

Development of Lipidic Nanoplatform for Intra-Oral Delivery of Chlorhexidine: Characterization, Biocompatibility, and Assessment of Depth of Penetration in Extracted Human Teeth

Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Preparation of Liposomal CHX
2.3. Characterization of Liposomal CHX
2.3.1. Determination of Particle Size, Poly-Dispersibility Index (PDI), and Zeta Potential
2.3.2. Determination of Encapsulation Efficiency
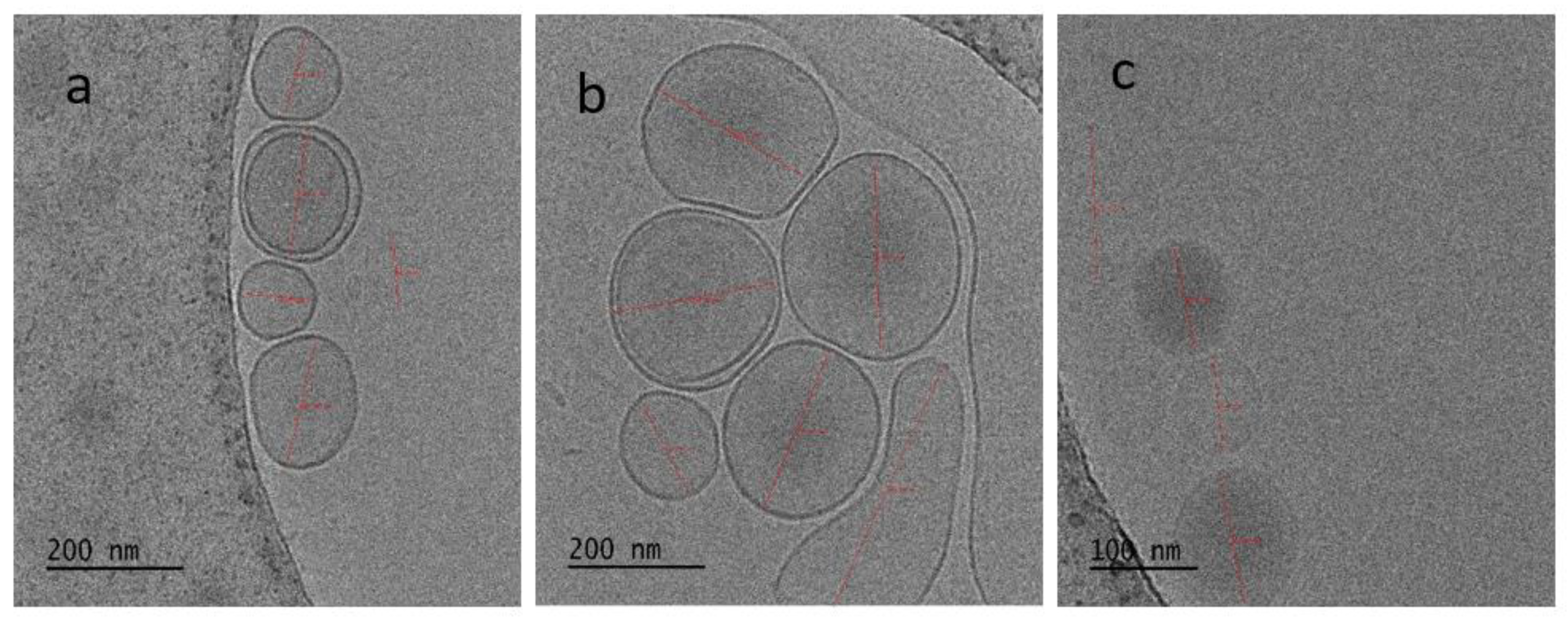
2.3.3. Surface Morphology
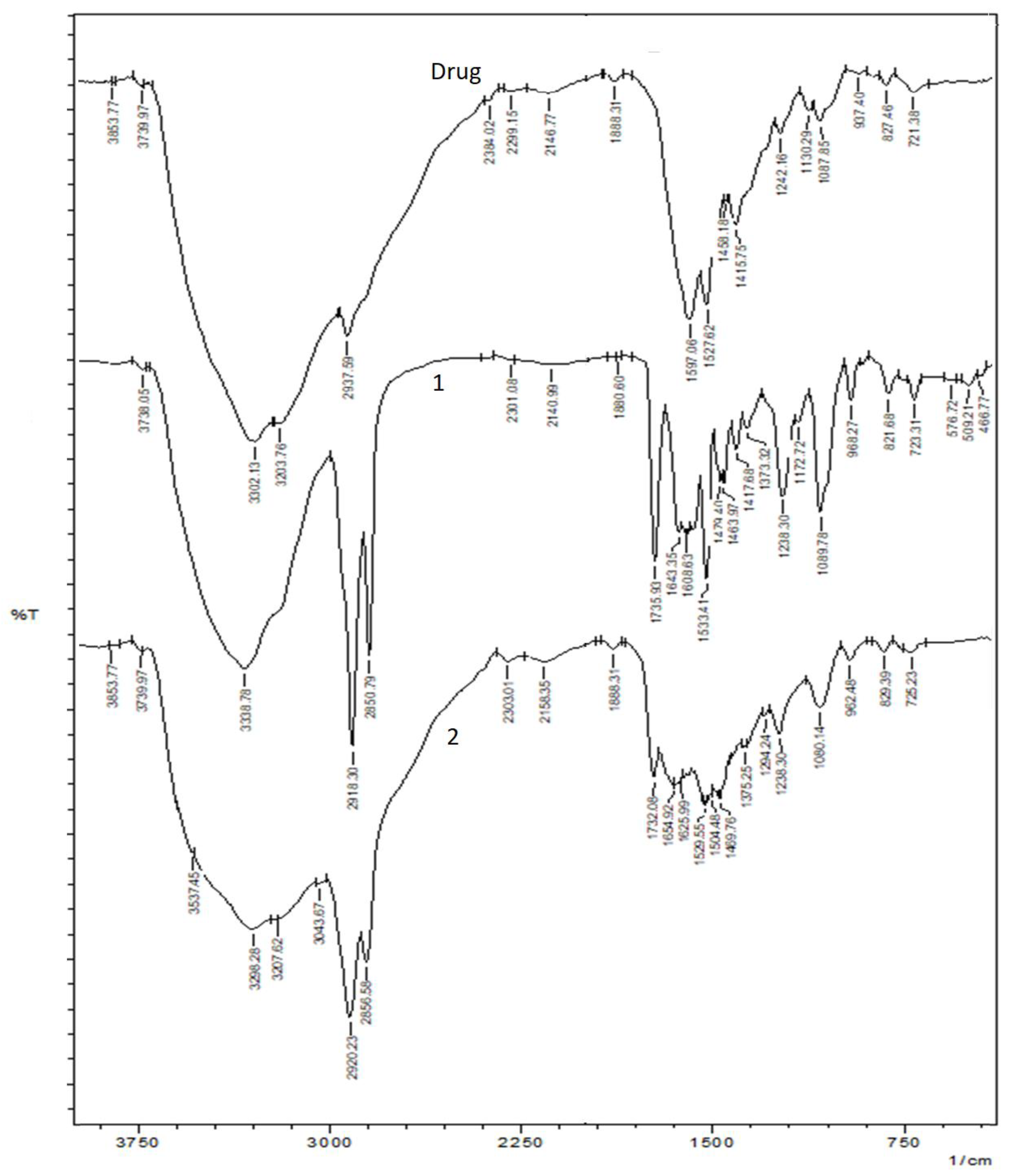
2.4. Fourier-Transform Infrared Spectroscopy (FTIR)
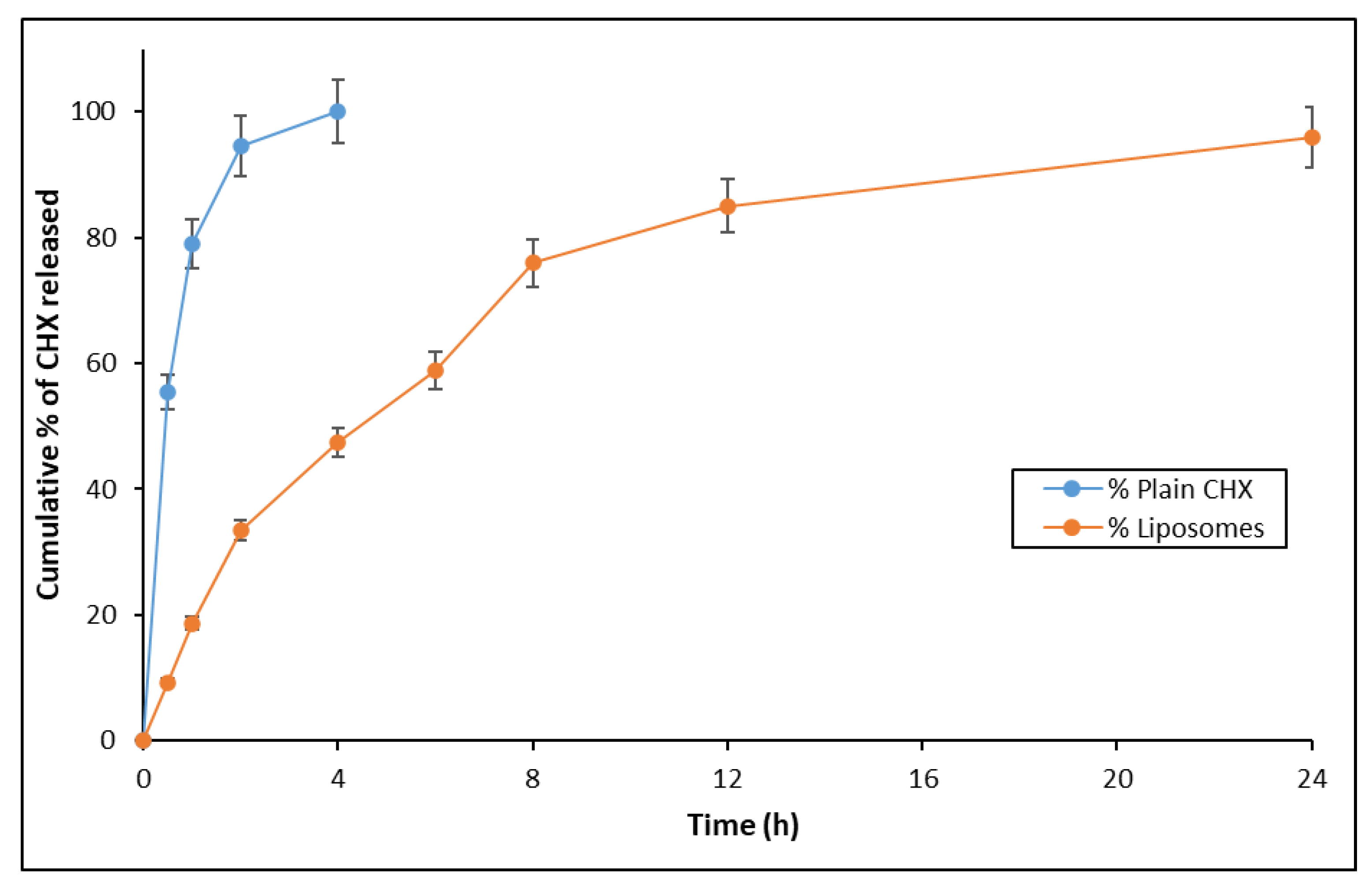
2.5. In Vitro Drug Release Study
2.6. Preparation of the Teeth for Experimentation
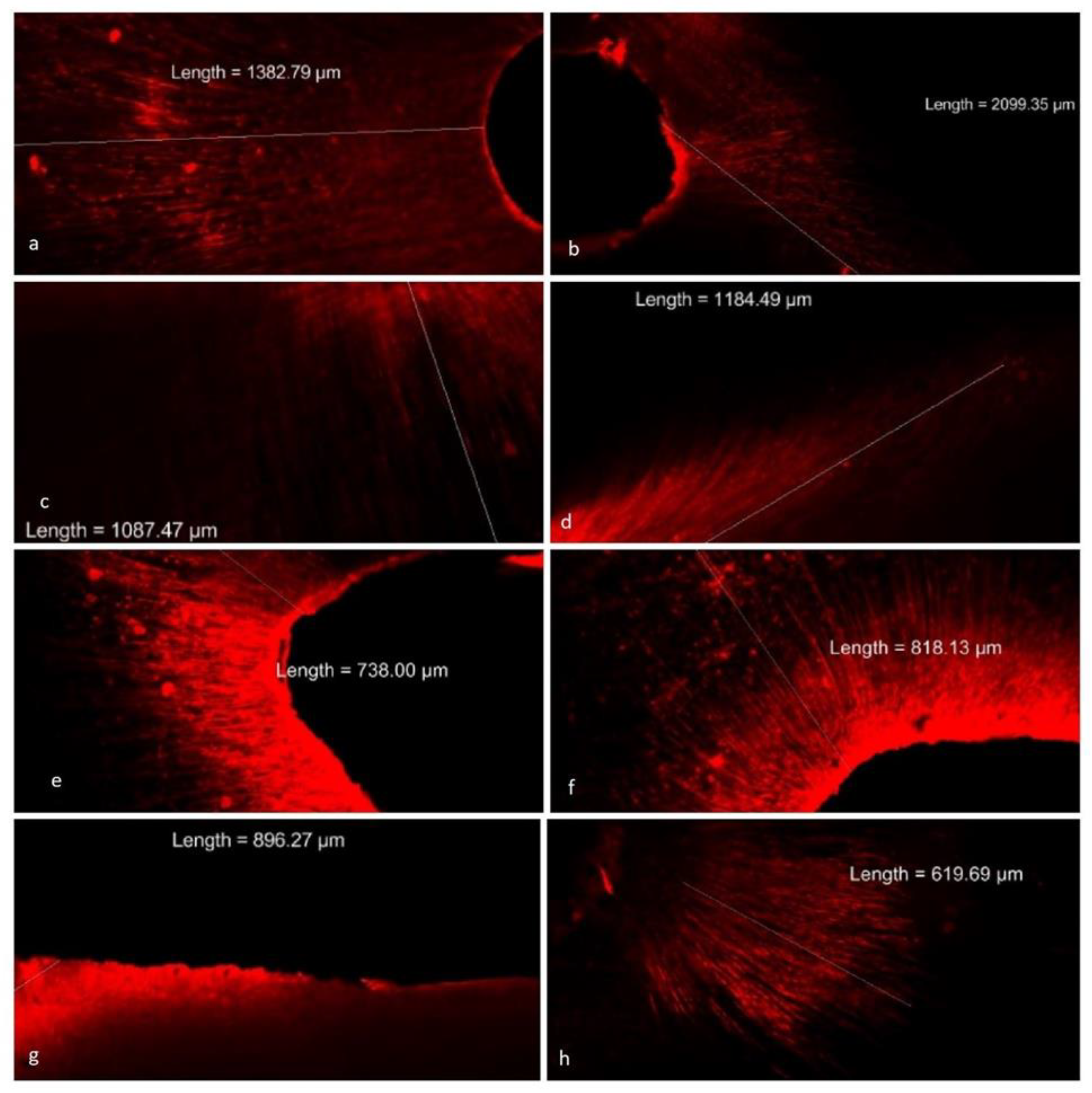
2.7. Determination of Depth of Penetration of Liposomal CHX in Dentinal Tubules
2.8. Cell Viability Assay
2.9. Antimicrobial Study
2.10. Statistical Analysis
3. Results
3.1. Preparation and Characterization of Liposomal CHX
3.2. In Vitro Drug Release Study
3.3. Evaluation of Liposomal CHX with Respect to Depth of Penetration in Dentinal Tubules
3.4. Antimicrobial Assay
3.5. Cell Viability Assay
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shrestha, A.; Fong, S.-W.; Khoo, B.-C.; Kishen, A. Delivery of Antibacterial Nanoparticles into Dentinal Tubules Using High-Intensity Focused Ultrasound. J. Endod. 2009, 35, 1028–1033. [Google Scholar] [CrossRef] [PubMed]
- Gendron, R.; Grenier, D.; Sorsa, T.; Mayrand, D. Inhibition of the Activities of Matrix Metalloproteinases 2, 8, and 9 by Chlorhexidine. Clin. Diagn. Lab. Immunol. 1999, 6, 437–439. [Google Scholar] [CrossRef]
- Haapasalo, M.; Shen, Y.; Qian, W.; Gao, Y. Irrigation in Endodontics. Dent. Clin. N. Am. 2010, 54, 291–312. [Google Scholar] [CrossRef]
- Gomes, C.; Moreira, R.G.; Castell-Perez, E. Poly (DL-Lactide-Co-Glycolide) (PLGA) Nanoparticles with Entrapped Trans-Cinnamaldehyde and Eugenol for Antimicrobial Delivery Applications. J. Food Sci. 2011, 76, N16–N24. [Google Scholar] [CrossRef] [PubMed]
- Hulsmann, M.; Hahn, W. Complications during Root Canal Irrigation-Literature Review and Case Reports. Int. Endod. J. 2000, 33, 186–193. [Google Scholar] [CrossRef]
- Faras, F.; Abo-Alhassan, F.; Sadeq, A.; Burezq, H. Complication of Improper Management of Sodium Hypochlorite Accident during Root Canal Treatment. J. Int. Soc. Prevent. Communit. Dent. 2016, 6, 493. [Google Scholar] [CrossRef] [PubMed]
- Peters, L.; Wesselink, P.; Buijs, J.; Vanwinkelhoff, A. Viable Bacteria in Root Dentinal Tubules of Teeth with Apical Periodontitis. J. Endod. 2001, 27, 76–81. [Google Scholar] [CrossRef]
- Priyadarshini, B.M.; Selvan, S.T.; Lu, T.B.; Xie, H.; Neo, J.; Fawzy, A.S. Chlorhexidine Nanocapsule Drug Delivery Approach to the Resin-Dentin Interface. J. Dent. Res. 2016, 95, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Chrai, S.S.; Murari, R.; Ahmad, I. Liposomes (a Review), Part One: Manufacturing Issues. BioPharm 2001, 14, 4. [Google Scholar]
- Kanumuru, P.K. Comparison of Penetration of Irrigant Activated by Traditional Methods with A Novel Technique. J. Clin. Diagn. Res. 2015, 9, ZC44. [Google Scholar] [CrossRef]
- Vadhana, S.; Latha, J.; Velmurugan, N. Evaluation of Penetration Depth of 2% Chlorhexidine Digluconate into Root Dentinal Tubules Using Confocal Laser Scanning Microscope. Restor. Dent. Endod. 2015, 40, 149. [Google Scholar] [CrossRef] [PubMed]
- Moyá, M.L.; López-López, M.; Lebrón, J.A.; Ostos, F.J.; Pérez, D.; Camacho, V.; Beck, I.; Merino-Bohórquez, V.; Camean, M.; Madinabeitia, N.; et al. Preparation and Characterization of New Liposomes. Bactericidal Activity of Cefepime Encapsulated into Cationic Liposomes. Pharmaceutics 2019, 11, 69. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, D.; Marley, J.; Hartwell, G. The Effect of Chlorhexidine Gluconate as an Endodontic Irrigant on the Apical Seal: Long-Term Results. J. Endod. 2003, 29, 91–94. [Google Scholar] [CrossRef]
- Managuli, R.S.; Wang, J.T.; Faruqu, F.N.; Kushwah, V.; Raut, S.Y.; Shreya, A.B.; Al-Jamal, K.T.; Jain, S.; Mutalik, S. Asenapine Maleate-Loaded Nanostructured Lipid Carriers: Optimization and in Vitro, Ex Vivo and in Vivo Evaluations. Nanomedicine 2019, 14, 889–910. [Google Scholar] [CrossRef] [PubMed]
- Manikkath, J.; Parekh, H.S.; Mutalik, S. Surface-Engineered Nanoliposomes with Lipidated and Non-Lipidated Peptide-Dendrimeric Scaffold for Efficient Transdermal Delivery of a Therapeutic Agent: Development, Characterization, Toxicological and Preclinical Performance Analyses. Eur. J. Pharm. Biopharm. 2020, 156, 97–113. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Leung, K.C.-F.; Wong, C.-H.; Lee, S.-F.; Li, X.; Leung, P.C.; Lau, C.B.S.; Wat, E.; Jin, L. Nanoparticle-Encapsulated Chlorhexidine against Oral Bacterial Biofilms. PLoS ONE 2014, 9, e103234. [Google Scholar] [CrossRef] [PubMed]
- Law, S.L.; Shih, C.L. Characterization of Calcitonin-Containing Liposome Formulations for Intranasal Delivery. J. Microencapsul. 2001, 18, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Quiram, G.; Montagner, F.; Palmer, K.; Stefan, M.; Washington, K.; Rodrigues, D. Novel Chlorhexidine-Loaded Polymeric Nanoparticles for Root Canal Treatment. J. Funct. Biomater. 2018, 9, 29. [Google Scholar] [CrossRef]
- Managuli, R.S.; Wang, J.T.-W.; Faruqu, F.M.; Pandey, A.; Jain, S.; Al-Jamal, K.T.; Mutalik, S. Surface Engineered Nanoliposomal Platform for Selective Lymphatic Uptake of Asenapine Maleate: In Vitro and in Vivo Studies. Mater. Sci. Eng. C 2020, 109, 110620. [Google Scholar] [CrossRef]
- Costalonga, B.L.; da Silva, R.C.; Caseli, L.; Molina, C. Interaction of chlorhexidine with biomembrane models on glass ionomer by using the Langmuir-Blodgett technique. Colloids Surf. B Biointerfaces 2012, 97, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Zorko, M.; Jerala, R. Alexidine and Chlorhexidine bind to lipopolysaccharide and lipoteichoic acid and prevent cell activation by antibiotics. J. Antimicrob. Chemother. 2008, 62, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Yacoub, T.J.; Reddy, A.S.; Szleifer, I. Structural Effects and Translocation of Doxorubicin in a DPPC/Chol Bilayer: The Role of Cholesterol. Biophys. J. 2011, 101, 378–385. [Google Scholar] [CrossRef]
- Ahmed, K.S.; Hussein, S.A.; Ali, A.H.; Korma, S.A.; Lipeng, Q.; Jinghua, C. Liposome: Composition, Characterisation, Preparation, and Recent Innovation in Clinical Applications. J. Drug Target. 2019, 27, 742–761. [Google Scholar] [CrossRef] [PubMed]
- Caddeo, C.; Teskač, K.; Sinico, C.; Kristl, J. Effect of Resveratrol Incorporated in Liposomes on Proliferation and UV-B Protection of Cells. Int. J. Pharm. 2008, 363, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Ahad, A.; Aqil, M.; Kohli, K.; Sultana, Y.; Mujeeb, M.; Ali, A. Formulation and Optimization of Nanotransfersomes Using Experimental Design Technique for Accentuated Transdermal Delivery of Valsartan. Nanomed. Nanotechnol. Biol. Med. 2012, 8, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Amplified Antimicrobial Action of Chlorhexidine Encapsulated in PDAC-Functionalized Acrylate Copolymer Nanogel Carriers|Semantic Scholar. Available online: https://www.semanticscholar.org/paper/Amplified-antimicrobial-action-of-chlorhexidine-in-Al-Awady-Weldrick/28d46efae97243ffacd9237e573383d72c26d885 (accessed on 20 January 2022).
- Chonkar, A.D.; Rao, J.V.; Managuli, R.S.; Mutalik, S.; Dengale, S.; Jain, P.; Udupa, N. Development of Fast Dissolving Oral Films Containing Lercanidipine HCl Nanoparticles in Semicrystalline Polymeric Matrix for Enhanced Dissolution and Ex Vivo Permeation. Eur. J. Pharm. Biopharm. 2016, 103, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Bedran-Russo, A.K.; Wu, C.D. In Vitro Remineralization Effects of Grape Seed Extract on Artificial Root Caries. J. Dent. 2008, 36, 900–906. [Google Scholar] [CrossRef]
- Ran, S.; Gu, S.; Wang, J.; Zhu, C.; Liang, J. Dentin Tubule Invasion by Enterococcus Faecalis under Stress Conditions Ex Vivo. Eur. J. Oral Sci. 2015, 123, 362–368. [Google Scholar] [CrossRef]
- Zou, L.; Shen, Y.; Li, W.; Haapasalo, M. Penetration of Sodium Hypochlorite into Dentin. J. Endod. 2010, 36, 793–796. [Google Scholar] [CrossRef]
- Zand, V.; Mokhtari, H.; Hasani, A.; Jabbari, G. Comparison of the Penetration Depth of Conventional and Nano-Particle Calcium Hydroxide into Dentinal Tubules. Iran. Endod. J. 2017, 12, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Ghorbanzadeh, A.; Aminsobhani, M.; Sohrabi, K.; Chiniforush, N.; Ghafari, S.; Shamshiri, A.R.; Noroozi, N. Penetration Depth of Sodium Hypochlorite in Dentinal Tubules after Conventional Irrigation, Passive Ultrasonic Agitation and Nd:YAG Laser Activated Irrigation. J. Lasers Med. Sci. 2016, 7, 105–111. [Google Scholar] [CrossRef]
- Kakoli, P.; Nandakumar, R.; Romberg, E.; Arola, D.; Fouad, A.F. The Effect of Age on Bacterial Penetration of Radicular Dentin. J. Endod. 2009, 35, 78–81. [Google Scholar] [CrossRef]
- Rajakumaran, A.; Ganesh, A. Comparative Evaluation of Depth of Penetration of Root Canal Irrigant after Using Manual, Passive Ultrasonic, and Diode Laser–Assisted Irrigant Activation Technique. J. Pharm. Bioallied Sci. 2019, 11, 216. [Google Scholar] [CrossRef] [PubMed]
- Ruozi, B.; Belletti, D.; Tombesi, A.; Tosi, G.; Bondioli, L.; Forni, F.; Vandelli, M.A. AFM, ESEM, TEM, and CLSM in Liposomal Characterization: A Comparative Study. Int. J. Nanomed. 2011, 6, 557–563. [Google Scholar] [CrossRef]
- Alavi, M.; Karimi, N.; Safaei, M. Application of Various Types of Liposomes in Drug Delivery Systems. Adv. Pharm. Bull. 2017, 7, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Gan, Y.; Li, X.; Chen, D.; Le, C.; Zhu, C.; Hovgaard, L.; Yang, M. Novel Mucus-Penetrating Liposomes as a Potential Oral Drug Delivery System: Preparation, in Vitro Characterization, and Enhanced Cellular Uptake. Int. J. Nanomed. 2011, 6, 3151. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Peralta, M.F.; Guzmán, M.L.; Pérez, A.P.; Apezteguia, G.A.; Fórmica, M.L.; Romero, E.L.; Olivera, M.E.; Carrer, D.C. Liposomes Can Both Enhance or Reduce Drugs Penetration through the Skin. Sci. Rep. 2018, 8, 13253. [Google Scholar] [CrossRef]
- Galler, K.M.; Grubmüller, V.; Schlichting, R.; Widbiller, M.; Eidt, A.; Schuller, C.; Wölflick, M.; Hiller, K.-A.; Buchalla, W. Penetration Depth of Irrigants into Root Dentine after Sonic, Ultrasonic and Photoacoustic Activation. Int. Endod. J. 2019, 52, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Cytoxicity of Root Canal Antiseptics Used in Dental Practice on L929 Fibroblasts: Calcium Hydroxide Powder vs. 2% Chlorhexidine Solution. Available online: https://www.researchgate.net/publication/267866304_Cytoxicity_of_root_canal_antiseptics_used_in_dental_practice_on_L929_fibroblasts_calcium_hydroxide_powder_vs_2_chlorhexidine_solution (accessed on 20 January 2022).
- Farhad Mollashahi, N.; Saberi, E.; Karkehabadi, H. Evaluation of Cytotoxic Effects of Various Endodontic Irrigation Solutions on the Survival of Stem Cell of Human Apical Papilla. Iran. Endod. J. 2016, 11, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Padya, B.S.; Pandey, A.; Pisay, M.; Koteshwara, K.B.; Chandrashekhar Hariharapura, R.; Bhat, K.U.; Biswas, S.; Mutalik, S. Stimuli-Responsive and Cellular Targeted Nanoplatforms for Multimodal Therapy of Skin Cancer. Eur. J. Pharmacol. 2021, 890, 173633. [Google Scholar] [CrossRef]
- Gopalan, D.; Pandey, A.; Udupa, N.; Mutalik, S. Receptor Specific, Stimuli Responsive and Subcellular Targeted Approaches for Effective Therapy of Alzheimer: Role of Surface Engineered Nanocarriers. J. Control. Release 2020, 319, 183–200. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Batches | Cholesterol (mg) | HSPC (mg) | Drug (mg) | Encapsulation Efficiency (%) | Size (nm) | Zeta Potential (mV) |
|---|---|---|---|---|---|---|
| 1 | 90 | 10 | 10 | 36 ± 2.42 | 148.2 ± 4.52 | 24.1 ± 2.60 |
| 2 | 90 | 10 | 20 | 48 ± 1.76 | 156.0 ± 5.36 | 29.3 ± 2.42 |
| 3 | 90 | 10 | 30 | 76 ± 2.80 | 178.4 ± 4.41 | 28.1 ± 2.56 |
| 4 | 90 | 10 | 40 | 56 ± 2.67 | 206.4 ± 3.63 | 34.2 ± 2.60 |
| 5 | 90 | 10 | 50 | 52 ± 2.45 | 223.6 ± 3.63 | 37.8 ± 2.12 |
| Groups | Sections | Number of Samples | Depth of Penetration (µm) | 95% Confidence Interval for Mean | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Group I (Plain CHX solution containing Rhodamine B) | Coronal | 7 | 700.67 ± 75.78 | 630.58 | 770.75 |
| Middle | 7 | 623.83 ± 68.48 | 560.49 | 687.16 | |
| Apical | 7 | 331.74 ± 39.40 | 295.30 | 368.18 | |
| Total | 21 | 552.08 ± 173.54 | 473.08 | 631.07 | |
| Group II (Liposomal CHX containing Rhodamine B) | Coronal | 14 | 1549.91 ± 422.56 | 1305.93 | 1793.89 |
| Middle | 14 | 1115.68 ± 410.50 | 878.66 | 1352.70 | |
| Apical | 14 | 758.34 ± 93.46 | 704.38 | 812.30 | |
| Total | 42 | 1141.31 ± 469.18 | 995.10 | 1287.52 | |
| Source | ANOVA F-Value | p-Values | Effect Size |
|---|---|---|---|
| Main effect due to Group | 58.982 | 0.000 | 0.509 |
| Main effect due to Subgroup | 19.156 | 0.000 | 0.402 |
| Interaction effect of Group vs. Subgroup | 2.932 | 0.061 | 0.093 |
| Viable Bacteria/Colony Counts | Organism | Liposomal CHX | 2% CHX |
|---|---|---|---|
| Viable bacterium remaining after exposure to the drug for 12 h (µg/mL) | Staphylococcus aureus | ˃16 | ˃32 |
| Streptococcus mutans | ˃4 | ˃8 | |
| Fusobacterium nucleatum | >4 | >16 | |
| Colony counts of bacterium after 72 h of exposure (‘-‘ = No colonies) | Staphylococcus aureus | - | >2 |
| Streptococcus mutans | - | >2 | |
| Fusobacterium nucleatum | - | - |
| Samples | Test Conc. (μg/mL) | Cell Viability (%) | IC50 (μg/mL) | ||
|---|---|---|---|---|---|
| L929 Cells | 3T3 Cells | L929 Cells | 3T3 Cells | ||
| Plain CHX solution | 250 | 10.41 ± 0.30 | 16.93 ± 0.13 | 12.32 ± 3.65 | 29.07 ± 2.14 |
| 125 | 10.41 ± 0.11 | 18.94± 1.23 | |||
| 62.5 | 10.46 ± 0.23 | 36.22 ± 0.44 | |||
| 31.25 | 12.10 ± 0.39 | 43.04 ± 0.36 | |||
| 15.62 | 47.95 ± 0.49 | 61.47 ± 0.11 | |||
| 7.81 | 72.88 ± 0.30 | 76.31 ± 0.98 | |||
| Liposomal CHX | 250 | 10.05 ± 0.17 | 26.98 ±0.76 | 37.90 ± 1.05 | 85.24 ± 3.22 |
| 125 | 10.18 ± 0.39 | 43.32 ± 1.28 | |||
| 62.5 | 10.26 ± 0.09 | 64.05 ± 0.03 | |||
| 31.25 | 69.04 ± 0.56 | 69.53 ± 0.48 | |||
| 15.62 | 89.59 ± 0.22 | 75.99 ± 1.11 | |||
| 7.81 | 95.34 ± 1.65 | 82.67 ± 0.73 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shirur, K.S.; Padya, B.S.; Pandey, A.; Hegde, M.M.; Narayan, A.I.; Rao, B.S.S.; Bhat, V.G.; Mutalik, S. Development of Lipidic Nanoplatform for Intra-Oral Delivery of Chlorhexidine: Characterization, Biocompatibility, and Assessment of Depth of Penetration in Extracted Human Teeth. Nanomaterials 2022, 12, 3372. https://doi.org/10.3390/nano12193372
Shirur KS, Padya BS, Pandey A, Hegde MM, Narayan AI, Rao BSS, Bhat VG, Mutalik S. Development of Lipidic Nanoplatform for Intra-Oral Delivery of Chlorhexidine: Characterization, Biocompatibility, and Assessment of Depth of Penetration in Extracted Human Teeth. Nanomaterials. 2022; 12(19):3372. https://doi.org/10.3390/nano12193372
Chicago/Turabian StyleShirur, Krishnaraj Somyaji, Bharath Singh Padya, Abhijeet Pandey, Manasa Manjunath Hegde, Aparna I. Narayan, Bola Sadashiva Satish Rao, Varadaraj G. Bhat, and Srinivas Mutalik. 2022. "Development of Lipidic Nanoplatform for Intra-Oral Delivery of Chlorhexidine: Characterization, Biocompatibility, and Assessment of Depth of Penetration in Extracted Human Teeth" Nanomaterials 12, no. 19: 3372. https://doi.org/10.3390/nano12193372
APA StyleShirur, K. S., Padya, B. S., Pandey, A., Hegde, M. M., Narayan, A. I., Rao, B. S. S., Bhat, V. G., & Mutalik, S. (2022). Development of Lipidic Nanoplatform for Intra-Oral Delivery of Chlorhexidine: Characterization, Biocompatibility, and Assessment of Depth of Penetration in Extracted Human Teeth. Nanomaterials, 12(19), 3372. https://doi.org/10.3390/nano12193372