
First Clinical Evidence About the Use of a New Silver-Coated Titanium Alloy Instrumentation to Counteract Surgical Site Infection at the Spine Level


 , , ,
, , ,  and
and 
Abstract
1. Introduction
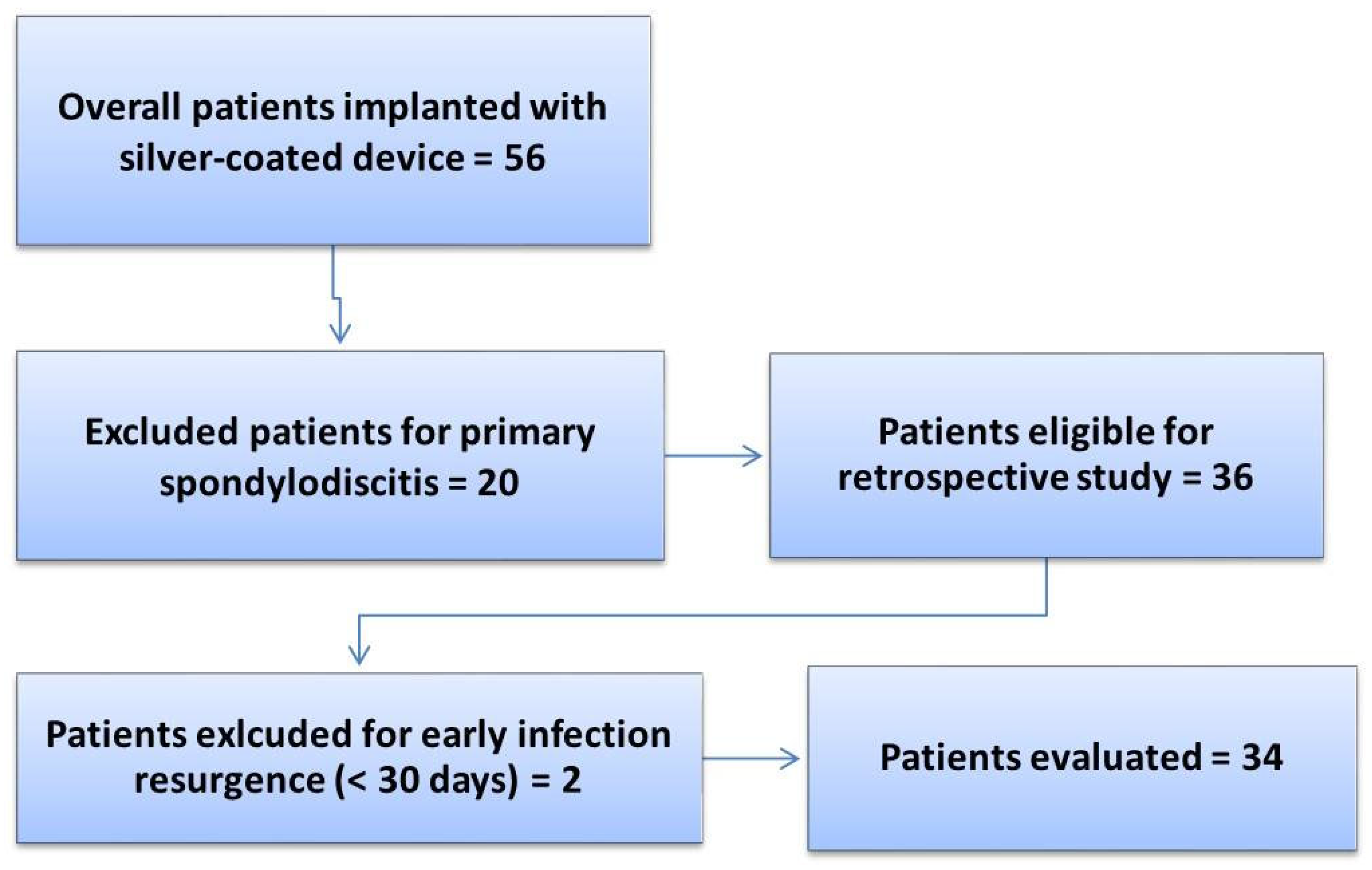
2. Materials and Methods
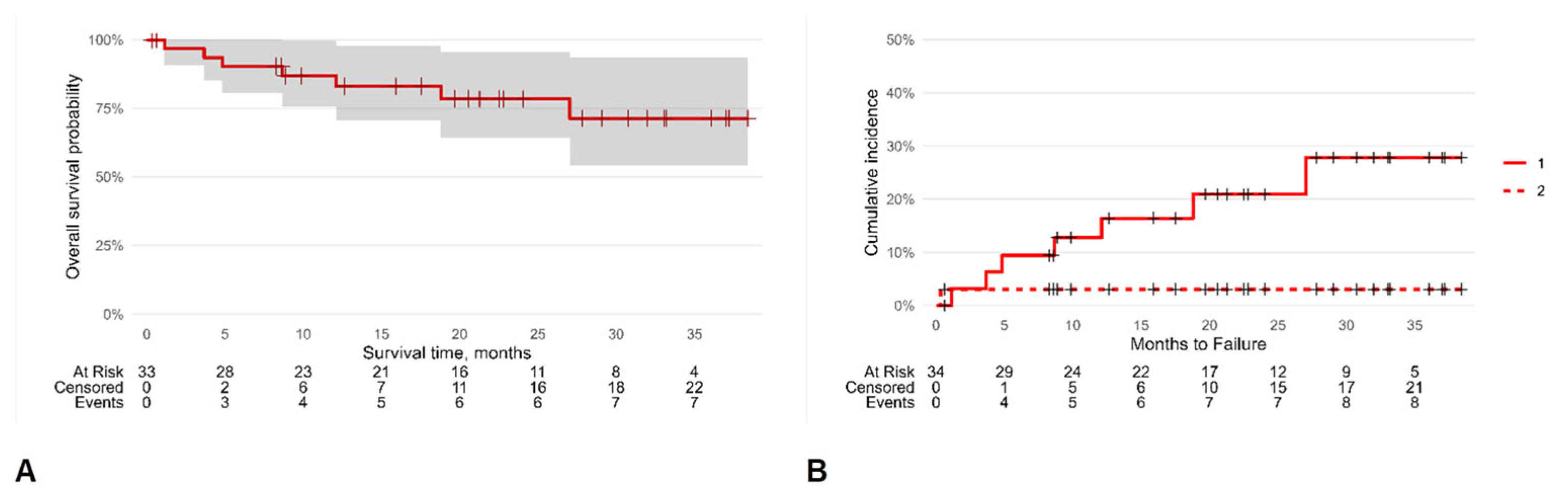
Statistical Analysis
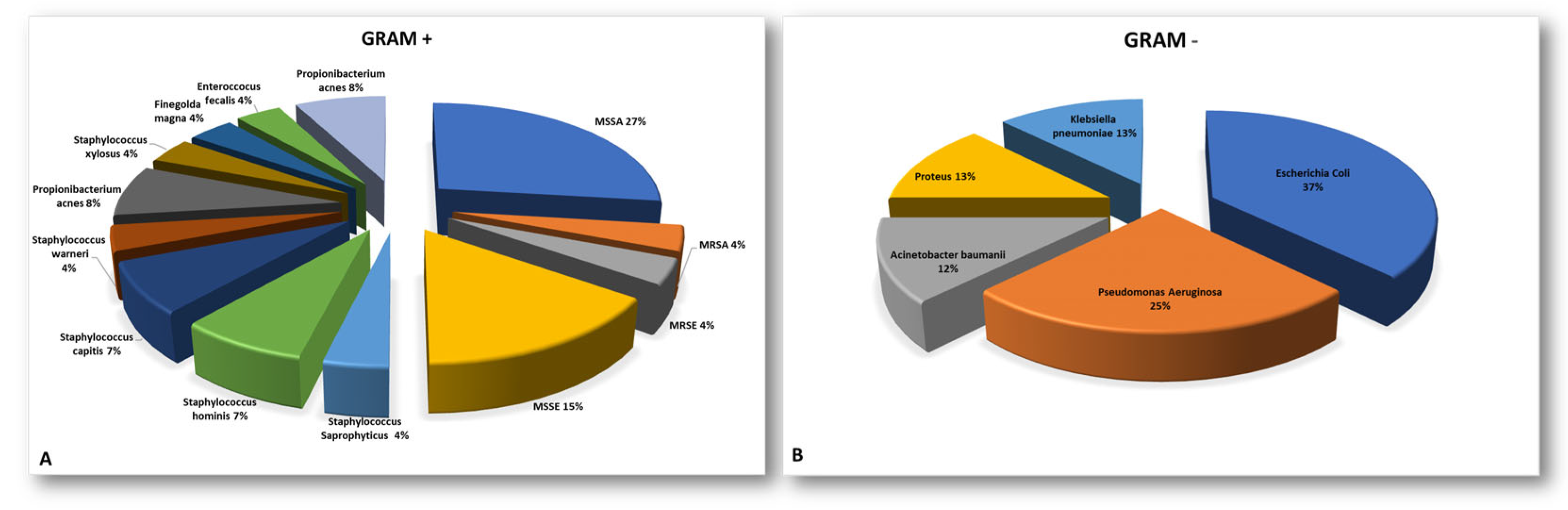
3. Results
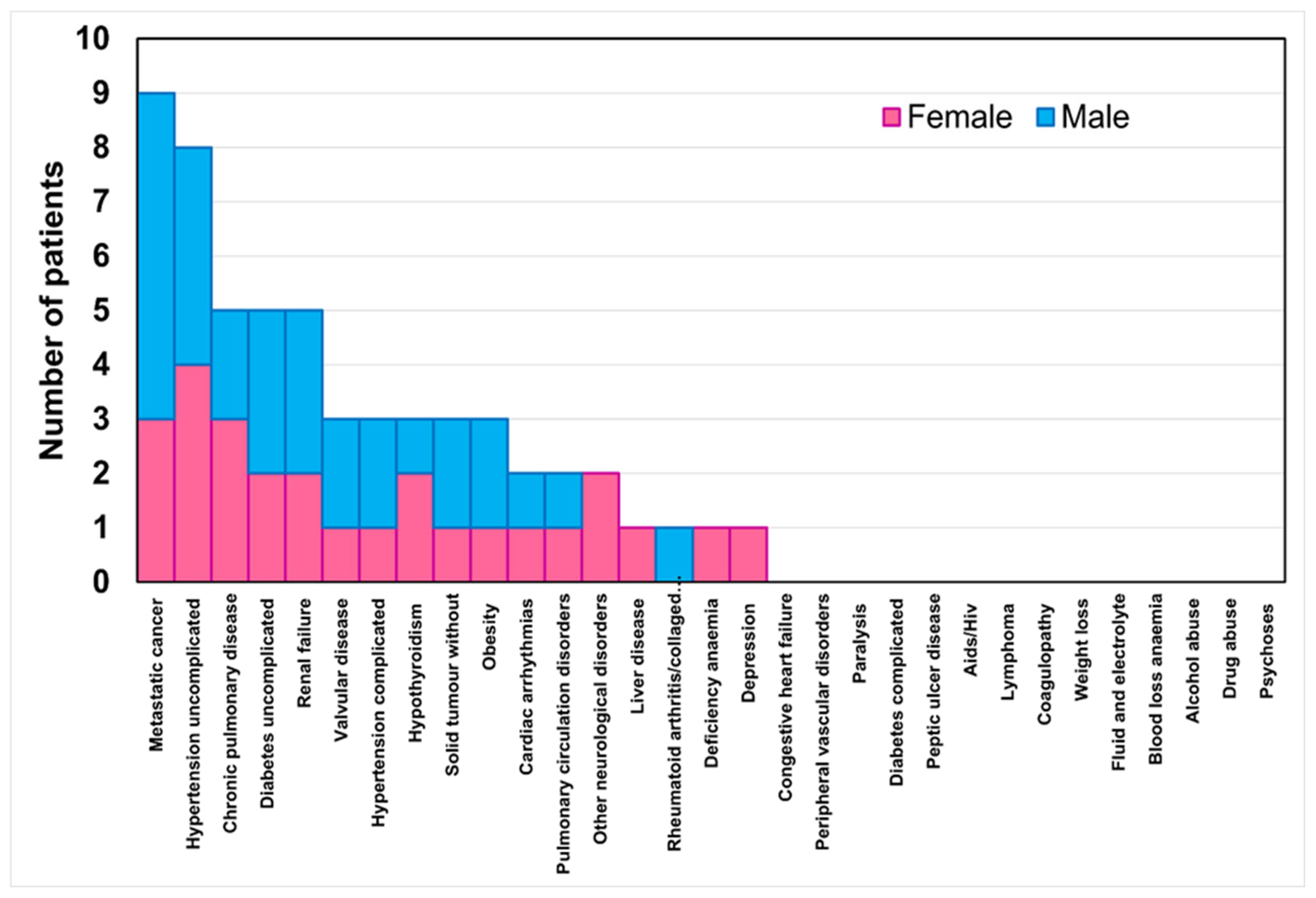
3.1. Clinical and Demographic Data of Patients Before the SFS Implant
3.2. Clinical Records from the SFS Implant
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antibiotic Theraphy | |||
|---|---|---|---|
| Pre-SFS Implant | No. of Patients (%) | Post-SFS Implant | % |
| Amoxicillin + Clavulanic Acid | 1 (3%) | Amoxicillin + Clavulanic Acid | 1 (3%) |
| Amoxicillin + Cotrimoxazole | 1 (3%) | Amphotericin B | 1 (3%) |
| Ciprofloxacin | 1 (3%) | Dalbavancin + Voriconazole | 1 (3%) |
| Daptomycin + Fosfomycin | 2 (6%) | Daptomycin + Piperalillin + Tazobactam | 3 (9%) |
| Daptomycin + Oxacillin | 1 (3%) | Daptomycin + Rifampicin + Fosfomycin | 1 (3%) |
| Daptomycin + Piperalillin + Tazobactam | 3 (9%) | Levofloxacin + Cefiderocol | 1 (3%) |
| Daptomycin + Rifampin + Levofluoxacin | 1 (3%) | Levofluoxacin + Rifampicin | 4 (12%) |
| Ertapenem + Fosfomycin | 1 (3%) | Linezolid + Ertapenem + Fosphomycin | 1 (3%) |
| Levofluoxacin + Rifampicin | 2 (6%) | Minocycline + Rifampicin | 6 (19%) |
| Macladin | 1 (3%) | NA | 5 (15%) |
| Piperalillin + Tazobactam | 1 (3%) | Piperalillin + Tazobactam | 1 (3%) |
| Piperalillin + Tazobactam + Linezolid + Ciprofloxacin | 1 (3%) | Piperalillin + Tazobactam + Ciprofloxacin | 1 (3%) |
| Teicoplanin | 1 (3%) | Piperalillin + Tazobactam + Linezolid + Ciprofloxacin | 1 (3%) |
| Teicoplanin + Ciprofloxacin | 1 (3%) | Piperalillin + Tazobactam + Minocycline | 1 (3%) |
| Teicoplanin + Piperalillin + Tazobactam | 1 (3%) | Rifampicin | 1 (3%) |
| No treatment | 15 (44%) | Teicoplanin | 3 (95) |
| Trimetoprim + Sulfametoxazolo + Ciprofluoxacin | 1 (3%) | ||
| Trimetoprim + Sulfametoxazolo + Rifampicin | 1 (3%) | ||
References
- Barbanti-Brodano, G.; Griffoni, C.; Halme, J.; Tedesco, G.; Terzi, S.; Bandiera, S.; Ghermandi, R.; Evangelisti, G.; Girolami, M.; Pipola, V.; et al. Spinal surgery complications: An unsolved problem-Is the World Health Organization Safety Surgical Checklist an useful tool to reduce them? Eur. Spine J. 2020, 9, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lin, Y.; Yao, W.; Zhang, A.; Gao, L.; Feng, F. Surgical site infection in spinal surgery: A bibliometric analysis. J. Orthop. Surg. Res. 2023, 18, 337. [Google Scholar] [CrossRef]
- Ogihara, S.; Yamazaki, T.; Shiibashi, M.; Chikuda, H.; Maruyama, T.; Miyoshi, K.; Inanami, H.; Oshima, Y.; Azuma, S.; Kawamura, N.; et al. Risk factors for deep surgical site infection following posterior instrumented fusion for degenerative diseases in the thoracic and/or lumbar spine: A multicenter, observational cohort study of 2913 consecutive cases. Eur. Spine J. 2021, 30, 1756–1764. [Google Scholar] [CrossRef]
- Janssen, D.M.C.; Kramer, M.; Geurts, J.; Rhijn, L.V.; Walenkamp, G.H.I.M.; Willems, P.C. A Retrospective Analysis of Deep Surgical Site Infection Treatment after Instrumented Spinal Fusion with the Use of Supplementary Local Antibiotic Carriers. J. Bone Jt. Infect. 2018, 3, 94–103. [Google Scholar] [CrossRef]
- Abdul-Jabbar, A.; Takemoto, S.; Weber, M.H.; Hu, S.S.; Mummaneni, P.V.; Deviren, V.; Ames, C.P.; Chou, D.; Weinstein, P.R.; Burch, S.; et al. Surgical site infection in spinal surgery: Description of surgical and patient-based risk factors for postoperative infection using administrative claims data. Spine 2012, 37, 1340–1345. [Google Scholar] [CrossRef]
- Dunne, W.M., Jr. Bacterial adhesion: Seen any good biofilms lately? Clin. Microbiol. Rev. 2002, 15, 155–166. [Google Scholar] [CrossRef]
- Labler, L.; Keel, M.; Trentz, O.; Heinzelmann, M. Wound conditioning by vacuum assisted closure (V.A.C.) in postoperative infections after dorsal spine surgery. Eur. Spine J. 2006, 15, 1388–1396. [Google Scholar] [CrossRef]
- Fields, A.C.; Pradarelli, J.C.; Itani, K. Preventing Surgical Site Infections: Looking Beyond the Current Guidelines. JAMA 2020, 323, 1087–1088. [Google Scholar] [CrossRef]
- Stewart, P.S. Mechanisms of antibiotic resistance in bacterial biofilms. Int. J. Med. Microbiol. 2002, 292, 107–113. [Google Scholar] [CrossRef]
- Lemire, J.A.; Harrison, J.J.; Turner, R.J. Antimicrobial activity of metals: Mechanisms, molecular targets and applications. Nat. Rev. Microbiol. 2013, 11, 371–384. [Google Scholar] [CrossRef]
- Durán, N.; Marcato, P.D.; De Conti, R.; Alves, O.L.; Costa, F.T.M.; Brocchi, M. Potential use of silver nanoparticles on pathogenic bacteria, their toxicity and possible mechanisms of action. J. Braz. Chem. Soc. 2010, 21, 949–959. [Google Scholar] [CrossRef]
- Feng, Q.L.; Wu, J.; Chen, G.Q.; Cui, F.Z.; Kim, T.N.; Kim, J.O. A mechanistic study of the antibacterial effect of silver ions on Escherichia coli and Staphylococcus aureus. J. Biomed. Mater. Res. 2000, 52, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Bruna, T.; Maldonado-Bravo, F.; Jara, P.; Caro, N. Silver Nanoparticles and Their Antibacterial Applications. Int. J. Mol. Sci. 2021, 22, 7202. [Google Scholar] [CrossRef] [PubMed]
- Reidy, B.; Haase, A.; Luch, A.; Dawson, K.A.; Lynch, I. Mechanisms of Silver Nanoparticle Release, Transformation and Toxicity: A Critical Review of Current Knowledge and Recommendations for Future Studies and Applications. Materials 2013, 6, 2295–2350. [Google Scholar] [CrossRef]
- Dhayalan, M.; Karikalan, P.; Riyaz Savaas Umar, M.; Srinivasan, N. Biomedical Applications of Silver Nanoparticles. In Silver Micro-Nanoparticles—Properties, Synthesis, Characterization, and Applications; IntechOpen: New York, NY, USA, 2021. [Google Scholar] [CrossRef]
- Fiore, M.; Bruschi, A.; Giannini, C.; Morante, L.; Rondinella, C.; Filippini, M.; Sambri, A.; De Paolis, M. Is Silver the New Gold? A Systematic Review of the Preclinical Evidence of Its Use in Bone Substitutes as Antiseptic. Antibiotics 2022, 11, 995. [Google Scholar] [CrossRef]
- Sambri, A.; Zucchini, R.; Giannini, C.; Zamparini, E.; Viale, P.; Donati, D.M.; De Paolis, M. Silver-coated (PorAg®) endoprosthesis can be protective against reinfection in the treatment of tumor prostheses infection. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 1345–1353. [Google Scholar] [CrossRef]
- Fiore, M.; Sambri, A.; Zucchini, R.; Giannini, C.; Donati, D.M.; De Paolis, M. Silver-coated megaprosthesis in prevention and treatment of peri-prosthetic infections: A systematic review and meta-analysis about efficacy and toxicity in primary and revision surgery. Eur. J. Orthop. Surg. Traumatol. 2021, 31, 201–220. [Google Scholar] [CrossRef]
- Dowdell, J.; Brochin, R.; Kim, J.; Overley, S.; Oren, J.; Freedman, B.; Cho, S. Postoperative Spine Infection: Diagnosis and Management. Global Spine J. 2018, 8 (Suppl. S4), 37S–43S. [Google Scholar] [CrossRef]
- Elixhauser, A.; Steiner, C.; Harris, D.R.; Coffey, R.M. Comorbidity measures for use with administrative data. Med. Care 1998, 36, 8–27. [Google Scholar] [CrossRef]
- Sharma, N.; Schwendimann, R.; Endrich, O.; Ausserhofer, D.; Simon, M. Comparing Charlson and Elixhauser comorbidity indices with different weightings to predict in-hospital mortality: An analysis of national inpatient data. BMC Health Serv. Res. 2021, 21, 13. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2023; Available online: https://www.R-project.org (accessed on 13 January 2025).
- Therneau, T.M.; Lumley, T. Survival Analysis Package. Version 2.39-4. 2016. Available online: https://cran.r-project.org/web/packages/survival/survival.pdf (accessed on 24 April 2024).
- Gray, B. Subdistribution Analysis of Competing Risks. Version 2.2-7. 2014. Available online: https://cran.r-project.org/web/packages/cmprsk/cmprsk.pdf (accessed on 24 May 2024).
- Fine, J.P.; Gray, R.J. A proportional hazards model for the subdistribution of a competing risk. JASA 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Morimoto, T.; Hirata, H.; Eto, S.; Hashimoto, A.; Kii, S.; Kobayashi, T.; Tsukamoto, M.; Yoshihara, T.; Toda, Y.; Mawatari, M. Development of Silver-Containing Hydroxyapatite-Coated Antimicrobial Implants for Orthopaedic and Spinal Surgery. Medicina 2022, 58, 519. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Zhang, P.; Bi, J.; Nguyen, N.H.; Dang, Y.; Xu, Z.; Wang, H.; Ninan, N.; Bright, R.; Pham, T.; et al. Silver-Gallium Nano-Amalgamated Particles as a Novel, Biocompatible Solution for Antibacterial Coatings. Adv. Funct. Mater. 2024, 34, 2310539. [Google Scholar] [CrossRef]
- Seçinti, K.D.; Attar, A.; Seçinti, E. Clinical Trial Using A Silver-Coated Screw-Rod System and One-Year Follow-Up of The First 50 Patients. J. Nerv. Sys. Surg. 2016, 6, 10–21. [Google Scholar]
- Morimoto, T.; Tsukamoto, M.; Aita, K.; Fujita, N.; Mawatari, M. First clinical experience with posterior lumbar interbody fusion using a thermal-sprayed silver-containing hydroxyapatite-coated cage. J. Orthop. Surg. Res. 2023, 18, 392. [Google Scholar] [CrossRef]
- Tsuchiya, H.; Shirai, T.; Nishida, H.; Murakami, H.; Kabata, T.; Yamamoto, N.; Watanabe, K.; Nakase, J. Innovative antimicrobial coating of titanium implants with iodine. J. Orthop. Sci. 2012, 17, 595–604. [Google Scholar] [CrossRef]
- Shirai, T.; Tsuchiya, H.; Terauchi, R.; Tsuchida, S.; Mizoshiri, N.; Mori, Y.; Takeuchi, A.; Hayashi, K.; Yamamoto, N.; Ikoma, K.; et al. A retrospective study of antibacterial iodine-coated implants for postoperative infection. Medicine 2019, 98, e17932. [Google Scholar] [CrossRef]
- Demura, S.; Murakami, H.; Shirai, T.; Kato, S.; Yoshioka, K.; Ota, T.; Ishii, T.; Igarashi, T.; Tsuchiya, H. Surgical treatment for pyogenic vertebral osteomyelitis using iodine-supported spinal instruments: Initial case series of 14 patients. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 261–266. [Google Scholar] [CrossRef]
- Scoccianti, G.; Frenos, F.; Beltrami, G.; Campanacci, D.A.; Capanna, R. Levels of silver ions in body fluids and clinical results in silver-coated megaprostheses after tumour, trauma or failed arthroplasty. Injury 2016, 47 (Suppl. S4), S11–S16. [Google Scholar] [CrossRef]
- Wafa, H.; Grimer, R.J.; Reddy, K.; Jeys, L.; Abudu, A.; Carter, S.R.; Tillman, R.M. Retrospective evaluation of the incidence of early periprosthetic infection with silver-treated endoprostheses in high-risk patients: Case-control study. Bone Jt. J. 2015, 97-B, 252–257. [Google Scholar] [CrossRef]
- Smolle, M.A.; Bergovec, M.; Scheipl, S.; Gössler, W.; Amerstorfer, F.; Glehr, M.; Leithner, A.; Friesenbichler, J. Long-term changes in serum silver concentrations after extremity reconstruction with silver-coated megaprostheses. Sci. Rep. 2022, 12, 13041. [Google Scholar] [CrossRef]
| Variables | Total | p-Value | Female | Male | p-Value | |
|---|---|---|---|---|---|---|
| Patients (n) | 34 | 15 | 19 | 0.398 | ||
| Age (yrs) | 59 [55, 63] | 58 [53, 63] | 59 [55, 63] | 0.608 | ||
| Age class, n (%) | ≤40 | 4 (11.8) | 0.159 | 2 (5.9) | 2 (5.9) | 0.923 |
| 41–50 | 4 (11.8) | 2 (5.9) | 2 (5.9) | |||
| 51–60 | 8 (23.4) | 4 (11.7) | 4 (11.7) | |||
| 61–70 | 12 (35.2) | 4 (11.7) | 8 (23.5) | |||
| >70 | 6 (17.8) | 3 (8.9) | 3 (8.9) | |||
| BMI class, n (%) | Underweight <18.5 | 2 (5.8) | <0.005 | 1 (2.9) | 1 (2.9) | 0.943 |
| Healthy weight 18.5–24.9 | 13 (38.3) | 6 (17.7) | 7 (20.6) | |||
| Overweight 25.0–29.9 | 13 (38.3) | 6 (17.7) | 7 (20.6) | |||
| Class 1 obesity 30.0–34.9 | 4 (11.8) | 1 (2.9) | 3 (8.9) | |||
| Class 2 obesity 35.0–39.9 | 2 (5.8) | 1 (2.9) | 1 (2.9) | |||
| Smoking, n (%) | N | 24 (70.6) | 0.016 | 11 (32.4) | 13 (38.2) | 1.000 |
| Y | 10 (29.4) | 4 (11.8) | 6 (17.6) | |||
| Oncological diseases, n (%) | N | 19 (55.9) | 0.493 | 10 (29.4) | 9 (26.5) | 0.314 |
| Y | 15 (44.1) | 5 (14.7) | 10 (29.4) | |||
| Type of surgery before SFS, n (%) | Arthrodesis | 11 (32.4) | 0.572 | 4 (11.8) | 7 (20.6) | 0.657 |
| Revision surgery | 14 (41.2) | 9 (26.4) | 5 (14.7) | |||
| Vertebrectomy | 9 (26.4) | 2 (5.9) | 7 (20.6) | |||
| Treatment for infection before SFS, n (%) | Spinal fixation removal | 3 (23.0) | < 0.005 | 1 (7.7) | 2 (15.4) | 0.842 |
| Surgical debridement | 10 (77.0) | 4 (30.7) | 6 (46.2) | |||
| Total | p-Value | Female | Male | p-Value | ||
|---|---|---|---|---|---|---|
| Patients (n) | 34 | 15 | 19 | |||
| Site, n (%) | Thoracic | 7 (20.7) | 0.248 | 3 (8.8) | 4 (11.9) | 0.739 |
| Lumbar | 3 (8.8) | 2 (5.9) | 1 (2.9) | |||
| Thoracolumbar | 8 (23.5) | 2 (5.9) | 6 (17.6) | |||
| Lumbosacral | 11 (32.3) | 5 (14.7) | 6 (17.6) | |||
| Thoraco-lumbosacral | 5 (14.7) | 3 (8.8) | 2 (5.9) | |||
| Complications, n (%) | No | 26 (76.6) | <0.0005 | 11 (32.4) | 15 (44.2) | 0.929 |
| Mobilization/break of SFS components | 2 (5.9) | 1 (2.9) | 1 (2.9) | |||
| Suspected or relapsing infective event | 6 (17.6) | 3 (8.8) | 3 (8.8 | |||
| LOS (days) | 15 [11, 19] | - | 14 [10, 18] | 17 [10, 23] | 0.559 | |
| Healing time after SFS (months) | 4.2 [3.1, 5.3] | - | 4.0 [2.3, 5.7] | 4.4 [2.8, 6.0] | 0.715 | |
| Life SFS (months) | 19.1 [15.8, 22.4] | - | 15.8 [10.8, 20.8] | 21.6 [17.4, 25.9] | 0.067 | |
| Score | p-Value | <0 | 0 | 1 to 4 | ≥5 | p-Value | |
|---|---|---|---|---|---|---|---|
| N | 7 [4, 10] | - | 8 | 5 | 2 | 19 | - |
| Sex (n) | |||||||
| Female | 7 [2, 12] | 0.954 | 3 | 2 | 2 | 8 | 0.536 |
| Male | 7 [3, 10] | 5 | 3 | - | 11 | ||
| Age (n) | |||||||
| ≤40 | 5 [−2, 12] | 0.592 | 0 | 2 | 1 | 1 | 0.167 |
| 41–50 | 1 [−3, 4] | 2 | 1 | 0 | 1 | ||
| 51–60 | 9 [1, 16] | 2 | 0 | 0 | 6 | ||
| 61–70 | 10 [4, 15] | 2 | 2 | 0 | 8 | ||
| >70 | 5 [1, 10] | 2 | 0 | 1 | 3 | ||
| BMI (n) | |||||||
| Underweight <18.5 | 2 [−23, 26] | 0.795 | 1 | 0 | 0 | 1 | 0.502 |
| Healthy weight 18.5–24.9 | 7 [4, 11] | 2 | 3 | 0 | 8 | ||
| Overweight 25.0–29.9 | 8 [3, 14] | 3 | 1 | 1 | 8 | ||
| Class 1 obesity 30.0–34.9 | 2 [−7, 10] | 2 | 1 | 0 | 1 | ||
| Class 2 obesity 35.0–39.9 | 9 [−3, 21] | 0 | 0 | 1 | 1 | ||
| LOS (days) | |||||||
| - | 19 [6, 32] | 13 [9, 17] | 11 [5, 16] | 15 [10, 20] | 0.818 | ||
| Healing time after SFS (months) | |||||||
| - | 5 [3, 7] | 4 [1, 9] | 8 [1, 17] | 2 [2, 5] | 0.509 | ||
| SFS failure | |||||||
| Y | 7 [3, 10] | 0.996 | 6 | 5 | 1 | 14 | 0.700 |
| N | 7 [0, 13] | 2 | 0 | 1 | 4 | ||
| SFS life (months) | |||||||
| - | 23.3 [15.2, 3.3] | 16.0 [6.7, 25.3] | 12.3 [6.3, 8.2] | 18.8 [14.6,3.0] | 0.582 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leggi, L.; Terzi, S.; Sartori, M.; Salamanna, F.; Boriani, L.; Asunis, E.; Griffoni, C.; Giavaresi, G.; Gasbarrini, A. First Clinical Evidence About the Use of a New Silver-Coated Titanium Alloy Instrumentation to Counteract Surgical Site Infection at the Spine Level. J. Funct. Biomater. 2025, 16, 30. https://doi.org/10.3390/jfb16010030
Leggi L, Terzi S, Sartori M, Salamanna F, Boriani L, Asunis E, Griffoni C, Giavaresi G, Gasbarrini A. First Clinical Evidence About the Use of a New Silver-Coated Titanium Alloy Instrumentation to Counteract Surgical Site Infection at the Spine Level. Journal of Functional Biomaterials. 2025; 16(1):30. https://doi.org/10.3390/jfb16010030
Chicago/Turabian StyleLeggi, Lucrezia, Silvia Terzi, Maria Sartori, Francesca Salamanna, Luca Boriani, Emanuela Asunis, Cristiana Griffoni, Gianluca Giavaresi, and Alessandro Gasbarrini. 2025. "First Clinical Evidence About the Use of a New Silver-Coated Titanium Alloy Instrumentation to Counteract Surgical Site Infection at the Spine Level" Journal of Functional Biomaterials 16, no. 1: 30. https://doi.org/10.3390/jfb16010030
APA StyleLeggi, L., Terzi, S., Sartori, M., Salamanna, F., Boriani, L., Asunis, E., Griffoni, C., Giavaresi, G., & Gasbarrini, A. (2025). First Clinical Evidence About the Use of a New Silver-Coated Titanium Alloy Instrumentation to Counteract Surgical Site Infection at the Spine Level. Journal of Functional Biomaterials, 16(1), 30. https://doi.org/10.3390/jfb16010030