
Evaluation of Everyday Living Areas for Deinstitutionalized Community-Living People with Mental Illness
Abstract
1. Introduction
2. Materials and Methods
2.1. Target Area
2.2. Data Collection
2.3. Analysis Methods
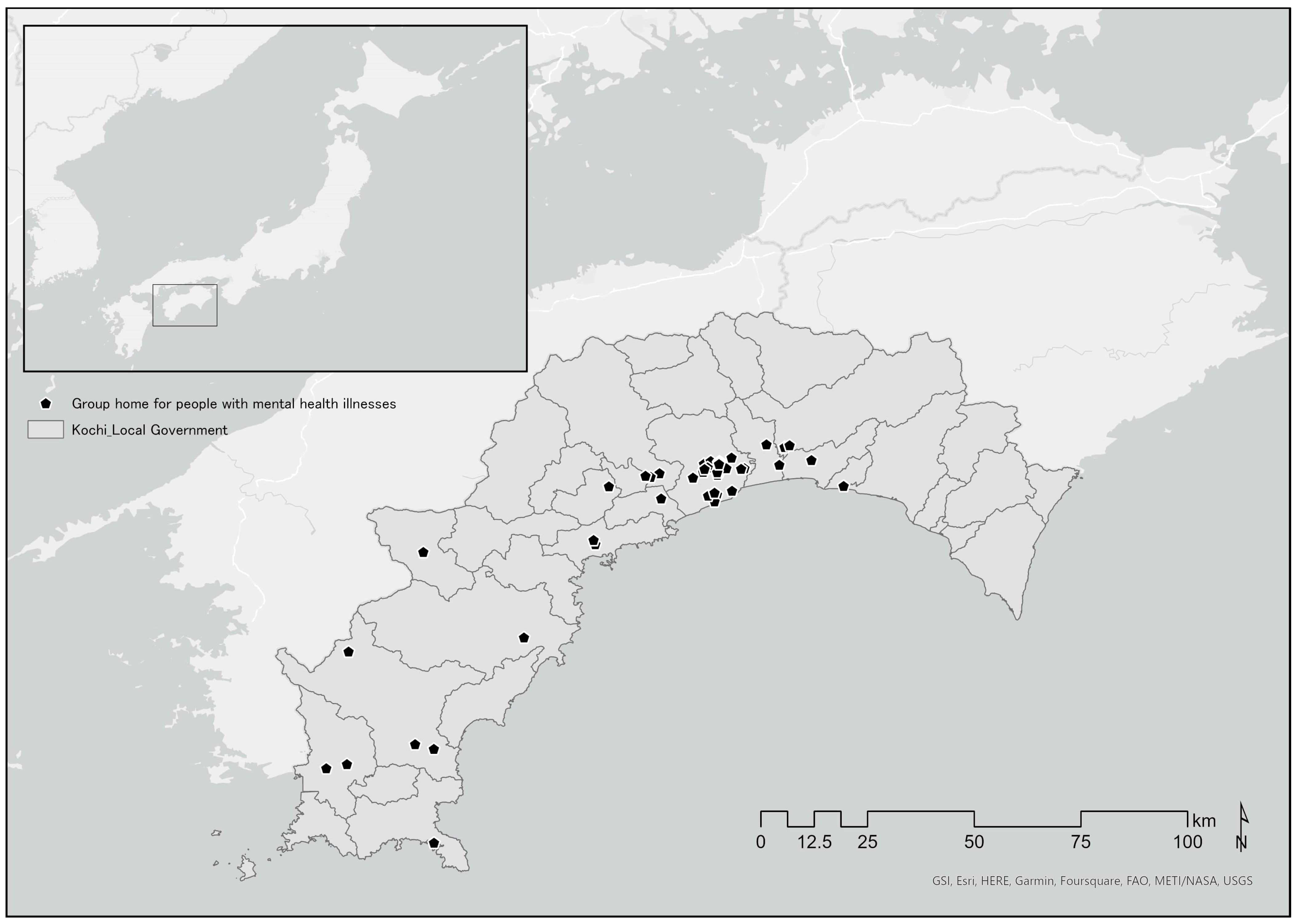
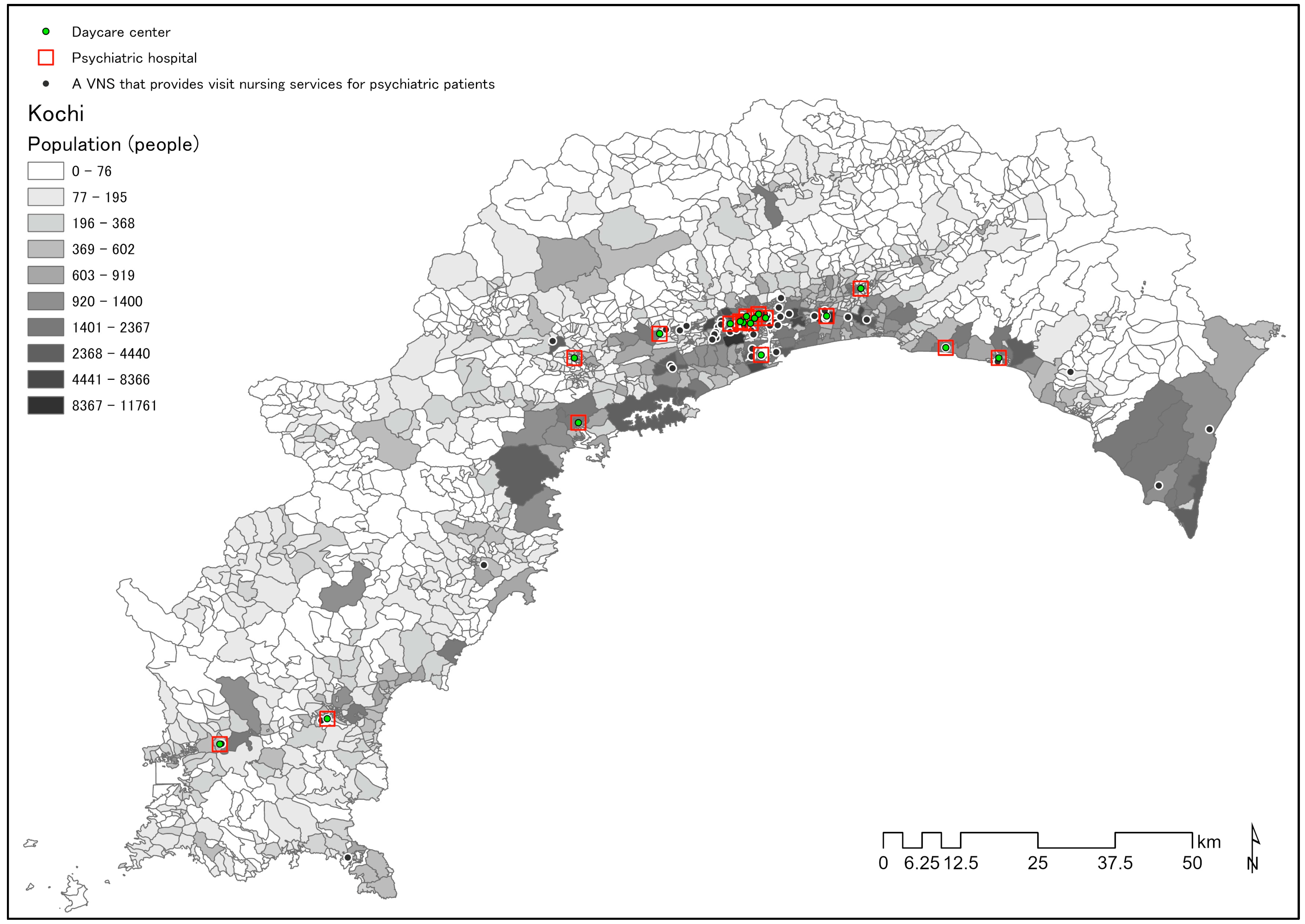
2.3.1. Distribution of GHs, VNSs, PHs, DCs, and SCEBs
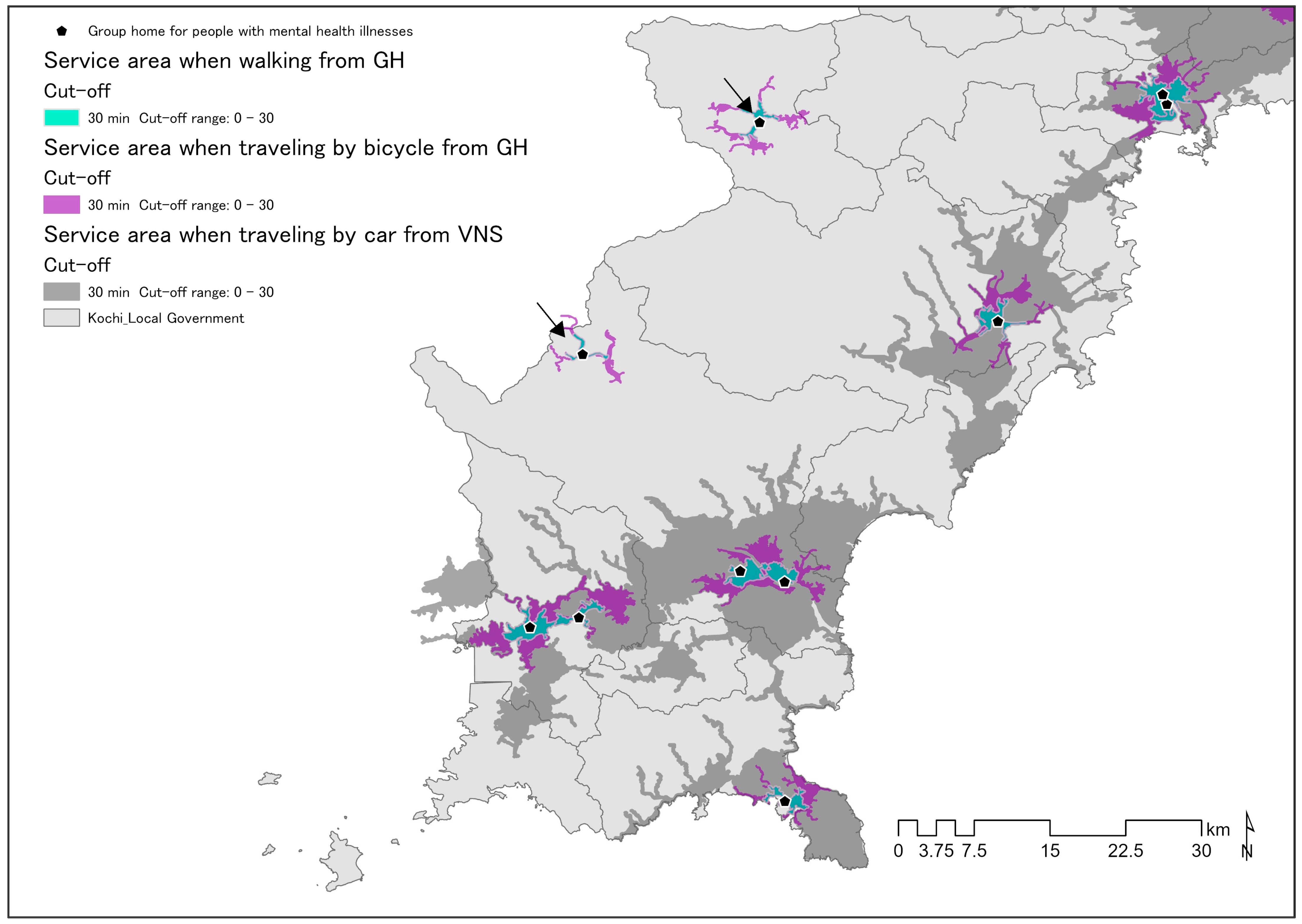
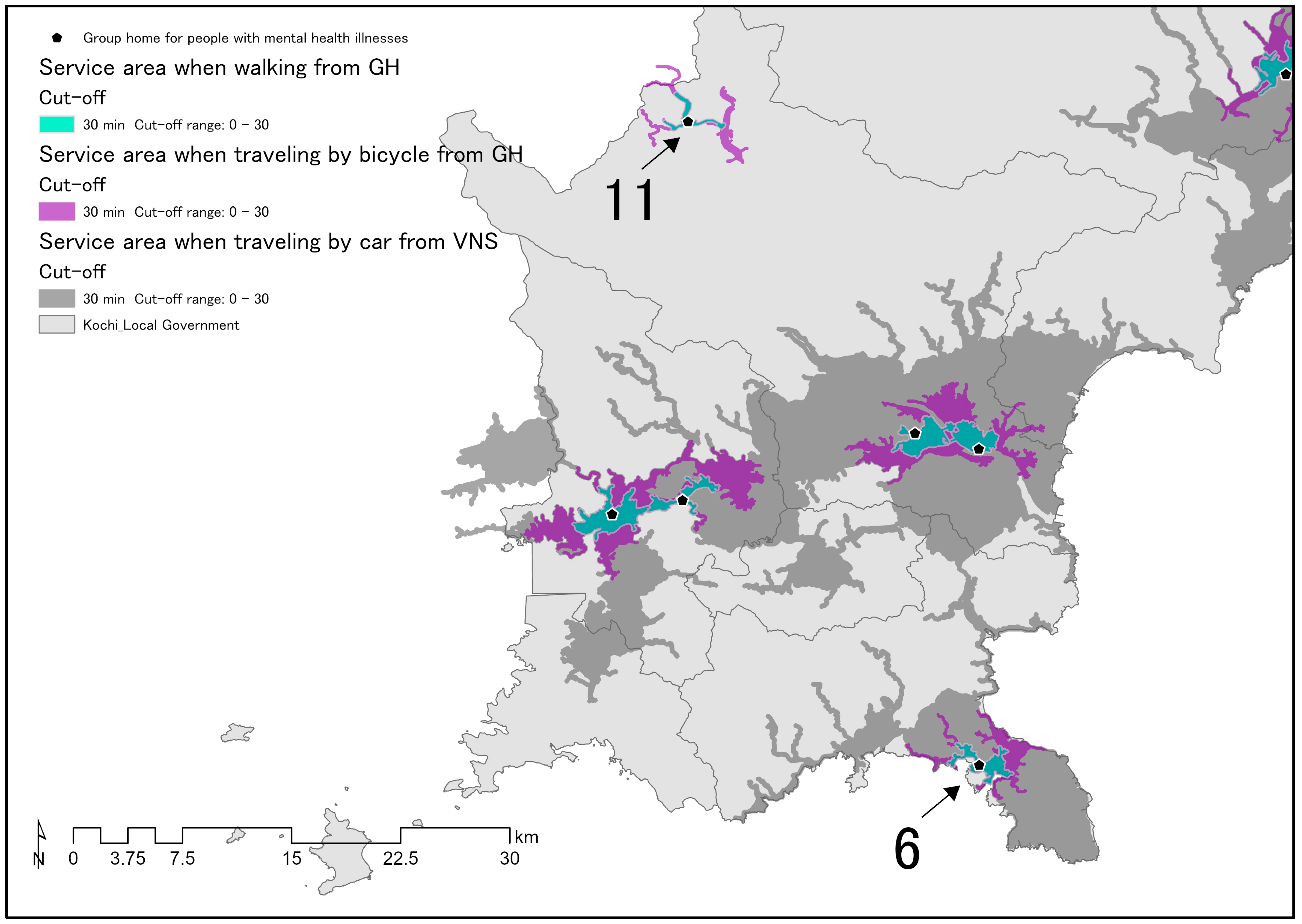
2.3.2. ELA Location Simulation
- (1)
- ELA 1: An area that can be reached by a visiting nurse in 30 min by car from each VNS.
- (2)
- ELA 2: Areas reachable on foot by people with mental illness from each GH.
- (3)
- ELA 3: Areas reachable by bicycle by people with mental illness from each GH.
2.3.3. PH, DC, and SCEB Capacities in ELAs
3. Results
3.1. Overview of GHs, PHs, DCs, SCEBs, and VNSs in Kochi Prefecture
3.2. Results of ELA Location Simulation
3.2.1. ELA 1: GH Location in an Area Reachable by Car from a VNS in 30 Min
3.2.2. ELA 2, 3: Location of Social Resources within the ELA When Walking and Cycling from GH
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamb, H.R. Deinstitutionalization at the Beginning of the New Millennium. Harv. Rev. Psychiatry 1998, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bülow, P.H.; Finkel, D.; Allgurin, M.; Torgé, C.J.; Jegermalm, M.; Ernsth-Bravell, M.; Bülow, P. Aging of severely mentally ill patients first admitted before or after the reorganization of psychiatric care in Sweden. Int. J. Ment. Health Syst. 2022, 16, 35. [Google Scholar] [CrossRef]
- Leff, J.; Trieman, N.; Knapp, M.; Hallam, A. The TAPS Project: Areport on 13 years of research, 1985–1998. Psychiatr. Bull. 2000, 24, 165–168. [Google Scholar] [CrossRef]
- Mortensen, P.B.; Juel, K. Mortality and Causes of Death in First Admitted Schizophrenic Patients. Br. J. Psychiatry 1993, 163, 183–189. [Google Scholar] [CrossRef]
- Craig, T. Homelessness and mental health. Psychiatr. Bull. 1998, 22, 195–197. [Google Scholar] [CrossRef]
- Wallace, C.; Mullen, P.E.; Burgess, P. Criminal Offending in Schizophrenia Over a 25-Year Period Marked by Deinstitutionalization and Increasing Prevalence of Comorbid Substance Use Disorders. Am. J. Psychiatry 2004, 161, 716–727. [Google Scholar] [CrossRef]
- Kim, D.-Y. Psychiatric Deinstitutionalization and Prison Population Growth: A Critical Literature Review and Its Implications. Crim. Justice Policy Rev. 2016, 27, 3–21. [Google Scholar] [CrossRef]
- Lamb, H.R.; Bachrach, L.L. Some Perspectives on Deinstitutionalization. Psychiatr. Serv. 2001, 52, 1039–1045. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Recent Trends in Mental Health and Medical Welfare Measures. Available online: https://www.mhlw.go.jp/content/12200000/000462293.pdf (accessed on 19 March 2023). (In Japanese)
- Barbui, C.; Papola, D.; Saraceno, B. Forty years without mental hospitals in Italy. Int. J. Ment. Health Syst. 2018, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. The 13th “Study Group for Realizing a Mental Health Medical Welfare System Where People Can Live with Peace of Mind”. Available online: https://www.mhlw.go.jp/stf/newpage_26129.html (accessed on 7 June 2023). (In Japanese)
- Ministry of Health, Labour and Welfare. 1st Study Group on Building a Japanese Community-Based Integrated Care System for People with Mental Illness, Reference Material. Available online: https://www.mhlw.go.jp/stf/seishinhoukatukentoukai_00001.html (accessed on 7 June 2023). (In Japanese)
- Ministry of Health, Labour and Welfare. Care for the Older in 2015, (4) Establishment of a Community-Based Integrated Care System. Available online: https://www.mhlw.go.jp/topics/kaigo/kentou/15kourei/3.html#3-2-4 (accessed on 19 March 2023). (In Japanese)
- Ministry of Health, Labour and Welfare. Building a Community-Based Integrated Care System for People with Mental Illness. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/chiikihoukatsu.html (accessed on 20 February 2023). (In Japanese)
- Ministry of Health, Labour and Welfare. Portal Site to Support the Construction of the Community-Based Integrated Care System for People with Mental Illness: What is the “Community-Based Integrated Care System for People with Mental Illness”? Available online: https://www.mhlw-houkatsucare-ikou.jp/ref.html (accessed on 8 February 2023). (In Japanese).
- Nagayama, Y.; Nakai, H. Community-Based Integrated Care System for People with Mental Illness in Japan: Evaluating Location Characteristics of Group Homes to Determine the Feasibility of Daily Life Skill Training. Challenges 2022, 13, 38. [Google Scholar] [CrossRef]
- Community-Based Integrated Care Study Group. Community-Based Integrated Care Study Group Report, Discussion Points for the Future. Available online: https://www.mhlw.go.jp/houdou/2009/05/dl/h0522-1.pdf (accessed on 19 March 2023). (In Japanese)
- Miyajima, T. Promotion of Integrated Community Care System. Available online: https://www.niph.go.jp/journal/data/61-2/201261020001.pdf (accessed on 19 March 2023). (In Japanese)
- Ministry of Health, Labour and Welfare. Community-Based Integrated Care System and Regional Management. Research Report on Systems and Services Related to Building a Community-Based Integrated Care System. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-12400000-Hokenkyoku/0000126435.pdf (accessed on 19 March 2023). (In Japanese)
- Bureau of Social Welfare and Public Health. Tokyo Metropolitan Government Health and Welfare. Plan for the Elderly People (FY2012-FY2014). Available online: https://www.fukushihoken.metro.tokyo.lg.jp/kourei/shisaku/koureisyakeikaku/05keikaku2426/05keikakupdf.html?SLANG=ja&TLANG=en&XMODE=0&XCHARSET=utf-8&XJSID=0 (accessed on 19 March 2023). (In Japanese).
- Xia, J.; Merinder, L.B.; Belgamwar, M.R. Psychoeducation for schizophrenia. Cochrane Database Syst. Rev. 2011, 2011, CD002831. [Google Scholar] [CrossRef] [PubMed]
- Bighelli, I.; Rodolico, A.; Pitschel-Walz, G.; Hansen, W.-P.; Barbui, C.; Furukawa, T.A.; Salanti, G.; Leucht, S. Psychosocial treatments for relapse prevention in schizophrenia: Study protocol for a systematic review and network meta-analysis of randomised evidence. BMJ Open 2020, 10, e035073. [Google Scholar] [CrossRef]
- Chan, S.W.; Yip, B.; Tso, S.; Cheng, B.; Tam, W. Evaluation of a psychoeducation program for Chinese clients with schizophrenia and their family caregivers. Patient Educ. Couns. 2009, 75, 67–76. [Google Scholar] [CrossRef]
- Geospatial Information Authority of Japan What is GIS? Available online: https://www.gsi.go.jp/GIS/whatisgis.html (accessed on 7 June 2023). (In Japanese)
- McLafferty, S.L. GIS and Health Care. Annu. Rev. Public Health 2003, 24, 25–42. [Google Scholar] [CrossRef] [PubMed]
- Khashoggi, B.F.; Murad, A. Issues of Healthcare Planning and GIS: A Review. ISPRS Int. J. Geo-Inf. 2020, 9, 352. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention GIS and Public Health at CDC|cdc.gov. Available online: https://www.cdc.gov/gis/index.htm (accessed on 7 June 2023).
- Fradelos, E.C.; Papathanasiou, I.V.; Mitsi, D.; Tsaras, K.; Kleisiaris, C.F.; Kourkouta, L. Health Based Geographic Information Systems (GIS) and their Applications. Acta Inform. Med. 2014, 22, 402–405. [Google Scholar] [CrossRef]
- Higgs, G. A Literature Review of the Use of GIS-Based Measures of Access to Health Care Services. Health Serv. Outcomes Res. Methodol. 2004, 5, 119–139. [Google Scholar] [CrossRef]
- Salvador-Carulla, L.; Amaddeo, F.; Gutiérrez-Colosía, M.R.; Salazzari, D.; Gonzalez-Caballero, J.L.; Montagni, I.; Tedeschi, F.; Cetrano, G.; Chevreul, K.; Kalseth, J.; et al. Developing a tool for mapping adult mental health care provision in Europe: The REMAST research protocol and its contribution to better integrated care. Int. J. Integr. Care 2015, 15, e042. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef]
- Bhana, A.; Pillay, Y.G. The Use of the Geographical Information System (GIS) to Determine Potential Access and Allocation of Public Mental Health Resources in KwaZulu-Natal. S. Afr. J. Psychol. 1998, 28, 222–233. [Google Scholar] [CrossRef]
- Walker, S.C.; Hurvitz, P.M.; Leith, J.; Rodriguez, F.I.; Endler, G.C. Evidence-Based Program Service Deserts: A Geographic Information Systems (GIS) Approach to Identifying Service Gaps for State-Level Implementation Planning. Adm. Policy Ment. Health Ment. Health Serv. Res. 2016, 43, 850–860. [Google Scholar] [CrossRef] [PubMed]
- Helbich, M. Toward dynamic urban environmental exposure assessments in mental health research. Environ. Res. 2018, 161, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Nishino, T.; Omori, K. A case study of senior case services area settings based on junior high school districts. A comparative study of official service area settings and actual living spheres of the elderly in a regional core city. Trans. AIJ J. Archit. Plan. Environ. Eng. (In Japanese). 2014, 79, 1109–1118. [Google Scholar] [CrossRef]
- Munk-Jørgensen, P. Has deinstitutionalization gone too far? Eur. Arch. Psychiatry Clin. Neurosci. 1999, 249, 136–143. [Google Scholar] [CrossRef]
- Kochi Prefecture Kochi Prefecture Estimated Population. Available online: https://www.pref.kochi.lg.jp/soshiki/121901/t-suikei.html (accessed on 8 June 2023). (In Japanese).
- Kochi Prefecture Introduction to Kochi Prefecture. Available online: https://www.pref.kochi.lg.jp/soshiki/030203/kannnainosizen.html (accessed on 8 June 2023). (In Japanese).
- Kochi City Statistics of Kochi City. Available online: https://www.city.kochi.kochi.jp/soshiki/7/toukei1.html (accessed on 8 June 2023). (In Japanese).
- Kochi Prefecture Mental Illness, Patient Situation, Kochi Prefecture. Available online: https://www.pref.kochi.lg.jp/soshiki/131301/files/2018032800404/file_20183305113413_1.pdf (accessed on 8 June 2023). (In Japanese).
- Kochi City Act on Providing Comprehensive Support for the Daily Life and Life in Society of Persons with Disabilities, Disabled Person Welfare Service Establishments Based on the Child Welfare Act, Etc. Available online: https://www.city.kochi.kochi.jp/soshiki/29/syougaihukushisha-bishu.html (accessed on 1 March 2023). (In Japanese).
- Kochi Prefecture Welfare Service Provider for Persons with Disabilities Designated by Kochi Prefecture. Available online: https://www.pref.kochi.lg.jp/soshiki/060301/kouji.html (accessed on 12 April 2023). (In Japanese).
- Kochi Prefecture Psychiatric Hospital in Kochi. Available online: https://www.pref.kochi.lg.jp/soshiki/060303/seisin-iryoukikan.html (accessed on 7 February 2023). (In Japanese).
- Kochi Medical Social Workers Association List of Psychiatric Medical Institutions in Kochi. Available online: https://kochi-msw.com/data/20211222_research_psychiatric_hospital.pdf (accessed on 1 March 2023). (In Japanese).
- Kochi Prefecture Kochi Prefecture, Nursing Care Service Information Disclosure System. Available online: https://www.kaigokensaku.mhlw.go.jp/39/ (accessed on 12 April 2023). (In Japanese)
- Kochi Visiting Nursing Association List of Visiting Nursing Stations. Available online: https://www.kochi-houkan.com (accessed on 8 April 2023). (In Japanese).
- Ministry of Land, Infrastructure, Transport and Tourism National Land Numerical Infor-mation, Download Site. Available online: https://nlftp.mlit.go.jp/ksj/gml/datalist/KsjTmplt-P05.html (accessed on 10 February 2023). (In Japanese)
- 2016 Startup Seminar, Current Status and Issues of Local Public Transportation 2016 Startup Seminar, Current Status and Issues of Local Public Transportation. Available online: https://wwwtb.mlit.go.jp/hokushin/hrt54/com_policy/pdf/H28startup-koutuukikaku.pdf (accessed on 10 February 2023). (In Japanese)
- Mihoshi, A.; Kitagawa, H.; Yanagihara, T.; Ikeda, H. Extraction of Problems Related to the Movement of Persons with Intellectual and Mental Disabilities. Available online: https://www.e-sora.net/k-sts/titekiidou.pdf (accessed on 16 February 2023). (In Japanese).
- Mimura, Y.; Nishihori, Y.; Kawai, M.; Kachi, N.; Inagaki, T. Fundamental Examination on Travel Behaviors and the limitation factors of Intellectual and Mental Disabilities. A Case Study of Toyota City. J. City Plan. Inst. Jpn. 2010, 45, 469–474. (In Japanese) [Google Scholar] [CrossRef]
- Morota, K.; Ohwaki, T.; Uesaka, K. Investigation of reality of the situation of bicycle use in Japan. Civ. Eng. J. 2009, 51, 6–9. (In Japanese) [Google Scholar]
- Yamanaka, H. Improvement of the Environment for Bicycle Use and Community Development, Meeting of Persons in Charge of Community Cycle. Available online: https://www.mlit.go.jp/common/000990569.pdf (accessed on 1 March 2023). (In Japanese)
- Chang, Y.-C.; Chou, F.H.-C. Effects of Home Visit Intervention on Re-hospitalization Rates in Psychiatric Patients. Community Ment. Health J. 2015, 51, 598–605. [Google Scholar] [CrossRef]
- Uchida, E.; Hosoya, T. The necessity of livelihood support for community psychiatric patients: Contents of home-visit nursing and life support. Jpn. J. Nurs. Sci. 1997, 17, 384–385. (In Japanese) [Google Scholar] [CrossRef]
- Parker, S.; Arnautovska, U.; Siskind, D.; Dark, F.; McKeon, G.; Korman, N.; Harris, M. Community-care unit model of residential mental health rehabilitation services in Queensland, Australia: Predicting outcomes of consumers 1-year post discharge. Epidemiol. Psychiatr. Sci. 2020, 29, e109. [Google Scholar] [CrossRef]
- Dalton-Locke, C.; Marston, L.; McPherson, P.; Killaspy, H. The Effectiveness of Mental Health Rehabilitation Services: A Systematic Review and Narrative Synthesis. Front. Psychiatry 2021, 11, 607933. [Google Scholar] [CrossRef]
- Kawachi, I.; Berkman, L.F. Social ties and mental health. J. Urban Health 2001, 78, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Grinshpoon, A.; Lerner, Y.; Hornik-Lurie, T.; Zilber, N.; Ponizovsky, A.M. Post-discharge contact with mental health clinics and psychiatric readmission: A 6-month follow-up study. Isr. J. Psychiatry Relat. Sci. 2011, 48, 262–267. [Google Scholar] [PubMed]
- Kochi Prefecture Biodiversity Conservation, Kochi’s Strategy. Available online: https://www.pref.kochi.lg.jp/soshiki/030701/kochisenryaku.html (accessed on 12 April 2023). (In Japanese).
- Gandré, C.; Gervaix, J.; Thillard, J.; Macé, J.-M.; Roelandt, J.-L.; Chevreul, K. Geographic variations in involuntary care and associations with the supply of health and social care: Results from a nationwide study. BMC Health Serv. Res. 2018, 18, 253. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Data Type | Source | Use |
|---|---|---|---|
| 1 | Kochi Prefecture (polygon) | National Land Numerical Information, download site [47]. | We created a polygon layer of Kochi Prefecture divided according to local government. |
| 2 | Address of group home for people with mental illness (point) | Website of Kochi Prefecture [42] and Kochi City [41]. | Using GIS, we converted the address into coordinate values and plotted the center of the building on the map. |
| 3 | Psychiatric hospital (point) | Website of Kochi Prefecture [43] and Kochi Medical Social Workers Association [44]. | |
| 4 | Support office for continuous employment type B (point) | Website of Kochi Prefecture [42] and Kochi City [41]. | |
| 5 | Visiting nursing station (point) | Website of Kochi Prefecture [45] and Kochi Prefecture Visiting Nurse Association [46]. |
| Characteristics | Median (Range) | n | % |
|---|---|---|---|
| Group home | 73 | 100 | |
| Group home admission capacity (people) | 12.0 (4–99) | ||
| Accepts people with mental illness | 49 | 67.1 | |
| Psychiatric hospital | 41 | 100 | |
| Psychiatric hospital number of beds (beds) | 60.0 (0–271) | ||
| Daycare center * | 18 | 43.9 | |
| Support office for continuous employment type B | 111 | 100 | |
| Support office for continuous employment type B admission capacity (people) | 20.0 (10–44) | ||
| Visiting nursing station | 80 | 100 | |
| Visiting nursing station number of nurses calculated on a full-time equivalent basis (people) | 4.5 (2.5–16.5) | ||
| Visiting nursing station providing visiting nursing care services to psychiatric patients | 53 | 66.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakai, Y.; Nakai, H. Evaluation of Everyday Living Areas for Deinstitutionalized Community-Living People with Mental Illness. Challenges 2023, 14, 30. https://doi.org/10.3390/challe14030030
Nakai Y, Nakai H. Evaluation of Everyday Living Areas for Deinstitutionalized Community-Living People with Mental Illness. Challenges. 2023; 14(3):30. https://doi.org/10.3390/challe14030030
Chicago/Turabian StyleNakai, Yuri, and Hisao Nakai. 2023. "Evaluation of Everyday Living Areas for Deinstitutionalized Community-Living People with Mental Illness" Challenges 14, no. 3: 30. https://doi.org/10.3390/challe14030030
APA StyleNakai, Y., & Nakai, H. (2023). Evaluation of Everyday Living Areas for Deinstitutionalized Community-Living People with Mental Illness. Challenges, 14(3), 30. https://doi.org/10.3390/challe14030030