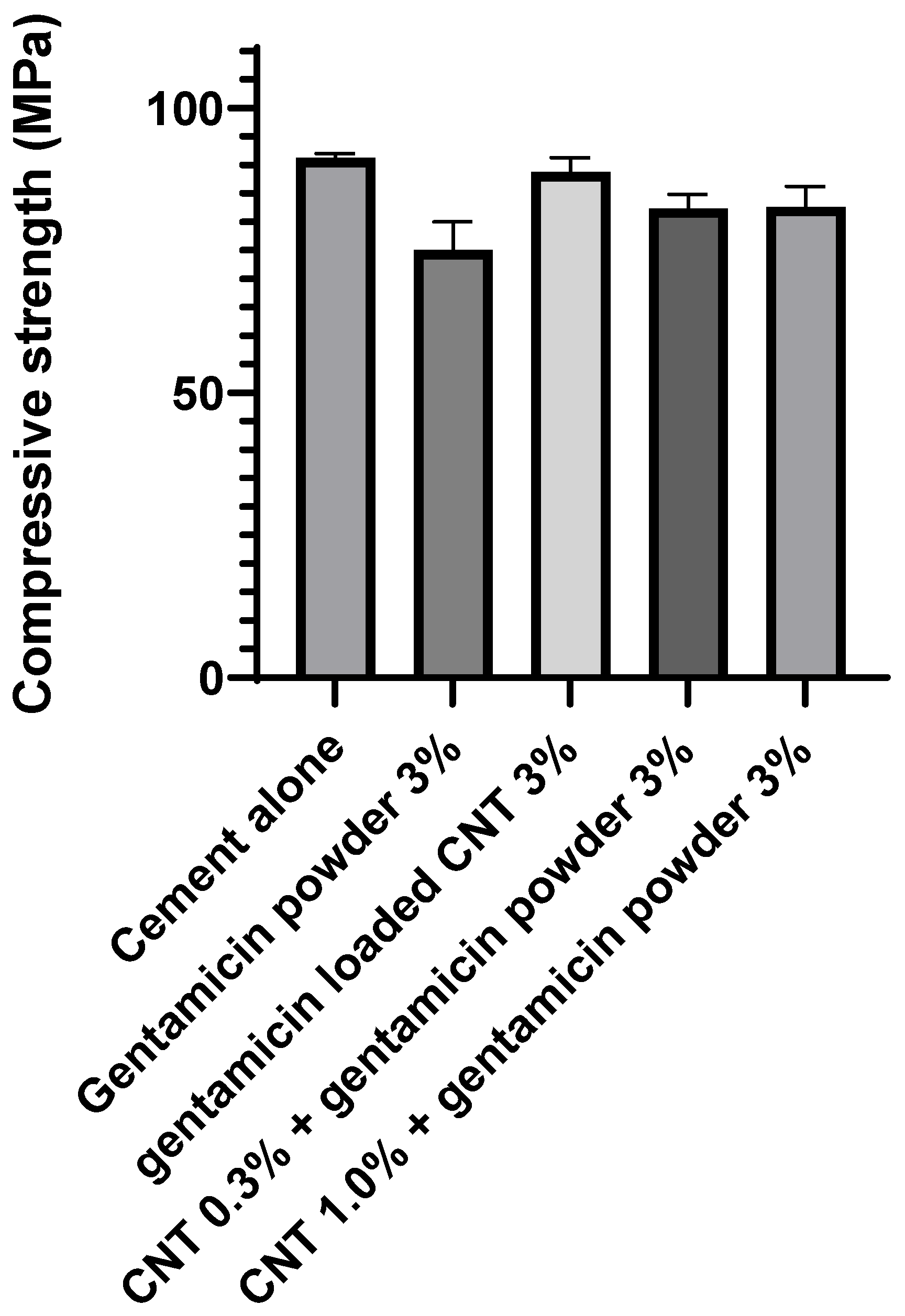
3.4. Mechanical Properties
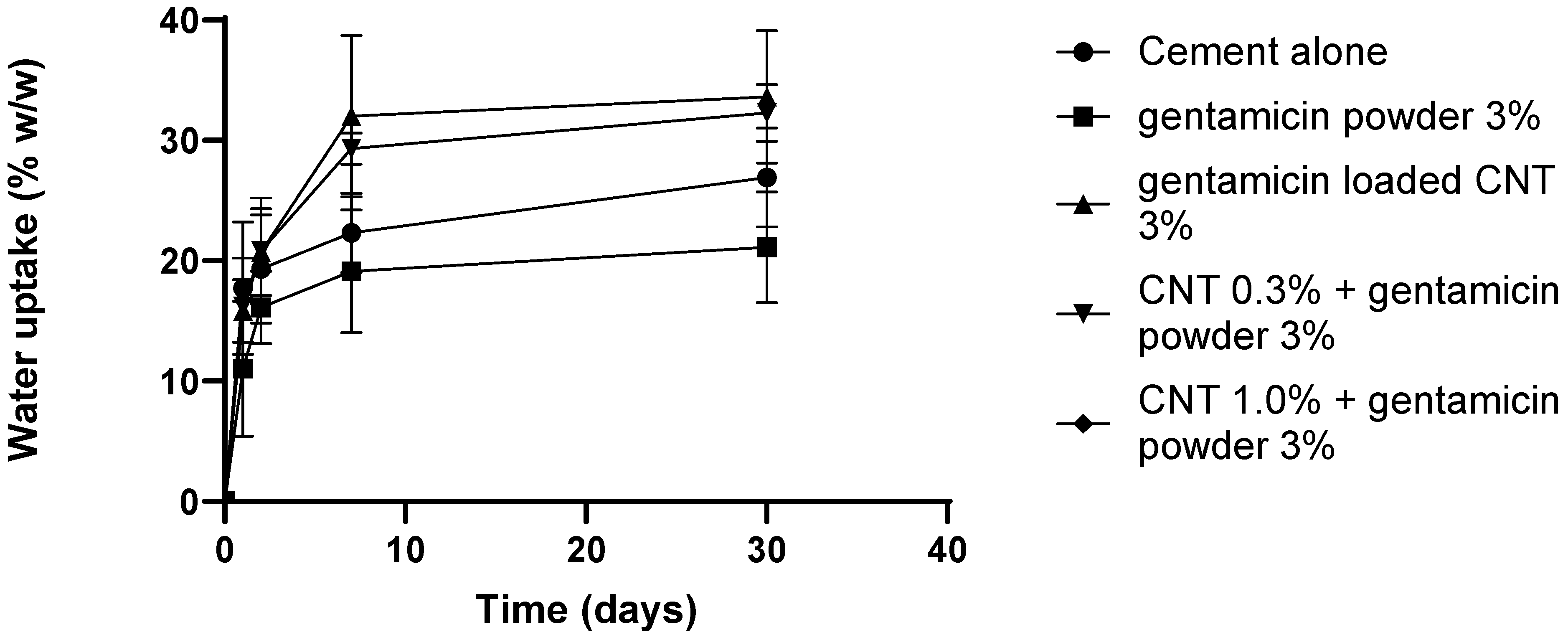
3.5. Water Uptake Study
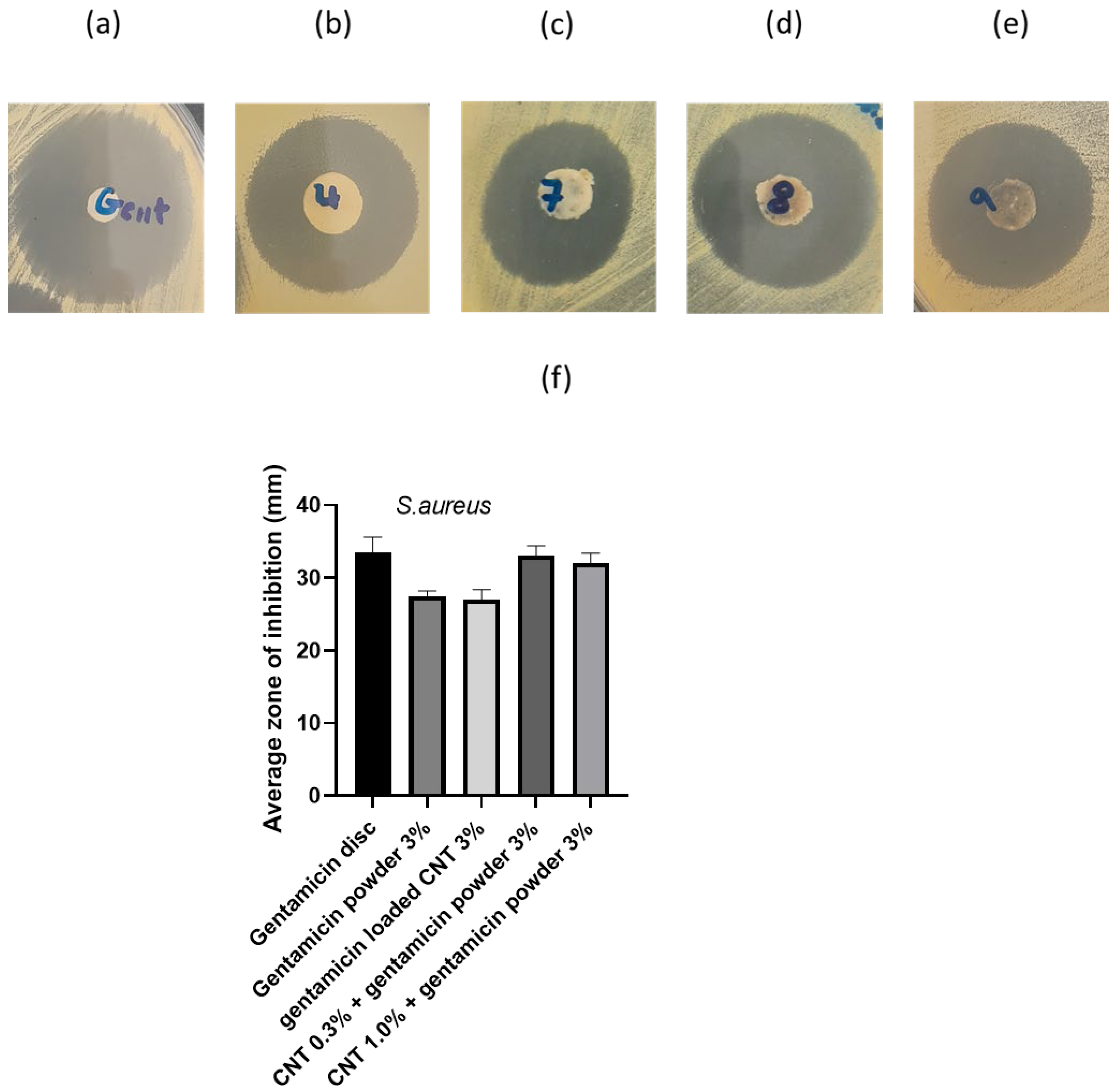
3.6. Antimicrobial Activity
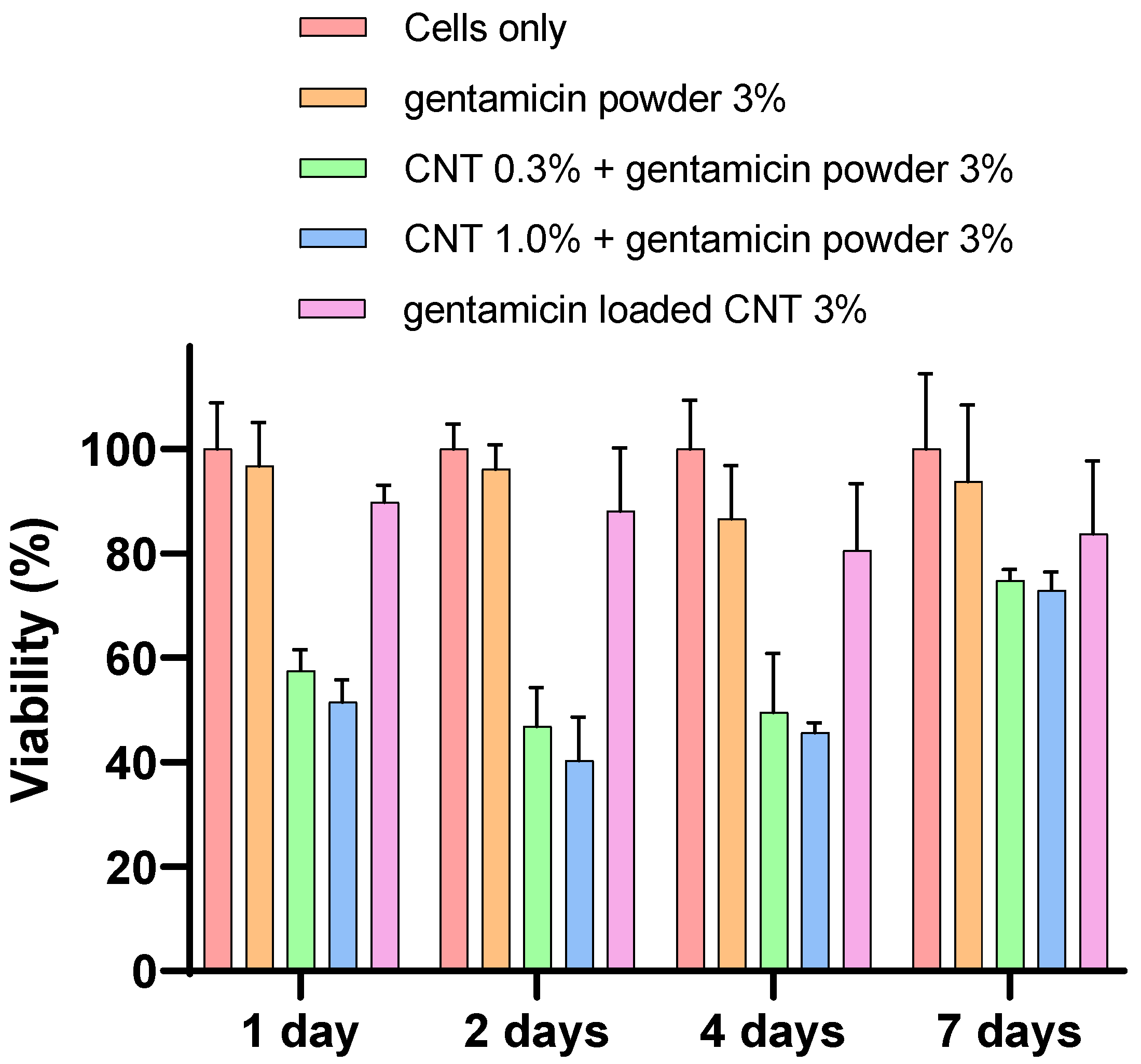
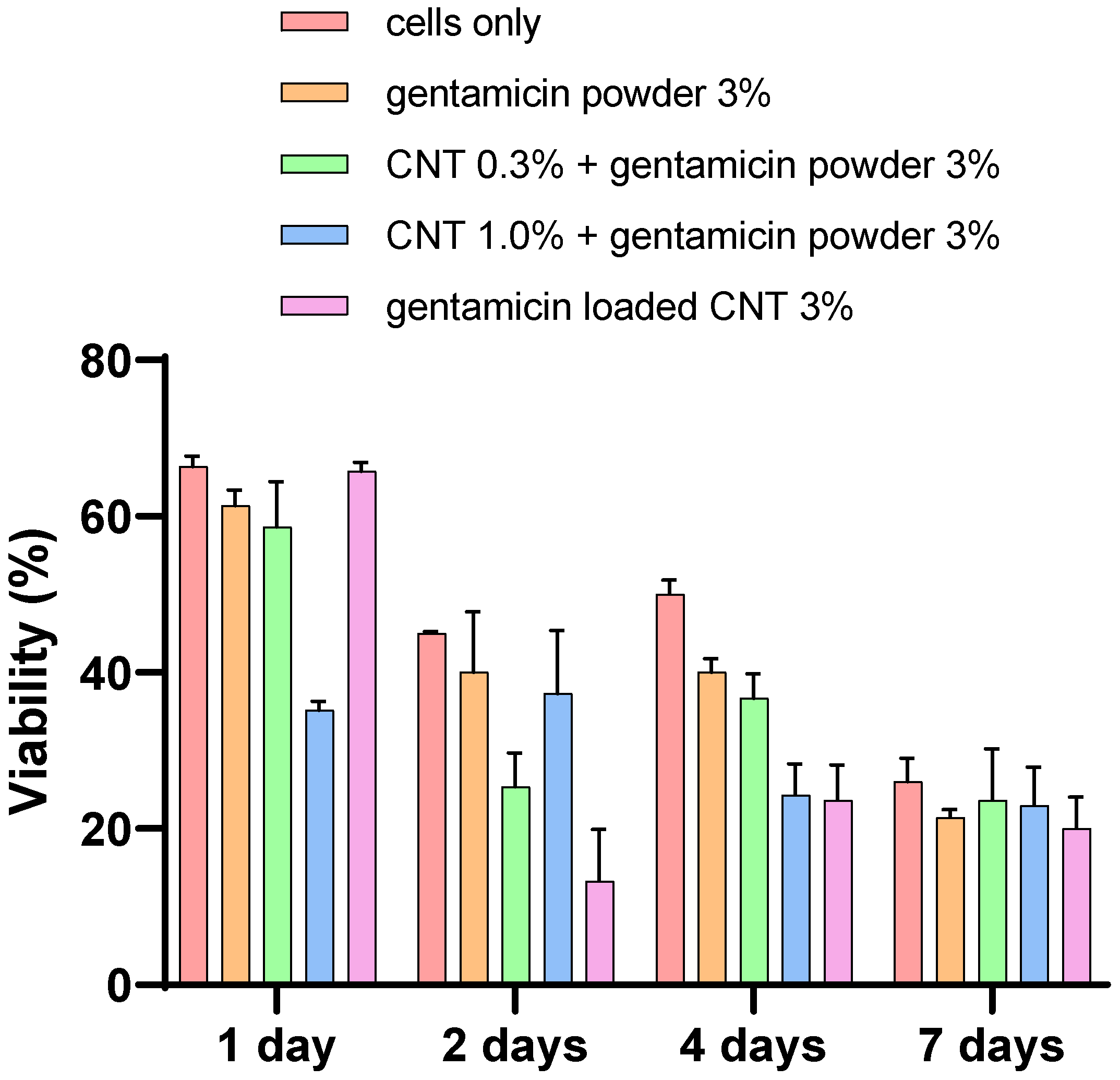
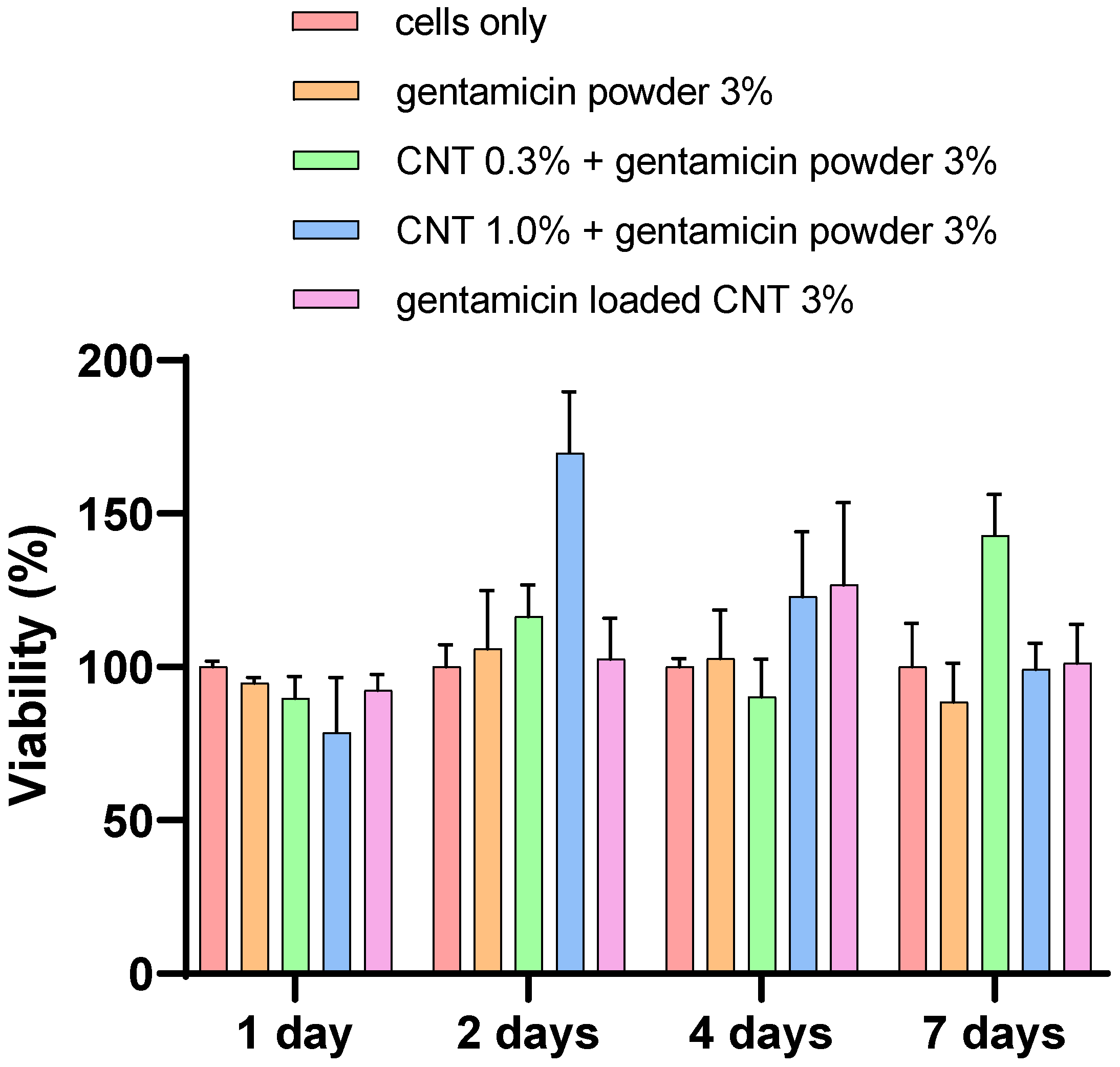
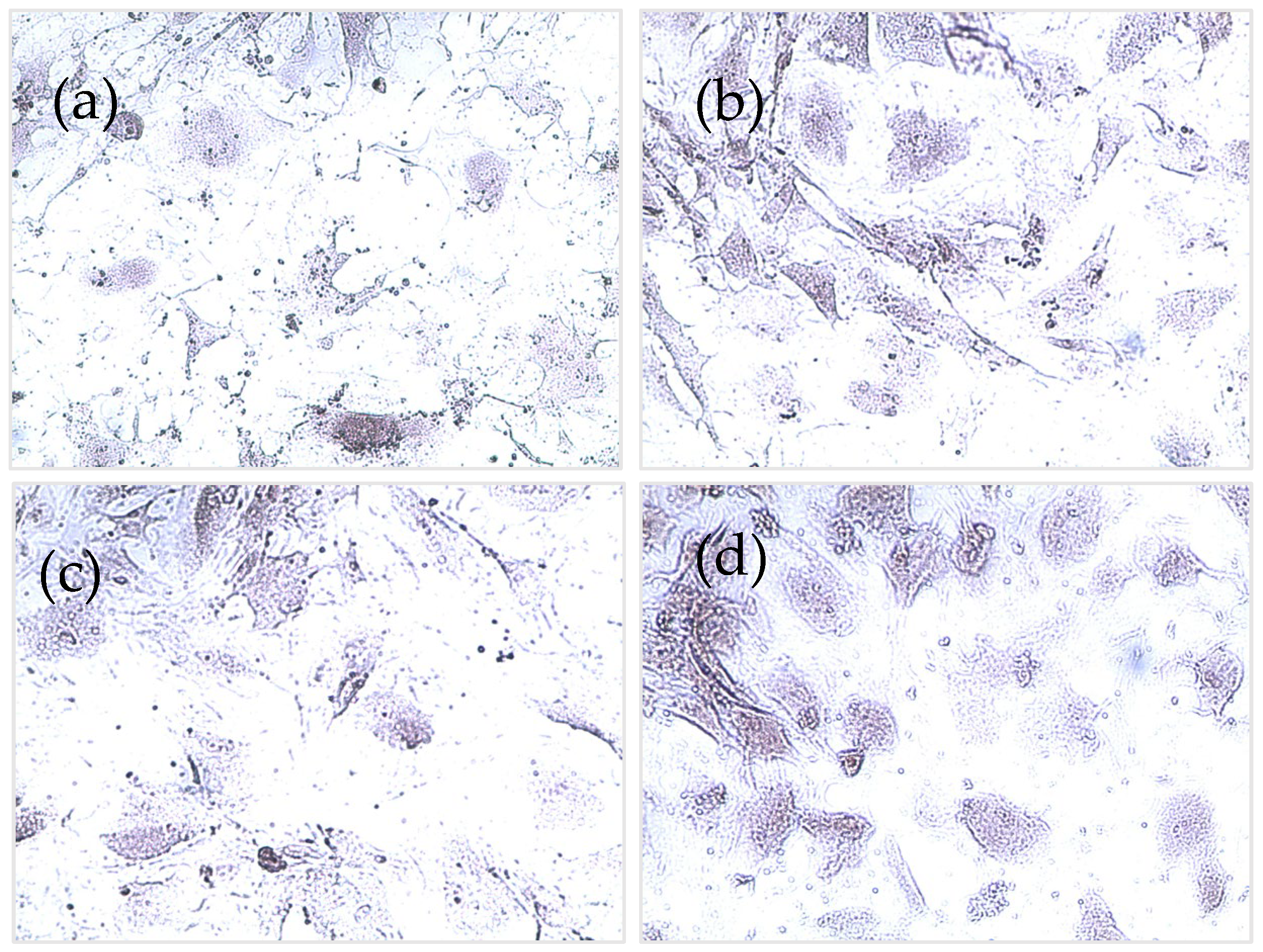
3.7. Cytotoxicity Analysis
- MTT assay
- LDH assay
- Alizarin red
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liddle, A.D.; Judge, A.; Pandit, H.; Murray, D.W. Adverse Outcomes after Total and Unicompartmental Knee Replacement in 101330 Matched Patients: A Study of Data from the National Joint Registry for England and Wales. Lancet 2014, 384, 1437–1445. [Google Scholar] [CrossRef]
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future Young Patient Demand for Primary and Revision Joint Replacement: National Projections from 2010 to 2030. Clin. Orthop. 2009, 467, 2606–2612. [Google Scholar] [CrossRef] [PubMed]
- Maradit Kremers, H.; Larson, D.R.; Noureldin, M.; Schleck, C.D.; Jiranek, W.A.; Berry, D.J. Long-Term Mortality Trends After Total Hip and Knee Arthroplasties: A Population-Based Study. J. Arthroplast. 2016, 31, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Cobo, J.; Del, P. Prosthetic Joint Infection: Diagnosis and Management. Expert Rev. Anti Infect. Ther. 2011, 9, 787–802. [Google Scholar] [CrossRef] [PubMed]
- Al Thaher, Y.; Alfuqaha, O.A.; Dweidari, A. Health-Related Quality of Life and Outcome after Total Knee Replacement: Results from a Cross-Sectional Survey in Jordan. Adv. Orthop. 2021, 2021, e5506809. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Watson, H.; Schmier, J.K.; Parvizi, J. Economic Burden of Periprosthetic Joint Infection in the United States. J. Arthroplast. 2012, 27, 61–65.e1. [Google Scholar] [CrossRef] [PubMed]
- Anagnostakos, K. Therapeutic Use of Antibiotic-Loaded Bone Cement in the Treatment of Hip and Knee Joint Infections. J. Bone Jt. Infect. 2017, 2, 29–37. [Google Scholar] [CrossRef]
- Chang, Y.; Tai, C.-L.; Hsieh, P.-H.; Ueng, S.W.N. Gentamicin in Bone Cement: A Potentially More Effective Prophylactic Measure of Infectionin Joint Arthroplasty. Bone Jt. Res. 2013, 2, 220–226. [Google Scholar] [CrossRef]
- Bertazzoni Minelli, E.; Benini, A.; Samaila, E.; Bondi, M.; Magnan, B. Antimicrobial Activity of Gentamicin and Vancomycin Combination in Joint Fluids after Antibiotic-Loaded Cement Spacer Implantation in Two-Stage Revision Surgery. J. Chemother. 2015, 27, 17–24. [Google Scholar] [CrossRef]
- Al Thaher, Y.; Perni, S.; Prokopovich, P. Nano-Carrier Based Drug Delivery Systems for Sustained Antimicrobial Agent Release from Orthopaedic Cementous Material. Adv. Colloid Interface Sci. 2017, 249, 234–247. [Google Scholar] [CrossRef]
- Liu, X.-W.; Zi, Y.; Xiang, L.-B.; Wang, Y. Total Hip Arthroplasty: Areview of Advances, Advantages and Limitations. Int. J. Clin. Exp. Med. 2015, 8, 27–36. [Google Scholar] [PubMed]
- Świeczko-Żurek, B.; Zieliński, A.; Bociąga, D.; Rosińska, K.; Gajowiec, G. Influence of Different Nanometals Implemented in PMMA Bone Cement on Biological and Mechanical Properties. Nanomaterials 2022, 12, 732. [Google Scholar] [CrossRef] [PubMed]
- Swearingen, M.C.; Granger, J.F.; Sullivan, A.; Stoodley, P. Elution of Antibiotics from Poly(Methyl Methacrylate) Bone Cement after Extended Implantation Does Not Necessarily Clear the Infection despite Susceptibility of the Clinical Isolates. Pathog. Dis. 2016, 74, ftv103. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Tande, A.J.; Patel, R. Prosthetic Joint Infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Wendling, A.; Mar, D.; Wischmeier, N.; Anderson, D.; McIff, T. Combination of Modified Mixing Technique and Low Frequency Ultrasound to Control the Elution Profile of Vancomycin-Loaded Acrylic Bone Cement. Bone Jt. Res. 2016, 5, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.; Chen, Y.-C.; Hsu, Y.-M.; Chang, C.-H. Enhancing Drug Release From Antibiotic-Loaded Bone Cement Using Porogens. J. Am. Acad. Orthop. Surg. 2016, 24, 188–195. [Google Scholar] [CrossRef]
- Al Thaher, Y.; Yang, L.; Jones, S.A.; Perni, S.; Prokopovich, P. LbL-Assembled Gentamicin Delivery System for PMMA Bone Cements to Prolong Antimicrobial Activity. PLoS ONE 2018, 13, e0207753. [Google Scholar] [CrossRef]
- Thaher, Y.A.; Alotaibi, H.F.; Yang, L.; Prokopovich, P. PMMA Bone Cement Containing Long Releasing Silica-Based Chlorhexidine Nanocarriers. PLoS ONE 2021, 16, e0257947. [Google Scholar] [CrossRef]
- Ayre, W.N.; Birchall, J.C.; Evans, S.L.; Denyer, S.P. A Novel Liposomal Drug Delivery System for PMMA Bone Cements. J. Biomed. Mater. Res. B Appl. Biomater. 2015, 104, 1510–1524. [Google Scholar] [CrossRef]
- Wei, W.; Abdullayev, E.; Hollister, A.; Mills, D.; Lvov, Y.M. Clay Nanotube/Poly(Methyl Methacrylate) Bone Cement Composites with Sustained Antibiotic Release. Macromol. Mater. Eng. 2012, 297, 645–653. [Google Scholar] [CrossRef]
- Shen, S.-C.; Ng, W.K.; Dong, Y.-C.; Ng, J.; Tan, R.B.H. Nanostructured Material Formulated Acrylic Bone Cements with Enhanced Drug Release. Mater. Sci. Eng. C 2016, 58, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Ormsby, R.; McNally, T.; Mitchell, C.; Dunne, N. Incorporation of Multiwalled Carbon Nanotubes to Acrylic Based Bone Cements: Effects on Mechanical and Thermal Properties. J. Mech. Behav. Biomed. Mater. 2010, 3, 136–145. [Google Scholar] [CrossRef]
- Zeng, C.; Hossieny, N.; Zhang, C.; Wang, B.; Walsh, S.M. Morphology and Tensile Properties of PMMA Carbon Nanotubes Nanocomposites and Nanocomposites Foams. Compos. Sci. Technol. 2013, 82, 29–37. [Google Scholar] [CrossRef]
- Lewis, G. Properties of Nanofiller-Loaded Poly (Methyl Methacrylate) Bone Cement Composites for Orthopedic Applications: A Review. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 1260–1284. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Gao, H.; Uo, M.; Sato, Y.; Akasaka, T.; Feng, Q.; Cui, F.; Liu, X.; Watari, F. Effect of Carbon Nanotubes on Cellular Functions in Vitro. J. Biomed. Mater. Res. A 2009, 91, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, H.; Niu, X.; Yu, B.; Fan, Y.; Feng, Q.; Cui, F.; Watari, F. The Use of Carbon Nanotubes to Induce Osteogenic Differentiation of Human Adipose-Derived MSCs in Vitro and Ectopic Bone Formation in Vivo. Biomaterials 2012, 33, 4818–4827. [Google Scholar] [CrossRef]
- Li, X.; Gao, H.; Uo, M.; Sato, Y.; Akasaka, T.; Abe, S.; Feng, Q.; Cui, F.; Watari, F. Maturation of Osteoblast-like SaoS2 Induced by Carbon Nanotubes. Biomed. Mater. 2008, 4, 015005. [Google Scholar] [CrossRef]
- Gonçalves, G.; Portolés, M.-T.; Ramírez-Santillán, C.; Vallet-Regí, M.; Serro, A.P.; Grácio, J.; Marques, P.A.A.P. Evaluation of the in Vitro Biocompatibility of PMMA/High-Load HA/Carbon Nanostructures Bone Cement Formulations. J. Mater. Sci. Mater. Med. 2013, 24, 2787–2796. [Google Scholar] [CrossRef]
- ISO 5833:2002—Implants for Surgery—Acrylic Resin Cements. Available online: https://www.iso.org/standard/30980.html (accessed on 1 February 2022).
- Al Thaher, Y. Tailored Gentamicin Release from Silica Nanocarriers Coated with Polyelectrolyte Multilayers. Colloids Surf. Physicochem. Eng. Asp. 2021, 614, 126210. [Google Scholar] [CrossRef]
- Rathbone, C.R.; Cross, J.D.; Brown, K.V.; Murray, C.K.; Wenke, J.C. Effect of Various Concentrations of Antibiotics on Osteogenic Cell Viability and Activity. J. Orthop. Res. 2011, 29, 1070–1074. [Google Scholar] [CrossRef]
- Cha, H.; Lee, J.; Park, H.H.; Park, J.H. Direct Conversion of Human Fibroblasts into Osteoblasts Triggered by Histone Deacetylase Inhibitor Valproic Acid. Appl. Sci. 2020, 10, 7372. [Google Scholar] [CrossRef]
- Carbon Nanotube, Multi-Walled, Carboxylic Acid Functionalized Thin, Extent of Labeling: >8% Carboxylic Acid Functionalized, Avg. Diam. × L 9.5 Nm × 1.5 Μm|Sigma-Aldrich. Available online: http://www.sigmaaldrich.com/ (accessed on 8 April 2022).
- Fan, L.; Sun, W.; Zou, Y.; Xu, Q.; Zeng, R.-C.; Tian, J. Enhanced Corrosion Resistance, Antibacterial Activity and Biocompatibility of Gentamicin-Montmorillonite Coating on Mg Alloy-in Vitro and in Vivo Studies. J. Mater. Sci. Technol. 2022, 111, 167–180. [Google Scholar] [CrossRef]
- Zhao, J.; Liu, H.; Xue, P.; Tian, S.; Sun, S.; Lv, X. Highly-Efficient PVDF Adsorptive Membrane Filtration Based on Chitosan@CNTs-COOH Simultaneous Removal of Anionic and Cationic Dyes. Carbohydr. Polym. 2021, 274, 118664. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, M.; Monteiro, F.J.; Ferraz, M.P. Infection of Orthopedic Implants with Emphasis on Bacterial Adhesion Process and Techniques Used in Studying Bacterial-Material Interactions. Biomatter 2012, 2, 176–194. [Google Scholar] [CrossRef] [PubMed]
- Kong, L.; Cao, J.; Zhang, Y.; Ding, W.; Shen, Y. Risk Factors for Periprosthetic Joint Infection Following Primary Total Hip or Knee Arthroplasty: A Meta-Analysis. Int. Wound J. 2017, 14, 529–536. [Google Scholar] [CrossRef]
- Shuman, E.K.; Urquhart, A.; Malani, P.N. Management and Prevention of Prosthetic Joint Infection. Infect. Dis. Clin. N. Am. 2012, 26, 29–39. [Google Scholar] [CrossRef]
- Goldie, I.; Nachemson, A. Synovial PH in Rheumatoid Knee Joints: II. The Effect of Local Corticosteroid Treatment. Acta Orthop. Scand. 1970, 41, 354–362. [Google Scholar] [CrossRef]
- de Nadai, T.R.; de Nadai, M.N.; Albuquerque, A.A.S.; de Carvalho, M.T.M.; Celotto, A.C.; Evora, P.R.B. Metabolic Acidosis Treatment as Part of a Strategy to Curb Inflammation. Int. J. Inflamm. 2013, 2013, e601424. [Google Scholar] [CrossRef]
- Perni, S.; Caserta, S.; Pasquino, R.; Jones, S.A.; Prokopovich, P. Prolonged Antimicrobial Activity of PMMA Bone Cement with Embedded Gentamicin-Releasing Silica Nanocarriers. ACS Appl. Bio Mater. 2019, 2, 1850–1861. [Google Scholar] [CrossRef]
- Bechert, T.; Steinrücke, P.; Guggenbichler, J.-P. A New Method for Screening Anti-Infective Biomaterials. Nat. Med. 2000, 6, 1053–1056. [Google Scholar] [CrossRef]
- Trampuz, A.; Zimmerli, W. Prosthetic Joint Infections: Update in Diagnosis and Treatment. Swiss Med. Wkly. 2005, 135, 243–251. [Google Scholar] [PubMed]
- Jin, Z.; Pramoda, K.P.; Xu, G.; Goh, S.H. Dynamic Mechanical Behavior of Melt-Processed Multi-Walled Carbon Nanotube/Poly(Methyl Methacrylate) Composites. Chem. Phys. Lett. 2001, 337, 43–47. [Google Scholar] [CrossRef]
- Jia, Z.; Wang, Z.; Xu, C.; Liang, J.; Wei, B.; Wu, D.; Zhu, S. Study on Poly(Methyl Methacrylate)/Carbon Nanotube Composites. Mater. Sci. Eng. A 1999, 271, 395–400. [Google Scholar] [CrossRef]
- Goh, P.S.; Ismail, A.F.; Ng, B.C. Directional Alignment of Carbon Nanotubes in Polymer Matrices: Contemporary Approaches and Future Advances. Compos. Part Appl. Sci. Manuf. 2014, 56, 103–126. [Google Scholar] [CrossRef]
- Iijima, S. Helical Microtubules of Graphitic Carbon. Nature 1991, 354, 56–58. [Google Scholar] [CrossRef]
- Kearns, J.C.; Shambaugh, R.L. Polypropylene Fibers Reinforced with Carbon Nanotubes. J. Appl. Polym. Sci. 2002, 86, 2079–2084. [Google Scholar] [CrossRef]
- Hughes, K.F.; Ries, M.D.; Pruitt, L.A. Structural Degradation of Acrylic Bone Cements Due to in Vivo and Simulated Aging. J. Biomed. Mater. Res. A 2003, 65, 126–135. [Google Scholar] [CrossRef]
- Arnold, J.C.; Venditti, N.P. Effects of Environment on the Creep Properties of a Poly(Ethylmethacrylate) Based Bone Cement. J. Mater. Sci. Mater. Med. 2001, 12, 707–717. [Google Scholar] [CrossRef]
- Cenni, E.; Granchi, D.; Ciapetti, G.; Savarino, L.; Corradini, A.; Vancini, M.; Giunti, A. Gene Expression of Bone-Associated Cytokines in MG63 Osteoblast-like Cells Incubated with Acrylic Bone Cement Extracts in Minimum Essential Medium. J. Biomater. Sci. Polym. Ed. 2002, 13, 1283–1294. [Google Scholar] [CrossRef]
- Bordea, I.R.; Candrea, S.; Alexescu, G.T.; Bran, S.; Băciuț, M.; Băciuț, G.; Lucaciu, O.; Dinu, C.M.; Todea, D.A. Nano-Hydroxyapatite Use in Dentistry: A Systematic Review. Drug Metab. Rev. 2020, 52, 319–332. [Google Scholar] [CrossRef]
- Ormsby, R.; McNally, T.; O’Hare, P.; Burke, G.; Mitchell, C.; Dunne, N. Fatigue and Biocompatibility Properties of a Poly(Methyl Methacrylate) Bone Cement with Multi-Walled Carbon Nanotubes. Acta Biomater. 2012, 8, 1201–1212. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yu, B.; Fan, Y.; Ormsby, R.W.; McCarthy, H.O.; Dunne, N.; Li, X. Incorporation of Multi-Walled Carbon Nanotubes to PMMA Bone Cement Improves Cytocompatibility and Osseointegration. Mater. Sci. Eng. C 2019, 103, 109823. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Property | Unit | Value | Method of Measurement |
|---|---|---|---|
| Average diameter | 10−9 m | 9.5 | TEM |
| Average length | μm | 1.5 | TEM |
| Carbon content | % | >87 | TGA (thermal gravimetric analyzer) |
| Surface area | m2/g | 500 | BET (Brunauer, Emmett, and Teller) |
| –COOH groups (surface modification) | % | 10 | XPS (X-ray photoelectron spectroscopy) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Thaher, Y.; Khalil, R.; Abdelghany, S.; Salem, M.S. Antimicrobial PMMA Bone Cement Containing Long Releasing Multi-Walled Carbon Nanotubes. Nanomaterials 2022, 12, 1381. https://doi.org/10.3390/nano12081381
Al Thaher Y, Khalil R, Abdelghany S, Salem MS. Antimicrobial PMMA Bone Cement Containing Long Releasing Multi-Walled Carbon Nanotubes. Nanomaterials. 2022; 12(8):1381. https://doi.org/10.3390/nano12081381
Chicago/Turabian StyleAl Thaher, Yazan, Raida Khalil, Sharif Abdelghany, and Mutaz S. Salem. 2022. "Antimicrobial PMMA Bone Cement Containing Long Releasing Multi-Walled Carbon Nanotubes" Nanomaterials 12, no. 8: 1381. https://doi.org/10.3390/nano12081381
APA StyleAl Thaher, Y., Khalil, R., Abdelghany, S., & Salem, M. S. (2022). Antimicrobial PMMA Bone Cement Containing Long Releasing Multi-Walled Carbon Nanotubes. Nanomaterials, 12(8), 1381. https://doi.org/10.3390/nano12081381