

Fracture Resistance of 3D-Printed Partial and Conventional Veneers

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
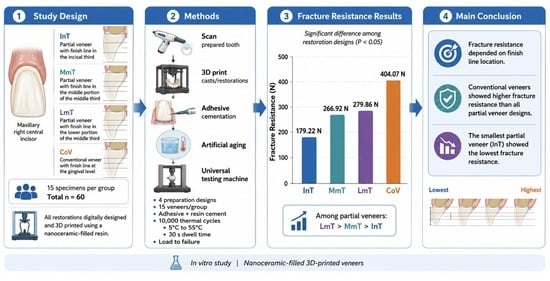
- The fracture resistance of 3D-printed nanoceramic-filled resin veneers was influenced by the extent of surface coverage.
- Partial-coverage veneers with margins located closer to the gingival level demonstrated higher fracture resistance than those with more incisal margins.
- Conventional veneers with margins at the gingival level demonstrated higher fracture resistance than partial veneers.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, Y.W.; Raigrodski, A.J. A conservative approach for treating young adult patients with porcelain laminate veneers. J. Esthet. Restor. Dent. 2008, 20, 223–236; discussion 237-8. [Google Scholar] [CrossRef] [PubMed]
- Blatz, M.B. Adhesive Dentistry: Just Bond It! Compend. Contin. Educ. Dent. 2021, 42, 536–537. [Google Scholar] [PubMed]
- Gürel, G. Porcelain laminate veneers: Minimal tooth preparation by design. Dent. Clin. N. Am. 2007, 51, 419–431, ix. [Google Scholar] [CrossRef] [PubMed]
- Caetano, G.M.; Slomp, C.; Andrade, J.P.; Spohr, A.M.; Kunrath, M.F. Partial Ceramic Veneer Technique for Challenging Esthetic Frontal Restorative Procedures. Dent. J. 2023, 11, 101. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Christensen, G.J. The advantages of minimally invasive dentistry. J. Am. Dent. Assoc. 2005, 136, 1563–1565. [Google Scholar] [CrossRef] [PubMed]
- Araujo, E.; Perdigão, J. Anterior Veneer Restorations—An Evidence-based Minimal-Intervention Perspective. J. Adhes. Dent. 2021, 23, 91–110. [Google Scholar] [CrossRef] [PubMed]
- Reis, J.M.D.S.N.; Pansani, T.N.; Del’Acqua, M.A.; Abi-Rached, F.O. Minimally Invasive Ceramic Laminate Veneers for Maxillary Anterior Esthetic Rehabilitation: A 12+ Years Follow-Up. J. Esthet. Restor. Dent. 2025, 37, 2171–2179. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, S.; Demirkol, N.; Eyüboğlu, T.F.; Özcan, M. Clinical Performance Comparison of Prepless and Minimally Invasive Ceramic Laminate Veneer Restorations: A Prospective Clinical Study. J. Esthet. Restor. Dent. 2026, 38, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Edelhoff, D.; Sorensen, J.A. Tooth structure removal associated with various preparation designs for anterior teeth. J. Prosthet. Dent. 2002, 87, 503–509. [Google Scholar] [CrossRef]
- Nejatidanesh, F.; Savabi, G.; Amjadi, M.; Abbasi, M.; Savabi, O. Five year clinical outcomes and survival of chairside CAD/CAM ceramic laminate veneers—A retrospective study. J. Prosthodont. Res. 2018, 62, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Lobo, M.M.; Scopin de Andrade, O.; Malta Barbosa, J.; Sampaio, C.S.; de Castro Folgueras, D.; Hirata, R. Minimally invasive ceramic laminate veneers. A 5-year CT evaluation of periodontal health. Int. J. Esthet. Dent. 2024, 19, 312–322. [Google Scholar] [PubMed]
- Durán Ojeda, G.; Henríquez Gutiérrez, I.; Guzmán Marusic, Á.; Báez Rosales, A.; Tisi Lanchares, J.P. A Step-by-Step Conservative Approach for CAD-CAM Laminate Veneers. Case Rep. Dent. 2017, 2017, 3801419. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, G.; Li, J.; Li, J.; Zhou, X.; Xie, J.; Wang, A. Selective Laser Melting Molding of Individualized Femur Implant: Design, Process, Optimization. J. Bionic Eng. 2021, 18, 128–137. [Google Scholar] [CrossRef]
- Duarte, S., Jr.; Phark, J.H. Advances in Dental Restorations: A Comprehensive Review of Machinable and 3D-Printed Ceramic-Reinforced Composites. J. Esthet. Restor. Dent. 2025, 37, 257–276. [Google Scholar] [CrossRef]
- Sailer, I.; Benic, G.I.; Fehmer, V.; Hämmerle, C.H.F.; Mühlemann, S. Randomized controlled within-subject evaluation of digital and conventional workflows for the fabrication of lithium disilicate single crowns. Part II: CAD-CAM versus conventional laboratory procedures. J. Prosthet. Dent. 2017, 118, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Luna-Domínguez, C.R.; Luna-Domínguez, J.H.; Blatz, M. Full-mouth rehabilitation in a completely digital workflow using partially adhesive monolithic zirconia restorations. J. Esthet. Restor. Dent. 2023, 35, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Akgungor, G.; Sen, D.; Bal, E.; Ozcan, M. Simultaneous Replacement of Maxillary Central Incisors with CEREC Biogeneric Reference Technique: A Case Report. J. Dent. Res. Dent. Clin. Dent. Prospect. 2013, 7, 112–118. [Google Scholar] [CrossRef]
- McCracken, M.S.; Louis, D.R.; Litaker, M.S.; Minyé, H.M.; Mungia, R.; Gordan, V.V.; Marshall, D.G.; Gilbert, G.H. Treatment recommendations for single-unit crowns: Findings from The National Dental Practice-Based Research Network. J. Am. Dent. Assoc. 2016, 147, 882–890. [Google Scholar] [CrossRef]
- Jurado, C.A.; Villalobos-Tinoco, J.; Watanabe, H.; Sanchez-Hernandez, R.; Tsujimoto, A. Novel translucent monolithic zirconia fixed restorations in the esthetic zone. Clin. Case Rep. 2022, 10, e05499. [Google Scholar] [CrossRef]
- Jeong, M.; Radomski, K.; Lopez, D.; Liu, J.T.; Lee, J.D.; Lee, S.J. Materials and Applications of 3D Printing Technology in Dentistry: An Overview. Dent. J. 2023, 12, 1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Balhaddad, A.A.; Garcia, I.M.; Mokeem, L.; Alsahafi, R.; Majeed-Saidan, A.; Albagami, H.H.; Khan, A.S.; Ahmad, S.; Collares, F.M.; Della Bona, A.; et al. Three-dimensional (3D) printing in dental practice: Applications, areas of interest, and level of evidence. Clin. Oral Investig. 2023, 27, 2465–2481. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Li, J.; Wang, H.; Shangguan, C.; Xie, J.; Zhou, Y. Research on the Impact Toughness of 3D-Printed CoCrMo Alloy Components Based on Fractal Theory. Biomimetics 2025, 10, 292. [Google Scholar] [CrossRef]
- Unkovskiy, A.; Huettig, F.; Kraemer-Fernandez, P.; Spintzyk, S. Multi-Material 3D Printing of a Customized Sports Mouth Guard: Proof-of-Concept Clinical Case. Int. J. Env. Res. Public Health 2021, 18, 12762. [Google Scholar] [CrossRef]
- Abad-Coronel, C.; Ruano Espinosa, C.; Ordóñez Palacios, S.; Paltán, C.A.; Fajardo, J.I. Comparative Analysis between Conventional Acrylic, CAD/CAM Milled, and 3D CAD/CAM Printed Occlusal Splints. Materials 2023, 16, 6269. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, L.E.B.; da Silva Rodrigues, C.; Grangeiro, M.T.V.; Campos, T.M.B.; de Melo, R.M. Characterization of 3D printed composite for final dental restorations. Clin. Oral Investig. 2024, 28, 617. [Google Scholar] [CrossRef] [PubMed]
- Flottes, Y.; Smail, Y.; Palomino-Durand, C.; Attal, J.P.; Ceinos, R.; François, P.; Dursun, E. Properties of 3D printed resins for definitive dental restorations: A systematic review. J. Prosthet. Dent. 2026, 135, e6–e27. [Google Scholar] [CrossRef] [PubMed]
- Ojeda, G.D.; Naves, L.Z.; Oosterhaven, A.; Kleinsman, R.; Bäumer-König, A.; Körner, G.; Wendler, M.; Gresnigt, M. 8-year multicenter retrospective study on partial laminate veneers. J. Prosthodont. Res. 2023, 67, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Villalobos-Tinoco, J.; Jurado, C.A.; Antal, M.A.; Rojas-Rueda, S.; Nurrohman, H. Partial Ceramic Veneers as a Conservative Restorative Strategy: A Narrative Review with Case Report. Dent. J. 2026, 14, 186. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ceinos, R.; Pouyssegur, V.; Allard, Y.; Bertrand, M.F. Esthetic rehabilitation of the smile with partial laminate veneers in an older adult. Clin. Case Rep. 2018, 6, 1407–1411. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fonseca, M.; Molinero-Mourelle, P.; Dönmez, M.B.; Abou-Ayash, S.; Buser, D.; Sculean, A.; Yilmaz, B. Management of Compromised Spacing in the Esthetic Zone by Combining an Ultra-Thin Partial Ceramic Veneer and a Ceramic Implant Crown: A Case Report of a Multidisciplinary Approach and Technique Description. Int. J. Periodontics Restor. Dent. 2024, 44, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Lopez, D.; Ziada, H.; Abubakr, N.H. Influence of thermal aging on the marginal integrity of computer aided design/computer aided manufacturing fabricated crowns. J. Dent. Sci. 2024, 19, 971–977. [Google Scholar] [CrossRef]
- Yılmaz, D.; Çakmak, G.; Güven, M.E.; Pieralli, S.; Yoon, H.I.; Revilla-León, M.; Yilmaz, B. Effect of Hydrothermal Aging on the Flexural Strength and Microhardness of Materials Used for Additive or Subtractive Manufacturing of Definitive Restorations. Int. J. Prosthodont. 2024, 37, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Abuhammoud, S.; Jurado, C.A.; Rojas-Rueda, S.; Garcia-Contreras, R.; Vegh, D.; Lee, D.J. Impact of endodontic access design on the fracture resistance of zirconia mandibular molar crowns. J. Prosthodont. 2026, 35, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Honda, J.; Takano, R.; Saito, T.; Kobayashi, T.; Kubochi, K.; Blatz, M.B.; Komine, F. Fracture resistance of premolar screw-retained implant-supported hybrid abutment crowns with monolithic restorations after thermomechanical aging. J. Adv. Prosthodont. 2026, 18, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Alhotan, A.; Jurado, C.A.; Alamoush, R.A.; Abuhammoud, S.; Robles, M.; Lackey, M.A.; Alhijji, S.; Dönmez, M.B. Fracture resistance of highly translucent zirconia laminate veneers with different finish line locations. Sci. Rep. 2025, 15, 41887. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jurado, C.A.; Mekled, S.; Abuhammoud, S.; Azpiazu-Flores, F.X.; Vegh, D.; Wang, T.; Morton, D. Fracture resistance of partial and complete coverage veneers and ceramic crowns for maxillary central incisors. J. Prosthet. Dent. 2024, 132, 420.e1–420.e6. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, S.S.; Quinn, J.B.; Quinn, G.D.; Wiskott, H.W.A. Fractographic Ceramic Failure Analysis Using the Replica Technique. Dent. Mater. 2007, 23, 1397–1404. [Google Scholar] [CrossRef]
- Cesar, P.F.; Della Bona, A.; Scherrer, S.S.; Tholey, M.; van Noort, R.; Vichi, A.; Kelly, R.; Lohbauer, U. ADM Guidance-Ceramics: Fracture Toughness Testing and Method Selection. Dent. Mater. 2017, 33, 575–584. [Google Scholar] [CrossRef] [PubMed]
- Abid, S.; Mohammed, K. The Effect of Preparation Design on Stress Distribution in Lithium Disilicate Laminate Veneer Using 3D Finite Element Analysis. Open Dent. J. 2023, 17, e18742106243827. [Google Scholar] [CrossRef]
- Giannini, M.; Soares, C.J.; de Carvalho, R.M. Ultimate tensile strength of tooth structures. Dent. Mater. 2004, 20, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Staninec, M.; Marshall, G.W.; Hilton, J.F.; Pashley, D.H.; Gansky, S.A.; Marshall, S.J.; Kinney, J.H. Ultimate tensile strength of dentin: Evidence for a damage mechanics approach to dentin failure. J. BioMed Mater. Res. 2002, 63, 342–345. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, A.A.; Morrow, B.; Mireles, S.; Jurado, C.A.; Antal, M.A.; Rojas-Rueda, S.; Nurrohman, H.; Garcia-Godoy, F. Fracture Resistance of CAD/CAM Resin-Matrix Ceramic Overlays and Full-Coverage Crowns for Maxillary Premolars. Biomimetics 2026, 11, 291. [Google Scholar] [CrossRef]
- Chen, P.H.; Elamin, E.; Sayed Ahmed, A.; Givan, D.A.; Fu, C.C.; Lawson, N.C. The Effect of Restoration Thickness on the Fracture Resistance of 5 mol% Yttria-Containing Zirconia Crowns. Materials 2024, 17, 365. [Google Scholar] [CrossRef]
- Sayed Ahmed, A.; Lawson, N.C.; Fu, C.C.; Bora, P.V.; Kee, E.; Nejat, A.H. The effect of die material on the crown fracture strength of zirconia crowns. Materials 2024, 17, 1096. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Restoration | Number of Samples | Load for Fracture (SD), Newtons |
|---|---|---|
| Partial veneer with margin in the incisal third (InT) | 15 | 179.22 (±11.67) a |
| Partial veneer with margin in the middle portion of the middle third (MmT) | 15 | 266.92 (±13.32) b |
| Partial veneer with margin in the lower portion of the middle third (LmT) | 15 | 279.86 (±9.71) c |
| Conventional veneer with margin at the gingival level (CoV) | 15 | 404.07 (±11.53) d |
| Group 1 (InT) | Group 2 (MmT) | Group 3 (LmT) | Group 4 (CoV) | |
|---|---|---|---|---|
| Mean | 179.22 | 266.92 | 279.86 | 404.07 |
| Standard error (SE) | 3.01 | 3.44 | 2.50 | 2.97 |
| Shapiro–Wilk (p value) | 0.584 | 0.219 | 0.862 | 0.093 |
| Range | 161.13–201.21 | 247.92–288.41 | 261.65–294.48 | 388.04–420.89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Share and Cite
Alshabib, A.; Rojas-Rueda, S.; Alotaibi, S.; Jurado, C.A.; Antal, M.A.; Morrow, B.R.; Garcia-Godoy, F. Fracture Resistance of 3D-Printed Partial and Conventional Veneers. J. Funct. Biomater. 2026, 17, 298. https://doi.org/10.3390/jfb17060298
Alshabib A, Rojas-Rueda S, Alotaibi S, Jurado CA, Antal MA, Morrow BR, Garcia-Godoy F. Fracture Resistance of 3D-Printed Partial and Conventional Veneers. Journal of Functional Biomaterials. 2026; 17(6):298. https://doi.org/10.3390/jfb17060298
Chicago/Turabian StyleAlshabib, Abdulrahman, Silvia Rojas-Rueda, Saad Alotaibi, Carlos A. Jurado, Mark A. Antal, Brian R. Morrow, and Franklin Garcia-Godoy. 2026. "Fracture Resistance of 3D-Printed Partial and Conventional Veneers" Journal of Functional Biomaterials 17, no. 6: 298. https://doi.org/10.3390/jfb17060298
APA StyleAlshabib, A., Rojas-Rueda, S., Alotaibi, S., Jurado, C. A., Antal, M. A., Morrow, B. R., & Garcia-Godoy, F. (2026). Fracture Resistance of 3D-Printed Partial and Conventional Veneers. Journal of Functional Biomaterials, 17(6), 298. https://doi.org/10.3390/jfb17060298