
Rapid Recovery after Reparation of Full-Thickness Chondral Defects of the Knee with the Use of Hyaluronan (HA)-Based 3-D Scaffold


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Ethical Considerations
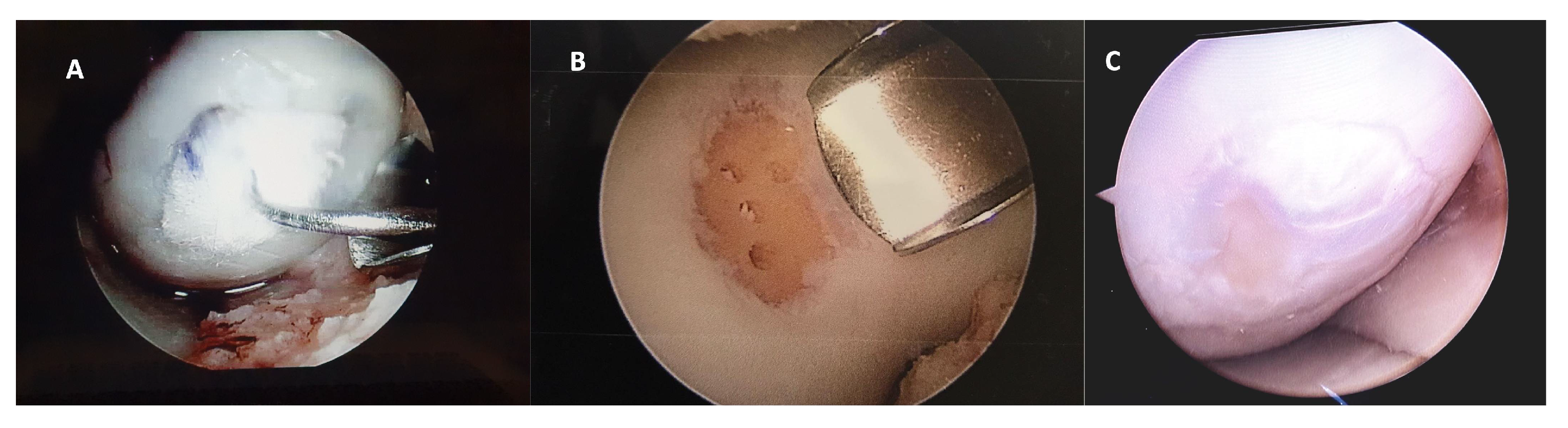
2.3. Surgical Techniques
2.4. Functional Status
2.5. MRI Assessment and Henderson Scale
2.6. Second-Look Arthroscopy
2.7. Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Curl, W.W.; Krome, J.; Gordon, E.S.; Rushing, J.; Smith, B.P.; Poehling, G.G. Cartilage injuries: A review of 31,516 knee arthroscopies. Arthroscopy 1997, 13, 456–460. [Google Scholar] [CrossRef]
- Widuchowski, W.; Widuchowski, J.; Trzaska, T. Articular cartilage defects: Study of 25,124 knee arthroscopies. Knee 2007, 14, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Sophia Fox, A.J.; Bedi, A.; Rodeo, S.A. The basic science of articular cartilage: Structure, composition, and function. Sports Health 2009, 1, 461–468. [Google Scholar] [CrossRef]
- Guermazi, A.; Hayashi, D.; Roemer, F.W.; Niu, J.; Quinn, E.K.; Crema, M.D.; Nevitt, M.C.; Torner, J.; Lewis, C.E.; Felson, D.T. Brief Report: Partial- and Full-Thickness Focal Cartilage Defects Contribute Equally to Development of New Cartilage Damage in Knee Osteoarthritis: The Multicenter Osteoarthritis Study. Arthritis Rheumatol. 2017, 69, 560–564. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, D.; Calvo, R.; Vaisman, A.; Carrasco, M.A.; Moraga, C.; Delgado, I. Knee chondral lesions: Incidence and correlation between arthroscopic and magnetic resonance findings. Arthroscopy 2007, 23, 312–315. [Google Scholar] [CrossRef]
- Hopkins, T.; Roberts, S.; Richardson, J.B.; Gallacher, P.; Bailey, A.; Kuiper, J.H. Relationship Between Activity Level and Knee Function Is Influenced by Negative Affect in Patients Undergoing Cell Therapy for Articular Cartilage Defects in the Knee. Orthop. J. Sports Med. 2023, 11, 23259671231151925. [Google Scholar] [CrossRef] [PubMed]
- Goldring, M.B.; Marcu, K.B. Cartilage homeostasis in health and rheumatic diseases. Arthritis Res. Ther. 2009, 11, 224. [Google Scholar] [CrossRef]
- Seewoonarain, S.; Ganesh, D.; Perera, E.; Popat, R.; Jones, J.; Sugand, K.; Gupte, C. Scaffold-associated procedures are superior to microfracture in managing focal cartilage defects in the knee: A systematic review & meta-analysis. Knee 2023, 42, 320–338. [Google Scholar] [CrossRef]
- Zamborsky, R.; Danisovic, L. Surgical Techniques for Knee Cartilage Repair: An Updated Large-Scale Systematic Review and Network Meta-analysis of Randomized Controlled Trials. Arthroscopy 2020, 36, 845–858. [Google Scholar] [CrossRef]
- Brittberg, M.; Lindahl, A.; Nilsson, A.; Ohlsson, C.; Isaksson, O.; Peterson, L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N. Engl. J. Med. 1994, 331, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Knutsen, G.; Drogset, J.O.; Engebretsen, L.; Grontvedt, T.; Ludvigsen, T.C.; Loken, S.; Solheim, E.; Strand, T.; Johansen, O. A Randomized Multicenter Trial Comparing Autologous Chondrocyte Implantation with Microfracture: Long-Term Follow-up at 14 to 15 Years. J. Bone Joint Surg. Am. 2016, 98, 1332–1339. [Google Scholar] [CrossRef]
- Shimomura, K.; Ando, W.; Moriguchi, Y.; Sugita, N.; Yasui, Y.; Koizumi, K.; Fujie, H.; Hart, D.A.; Yoshikawa, H.; Nakamura, N. Next Generation Mesenchymal Stem Cell (MSC)-Based Cartilage Repair Using Scaffold-Free Tissue Engineered Constructs Generated with Synovial Mesenchymal Stem Cells. Cartilage 2015, 6, 13S–29S. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, K.; Yasui, Y.; Koizumi, K.; Chijimatsu, R.; Hart, D.A.; Yonetani, Y.; Ando, W.; Nishii, T.; Kanamoto, T.; Horibe, S.; et al. First-in-Human Pilot Study of Implantation of a Scaffold-Free Tissue-Engineered Construct Generated From Autologous Synovial Mesenchymal Stem Cells for Repair of Knee Chondral Lesions. Am. J. Sports Med. 2018, 46, 2384–2393. [Google Scholar] [CrossRef] [PubMed]
- Galarraga, J.H.; Zlotnick, H.M.; Locke, R.C.; Gupta, S.; Fogarty, N.L.; Masada, K.M.; Stoeckl, B.D.; Laforest, L.; Castilho, M.; Malda, J.; et al. Evaluation of surgical fixation methods for the implantation of melt electrowriting-reinforced hyaluronic acid hydrogel composites in porcine cartilage defects. Int. J. Bioprint 2023, 9, 775. [Google Scholar] [CrossRef]
- Patrascu, J.M.; Freymann, U.; Kaps, C.; Poenaru, D.V. Repair of a post-traumatic cartilage defect with a cell-free polymer-based cartilage implant: A follow-up at two years by MRI and histological review. J. Bone Joint Surg. Br. 2010, 92, 1160–1163. [Google Scholar] [CrossRef] [PubMed]
- Kon, E.; Gobbi, A.; Filardo, G.; Delcogliano, M.; Zaffagnini, S.; Marcacci, M. Arthroscopic second-generation autologous chondrocyte implantation compared with microfracture for chondral lesions of the knee: Prospective nonrandomized study at 5 years. Am. J. Sports Med. 2009, 37, 33–41. [Google Scholar] [CrossRef]
- Amirsaadat, S.; Amirazad, H.; Hashemihesar, R.; Zarghami, N. An update on the effect of intra-articular intervention strategies using nanomaterials in osteoarthritis: Possible clinical application. Front. Bioeng. Biotechnol. 2023, 11, 1128856. [Google Scholar] [CrossRef]
- Evaniew, N.; Simunovic, N.; Karlsson, J. Cochrane in CORR(R): Viscosupplementation for the treatment of osteoarthritis of the knee. Clin. Orthop. Relat. Res. 2014, 472, 2028–2034. [Google Scholar] [CrossRef]
- Bowden, D.J.; Byrne, C.A.; Alkhayat, A.; Eustace, S.J.; Kavanagh, E.C. Injectable Viscoelastic Supplements: A Review for Radiologists. AJR Am. J. Roentgenol. 2017, 209, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Marx, R.G.; Jones, E.C.; Allen, A.A.; Altchek, D.W.; O’Brien, S.J.; Rodeo, S.A.; Williams, R.J.; Warren, R.F.; Wickiewicz, T.L. Reliability, validity, and responsiveness of four knee outcome scales for athletic patients. J. Bone Joint Surg. Am. 2001, 83, 1459–1469. [Google Scholar] [CrossRef]
- Henderson, I.; Francisco, R.; Oakes, B.; Cameron, J. Autologous chondrocyte implantation for treatment of focal chondral defects of the knee--a clinical, arthroscopic, MRI and histologic evaluation at 2 years. Knee 2005, 12, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo Quiceno, G.A.; Sarmiento Riveros, P.A.; Ochoa Perea, G.A.; Vergara, M.G.; Rodriguez Munoz, L.F.; Arias Perez, R.D.; Piovesan, N.O.; Munoz Salamanca, J.A. Satisfactory clinical outcomes with autologous matrix-induced chondrogenesis in the treatment of grade IV chondral injuries of the knee. J. ISAKOS 2023, 8, 86–93. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.I.; Tho, S.J.W.; Tho, K.S. Biological resurfacing of grade IV articular cartilage ulcers in knee joint with Hyalofast. J. Orthop. Surg. 2020, 28, 2309499020905158. [Google Scholar] [CrossRef]
- McCormick, F.; Harris, J.D.; Abrams, G.D.; Frank, R.; Gupta, A.; Hussey, K.; Wilson, H.; Bach, B., Jr.; Cole, B. Trends in the surgical treatment of articular cartilage lesions in the United States: An analysis of a large private-payer database over a period of 8 years. Arthroscopy 2014, 30, 222–226. [Google Scholar] [CrossRef]
- Wasyleczko, M.; Sikorska, W.; Chwojnowski, A. Review of Synthetic and Hybrid Scaffolds in Cartilage Tissue Engineering. Membranes 2020, 10, 348. [Google Scholar] [CrossRef]
- Altschuler, N.; Zaslav, K.R.; Di Matteo, B.; Sherman, S.L.; Gomoll, A.H.; Hacker, S.A.; Verdonk, P.; Dulic, O.; Patrascu, J.M.; Levy, A.S.; et al. Aragonite-Based Scaffold Versus Microfractures and Debridement for the Treatment of Knee Chondral and Osteochondral Lesions: Results of a Multicenter Randomized Controlled Trial. Am. J. Sports Med. 2023, 51, 957–967. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.; Orozco, Y.; Betancur, A.; Moreno, A.I.; Fuentes, K.; Lopera, A.; Suarez, O.; Lobo, T.; Ossa, A.; Pelaez-Vargas, A.; et al. Fabrication of polycaprolactone/calcium phosphates hybrid scaffolds impregnated with plant extracts using 3D printing for potential bone regeneration. Heliyon 2023, 9, e13176. [Google Scholar] [CrossRef]
- Freymann, U.; Endres, M.; Neumann, K.; Scholman, H.J.; Morawietz, L.; Kaps, C. Expanded human meniscus-derived cells in 3-D polymer-hyaluronan scaffolds for meniscus repair. Acta Biomater. 2012, 8, 677–685. [Google Scholar] [CrossRef]
- Brockmeier, S.F.; Shaffer, B.S. Viscosupplementation therapy for osteoarthritis. Sports Med. Arthrosc. Rev. 2006, 14, 155–162. [Google Scholar] [CrossRef]
- Yagishita, K.; Sekiya, I.; Sakaguchi, Y.; Shinomiya, K.; Muneta, T. The effect of hyaluronan on tendon healing in rabbits. Arthroscopy 2005, 21, 1330–1336. [Google Scholar] [CrossRef]
- Leng, Y.; Abdullah, A.; Wendt, M.K.; Calve, S. Hyaluronic acid, CD44 and RHAMM regulate myoblast behavior during embryogenesis. Matrix Biol. 2019, 78–79, 236–254. [Google Scholar] [CrossRef]
- Kawano, M.; Ariyoshi, W.; Iwanaga, K.; Okinaga, T.; Habu, M.; Yoshioka, I.; Tominaga, K.; Nishihara, T. Mechanism involved in enhancement of osteoblast differentiation by hyaluronic acid. Biochem. Biophys. Res. Commun. 2011, 405, 575–580. [Google Scholar] [CrossRef]
- Snetkov, P.; Zakharova, K.; Morozkina, S.; Olekhnovich, R.; Uspenskaya, M. Hyaluronic Acid: The Influence of Molecular Weight on Structural, Physical, Physico-Chemical, and Degradable Properties of Biopolymer. Polymers 2020, 12, 1800. [Google Scholar] [CrossRef]
- Karam, J.; Singer, B.J.; Miwa, H.; Chen, L.H.; Maran, K.; Hasani, M.; Garza, S.; Onyekwere, B.; Yeh, H.C.; Li, S.; et al. Molecular weight of hyaluronic acid crosslinked into biomaterial scaffolds affects angiogenic potential. Acta Biomater. 2023, 169, 228–242. [Google Scholar] [CrossRef]
- Garrity, J.T.; Stoker, A.M.; Sims, H.J.; Cook, J.L. Improved osteochondral allograft preservation using serum-free media at body temperature. Am. J. Sports Med. 2012, 40, 2542–2548. [Google Scholar] [CrossRef] [PubMed]
- Themistocleous, G.S.; Chloros, G.D.; Kyrantzoulis, I.M.; Georgokostas, I.A.; Themistocleous, M.S.; Papagelopoulos, P.J.; Savvidou, O.D. Effectiveness of a single intra-articular bone marrow aspirate concentrate (BMAC) injection in patients with grade 3 and 4 knee osteoarthritis. Heliyon 2018, 4, e00871. [Google Scholar] [CrossRef] [PubMed]
- Spees, J.L.; Lee, R.H.; Gregory, C.A. Mechanisms of mesenchymal stem/stromal cell function. Stem Cell Res. Ther. 2016, 7, 125. [Google Scholar] [CrossRef]
- Hajduga, M.B.; Bobinski, R.; Dutka, M.; Ulman-Wlodarz, I.; Bujok, J.; Pajak, C.; Cwiertnia, M.; Kurowska, A.; Dziadek, M.; Rajzer, I. Analysis of the antibacterial properties of polycaprolactone modified with graphene, bioglass and zinc-doped bioglass. Acta Bioeng. Biomech. 2021, 23, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Zhai, P.; Peng, X.; Li, B.; Liu, Y.; Sun, H.; Li, X. The application of hyaluronic acid in bone regeneration. Int. J. Biol. Macromol. 2020, 151, 1224–1239. [Google Scholar] [CrossRef]
- Huang, G.; Huang, H. Hyaluronic acid-based biopharmaceutical delivery and tumor-targeted drug delivery system. J. Control Release 2018, 278, 122–126. [Google Scholar] [CrossRef]
- Toonstra, J.L.; Howard, J.S.; Uhl, T.L.; English, R.A.; Mattacola, C.G. The role of rehabilitation following autologous chondrocyte implantation: A retrospective chart review. Int. J. Sports Phys. Ther. 2013, 8, 670–679. [Google Scholar] [PubMed]
- Ebert, J.R.; Smith, A.; Edwards, P.K.; Hambly, K.; Wood, D.J.; Ackland, T.R. Factors predictive of outcome 5 years after matrix-induced autologous chondrocyte implantation in the tibiofemoral joint. Am. J. Sports Med. 2013, 41, 1245–1254. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Microfractures (n = 21) | HA 3-D Scaffold (n = 12) | p |
|---|---|---|---|
| Age (mean ± SD) | 34.8 ± 5.1 | 32.3 ± 6.6 | 0.2360 |
| Feminine gender n (%) | 16 (76) | 9 (75) | 0.939 |
| Lesion in the right knee n (%) | 16 (76) | 7 (58) | 0.283 |
| Injury of the medial condyle n (%) | 16 (76) | 7 (58) | 0.283 |
| Lesion site (condyle femoral medial) n (%) | 16 (76) | 7 (58) | 0.283 |
| Lesion size (mm) median (ICR) | 125 (100–225) | 100 (80–100) | 0.088 |
| MCKRS scores before surgery median (ICR) | 46 (44–56) | 44 (43–46) | 0.2696 |
| Henderson scale before surgery median (ICR) | 4 (4–4) | 4 (4–4) | 0 |
| Amateur physical activity n (%) | 19 (91) | 11 (92) | 0.693 |
| Treatment | Baseline | 6 Months | p | 12 Months | p |
|---|---|---|---|---|---|
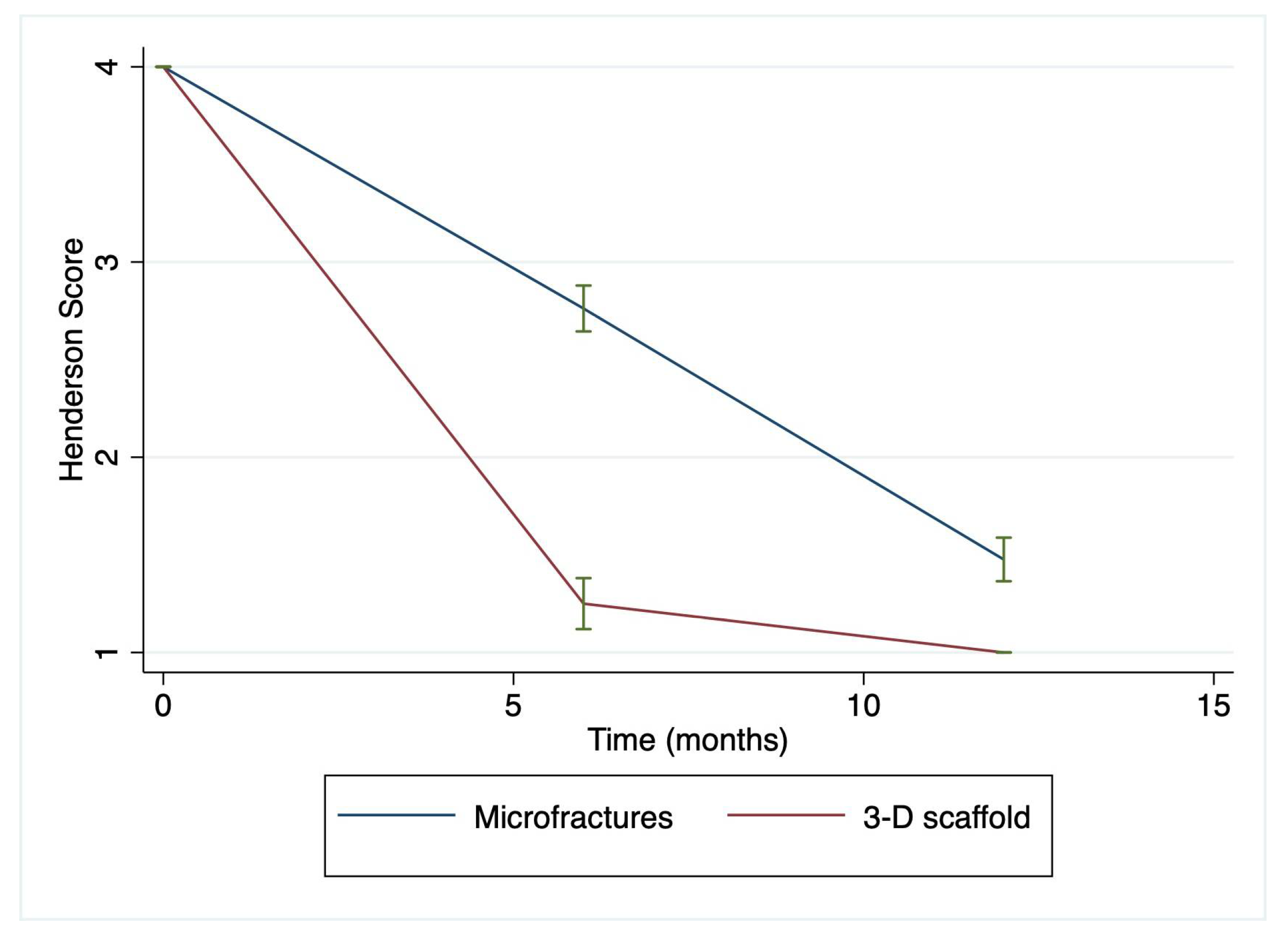
| Henderson Score | |||||
| Microfractures | 4 (4–4) | 3 (2–3) | 0.0001 | 1 (1–2) | 0.0048 |
| 3-D scaffold | 4 (4–4) | 1 (1–1.5) | 1 (1–1) | ||
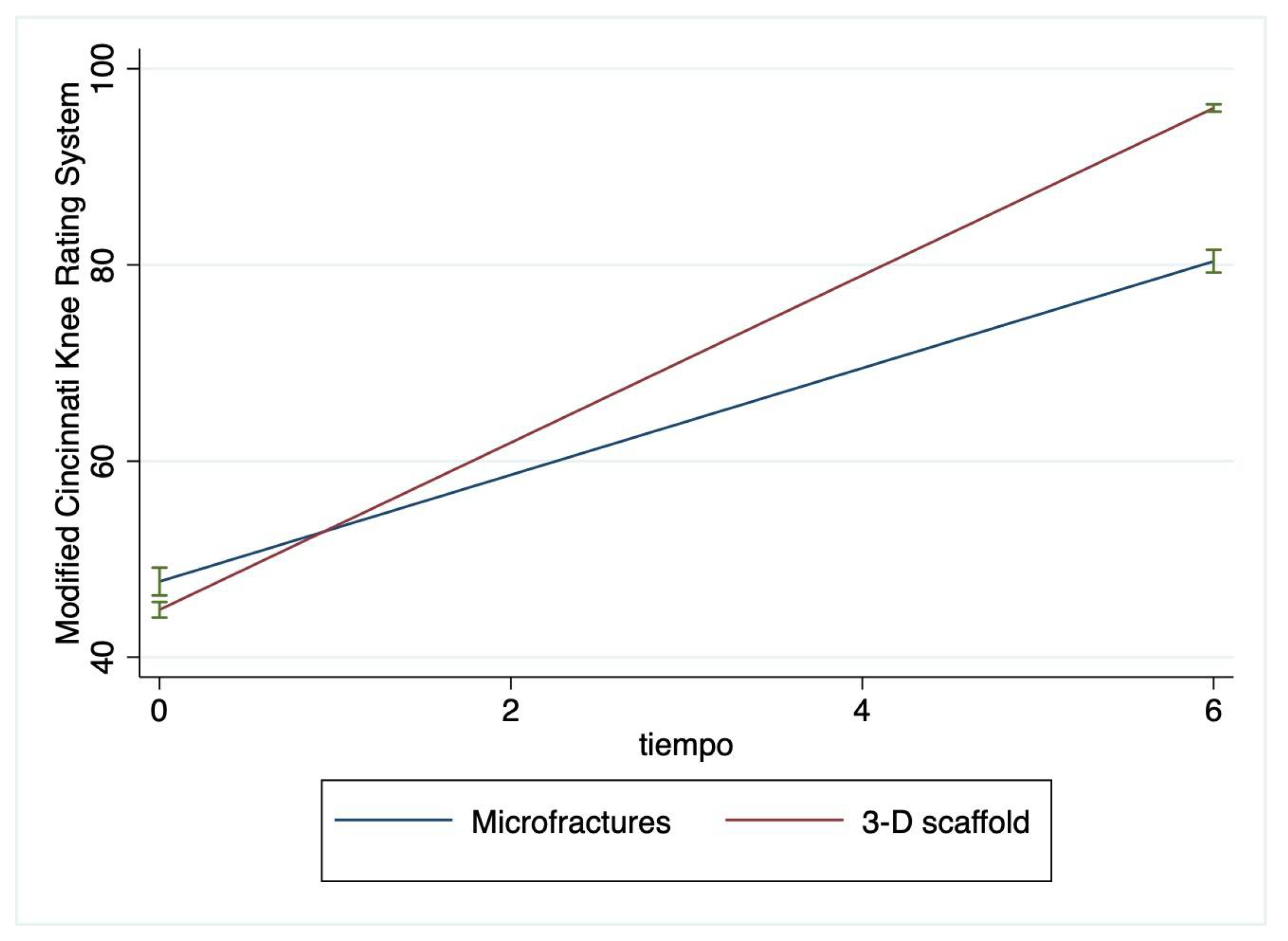
| Modified Cincinnati Knee Rating System | |||||
| Microfractures | 46 (44–56) | 81 (77–83) | 0.0001 | - | - |
| 3-D scaffold | 44 (43–46) | 96.5 (95–97) | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valladares, N.; Cabrero Montes, M.A.; Jacobo-Jimenez, G.J.; Zavala-Cerna, M.G. Rapid Recovery after Reparation of Full-Thickness Chondral Defects of the Knee with the Use of Hyaluronan (HA)-Based 3-D Scaffold. J. Funct. Biomater. 2023, 14, 491. https://doi.org/10.3390/jfb14100491
Valladares N, Cabrero Montes MA, Jacobo-Jimenez GJ, Zavala-Cerna MG. Rapid Recovery after Reparation of Full-Thickness Chondral Defects of the Knee with the Use of Hyaluronan (HA)-Based 3-D Scaffold. Journal of Functional Biomaterials. 2023; 14(10):491. https://doi.org/10.3390/jfb14100491
Chicago/Turabian StyleValladares, Nicolas, Monica Araceli Cabrero Montes, Gibran J. Jacobo-Jimenez, and Maria G. Zavala-Cerna. 2023. "Rapid Recovery after Reparation of Full-Thickness Chondral Defects of the Knee with the Use of Hyaluronan (HA)-Based 3-D Scaffold" Journal of Functional Biomaterials 14, no. 10: 491. https://doi.org/10.3390/jfb14100491
APA StyleValladares, N., Cabrero Montes, M. A., Jacobo-Jimenez, G. J., & Zavala-Cerna, M. G. (2023). Rapid Recovery after Reparation of Full-Thickness Chondral Defects of the Knee with the Use of Hyaluronan (HA)-Based 3-D Scaffold. Journal of Functional Biomaterials, 14(10), 491. https://doi.org/10.3390/jfb14100491