
Intelligence Amplification-Based Smart Health Record Chain for Enterprise Management System

 ,
,  ,
,  ,
,  and
and
Abstract
1. Introduction
Motivations
- The adoption of blockchain technology in healthcare can be challenging due to the varied approaches of different institutions such as healthcare providers and insurance payers. Without a streamlined method such as a single-payer system, getting these organizations to adopt blockchain technology can be difficult, which can reduce the effectiveness of the entire system.
- Hospitals and insurance companies may intentionally avoid sharing data due to the competitive advantage of confidentiality. Data sharing between these entities can be challenging, which can hinder the implementation of blockchain technology in healthcare.
- The lack of effort and awareness of blockchain technology among those outside of information technology can be a barrier to its adoption, and even financial incentives may not be enough to address this issue.
- Health record chain is a permissioned blockchain technology that allows data sharing while maintaining anonymity. A modified SHA-512 algorithm was used to create new block structures that give a complete medical history for each patient while maintaining data integrity.
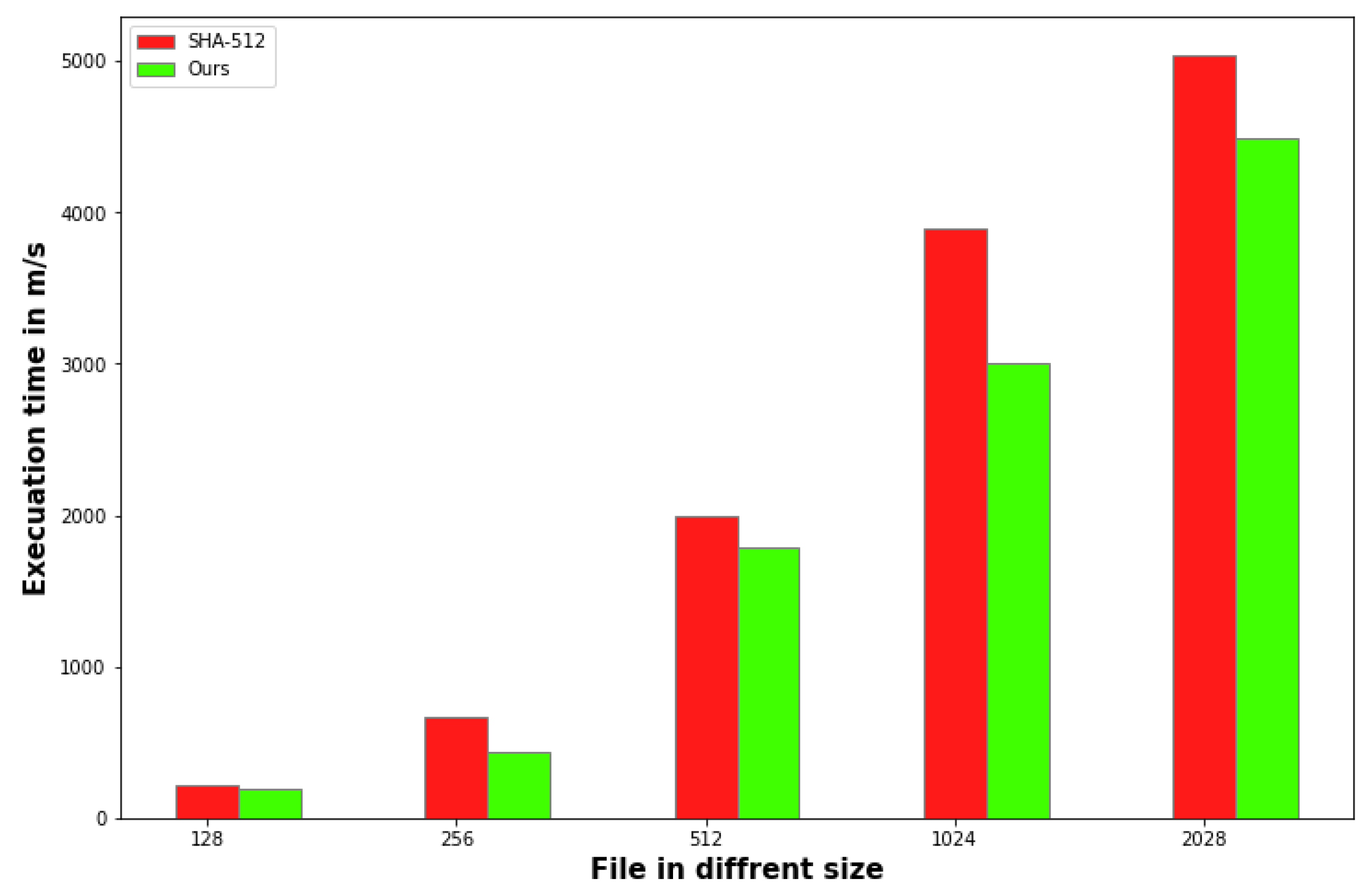
- A modified hash algorithm was designed to improve execution speed while keeping the SHA-512 structure.
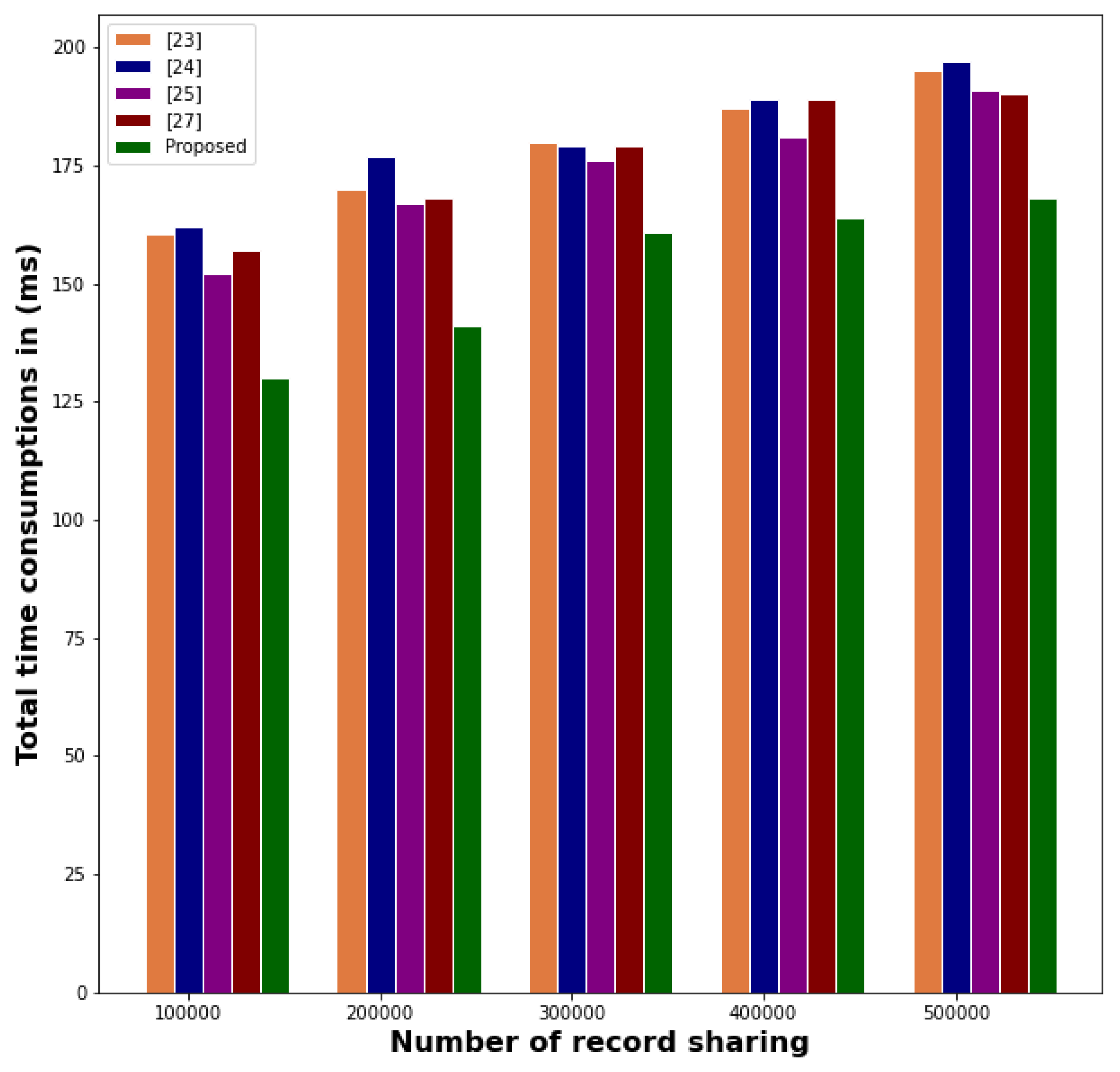
- The proposed solution was evaluated against state-of-the-art medical data-sharing methods using blockchain technology to assess its efficacy.
2. Related Works
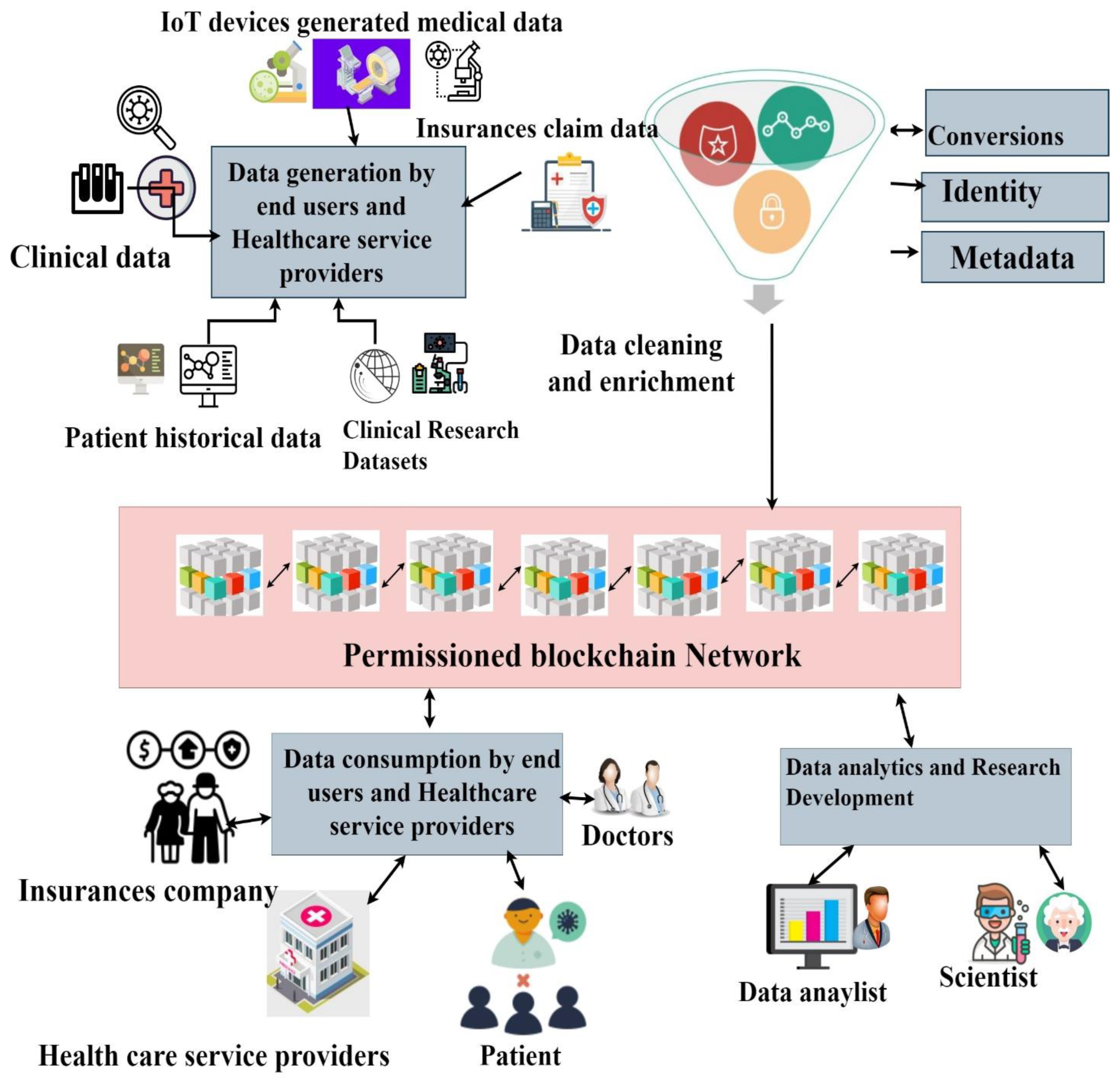
3. Proposed Methodology
3.1. Data Generations
3.2. Data Cleaning
3.3. Construction of Permissioned Blockchain Network
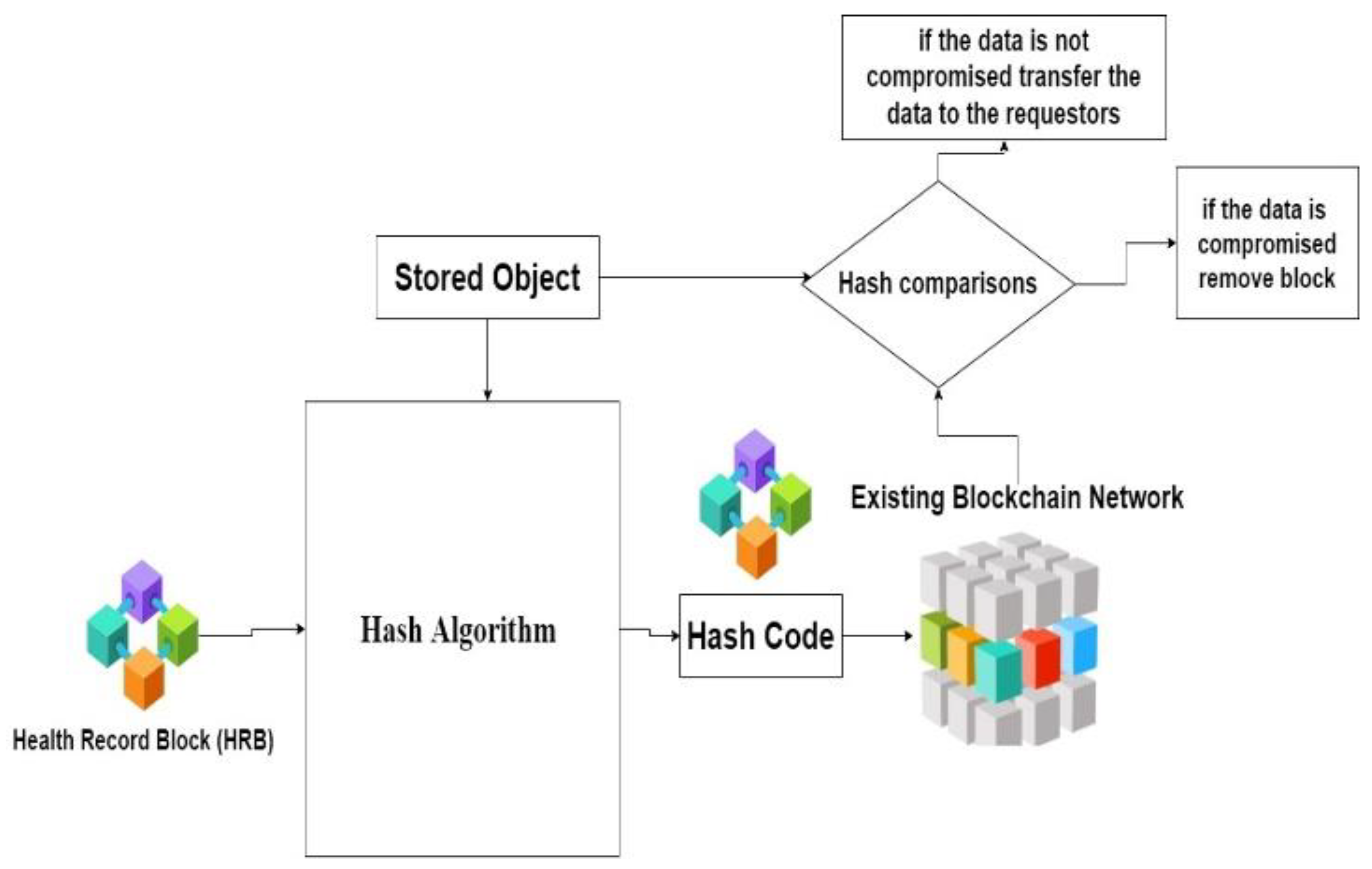
3.4. Hash Value Generations
3.5. Hash Code Algorithm
- Initialize the Initialize hash value
- 2.
- Process the Health Record Block (HRB)
- 2.1.
- Prepare the message schedule S
- 2.2.
- Initialize the intermediate buffer
- 2.3.
- Hash Code Computations
- 2.4.
- Compute the intermediate Hash value
- Return (hN,0|| hN,1|| hN,2||………………. hN,15)
3.6. Data Consumption Using Smart Contract
4. Experiments
4.1. Experimental Setup
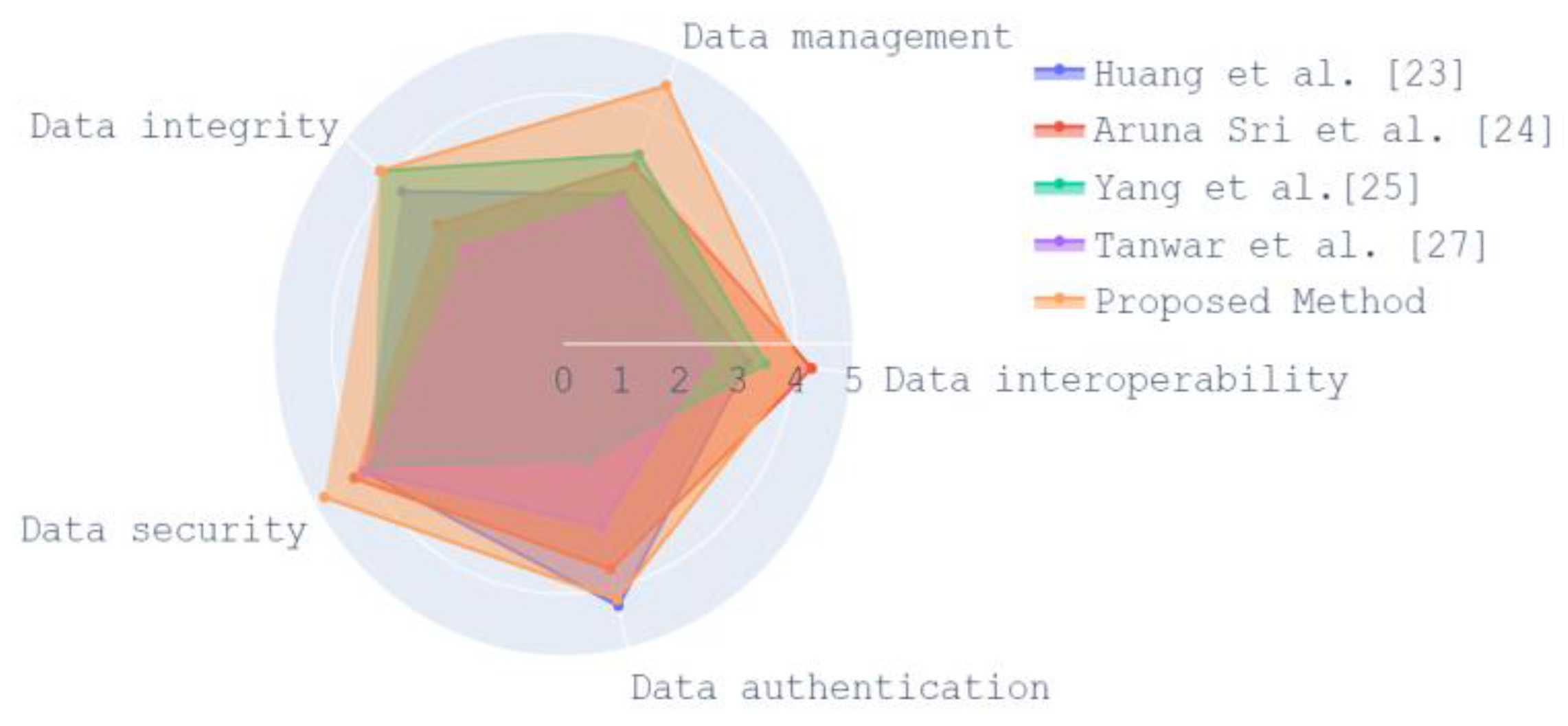
4.2. Result Discussion
4.3. Security Investigation of the Proposed Model
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Guo, R.; Shi, H.; Zhao, Q.; Zheng, D. Secure Attribute-Based Signature Scheme with Multiple Authorities for Blockchain in Electronic Health Records Systems. IEEE Access 2018, 6, 11676–11686. [Google Scholar] [CrossRef]
- Jabarulla, M.Y.; Lee, H.-N. A blockchain and artificial intelligence-based, patient-centric healthcare system for combating the COVID-19 pandemic: Opportunities and applications. Healthcare 2021, 9, 1019. [Google Scholar] [CrossRef] [PubMed]
- Ndzimakhwe, M.; Telukdarie, A.; Munien, I.; Vermeulen, A.; Chude-Okonkwo, U.K.; Philbin, S.P. A Framework for User-Focused Electronic Health Record System Leveraging Hyperledger Fabric. Information 2023, 14, 51. [Google Scholar] [CrossRef]
- Kumar, A.; Parihar, A.; Panda, U.; Parihar, D.S. Microfluidics-based point-of-care testing (POCT) devices in dealing with waves of COVID-19 pandemic: The emerging solution. ACS Appl. Bio Mater. 2022, 5, 2046–2068. [Google Scholar] [CrossRef]
- Reen, G.S.; Mohandas, M.; Venkatesan, S. Decentralized patient-centric e-Health record management system using blockchain and IPFS. In Proceedings of the 2019 IEEE Conference on Information and Communication Technology, CICT 2019, Allahabad, India, 6–8 December 2019; pp. 1–7. [Google Scholar] [CrossRef]
- Shi, S.; He, D.; Li, L.; Kumar, N.; Khan, M.K.; Choo, K.-K.R. Applications of blockchain in ensuring the security and privacy of electronic health record systems: A survey. Comput. Secur. 2020, 97, 101966. [Google Scholar] [CrossRef]
- Zou, R.; Lv, X.; Zhao, J. SPChain: Blockchain-based medical data sharing and privacy-preserving eHealth system. Inf. Process. Manag. 2021, 58, 102604. [Google Scholar] [CrossRef]
- Guimarães, T.; Silva, H.; Peixoto, H.; Santos, M. Modular Blockchain Implementation in Intensive Medicine. Procedia Comput. Sci. 2020, 170, 1059–1064. [Google Scholar] [CrossRef]
- Harshini, V.M.; Danai, S.; Usha, H.R.; Kounte, M.R. Health record management through blockchain technology. In Proceedings of the 2019 3rd ACM International Conference on Trends in Electronics and Informatics (ICOEI), Tirunelveli, India, 23–25 April 2019; pp. 1411–1415. [Google Scholar] [CrossRef]
- Alexaki, S.; Alexandris, G.; Katos, V.; Petroulakis, N.E. Blockchain-based Electronic Patient Records for Regulated Circular Healthcare Jurisdictions. In Proceedings of the 2018 IEEE 23rd International Workshop on Computer Aided Modeling and Design of Communication Links and Networks (CAMAD), Barcelona, Spain, 17–19 September 2018; pp. 1–6. [Google Scholar] [CrossRef]
- Wang, S.; Zhang, D.; Zhang, Y. Blockchain-Based Personal Health Records Sharing Scheme with Data Integrity Verifiable. IEEE Access 2019, 7, 102887–102901. [Google Scholar] [CrossRef]
- Vazirani, A.A.; O’donoghue, O.; Brindley, D.; Meinert, E. Blockchain vehicles for efficient Medical Record management. Npj Digit. Med. 2020, 3, 1–5. [Google Scholar] [CrossRef]
- Rahman, M.S.; Khalil, I.; Arachchige, P.C.M.; Bouras, A.; Yi, X. A novel architecture for tamper proof electronic health record management system using blockchain wrapper. In Proceedings of the 2019 ACM International Symposium on Blockchain and Secure Critical Infrastructure BSCI, Co-Located with AsiaCCS 2019, New York, NY, USA, 8 July 2019; pp. 97–105. [Google Scholar] [CrossRef]
- Wang, J.; Han, K.; Alexandridis, A.; Chen, Z.; Zilic, Z.; Pang, Y.; Jeon, G.; Piccialli, F. A blockchain-based eHealthcare system interoperating with WBANs. Futur. Gener. Comput. Syst. 2020, 110, 675–685. [Google Scholar] [CrossRef]
- Wang, S.; Wang, J.; Wang, X.; Qiu, T.; Yuan, Y.; Ouyang, L.; Guo, Y.; Wang, F.-Y. Blockchain-Powered Parallel Healthcare Systems Based on the ACP Approach. IEEE Trans. Comput. Soc. Syst. 2018, 5, 942–950. [Google Scholar] [CrossRef]
- Wang, Z.; Luo, N.; Zhou, P. GuardHealth: Blockchain empowered secure data management and Graph Convolutional Network-enabled anomaly detection in smart healthcare. J. Parallel Distrib. Comput. 2020, 142, 1–12. [Google Scholar] [CrossRef]
- Zhao, H.; Bai, P.; Peng, Y.; Xu, R. Efficient key management scheme for health blockchain. CAAI Trans. Intell. Technol. 2018, 3, 114–118. [Google Scholar] [CrossRef]
- Shamshad, S.; Minahil; Mahmood, K.; Kumari, S.; Chen, C.-M. A secure blockchain-based e-health records storage and sharing scheme. J. Inf. Secur. Appl. 2020, 55, 102590. [Google Scholar] [CrossRef]
- Rajput, A.R.; Li, Q.; Ahvanooey, M.T.; Masood, I. EACMS: Emergency Access Control Management System for Personal Health Record Based on Blockchain. IEEE Access 2019, 7, 84304–84317. [Google Scholar] [CrossRef]
- Xu, J.; Xue, K.; Li, S.; Tian, H.; Hong, J.; Hong, P.; Yu, N. Healthchain: A Blockchain-Based Privacy Preserving Scheme for Large-Scale Health Data. IEEE Internet Things J. 2019, 6, 8770–8781. [Google Scholar] [CrossRef]
- Chen, L.; Lee, W.-K.; Chang, C.-C.; Choo, K.-K.R.; Zhang, N. Blockchain based searchable encryption for electronic health record sharing. Futur. Gener. Comput. Syst. 2019, 95, 420–429. [Google Scholar] [CrossRef]
- Dagher, G.G.; Mohler, J.; Milojkovic, M.; Marella, P.B. Ancile: Privacy-preserving framework for access control and interoperability of electronic health records using blockchain technology. Sustain. Cities Soc. 2018, 39, 283–297. [Google Scholar] [CrossRef]
- Huang, J.; Qi, Y.W.; Asghar, M.R.; Meads, A.; Tu, Y.-C. MedBloc: A blockchain-based secure EHR system for sharing and accessing medical data. In Proceedings of the 2019 18th IEEE International Conference On Trust, Security And Privacy In Computing And Communications/13th IEEE International Conference On Big Data Science And Engineering (TrustCom/BigDataSE), Rotorua, New Zealand, 5–8 August 2019; pp. 594–601. [Google Scholar] [CrossRef]
- Aruna Sri, P.A.; Bhaskari, D.L. Blockchain technology for secure medical data sharing using consensus mechanism. Mater. Today Proc. 2020. [Google Scholar] [CrossRef]
- Yang, J.-J.; Li, J.-Q.; Niu, Y. A hybrid solution for privacy preserving medical data sharing in the cloud environment. Futur. Gener. Comput. Syst. 2015, 43, 74–86. [Google Scholar] [CrossRef]
- Roehrs, A.; da Costa, C.A.; da Rosa Righi, R.; da Silva, V.F.; Goldim, J.R.; Schmidt, D.C. Analyzing the performance of a blockchain-based personal health record implementation. J. Biomed. Inform. 2019, 92, 103140. [Google Scholar] [CrossRef] [PubMed]
- Tanwar, S.; Parekh, K.; Evans, R. Blockchain-based electronic healthcare record system for healthcare 4.0 applications. J. Inf. Secur. Appl. 2020, 50, 102407. [Google Scholar] [CrossRef]
- Sreenu, M.; Gupta, N.; Jatoth, C.; Saad, A.; Alharbi, A.; Nkenyereye, L. Blockchain based secure and reliable Cyber Physical ecosystem for vaccine supply chain. Comput. Commun. 2022, 191, 173–183. [Google Scholar] [CrossRef]
- Butt, G.Q.; Sayed, T.A.; Riaz, R.; Rizvi, S.S.; Paul, A. Secure healthcare record sharing mechanism with blockchain. Appl. Sci. 2022, 12, 2307. [Google Scholar] [CrossRef]












| S. No | User | Permission |
|---|---|---|
| 1 | Doctors or healthcare service providers |
|
| 2 | Patient |
|
| 3 | Insurances service providers |
|
| 4 | Research institution |
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velliangiri, S.; Karthikeyan, P.; Ravi, V.; Almeshari, M.; Alzamil, Y. Intelligence Amplification-Based Smart Health Record Chain for Enterprise Management System. Information 2023, 14, 284. https://doi.org/10.3390/info14050284
Velliangiri S, Karthikeyan P, Ravi V, Almeshari M, Alzamil Y. Intelligence Amplification-Based Smart Health Record Chain for Enterprise Management System. Information. 2023; 14(5):284. https://doi.org/10.3390/info14050284
Chicago/Turabian StyleVelliangiri, S., P. Karthikeyan, Vinayakumar Ravi, Meshari Almeshari, and Yasser Alzamil. 2023. "Intelligence Amplification-Based Smart Health Record Chain for Enterprise Management System" Information 14, no. 5: 284. https://doi.org/10.3390/info14050284
APA StyleVelliangiri, S., Karthikeyan, P., Ravi, V., Almeshari, M., & Alzamil, Y. (2023). Intelligence Amplification-Based Smart Health Record Chain for Enterprise Management System. Information, 14(5), 284. https://doi.org/10.3390/info14050284