
A COVID Support App Demonstrating the Use of a Rapid Persuasive System Design Approach

Abstract
1. Introduction
- -
- The need to invite and increase the behavior of downloading and using digital COVID apps within the community (something that was being avoided by many people at the very time when direct contact with other people was restricted).
- -
- The need to catalyze and increase users’ behaviors of sharing information with their COVID app, as well as sharing their questions with their app (based on increased confidence and comfort with the privacy of their data within the app, as well as the security of this information, and the safeguards protecting it, thus reducing/eliminating their fears of surveillance and hacking).
- -
- The need to nudge and increasingly precipitate users’ behaviors of using a digital app to look for and find solutions to their COVID-related needs.
- ○
- To increase their information-seeking behaviors within the app, increasing their search for appropriate, credible information about COVID-related topics (rather than relying on their own guesses, using hearsay, or using information from unverified sources).
- ○
- To increase their behavioral tendency to seek services and support for their COVID needs and those of their families.
- -
- The need to increase user’s behaviors of trying to verify the credibility/authenticity of information and services prior to accepting them and/or using them.
- -
- The need to increase the behaviors of using a digital app to connect with others.
2. Approach
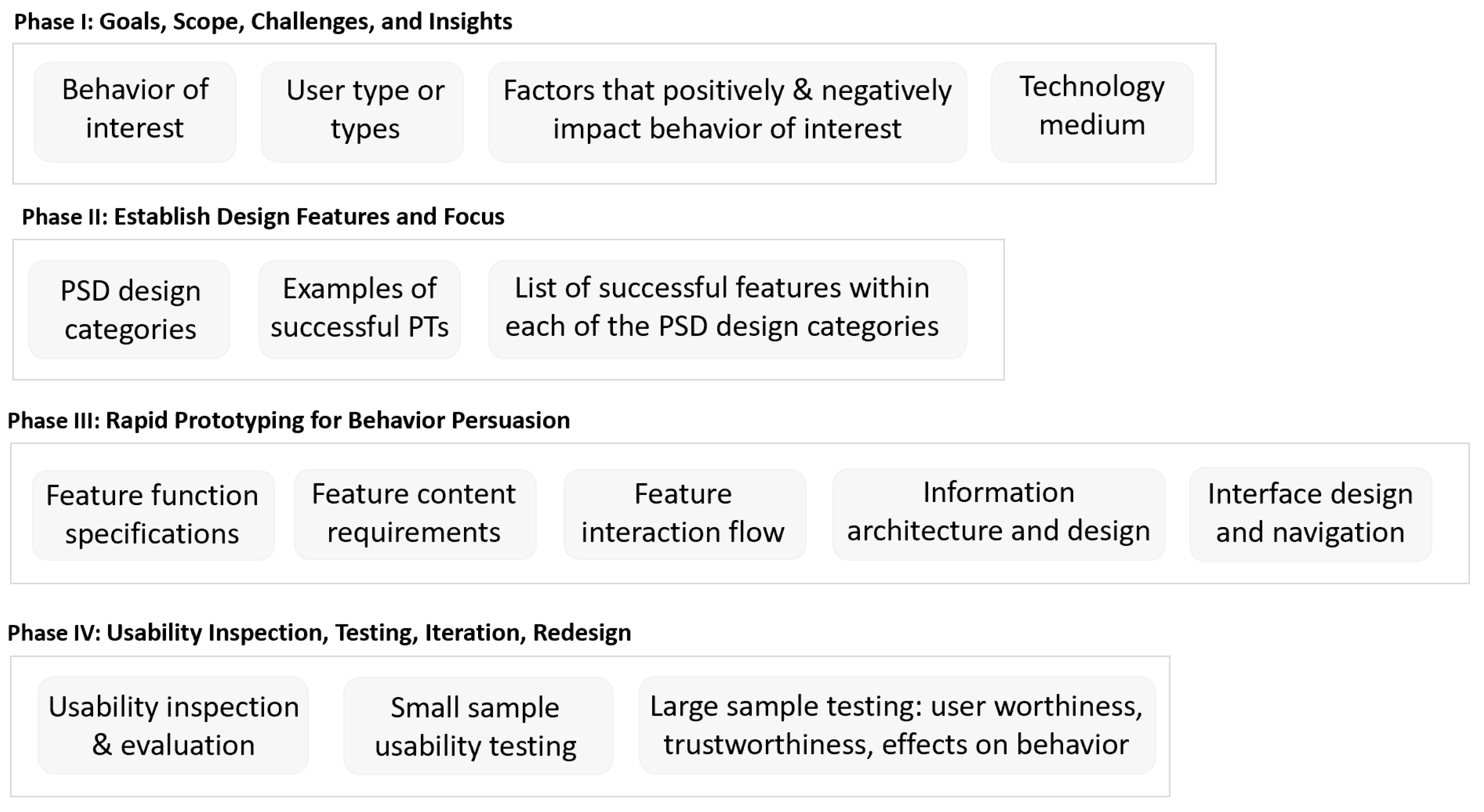
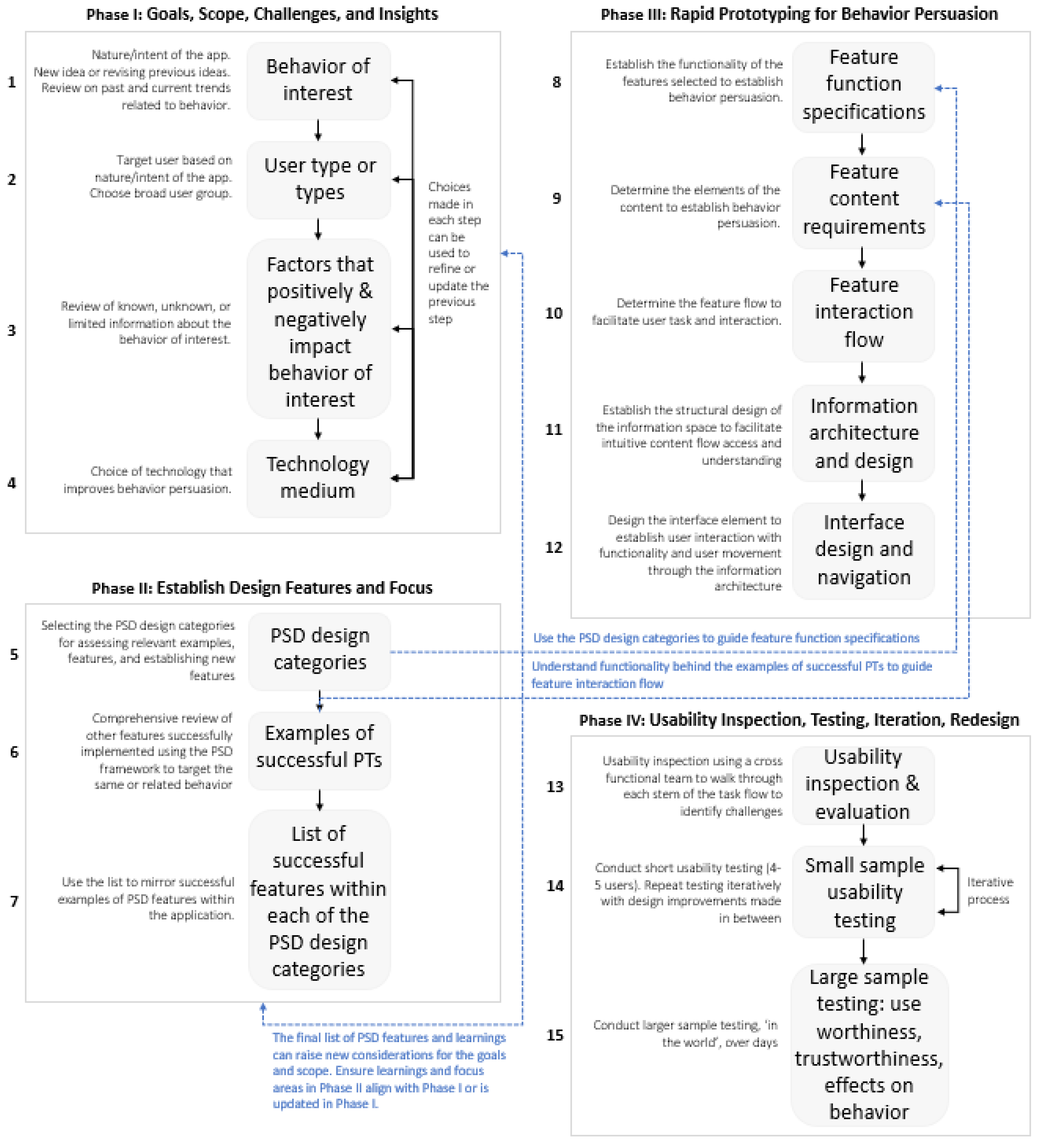
2.1. R-PSD Model
- (a)
- An increase in users’ level of knowledge about COVID (and their confidence in the information that they have), and a decrease in users’ feelings of uncertainty about the information needed/used for decisions affected by COVID.
- (b)
- An increase in the use of credible facts for decision-making, and a reduction in the use of guessing and hearsay as a basis for decision-making about everyday life decisions affected by COVID.
- (c)
- An increase in users’ feelings of comfort and confidence concerning COVID-related decisions and matters, and a reduction in users’ feelings of worry and fear.
- (d)
- An increase in users’ feelings of being connected and mobile, and a reduction in the feelings of being isolated, disconnected, and immobile or ’trapped’.
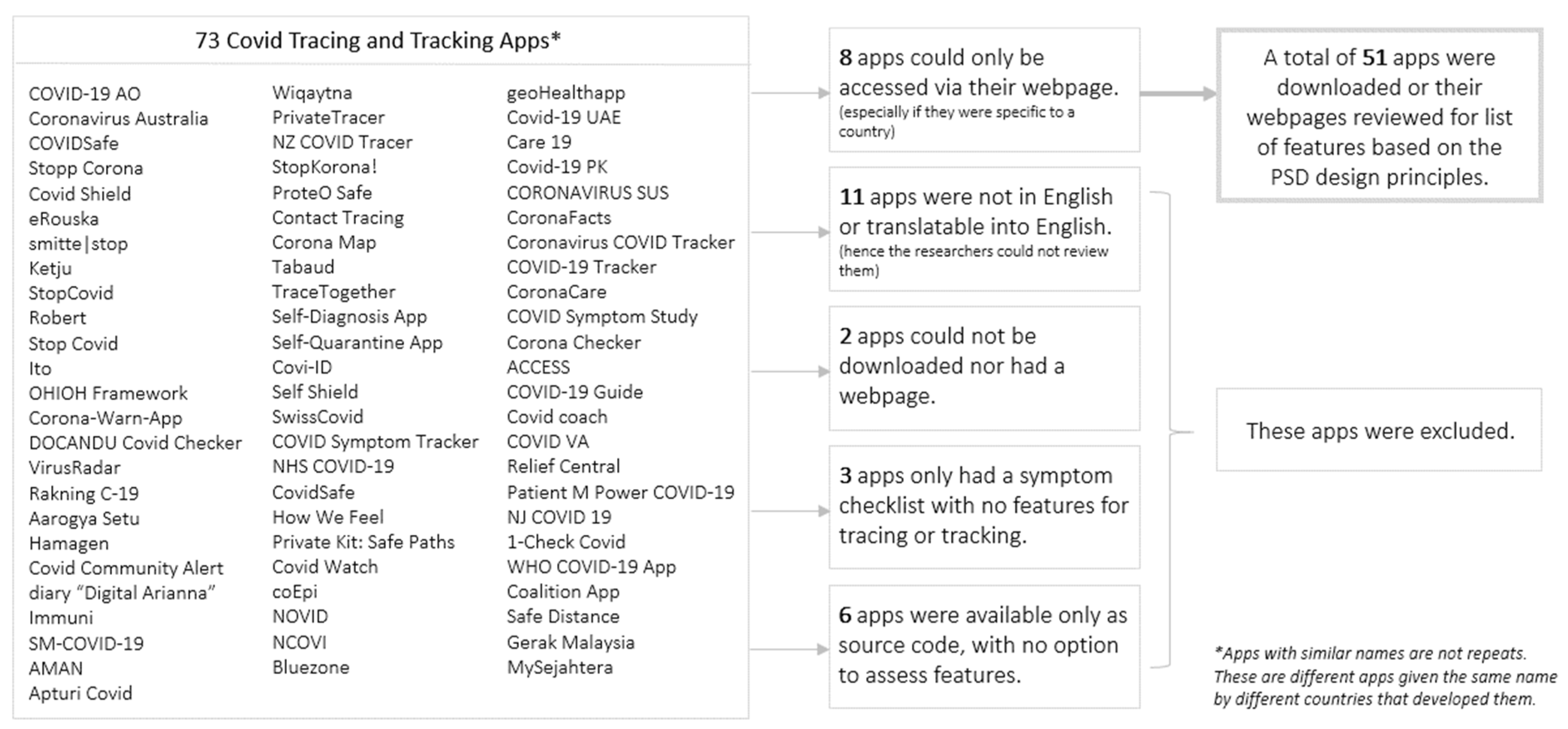
2.2. Literature Review for Extracting Successful PSD Feature Examples in COVID Apps
2.3. App Prototyping
2.4. Iterative User Testing
2.4.1. Participant Recruitment
2.4.2. Remote-Moderated Study Set Up and Testing Protocol
2.4.3. Pre-Test Questionnaires, Usability Evaluation Metrics, and Post-Test Questionnaires
3. Results
3.1. R-PSD Phase I: Establishing the Behavior of Interest, User Types (Their Goals or Use Cases), and Technology Medium for SafeTEI
- -
- Decreasing the behavioral tendency to make decisions based on guesses or hearsay, and increasing the reliance on credible facts;
- -
- Reducing users’ feelings of uncertainty about information needed for COVID-related decisions, and increasing their sense of being well-informed;
- -
- Decreasing feelings of worry and fear, and increasing feelings of comfort and confidence in making COVID-related decisions;
- -
- Reducing feelings of isolation and immobility and increasing users’ sense of connection and mobility.
3.2. R-PSD Phase II: Selecting the PSD Design Categories, and Persuasive Features from Successful Examples
- -
- Primary task support: providing users forms of behavior reduction, tunnelling, tailoring, personalization, and self-monitoring of COVID-related needs;
- -
- Dialog support: providing users with reminders, suggestions, and a social role to provide and obtain COVID-related support;
- -
- System credibility: providing users with affordances that promote trust, expertise, and credibility from relevant COVID-related information and resources;
- -
- Social support: providing users with a way to assess their behavior and outcomes related to COVID through features enabling comparison, cooperation, and inclusiveness.
3.3. R-PSD Phase III: Building the App Prototype for Behavior Persuasion Using Successful Examples
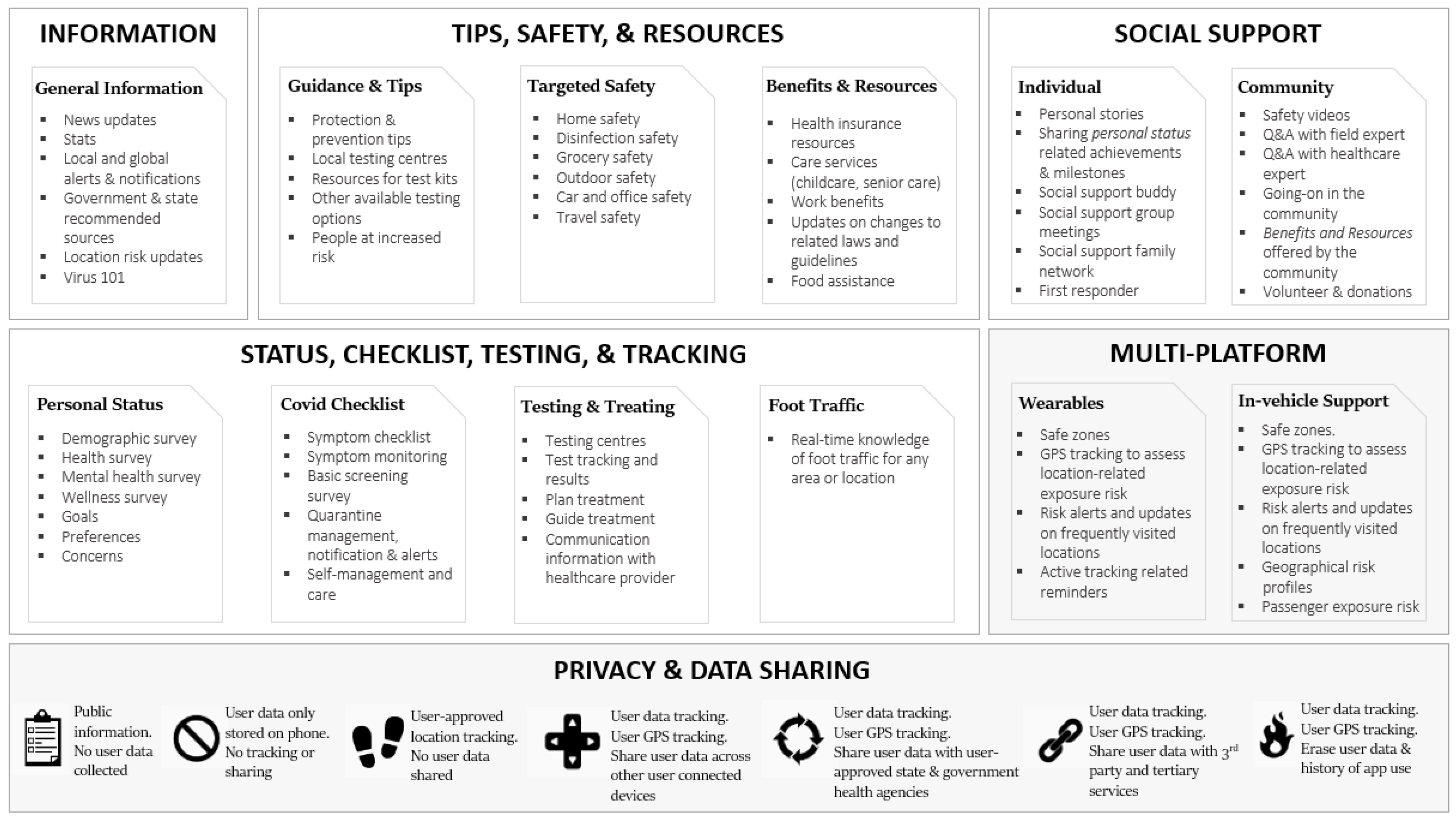
3.3.1. Prototyping SafeTEI
- -
- ‘COVID Rates and Policy Updates’, representing the information level with lowest data security and privacy concerns (Level 1);
- -
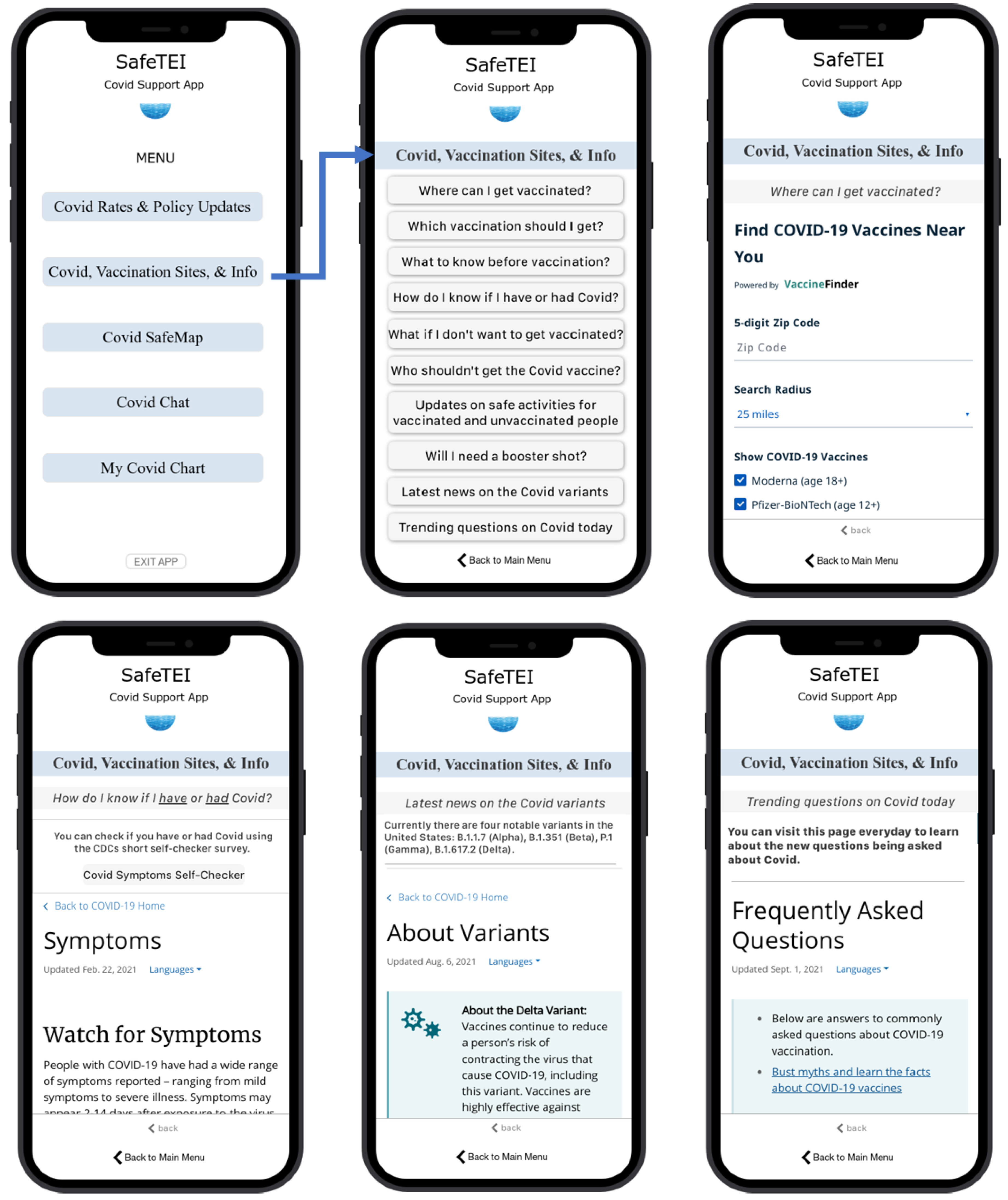
- ‘COVID, Vaccination Sites, and Info’, representing the tips, safety, and resources level with low data security and privacy concerns (Level 2);
- -
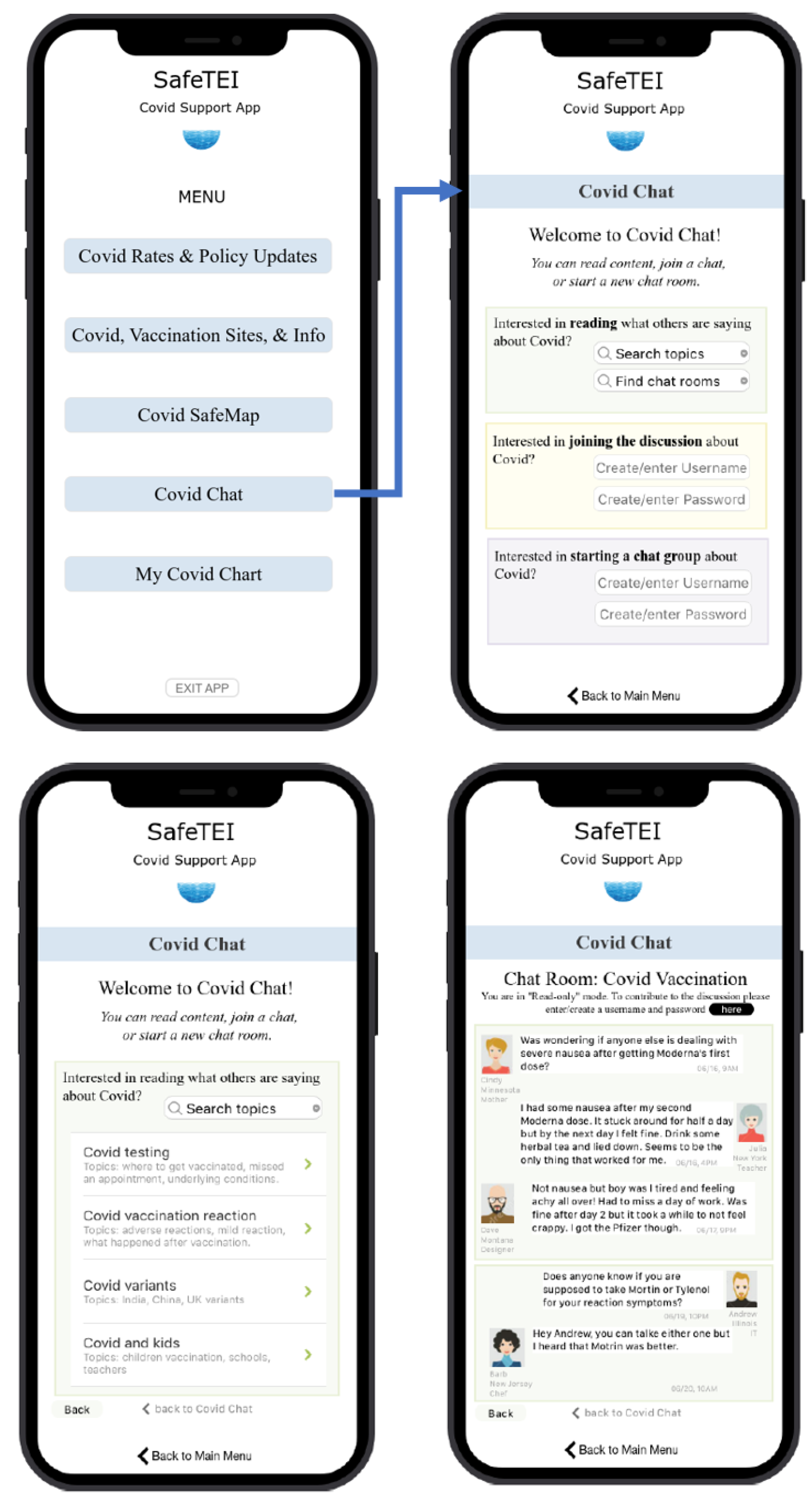
- ‘COVID Chat’, representing the social support level with medium to high data security and privacy concerns (Level 3);
- -
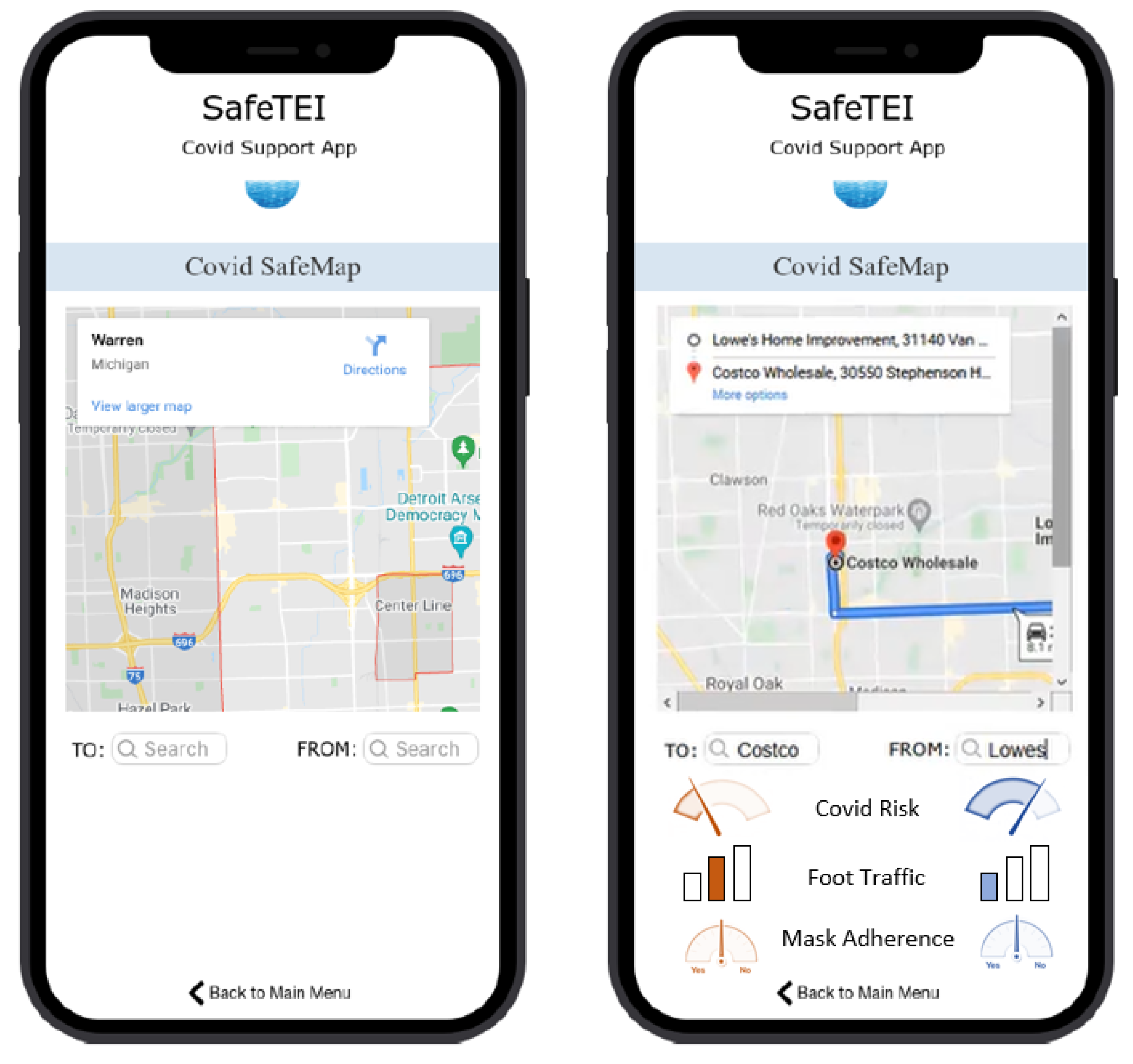
- ‘COVID SafeMap’ and ‘My COVID Chart’, representing the status, checklist, testing, and tracking level with highest data security and privacy concerns (Level 4).
Level 1: Prototyping the Information Layer
Level 2: Prototyping the Tips, Safety, and Resources Level for SafeTEI
Level 3: Prototyping the Social Support Level for SafeTEI
Level 4: Prototyping the Status, Checklist, Testing, and Tracking Level for SafeTEI
3.4. R-PSD Phase IV: Testing and Iterating the SafeTEI Prototype
3.4.1. Usability Inspection and Evaluation of SafeTEI
3.4.2. Small-Sample User Testing of SafeTEI
4. Discussion
- (a)
- The new R-PSD produced a usable and useful app.
- -
- SafeTEI was rated “easy to use” (low in difficulty). Mean rated usefulness was 5.9—above the midpoint of the scale, and mean rated learnability was 8.1 (out of 9).
- -
- SafeTEI was rated high for its information’s “usefulness”. (+Two ratings mapped to this, and the means were 6 and 8 (out of 9).
- -
- SafeTEI was rated high for providing the functions and information needed to be supportive for its purpose. This was evaluated with an open-ended question, and no additional functions, features, or types of information were identified by participants as “not provided”.
- (b)
- The R-PSD produced an app that precipitated changes in behavior that were established as goals in its usage context (Section 5.1):
- -
- SafeTEI decreased the behavioral tendency of users to make COVID decisions based on guesses or hearsay, and increased their reliance on credible facts;
- -
- SafeTEI decreased feelings of worry and fear, and increased their feelings of comfort and confidence in making COVID-related decisions;
- -
- Reduced customer fears of use (and increased users’ willingness-to-use a digital health app during a society-wide medical crisis);
- -
- SafeTEI improved user’s beliefs in—and ratings of—the credibility of the information made accessible by the app;
- -
- SafeTEI reduced users’ feelings of uncertainty about information needed for COVID-related decisions, and increased their sense of being well-informed;
- -
- SafeTEI reduced feelings of isolation and immobility and increased users’ sense of connection and mobility.
5. Conclusions
5.1. Implications and Applications
5.2. Impact Statement
- -
- The R-PSD can support development of future apps (and products) that are needed under time-pressure for community-level public health emergencies, including future pandemics;
- -
- The application of a process like this can help build a library of useful persuasive design principles and features, which could greatly facilitate more timely design and development in the future;
- -
- The ability to integrate more frequent remote usability testing leads to improved iterative testing speeds and efficiencies, and promises faster development processes in the future;
- -
- Including final phase large-sample testing (especially using field testing techniques) to formally evaluate the extent to which an app helps its users achieve targeted behavior change goals will begin to offer more definitive feedback on how behavior change can be facilitated and accomplished.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus disease 2019 (COVID-19). 2020. Available online: https://www.cdc.gov/covid/index.html (accessed on 12 May 2022).
- Ferguson, N.M.; Laydon, D.; Nedjati-Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunubá, Z.; Cuomo-Dannenburg, G.; et al. Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand; Imperial College COVID-19 Response Team: London, UK, 2020. [Google Scholar]
- Chowdhury, H.; Field, M.; Murphy, M. NHS Contact Tracing App: How Does It Work and When Can You Download It? The Telegraph: London, UK, 2020. [Google Scholar]
- Ferretti, L.; Wymant, C.; Kendall, M.; Zhao, L.; Nurtay, A.; Abeler-Dörner, L.; Fraser, C. Quantifying SARS-CoV-2 transmission suggests epidemic control with digital contact tracing. Science 2020, 368, eabb6936. [Google Scholar] [CrossRef]
- Pandit, J.A.; Radin, J.M.; Quer, G.; Topol, E.J. Smartphone apps in the COVID-19 pandemic. Nat. Biotechnol. 2022, 40, 1013–1022. [Google Scholar] [CrossRef]
- Cho, H.; Ippolito, D.; Yu, Y.W. Contact tracing mobile apps for COVID-19: Privacy considerations and related trade-offs. arXiv 2020, arXiv:2003.11511. [Google Scholar]
- Oxford University’s Big Data Institute. Digital Contact Tracing Can Slow or Even Stop Coronavirus Transmission and Ease Us Out of Lockdown. 2020. Available online: https://www.research.ox.ac.uk/article/2020-04-16-digital-contact-tracing-can-slow-or-even-stop-coronavirus-transmission-and-ease-us-out-of-lockdown (accessed on 12 May 2022).
- Abeler, J.; Altmann, S.; Milsom, L.; Toussaert, S.; Zillessen, H. Support in the UK for App-Based Contact Tracing of COVID-19; OSF. Io: Charlottesville, VA, USA, 2020. [Google Scholar]
- Ahmed, F.; Ahmed, N.E.; Pissarides, C.; Stiglitz, J. Why inequality could spread COVID-19. Lancet Public Health 2020, 5, 240. [Google Scholar] [CrossRef] [PubMed]
- Osmanlliu, E.; Rafie, E.; Bédard, S.; Paquette, J.; Gore, G.; Pomey, M.P. Considerations for the design and implementation of COVID-19 contact tracing apps: Scoping review. JMIR mHealth uHealth 2021, 9, e27102. [Google Scholar] [CrossRef]
- Gupta, A.; De Gasperis, T. Participatory Design to build better contact-and proximity-tracing apps. arXiv 2020, arXiv:2006.00432. [Google Scholar]
- Clemensen, J.; Rothmann, M.J.; Smith, A.C.; Caffery, L.J.; Danbjorg, D.B. Participatory design methods in telemedicine research. J. Telemed. Telecare 2017, 23, 780–785. [Google Scholar] [CrossRef]
- Pilemalm, S.; Timpka, T. Third generation participatory design in health informatics—Making user participation applicable to large-scale information system project. J. Biomed. Inform. 2008, 41, 327–339. [Google Scholar] [CrossRef]
- Hussain, Z.; Slany, W.; Holzinger, A. Current state of agile user-centered design: A survey. In HCI and Usability for E-Inclusion, Proceedings of the 5th Symposium of the Workgroup Human-Computer Interaction and Usability Engineering of the Austrian Computer Society, Linz, Austria, 9–10 November 2009; Springer: Berlin/Heidelberg, Germany, 2009; pp. 416–427. [Google Scholar]
- Thomas, S.A.; Bindu, V.R. Growth of agile software development methodologies in a web apps scenario. AIP Conf. Proc. 2022, 2520, 020006. [Google Scholar]
- Gefen, D.; Karahanna, E.; Straub, D.W. Trust and TAM in online shopping: An integrated model. MIS Q. 2003, 27, 51–90. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press: Florence, MA, USA, 2003. [Google Scholar]
- Deci, E.L.; Ryan, R.M. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol. Inq. 2000, 11, 227–268. [Google Scholar] [CrossRef]
- Lally, P.; van Jaarsveld, C.H.; Potts, H.W.; Wardle, J. How are habits formed: Modeling habit formation in the real world. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef]
- Cialdini, R.B. Influence: The Psychology of Persuasion; Harper Business: New York, NY, USA, 2006. [Google Scholar]
- Fogg, B.J. A behavior model for persuasive design. In Proceedings of the 4th International Conference on Persuasive Technology, Claremont, CA, USA, 26–29 April 2009; Association for Computing Machinery: New York, NY, USA, 2009; pp. 1–7. [Google Scholar]
- Orji, R.; Moffatt, K. Persuasive technology for health and wellness: State-of-the-art and emerging trends. Health Inform. J. 2018, 24, 66–91. [Google Scholar] [CrossRef] [PubMed]
- Oinas-Kukkonen, H.; Harjumaa, M. A systematic framework for designing and evaluating persuasive systems. In Proceedings of the International Conference on Persuasive Technology, Oulu, Finland, 4–6 June 2008; pp. 164–176. [Google Scholar]
- Fitzpatrick, K.K.; Darcy, A.; Vierhile, M. Delivering cognitive behavior therapy to young adults with symptoms of depression and anxiety using a fully automated conversational agent (Woebot): A randomized controlled trial. JMIR Ment. Health 2017, 4, e19. [Google Scholar] [CrossRef] [PubMed]
- Sepah, S.C.; Jiang, L.; Peters, A.L. Long-Term Outcomes of a Web-Based Diabetes Prevention Program: 2-Year Results of a Single-Arm Longitudinal Study. J. Med. Internet Res. 2015, 17, e92. [Google Scholar] [CrossRef]
- Meguro, T.; Takayama, F.; Hammarlund, H.; Honjo, M. Effects of a mobile health intervention on health-related outcomes in Japanese office workers: A pilot study. Int. J. Occup. Med. Environ. Health 2024, 37, 153–164. [Google Scholar] [CrossRef] [PubMed]
- McGowan, A.H.; Sittig, S.; Benton, R.; Bourrie, D.; Iyengar, S.; Dalogullari, A. Designing for diversity: Dynamic persuasive strategies in mHealth app development. In Proceedings of the 12th International Workshop on Behavior Change Support Systems, Wollongong, Australia, 10 April 2024. [Google Scholar]
- Ferreira, J.; Sharp, H.; Robinson, H. User Experience Design and Agile Development: Managing Cooperation through Articulation Work. Softw. Pract. Exp. 2011, 41, 963–974. [Google Scholar] [CrossRef]
- Gothelf, J. Lean UX: Applying Lean Principles to Improve User Experience; O’Reilly Media: Sevastopol, CA, USA, 2013. [Google Scholar]
- Garrett, J.J. The Elements of User Experience; Peachpit Press: Sacramento, CA, USA, 2003. [Google Scholar]
- Wikipedia. COVID-19 Apps. 23 April 2020. Available online: https://en.wikipedia.org/wiki/COVID-19_apps (accessed on 12 January 2022).
- Proto.io. Proto.io. 14 June 2020. Available online: Https://Proto.Io/ (accessed on 22 February 2022).
- Shi, J.; Danquah, S.K.N.; Dong, W. A Novel Block Chain Method for Urban Digitization Governance in Birth Registration Field: A Case Study. Int. J. Environ. Res. Public Health 2022, 19, 9309. [Google Scholar] [CrossRef]
- Our World in Data. 30 April 2020. Available online: https://ourworldindata.org/ (accessed on 12 May 2022).
- Lewis, J.R. Legitimate Use of Small Samples in Usability Studies: Three Examples; IBM Human Factors0, 20: Amonk City, NY, USA, 1991. [Google Scholar]
- Darviri, C.; Alexopoulos, E.C.; Artemiadis, A.K.; Tigani, X.; Kraniotou, C.; Darvyri, P.; Chrousos, G.P. The Healthy Lifestyle and Personal Control Questionnaire (HLPCQ): A novel tool for assessing self-empowerment through a constellation of daily activities. BMC Public Health 2014, 14, 995. [Google Scholar] [CrossRef]
- Reis, R.S.; Hino, A.A.; Añez, C.R. Perceived stress scale. J. Health Psychol. 2010, 15, 107–114. [Google Scholar] [CrossRef]
- Machleid, F.; Kaczmarczyk, R.; Johann, D.; Balčiūnas, J.; Atienza-Carbonell, B.; von Maltzahn, F.; Mosch, L. Perceptions of digital health education among European medical students: Mixed methods survey. J. Med. Internet Res. 2020, 22, e19827. [Google Scholar] [CrossRef]
- Hällgren, M.; Nygård, L.; Kottorp, A. Technology and everyday functioning in people with intellectual disabilities: A Rasch analysis of the Everyday Technology Use Questionnaire (ETUQ). J. Intellect. Disabil. Res. 2011, 55, 610–620. [Google Scholar] [CrossRef] [PubMed]
- ISO/IEC 9126-4; Software Product Quality—Part 4: Quality in Use Metrics. International Organization for Standardization: Geneva, Switzerland. Available online: https://www.iso.org/standard/35746.html (accessed on 4 April 2022).
- Chin, J.P.; Diehl, V.A.; Norman, K.L. Development of an instrument measuring user satisfaction of the human-computer interface. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Paris, France, 27 April–2 May 2013; pp. 213–218. [Google Scholar]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef]
- Lewis, J.R. Psychometric evaluation of the post-study system usability questionnaire: The PSSUQ. In Proceedings of the Human Factors Society Annual Meeting, Atlanta, GA, USA, 12–16 October 1992; pp. 1259–1260. [Google Scholar]
- Zhou, L.; Bao, J.; Setiawan, I.M.A.; Saptono, A.; Parmanto, B. The mHealth App Usability Questionnaire (MAUQ): Development and validation study. JMIR mHealth uHealth 2019, 7, e11500. [Google Scholar] [CrossRef] [PubMed]
- Schwarzer, R. Self-efficacy in the adoption and maintenance of health behaviors: Theoretcial approaches and a new mode. In Self-Efficacy: Thought Control of Action; Taylor & Francis: New York, NY, USA, 1992. [Google Scholar]
- Rhodes, R.E.; Dickau, L. Experimental evidence for the intention–behavior relationship in the physical activity domain: A meta-analysis. Health Psychol. 2012, 31, 724. [Google Scholar] [CrossRef] [PubMed]
- Sheeran, P. Intention—Behavior relations: A conceptual and empirical review. Eur. Rev. Soc. Psychol. 2002, 12, 1–36. [Google Scholar] [CrossRef]
- Dennison, L.; Morrison, L.; Conway, G.; Yardley, L. Opportunities and challenges for smartphone applications in supporting health behavior change: Qualitative study. J. Med. Internet Res. 2013, 15, e2583. [Google Scholar] [CrossRef]
- Kelders, S.M.; Kok, R.N.; Ossebaard, H.C.; Van Gemert-Pijnen, J.E. Persuasive system design does matter: A systematic review of adherence to web-based interventions. J. Med. Internet Res. 2012, 14, e152. [Google Scholar] [CrossRef]
- Lehto, T.; Oinas-Kukkonen, H. Examining the persuasive potential of web-based health behavior change support systems. AIS Trans. Hum.-Comput. Interact. 2015, 7, 126–140. [Google Scholar] [CrossRef]
- Hamari, J.; Koivisto, J. “Working out for likes”: An empirical study on social influence in exercise gamification. Comput. Hum. Behav. 2015, 50, 333–347. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Who Are They? | What Is a Key Goal for Them? | What Is Their Barrier to Achieving the Goal? | |
|---|---|---|---|
| User type 1 | Healthcare providers | Safety | Repeated exposure at work, protection of family and friends at home |
| User type 2 | Families with young children, or members with special needs | Up-to-date information | Applicability of information to kids of different ages and needs, school status, health check requirements |
| User type 3 | Those hesitant to get vaccinated | Credible stats on effectiveness and source of information | More evidence |
| User type 4 | Older adults | Mobility and access to what they need | Projected spread, lower immunity with age |
| Study Steps (Step-by-Step) | Estimated Completion Time |
|---|---|
| Welcome and consent forms | 10 min |
| Pre-test questionnaires | 20 min |
| App orientation session | 20 min |
| User testing | 40 min |
| Post-test questionnaires | 20 min |
| Debrief and session close | 10 min |
| Order | Scenario Context | Task |
|---|---|---|
| 0 | Initial explanation to set the stage: Please imagine that I am a friend of yours who needs some assistance dealing with COVID -related issues—and I’ve come to you for help with them. I would like you to use the COVID app to help me find the information that I need. So, I will be asking you to do some tasks using the new COVID app. | Reminders for participant after each task: Say “Done!” (when the task is finished.) Go back to the HOME page of the app. |
| 1 | I received my vaccinations very early—last January/February. I am wondering if I will need to get a booster shot—or if I even can. So, the task that I need help with is this: | To look for news about COVID vaccination boosters. Please begin now. |
| 2 | I want to be certain that I limit my exposure to COVID and its variants in the community. I have been wondering what activities are safe for me to do? I need some help finding out about this. So, the task that I need help with is this: | To look for activities that are safe for vaccinated people to do. Please begin now. |
| 3 | I am concerned about this new COVID variant that is affecting people now. And I need some help finding out about COVID testing rates. So, the task that I need help with is this: | Look for COVID test rates. Please begin now. |
| 4 | Okay, my family is planning a trip to California to visit our relatives, and we are wondering what we need to be prepared for as we travel. So, the task that I need help with is this: | Find the latest COVID travel restrictions to California. Please begin now. |
| 5 | Since I live in Michigan, I would really like to stay up-to-date on the resources that are available on COVID. So, the task that I need help with is this: | Find the latest COVID resources in Michigan. Please begin now. |
| 6 | My cousin lives in another state and she does not want to get vaccinated. I would really like to help her identify what she should do. So, the task that I need help with is this: | Find information on what someone should do if they don’t want to get vaccinated. Please begin now. |
| 7 | One of my close family members is pregnant and needs to find a vaccination site. She lives near your location—and her doctor has advised her to receive the Moderna vaccine. I would really like to help her find a nearby site to get the Moderna vaccine. So, the task that I need help with is this: | Find a COVID vaccination site near you for Moderna vaccines. Please begin now. |
| 8 | One of my teenagers is out running errands for me. He needs to drive from Lowes to Costco and I would really like to help him find a route to Costco that goes through a COVID -safe area where there’s a low risk of being exposed to COVID. I want him to stay healthy for school. So, the task that I need help with is this: | Use your COVID Safe Map to find a travel route from Lowes to Costco. Please begin now. |
| 9 | I’ve been hearing that there is some new information that is emerging in the online chat rooms related to COVID vaccines for kids. And I would like to find out about it. So, the task that I need help with is this: | Use your COVID Safe Map to find a travel route from Lowes to Costco. Please begin now. |
| 10 | I’ve been told that it is possible for me to enter my side-effects from the COVID vaccination into a central survey form. But I don’t where to do that, or how to do that. I wonder if you could help me out by showing me this and entering your own side effects (or you could enter some sample ones). So, the task that I need help with is this: | Use “My COVID Chart” to show how to take a survey of COVID vaccination side-effects. Please begin now. |
| Pre-Test | ||||
|---|---|---|---|---|
| Questionnaire | Total survey items within the questionnaire | |||
| Health Lifestyle and Personal Control (HLPCQ) | 26 | |||
| Perceived Stress Scale (PSS) | 10 | |||
| Use and Opinion of Digital Health | 5 | |||
| Technology Use | 4 | |||
| During-test: Quantitative measures | ||||
| Measure | Description | Unit of observation | ||
| Task completion | Each task is considered complete when the participant indicates that the scenario goal has been obtained (whether successfully or unsuccessfully), or the participant requested and received sufficient guidance as to warrant scoring the scenario as a critical error. | Binary (0 = no, 1 = yes) | ||
| Critical errors | When conducting a task, critical errors represent deviations from completion of the goals targeted by the task, or If a participant required assistance in order to achieve a correct output. Participants may or may not be aware that the task goal was incorrect or incomplete. | Count | ||
| Non-critical errors | When conducting a task, non-critical errors represent those errors that the participant recovered from, or, if not detected, did not result in deviation from the task goal or unexpected results. | Count | ||
| Completion rate | Completion rate represents the percentage of participants who successfully completed the task without critical errors. A completion rate of 100% was the goal for each task in this usability test. | Percentage | ||
| Error-free rate | Error-free rate is the percentage of participants who completed the task without any critical or non-critical errors. An error-free rate of 80% was the goal for each task in this usability test. | Percentage | ||
| Time on Task (TOT) | Time on Task (TOT) is the time to complete a task, measured from the time the participant begins the task to the time they signal completion (by saying ‘done’ in this usability testing). | Seconds | ||
| (task) difficulty rating | Rating of the usability test task on a scale of 1 to 9, where 1 represents low difficulty and 9 represents extreme difficulty. | Likert scale | ||
| (information) usefulness rating | Rating of the usability test task on a scale of 1 to 9, where 1 represents low usefulness of the information presented on the app page for the task, and 9 represents high usefulness of the information presented on the app page for the task. | Likert scale | ||
| During-test: Qualitative measures | ||||
| Measure | Description | Unit of observation | ||
| Think-Aloud | Recording user’s verbal statements as they work through each task to capture relevant information and context. | - | ||
| At the end of each task, participants were asked: ‘Do you have any additional comments or feedback about the task you just completed?’ | Recording user’s verbal responses after task completion. | - | ||
| Post-Test | ||||
| Questionnaire | Total survey items within the questionnaire | |||
| User Interface Satisfaction | 27 | |||
| Perceived Usefulness and Ease of Use | 12 | |||
| Post-Study System Usability Questionnaire (PSSUQ) | 16 | |||
| mHealth App Usability Questionnaire (MAUQ) | 21 | |||
| Ketju | Diary ‘Digital Arianna’ | Virus Radar | Trace Together | Corono Virus Australia | Stop COVID | NZ COVID Tracer | Blue Zone | Smitte|Stop | COVID Coach | |
|---|---|---|---|---|---|---|---|---|---|---|
| Primary Task Support | ||||||||||
| Reduction | ● | |||||||||
| Tunnelling | ● | ● | ● | ● | ● | |||||
| Tailoring | ● | ● | ● | |||||||
| Personalization | ● | |||||||||
| Self-monitoring | ● | ● | ● | ● | ● | |||||
| Simulation | ||||||||||
| Rehearsal | ||||||||||
| Optimality | ||||||||||
| Dialog Support | ||||||||||
| Praise | ||||||||||
| Rewards | ● | |||||||||
| Reminders | ● | |||||||||
| Suggestions | ● | ● | ● | |||||||
| Similarity | ||||||||||
| Liking | ● | |||||||||
| Social role | ● | ● | ||||||||
| User control and freedom | ● | |||||||||
| Flexibility | ● | |||||||||
| Emotion | ||||||||||
| Perceptible information | ● | ● | ||||||||
| System Credibility Support | ||||||||||
| Trust | ● | ● | ● | |||||||
| Expertise | ● | ● | ||||||||
| Credibility | ● | ● | ● | ● | ● | |||||
| Real-world feel | ● | ● | ● | ● | ● | |||||
| Authority | ● | ● | ● | ● | ||||||
| 3rd party | ||||||||||
| Verifiable | ● | ● | ||||||||
| Equitable | ● | ● | ● | ● | ||||||
| Transparency | ● | ● | ● | ● | ||||||
| Privacy | ● | ● | ● | ● | ● | ● | ||||
| Social Support | ||||||||||
| Learning | ● | |||||||||
| Comparison | ||||||||||
| Influence | ● | |||||||||
| Facilitation | ||||||||||
| Cooperation | ||||||||||
| Competition | ||||||||||
| Recognition | ||||||||||
| Inclusiveness | ||||||||||
| Top Fitness Apps (n = 17) | Top mHealth Apps (n = 23) | Top Health and Fitness Apps (n = 10) | |
|---|---|---|---|
| Dialog Support features | |||
| Activity type | 17 | 23 | 10 |
| Activity duration | 17 | 16 | 8 |
| Activity frequency | 17 | 22 | 10 |
| Activity recommendations | 17 | 22 | 10 |
| Activity knowledge and information | 15 | 19 | 10 |
| Activity scoring | 5 | 8 | 10 |
| Activity challenges | 11 | 11 | 10 |
| Reminders | 15 | 17 | 5 |
| Progress charts | 17 | 23 | 10 |
| Goal setting | 9 | 9 | 5 |
| Success/celebration | 17 | 18 | 5 |
| Social Support features | |||
| Friend circle | 4 | 3 | 1 |
| Score comparison | 5 | 3 | 2 |
| Social motivation | 3 | 3 | 2 |
| Multi-platform capabilities | |||
| Smartwatch | 5 | 7 | 2 |
| Web-based | 17 | 23 | 8 |
| Mobile phone | 17 | 23 | 10 |
| User Type | Families with Vulnerable Members | Older Adult | Healthcare Provider | Middle-Aged Adult |
|---|---|---|---|---|
| Demographics | ||||
| Age group (yrs.) | 35–44 | 65+ | 25–34 | 45–55 |
| Gender | Female | Female | Female | Female |
| Health Lifestyle and Personal Control Questionnaire (pre-test survey) | ||||
| Open-ended response to During COVID, have you noticed any changes concerning your everyday living/lifestyle? | Yes, fewer healthy habits and more isolations from outdoor activities | positive changes as related to paying more to my health and the health of others | Daily life is much more hectic. I don’t have much of a routine. Sleep is often interrupted. I’m indoors far more despite my state being “open”. | Yes. I limit interactions with outside people more than I used to. |
| Perceived Stress Scale Questionnaire (pre-test survey) | ||||
| Stress ratings during COVID Scale: Never (0)—very often (4) | 3.1 | 3.2 | 3.2 | 2.6 |
| Open-ended response to have you noticed any changes concerning your stress? | my current stress levels are higher now | One approach I utlized to controlling my stress was to limit watching the news | Stress increased significantly after having a baby in the midst of a pandemic. Anxiety also increased. So did my prozac prescription. | no |
| Small-sample usability testing (rating and participant feedback during-test) | ||||
| App information usefulness Scale: Less (1)—extremely useful (9) | 4.2 | 4.3 | 7.9 | 7.2 |
| Useful app features | - Having a map that informs you of destination covid status is useful | - Having all the relevant information in one spot | - Infographics useful and easy to read - COVID vaccination and COVID side effects tracker in one spot was very useful to have as a feature | - Having a map that informs you of destination covid status is useful |
| Design or information gaps in the app | - Menu item labels were confusing - Simple data points vs. charts or graphs preferred - More localized information at the county level - Do not find chat groups useful | - Menu item labels were confusing - Information is hard to find on charts - Font size is small | - Font size is small - Information is hard to find on charts - Search boxes were not intuitive for typing | - Font size is small |
| System Usability Scale Questionnaire (post-test survey) | ||||
| Screen satisfaction | 6.5 | 5.8 | 6.0 | 5.5 |
| Learnability | 6.7 | 8.3 | 9.1 | 8.9 |
| Perceived usefulness | 6.2 | 7.6 | 9.2 | 9 |
| Usability | 3 | 4.6 | 4.1 | 5.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Payyanadan, R.P.; Angell, L.S.; Zeidan, A. A COVID Support App Demonstrating the Use of a Rapid Persuasive System Design Approach. Information 2025, 16, 360. https://doi.org/10.3390/info16050360
Payyanadan RP, Angell LS, Zeidan A. A COVID Support App Demonstrating the Use of a Rapid Persuasive System Design Approach. Information. 2025; 16(5):360. https://doi.org/10.3390/info16050360
Chicago/Turabian StylePayyanadan, Rashmi P., Linda S. Angell, and Amanda Zeidan. 2025. "A COVID Support App Demonstrating the Use of a Rapid Persuasive System Design Approach" Information 16, no. 5: 360. https://doi.org/10.3390/info16050360
APA StylePayyanadan, R. P., Angell, L. S., & Zeidan, A. (2025). A COVID Support App Demonstrating the Use of a Rapid Persuasive System Design Approach. Information, 16(5), 360. https://doi.org/10.3390/info16050360