
Evaluation of Two Alloplastic Biomaterials in a Critical-Size Rat Calvarial Defect Model
 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Biomaterials
2.3. Study Design and Sample
2.4. Surgical Procedures
2.5. Postsurgery Procedures
2.6. Radiographic Evaluation
2.6.1. Mineralized Tissue Volume/Total Volume and Biomaterial Volume/Total Volume
2.6.2. Biomaterial Displacement
2.7. Histological Preparation
2.8. Histomorphometric Analysis
- Defect width: distance between the defect margins;
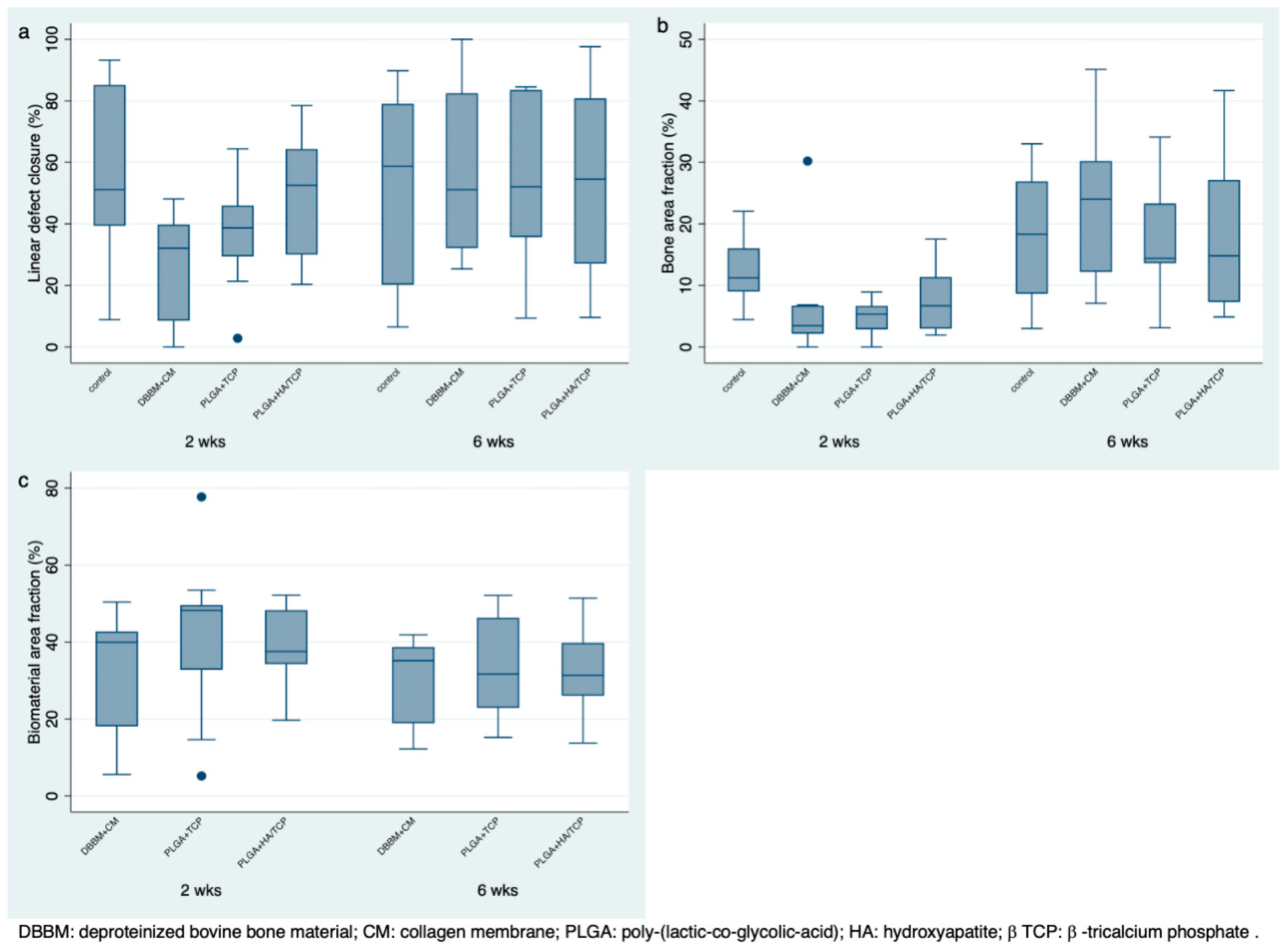
- Defect closure: fraction (%) of accumulated length of new bone formation between the defect margins;
- Defect area: area of regeneration including new bone formation, residual biomaterial and other tissue limited by the defect margins;
- Defect fill: total area of newly formed bone between the defect margins;
- Bone area fraction: fraction (%) of newly formed bone within the defect area;
- Residual biomaterial: total area of residual biomaterial between the defect margins;
- Biomaterial area fraction: fraction (%) of residual biomaterial within the defect area.
2.9. Statistical Analysis
3. Results
3.1. Surgical Outcomes
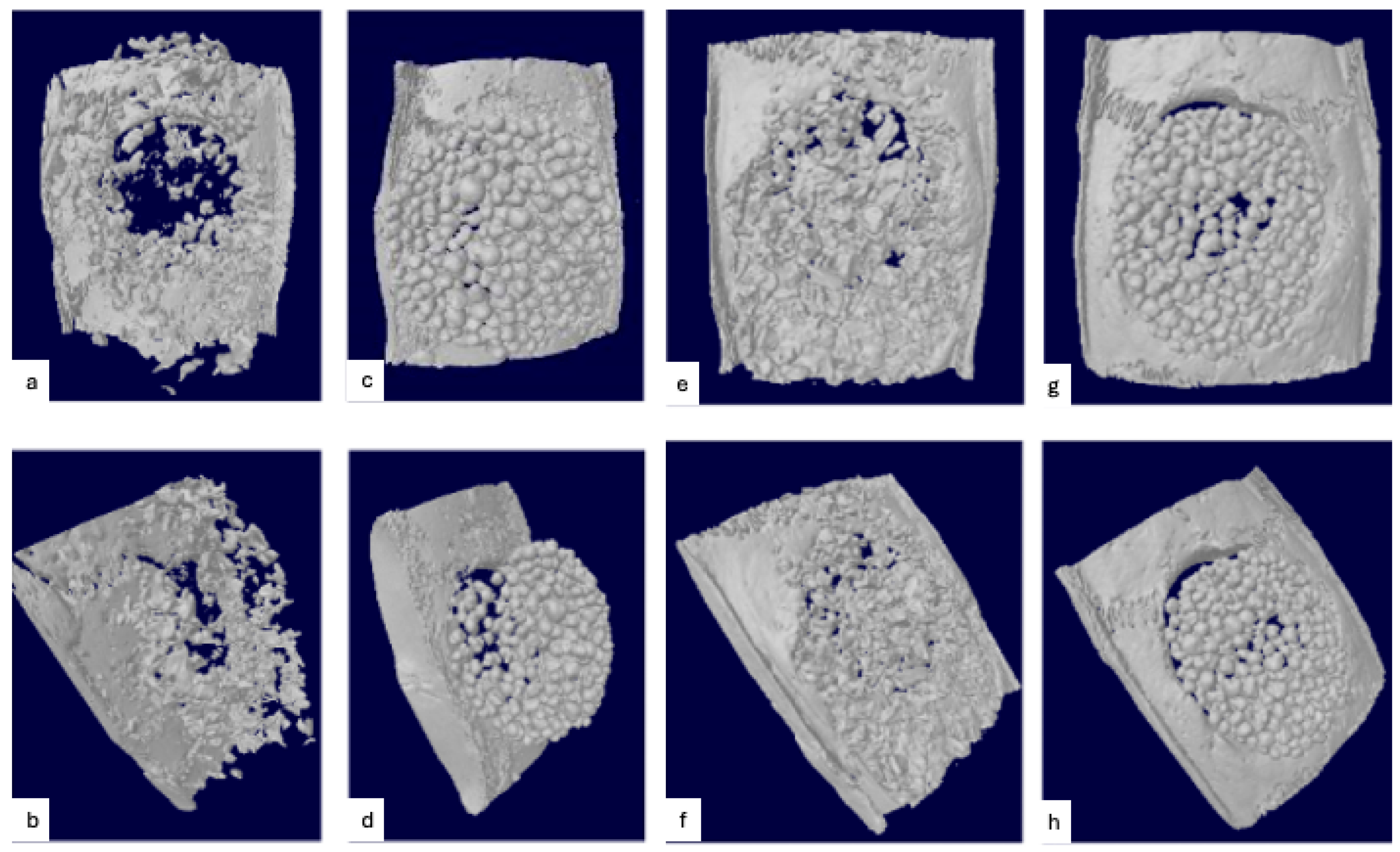
3.2. Radiographic Evaluation
Biomaterial Displacement
3.3. Histopathologic Observations
3.3.1. Sham Surgery
3.3.2. DBBM + CM
3.3.3. PLGA + β-TCP and PLGA + HA/β-TCP
3.4. Histomorphometric Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CM | collagen membrane |
| PLGA | poly-(lactic-co-glycolic-acid) |
| DBBM | deproteinized bovine bone mineral |
| HA | hydroxyapatite |
| β-TCP | β-tricalcium phosphate |
| μCT | microcomputed tomography |
| MTV | mineralized tissue volume |
| BIO | biomaterial volume |
| ICC | intraclass correlation |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomaterial | Composition | Particle Size (mm) | Source |
|---|---|---|---|
| Sham surgery | - | - | - |
| Bio-Oss | Bovine hydroxyapatite | 0.25–1.00 | Geistlich, Wolhusen, Switzerland |
| Easy-Graft Classic | Pure beta-tricalcium phosphate with poly(lactide-co-glycolide) + BioLinker (N-Methyl-2-pyrrolidone-solution) | 0.5–1.00 | Degradable Solutions AG, Schlieren, Switzerland |
| Easy-Graft Crystal | Biphasic calcium phosphate (60% hydroxyapatite, 40% beta-tricalcium phosphate) with poly(lactide-co-glycolide) + BioLinker (N-Methyl-2-pyrrolidone-solution) | 0.45–1.00 | Degradable Solutions AG, Schlieren, Switzerland |
Appendix B
References
- Araujo, M.G.; Lindhe, J. Dimensional Ridge Alterations Following Tooth Extraction. An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef] [PubMed]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone Grafts: Which Is the Ideal Biomaterial? J. Clin. Periodontol. 2019, 46, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, P.; Li, D.J.; Auston, D.A.; Mir, H.S.; Yoon, R.S.; Koval, K.J. Autograft, Allograft, and Bone Graft Substitutes: Clinical Evidence and Indications for Use in the Setting of Orthopaedic Trauma Surgery. J. Orthop. Trauma 2019, 33, 203–213. [Google Scholar] [CrossRef]
- Avila-Ortiz, G.; Elangovan, S.; Karimbux, N. Bone Graft Substitutes for Periodontal Use Available in the United States. Clin. Adv. Periodontol. 2013, 3, 187–190. [Google Scholar] [CrossRef]
- Spicer, P.P.; Kretlow, J.D.; Young, S.; Jansen, J.A.; Kasper, F.K.; Mikos, A.G. Evaluation of Bone Regeneration Using the Rat Critical Size Calvarial Defect. Nat. Protoc. 2012, 7, 1918–1929. [Google Scholar] [CrossRef]
- Herberg, S.; Susin, C.; Pelaez, M.; Howie, R.N.; Moreno de Freitas, R.; Lee, J.; Cray, J.J.; Johnson, M.H.; Elsalanty, M.E.; Hamrick, M.W.; et al. Low-Dose Bone Morphogenetic Protein-2/Stromal Cell-Derived Factor-1β Cotherapy Induces Bone Regeneration in Critical-Size Rat Calvarial Defects. Tissue Eng. Part A 2014, 20, 1444–1453. [Google Scholar] [CrossRef]
- Hyun, S.-J.; Han, D.-K.; Choi, S.-H.; Chai, J.-K.; Cho, K.-S.; Kim, C.-K.; Kim, C.-S. Effect of Recombinant Human Bone Morphogenetic Protein-2, -4, and -7 on Bone Formation in Rat Calvarial Defects. J. Periodontol. 2005, 76, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Poehling, S.; Pippig, S.D.; Hellerbrand, K.; Siedler, M.; Schütz, A.; Dony, C. Superior Effect of MD05, Beta-Tricalcium Phosphate Coated with Recombinant Human Growth/Differentiation Factor-5, Compared to Conventional Bone Substitutes in the Rat Calvarial Defect Model. J. Periodontol. 2006, 77, 1582–1590. [Google Scholar] [CrossRef]
- Susin, C.; Lee, J.; Fiorini, T.; Koo, K.-T.; Schüpbach, P.; Angst, P.D.M.; Finger Stadler, A.; Wikesjö, U.M. Screening of Candidate Biomaterials for Alveolar Augmentation Using a Critical-Size Rat Calvaria Defect Model. J. Clin. Periodontol. 2018, 45, 884–893. [Google Scholar] [CrossRef]
- Bizenjima, T.; Takeuchi, T.; Seshima, F.; Saito, A. Effect of Poly (Lactide-Co-Glycolide) (PLGA)-Coated Beta-Tricalcium Phosphate on the Healing of Rat Calvarial Bone Defects: A Comparative Study with Pure-Phase Beta-Tricalcium Phosphate. Clin. Oral Impl. Res. 2016, 27, 1360–1367. [Google Scholar] [CrossRef]
- Schmidlin, P.R.; Nicholls, F.; Kruse, A.; Zwahlen, R.A.; Weber, F.E. Evaluation of Moldable, in Situ Hardening Calcium Phosphate Bone Graft Substitutes. Clin. Oral Impl. Res. 2013, 24, 149–157. [Google Scholar] [CrossRef]
- Valdivia-Gandur, I.; Engelke, W.; Beltrán, V.; Borie, E.; Fuentes, R.; Manzanares-Céspedes, M.C. Novel Use of Cranial Epidural Space in Rabbits as an Animal Model to Investigate Bone Volume Augmentation Potential of Different Bone Graft Substitutes. Head. Face Med. 2016, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- Kakar, A.; Kakar, K.; Sripathi Rao, B.H.; Lindner, A.; Nagursky, H.; Jain, G.; Patney, A. Lateral Alveolar Ridge Augmentation Procedure Using Subperiosteal Tunneling Technique: A Pilot Study. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 3. [Google Scholar] [CrossRef]
- Leventis, M.D.; Fairbairn, P.; Kakar, A.; Leventis, A.D.; Margaritis, V.; Lückerath, W.; Horowitz, R.A.; Rao, B.H.; Lindner, A.; Nagursky, H. Minimally Invasive Alveolar Ridge Preservation Utilizing an In Situ Hardening β-Tricalcium Phosphate Bone Substitute: A Multicenter Case Series. Int. J. Dent. 2016, 2016, 5406736. [Google Scholar] [CrossRef] [PubMed]
- Kilkenny, C.; Browne, W.J.; Cuthill, I.C.; Emerson, M.; Altman, D.G. Improving Bioscience Research Reporting: The ARRIVE Guidelines for Reporting Animal Research. Vet. Clin. Pathol. 2012, 41, 27–31. [Google Scholar] [CrossRef]
- Pelaez, M.; Susin, C.; Lee, J.; Fiorini, T.; Bisch, F.C.; Dixon, D.R.; McPherson, J.C.; Buxton, A.N.; Wikesjö, U.M.E. Effect of rhBMP-2 Dose on Bone Formation/Maturation in a Rat Critical-Size Calvarial Defect Model. J. Clin. Periodontol. 2014, 41, 827–836. [Google Scholar] [CrossRef]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Müller, R. Guidelines for Assessment of Bone Microstructure in Rodents Using Micro-Computed Tomography. J. Bone Min. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, Z.; Hamdan, N.; Ikeda, Y.; Grynpas, M.; Ganss, B.; Glogauer, M. Natural Graft Tissues and Synthetic Biomaterials for Periodontal and Alveolar Bone Reconstructive Applications: A Review. Biomater. Res. 2017, 21, 9. [Google Scholar] [CrossRef]
- Tamimi, F.; Sheikh, Z.; Barralet, J. Dicalcium Phosphate Cements: Brushite and Monetite. Acta Biomater. 2012, 8, 474–487. [Google Scholar] [CrossRef]
- Wang, H.; Li, Y.; Zuo, Y.; Li, J.; Ma, S.; Cheng, L. Biocompatibility and Osteogenesis of Biomimetic Nano-Hydroxyapatite/Polyamide Composite Scaffolds for Bone Tissue Engineering. Biomaterials 2007, 28, 3338–3348. [Google Scholar] [CrossRef]
- Bagambisa, F.B.; Joos, U.; Schilli, W. Mechanisms and Structure of the Bond between Bone and Hydroxyapatite Ceramics. J. Biomed. Mater. Res. 1993, 27, 1047–1055. [Google Scholar] [CrossRef] [PubMed]
- Wildburger, A.; Bubalo, V.; Magyar, M.; Nagursky, H.; Jakse, N.; Schmelzeisen, R.; Sauerbier, S. Sinus Floor Augmentation Comparing an In Situ Hardening Biphasic Calcium Phosphate (Hydroxyapatite/β-Tricalcium Phosphate) Bone Graft Substitute with a Particulate Biphasic Calcium Phosphate (Hydroxyapatite/β-Tricalcium Phosphate) Bone Graft Substitute: An Experimental Study in Sheep. Tissue Eng. Part C Methods 2017, 23, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Salem, D.; Natto, Z.; Elangovan, S.; Karimbux, N. Usage of Bone Replacement Grafts in Periodontics and Oral Implantology and Their Current Levels of Clinical Evidence—A Systematic Assessment. J. Periodontol. 2016, 87, 872–879. [Google Scholar] [CrossRef] [PubMed]
- Caballe-Serrano, J.; Munar-Frau, A.; Ortiz-Puigpelat, O.; Soto-Penaloza, D.; Penarrocha, M.; Hernandez-Alfaro, F. On the Search of the Ideal Barrier Membrane for Guided Bone Regeneration. J. Clin. Exp. Dent. 2018, 10, e477–e483. [Google Scholar] [CrossRef]
- Susin, C.; Fiorini, T.; Lee, J.; De Stefano, J.A.; Dickinson, D.P.; Wikesjö, U.M.E. Wound Healing Following Surgical and Regenerative Periodontal Therapy. Periodontol 2000 2015, 68, 83–98. [Google Scholar] [CrossRef]
- Schmitz, J.P.; Hollinger, J.O. The Critical Size Defect as an Experimental Model for Craniomandibulofacial Nonunions. Clin. Orthop. Relat. Res. 1986, 205, 299–308. [Google Scholar] [CrossRef]
- Yip, I.; Ma, L.; Mattheos, N.; Dard, M.; Lang, N.P. Defect Healing with Various Bone Substitutes. Clin. Oral Impl. Res. 2015, 26, 606–614. [Google Scholar] [CrossRef]
- Naenni, N.; Sapata, V.; Bienz, S.P.; Leventis, M.; Jung, R.E.; Hämmerle, C.H.F.; Thoma, D.S. Effect of Flapless Ridge Preservation with Two Different Alloplastic Materials in Sockets with Buccal Dehiscence Defects—Volumetric and Linear Changes. Clin. Oral Investig. 2018, 22, 2187–2197. [Google Scholar] [CrossRef]
- Saito, H.; Couso-Queiruga, E.; Shiau, H.J.; Stuhr, S.; Prasad, H.; Allareddy, T.V.; Reynolds, M.A.; Avila-Ortiz, G. Evaluation of Poly Lactic-co-glycolic Acid-coated Β-tricalcium Phosphate for Alveolar Ridge Preservation: A Multicenter Randomized Controlled Trial. J. Periodontol. 2021, 92, 524–535. [Google Scholar] [CrossRef]



| Healing | Mean | Percentiles | Range | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Period | Group | n | Mean | SD | Median | 25 | 75 | Min | Max |
| 2 weeks | Sham | 10 | 56.08 A | 27.17 | 51.14 | 39.39 | 85.15 | 8.87 | 93.23 |
| DBBM + CM | 10 | 26.30 B | 16.73 | 32.09 | 8.53 | 39.80 | 0 | 48.1 | |
| PLGA + β-TCP | 9 | 37.48 AB | 18.54 | 38.70 | 29.43 | 45.98 | 2.84 | 64.39 | |
| PLGA + HA/β-TCP | 10 | 49.56 AB | 19.45 | 52.56 | 30.04 | 64.31 | 20.33 | 78.47 | |
| 6 weeks | Sham | 10 | 53.39 A | 30.94 | 58.67 | 20.20 | 79.07 | 6.52 | 89.79 |
| DBBM + CM | 10 | 57.50 A | 28.57 | 51.11 | 32.10 | 82.47 | 25.38 | 100 | |
| PLGA + β-TCP | 10 | 52.77 A | 26.91 | 52.04 | 35.70 | 83.54 | 9.42 | 84.52 | |
| PLGA + HA/β-TCP | 10 | 54.34 A | 32.02 | 54.51 | 27.05 | 80.82 | 9.61 | 97.61 | |
| Healing | Mean | Percentiles | Range | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Period | Group | n | Mean | SD | Median | 25 | 75 | Min | Max |
| 2 weeks | Sham | 10 | 12.17 A | 5.08 | 11.23 | 8.99 | 16.03 | 4.45 | 22.04 |
| DBBM + CM | 10 | 6.32 B | 8.72 | 3.46 | 2.16 | 6.74 | 0 | 30.21 | |
| PLGA + β-TCP | 9 | 4.71 B | 2.96 | 5.36 | 2.88 | 6.69 | 0 | 8.91 | |
| PLGA + HA/β-TCP | 10 | 7.64 AB | 5.60 | 6.69 | 2.97 | 11.37 | 1.93 | 17.51 | |
| 6 weeks | Sham | 10 | 17.84 A | 10.30 | 18.31 | 8.64 | 26.90 | 3.01 | 33.01 |
| DBBM + CM | 10 | 24.29 A | 12.94 | 24.01 | 12.18 | 30.21 | 7.08 | 45.11 | |
| PLGA + β-TCP | 10 | 17.84 A | 9.39 | 14.38 | 13.59 | 23.32 | 3.1 | 34.12 | |
| PLGA + HA/β-TCP | 10 | 18.11 A | 12.78 | 14.80 | 7.30 | 27.15 | 4.88 | 41.66 | |
| Healing | Mean | Percentiles | Range | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Period | Group | n | Mean | SD | Median | 25 | 75 | Min | Max |
| 2 weeks | Sham | 10 | - | - | - | - | - | - | - |
| DBBM + CM | 10 | 32.96 A | 14.45 | 39.96 | 18.08 | 42.71 | 5.56 | 50.41 | |
| PLGA + β-TCP | 9 | 40.82 A | 21.63 | 48.24 | 32.82 | 49.64 | 5.17 | 77.69 | |
| PLGA + HA/β-TCP | 10 | 38.47 A | 11.19 | 37.51 | 34.23 | 48.28 | 19.65 | 52.16 | |
| 6 weeks | Sham | 10 | - | - | - | - | - | - | - |
| DBBM + CM | 10 | 31.04 A | 10.88 | 35.15 | 18.89 | 38.67 | 12.18 | 41.86 | |
| PLGA + β-TCP | 10 | 34.05 A | 13.15 | 31.71 | 22.88 | 46.32 | 15.20 | 52.10 | |
| PLGA + HA/β-TCP | 10 | 32.71 A | 10.97 | 31.33 | 26.05 | 39.75 | 13.75 | 51.42 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Finger Stadler, A.; Musskopf, M.L.; Gohel, V.; Reside, J.; Everett, E.; Miguez, P.; Susin, C. Evaluation of Two Alloplastic Biomaterials in a Critical-Size Rat Calvarial Defect Model. J. Funct. Biomater. 2025, 16, 214. https://doi.org/10.3390/jfb16060214
Finger Stadler A, Musskopf ML, Gohel V, Reside J, Everett E, Miguez P, Susin C. Evaluation of Two Alloplastic Biomaterials in a Critical-Size Rat Calvarial Defect Model. Journal of Functional Biomaterials. 2025; 16(6):214. https://doi.org/10.3390/jfb16060214
Chicago/Turabian StyleFinger Stadler, Amanda, Marta Liliana Musskopf, Vishal Gohel, Jonathan Reside, Eric Everett, Patricia Miguez, and Cristiano Susin. 2025. "Evaluation of Two Alloplastic Biomaterials in a Critical-Size Rat Calvarial Defect Model" Journal of Functional Biomaterials 16, no. 6: 214. https://doi.org/10.3390/jfb16060214
APA StyleFinger Stadler, A., Musskopf, M. L., Gohel, V., Reside, J., Everett, E., Miguez, P., & Susin, C. (2025). Evaluation of Two Alloplastic Biomaterials in a Critical-Size Rat Calvarial Defect Model. Journal of Functional Biomaterials, 16(6), 214. https://doi.org/10.3390/jfb16060214