Patients with Initial Negative RT-PCR and Typical Imaging of COVID-19: Clinical Implications

 , , , and
, , , and
Abstract
:1. Introduction
2. Material and Methods
3. Statistical Analysis
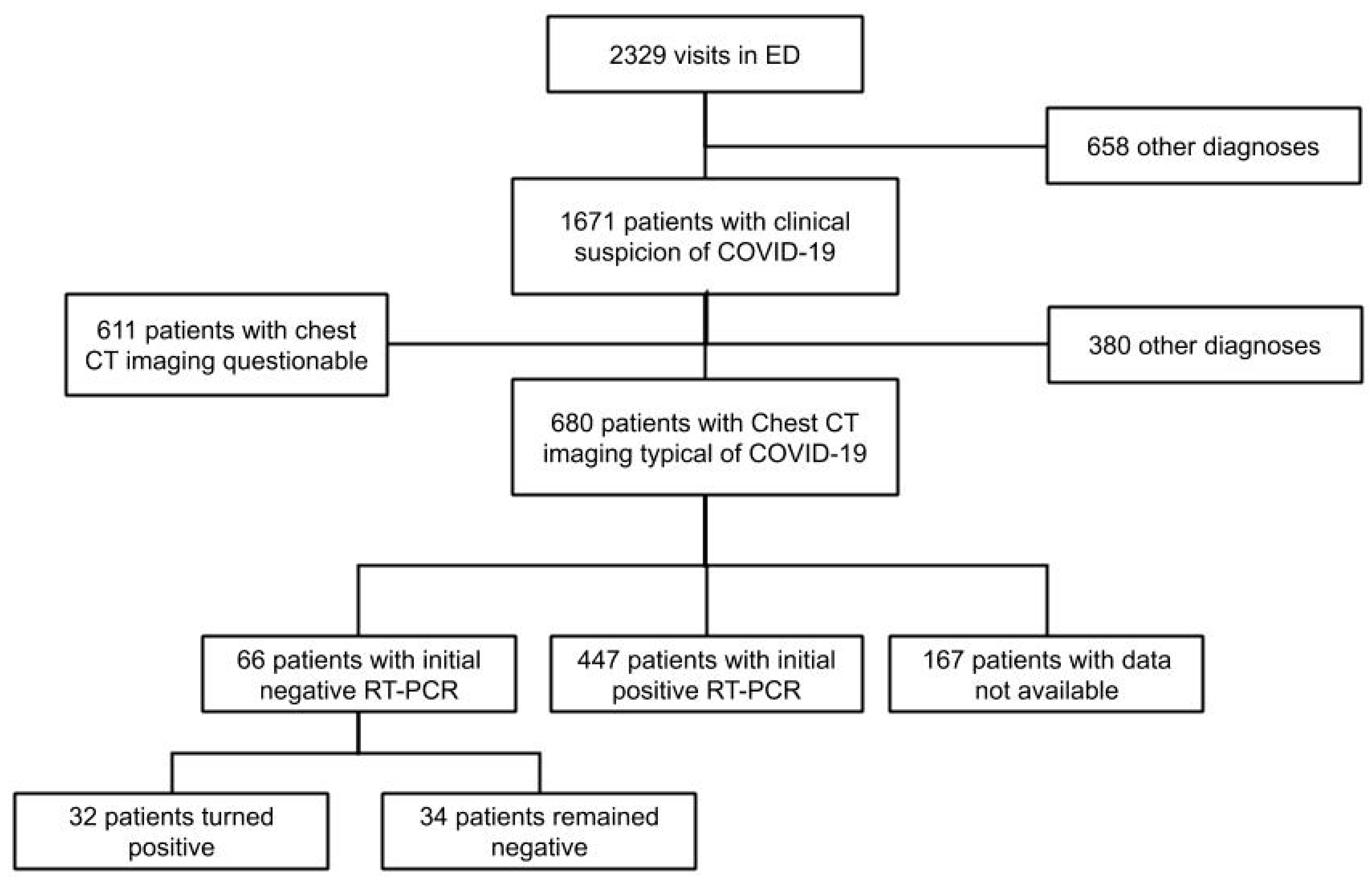
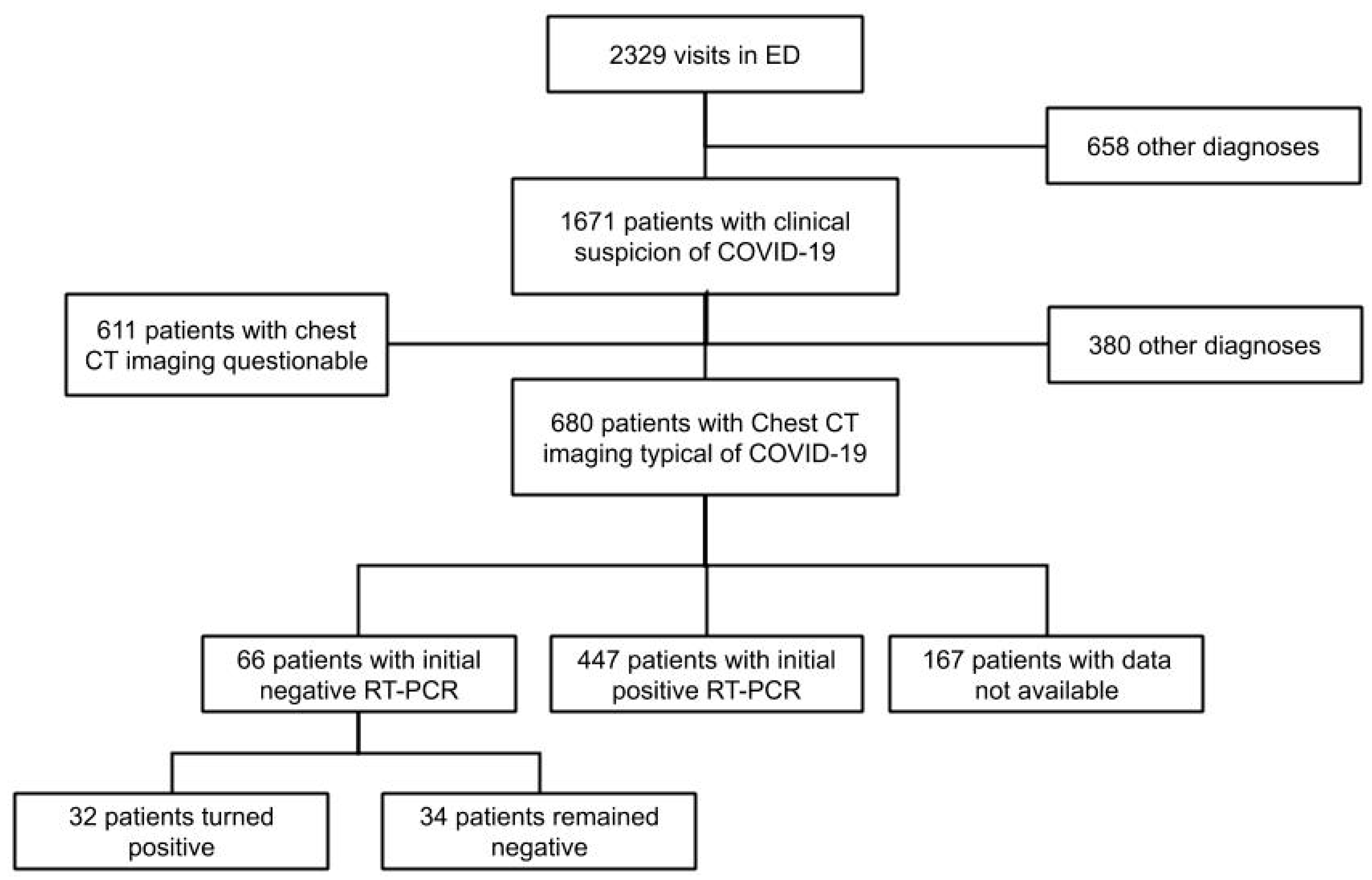
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.W.; Schmitz, J.E.; Persing, D.H.; Stratton, C.W. The Laboratory Diagnosis of COVID-19 Infection: Current Issues and Challenges. J. Clin. Microbiol. 2020, 58, 512–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubin, E.J.; Baden, L.R.; Morrissey, S.; Campion, E.W. Medical Journals and the 2019-nCoV Outbreak. N. Engl. J. Med. 2020, 382, 866. [Google Scholar] [CrossRef] [PubMed]
- Xie, X.; Zhong, Z.; Zhao, W.; Zheng, C.; Wang, F.; Liu, J. Chest CT for Typical 2019-nCoV Pneumonia: Relationship to Negative RT-PCR Testing. Radiology 2020, 296, E41–E45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing in Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, C.; Xu, H.; Shen, Q.; Zhang, X.; Fan, B.; Wang, C.; Zeng, B.; Li, Z.; Li, X.; Li, H.; et al. Diagnosis of the Coronavirus disease (COVID-19): rRT-PCR or CT? Eur. J. Radiol. 2020, 126, 108961. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hong, H.; Yoon, S.H. Diagnostic Performance of CT and Reverse Transcriptase-Polymerase Chain Reaction for Coronavirus Disease 2019: A Meta-Analysis. Radiology 2020. [Google Scholar] [CrossRef]
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert. Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Yao, L.; Li, J.; Chen, L.; Song, Y.; Cai, Z.; Yang, C. Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19. J. Med. Virol. 2020, 92, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Xiao, A.T.; Tong, Y.X.; Zhang, S. False-negative of RT-PCR and prolonged nucleic acid conversion in COVID-19: Rather than recurrence. J. Med. Virol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, F.; Yan, L.; Wang, N.; Yang, S.; Wang, L.; Tang, Y.; Gao, G.; Wang, S.; Ma, C.; Xie, R.; et al. Quantitative Detection and Viral Load Analysis of SARS-CoV-2 in Infected Patients. Clin. Infect. Dis. 2020, 71, 793–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavare, A.N.; Braddy, A.; Brill, S.; Jarvis, H.; Sivaramakrishnan, A.; Barnett, J.; Creer, D.D.; Hare, S.S. Managing high clinical suspicion COVID-19 inpatients with negative RT-PCR: A pragmatic and limited role for thoracic CT. Thorax 2020, 75, 537–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Wang, W.; Lei, Y.; Zhang, B.; Yang, J.; Hu, J.; Ren, Y.J.; Lu, F.Q. Comparison of the clinical characteristics between RNA positive and negative patients clinically diagnosed with 2019 novel coronavirus pneumonia. Chin. J. Tuberc. Respir. Dis. 2020, 43, 427–430. [Google Scholar]
- Salehi, S.; Abedi, A.; Balakrishnan, S.; Gholamrezanezhad, A. Coronavirus disease 2019 (COVID-19) imaging reporting and data system (COVID-RADS) and common lexicon: A proposal based on the imaging data of 37 studies. Eur. Radiol. 2020, 28, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pascarella, G.; Strumia, A.; Piliego, C.; Bruno, F.; Del Buono, R.; Costa, F.; Scarlata, S.; Agrò, F.E. COVID-19 diagnosis and management: A comprehensive review. J. Intern. Med. 2020, 288, 192–206. [Google Scholar] [CrossRef]
- Revel, M.P.; Parkar, A.P.; Prosch, H.; Silva, M.; Sverzellati, N.; Gleeson, F.; Brady, A. COVID-19 patients and the radiology department – advice from the European Society of Radiology (ESR) and the European Society of Thoracic Imaging (ESTI). Eur. Radiol. 2020, 30, 4903–4909. [Google Scholar] [CrossRef] [Green Version]
- Baden, L.R.; Drazen, J.M.; Kritek, P.A.; Curfman, G.D.; Morrissey, S.; Campion, E.W. H1N1 Influenza A Disease—Information for Health Professionals. N. Engl. J. Med. 2009, 360, 2666–2667. [Google Scholar] [CrossRef] [Green Version]
- Institut Pasteur, P. Protocol: Real-Time RT-PCR Assays for the Detection of SARS-CoV-2. Available online: https://www.who.int/docs/default-source/coronaviruse/real-time-rt-pcr-assays-for-the-detection-of-sars-cov-2-institut-pasteur-paris.pdf?sfvrsn=3662fcb6_2 (accessed on 15 September 2020).
- Du, R.H.; Liang, L.R.; Yang, C.Q.; Wang, W.; Cao, T.Z.; Li, M.; Guo, G.Y.; Du, J.; Zheng, C.L.; Zhu, Q. Predictors of Mortality for Patients with COVID-19 Pneumonia Caused by SARS-CoV-2: A Prospective Cohort Study. Eur. Respir. J. 2020, 55, 2000524. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, X.; Jia, X.; Li, J.; Hu, K.; Chen, G.; Wei, J.; Gong, Z.; Zhou, C.; Yu, H.; et al. Risk factors for disease severity, unimprovement, and mortality of COVID-19 patients in Wuhan, China. Clin. Microbiol. Infect. 2020, 26, 767–772. [Google Scholar] [CrossRef]
- Hu, Y.; Sun, J.; Dai, Z.; Deng, H.; Li, X.; Huang, Q.; Wu, Y.; Sun, L.; Xu, Y. Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis. J. Clin. Virol. 2020, 127, 104371. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; de Mendonca, A.; Cantraine, F.; Moreno, R.; Takala, J.; Suter, P.M.; Sprung, C.L.; Colardyn, F.; Blecher, S. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units: Results of a multicenter, prospective study. Crit. Care Med. 1998, 26, 1793–1800. [Google Scholar] [CrossRef] [PubMed]
- Oberlin, M.; Le Borgne, P.; Behr, M.; Kepka, S.; Bilbault, P. The organisation of a French emergency department in a coronavirus hotspot. Anaesth. Crit. Care Pain Med. 2020, 39, 457–458. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C.; Kwee, R.M. COVID-19 and chest CT: Do not put the sensitivity value in the isolation room and look beyond the numbers. Radiology 2020, 27, 201709. [Google Scholar] [CrossRef]
- Hope, M.D.; Raptis, C.A.; Shah, A.; Hammer, M.M.; Henry, T.S. A role for CT in COVID-19? What data really tell us so far. Lancet 2020, 395, 1189–1190. [Google Scholar] [CrossRef]
- Rubin, G.D.; Ryerson, C.J.; Haramati, L.B.; Sverzellati, N.; Kanne, J.P.; Raoof, S.; Volpi, A.; Yim, J.J.; Martin, I.B.K.; Anderson, D.J.; et al. The Role of Chest Imaging in Patient Management during the COVID-19 Pandemic: A Multinational Consensus Statement from the Fleischner Society. Radiology 2020. [Google Scholar] [CrossRef] [Green Version]
- Herpe, G.; Lederlin, M.; Naudin, M.; Ohana, M.; Chaumoitre, K.; Gregory, J.; Vilgrain, V.; Freitag, C.A.; De Margerie-Mellon, C.; Flory, V.; et al. Efficacy of Chest CT for COVID-19 Pneumonia in France. Radiology 2020, 214, 1280–1286. [Google Scholar] [CrossRef]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized With COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.; Wang, Z.; Liang, Y.; Huang, T.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Parameters | PCR− Group | PCR+ Group | Difference in Means or Proportion | Pr(Diff > 0) b |
|---|---|---|---|---|
| No = 66 | No = 198 | (CrI) a | ||
| Population | ||||
| Age, years, means (SD) | 59.7 (15.3) | 59.9 (15.9) | −0.17 (−4.13;3.73) | 0.47 |
| Gender, Male | 41 (62.1) | 128 (64.6) | −0.03 (−0.16;0.10) | 0.35 |
| Comorbidity | ||||
| BMI, kg/m2, mean (SD) | 25.0 (10.9) | 27.5 (10.4) | −2.20 (−5.41;1.00) | 0.09 * |
| Hypertension | 29 (43.9) | 86 (43.4) | 0.01 (−0.13;0.14) | 0.53 |
| Diabetes mellitus | 14 (21.2) | 46 (23.2) | −0.01 (−0.12;0.10) | 0.39 |
| Active smoking | 7 (10.6) | 11 (5.6) | 0.06 (−0.02;0.15) | 0.93 |
| Chronic heart disease | 5 (7.6) | 13 (6.6) | 0.02 (−0.05;0.10) | 0.66 |
| Chronic respiratory disease | 20 (30.3) | 23 (11.6) | 0.19 (0.07;0.31) | >0.99 * |
| Asthma | 7 (10.6) | 12 (6.1) | 0.05 (−0.02;0.14) | 0.90 * |
| Chronic bronchitis | 8 (12.1) | 4 (2.0) | 0.11 (0.03;0.20) | 0.99 * |
| Chronic kidney disease | 4 (6.1) | 17 (8.6) | −0.02 (−0.08;0.06) | 0.31 |
| Active cancer or hemopathy | 11 (16.7) | 25 (12.6) | 0.05 (−0.05;0.15) | 0.81 |
| Clinical features in the ED | ||||
| Time from onset to admission | ||||
| day, mean (SD) | 8.8 (6.6) | 8.2 (6.1) | 0.62 (−1.13;2.34) | 0.75 |
| ≥7 days | 34 (51.5) | 87 (43.9) | 0.07 (−0.06;0.21) | 0.86 |
| Systolic Blood Pressure | ||||
| mmHg, mean (SD) | 135.9 (24.6) | 134.5 (21.3) | 1.13 (−4.93;7.19) | 0.64 |
| Heart rate | ||||
| bpm, mean (SD) | 92.9 (19.0) | 92.8 (16.5) | 0.10 (−4.63;4.90) | 0.52 |
| ≥120 bpm | 8 (12.1) | 13 (6.6) | 0.06 (−0.02; 0.16) | 0.93 * |
| Glasgow coma scale | 15 (0.1) | 14.9 (0.4) | 0.08 (0.01;0.15) | 0.98 |
| Respiratory rate | ||||
| breaths per minute, mean (SD) | 23.8 (5.7) | 27.1 (9.1) | −3.16 (−5.42;−0.87) | <0.01 * |
| ≥24 breaths per minute | 21 (50.0) | 99 (68.8) | −0.18 (−0.35;0.02) | 0.01 * |
| Minimal oxygen saturation at admission | ||||
| %, mean (SD) | 92.1 (7.5) | 91.4 (8.6) | 0.76 (−1.44;2.89) | 0.75 |
| <94% | 31 (47.0) | 96 (48.5) | −0.01 (−0.15;0.12) | 0.42 |
| Maximal oxygen level at admission | ||||
| L/min, mean (SD) | 3.0 (3.5) | 4.4 (4.4) | −1.37 (−2.39;−0.34) | <0.01 * |
| ≥5 L/min | 10 (15.2) | 65 (32.8) | −0.17 (−0.27;−0.05) | <0.01 * |
| Parameters | PCR− Group | PCR+ Group | Difference in Means or Proportion | Pr(Diff > 0) b |
|---|---|---|---|---|
| No = 66 | No = 198 | (CrI) a | ||
| Laboratory Findings | ||||
| Neutrophil count, per µL, mean (SD) | 5294.8 (3419.4) | 5187.8 (2752.4) | 4.71 (−171.35;175.26) | 0.53 |
| Lymphocyte count, per µL, mean (SD) | 1083.6 (513.5) | 1054.8 (629.4) | 9.50 (−78.60;96.02) | 0.58 |
| Hemoglobin, g/dL, mean (SD) | 16.2 (16.7) | 13.6 (1.8) | 2.38 (−1.38;6.11) | 0.89 |
| Platelet count, per µL, mean (SD) | 223.0 (99.8) | 215.8 (78.9) | 4.17 (−15.5;23.62) | 0.66 |
| Natremia, mmol/L, mean (SD) | 136.3 (3.5) | 135.3 (3.5) | 0.94 (−0.03;1.91) | 0.97 * |
| Serum creatinine, µmol/L, mean (SD) | 81.4 (39.1) | 85.8 (57.4) | −3.63 (−15.13;7.85) | 0.27 |
| ALT, U/L, mean (SD) | 46.4 (33.5) | 88.0 (63.4) | −36.26 (−88.03;13.94) | 0.08 * |
| AST, U/L, mean (SD) | 50.0 (33.5) | 63.3 (60.2) | −11.19 (−23.19;0.92) | 0.03 * |
| C−Reactive Protein | ||||
| mg/L, mean (SD) | 96.7 (81.7) | 113.2 (83.9) | −10.10 (−27.98;8.80) | 0.14 |
| inf 100 mg/L | 39 (61.9) | 101 (51) | 0.10 (−0.03;0.24) | 0.93 * |
| 100−200mg/L | 16 (25.4) | 70 (35.4) | −0.09 (−0.21;0.04) | 0.08 * |
| ≥200 mg/L | 8 (12.7) | 27 (13.6) | −0.01 (−0.09;0.10) | 0.47 |
| Lactate | ||||
| mmol/L, mean (SD) | 1.3 (1.1) | 1.1 (0.6) | 0.21 (−0.16;0.57) | 0.87 |
| >2 mmol/L | 4 (9.5) | 10 (7.4) | 0.03 (−0.06;0.15) | 0.73 |
| Imaging | ||||
| Mild | 17 (26.6) | 26 (13.0) | 0.14 (0.03;0.27) | 0.99 * |
| Moderate | 30 (46.9) | 87 (44.8) | 0.01 (−0.12;0.15) | 0.57 |
| Extended | 8 (12.5) | 41 (21.1) | −0.08 (−0.17;0.02) | 0.06 * |
| Severe to critical | 9 (14.1) | 40 (20.6) | −0.06 (−0.16;0.05) | 0.13 |
| Severity | ||||
| SOFA score | 5.0 (1.7) | 5.6 (1.7) | −0.55 (−1.04;0.08) | 0.01 * |
| Mechanical ventilation | 5 (7.6) | 29 (14.7) | −0.06 (0.14;0.03) | 0.08 * |
| Outcome | PCR− Group | PCR+ Group | Difference in Means or Proportion | Pr(Diff > 0) b |
|---|---|---|---|---|
| No = 66 | No = 198 | (CrI) a | ||
| In−hospital mortality, n (%) | 6 (9.1) | 19 (9.6) | 0.01 (−0.07;0.09) | 0.50 |
| ICU admission, n (%) | 15 (22.7) | 61 (30.8) | −0.07 (−0.19;0.05) | 0.11 |
| Hospital LOS, days, mean (SD) | 8.7 (7.4) | 9.8 (8.3) | −1.01 (−3.06;1.16) | 0.17 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baicry, F.; Le Borgne, P.; Fabacher, T.; Behr, M.; Lemaitre, E.L.; Gayol, P.-A.; Harscoat, S.; Issur, N.; Garnier-Kepka, S.; Ohana, M.; et al. Patients with Initial Negative RT-PCR and Typical Imaging of COVID-19: Clinical Implications. J. Clin. Med. 2020, 9, 3014. https://doi.org/10.3390/jcm9093014
Baicry F, Le Borgne P, Fabacher T, Behr M, Lemaitre EL, Gayol P-A, Harscoat S, Issur N, Garnier-Kepka S, Ohana M, et al. Patients with Initial Negative RT-PCR and Typical Imaging of COVID-19: Clinical Implications. Journal of Clinical Medicine. 2020; 9(9):3014. https://doi.org/10.3390/jcm9093014
Chicago/Turabian StyleBaicry, Florent, Pierrick Le Borgne, Thibaut Fabacher, Martin Behr, Elena Laura Lemaitre, Paul-Albert Gayol, Sébastien Harscoat, Nirvan Issur, Sabrina Garnier-Kepka, Mickael Ohana, and et al. 2020. "Patients with Initial Negative RT-PCR and Typical Imaging of COVID-19: Clinical Implications" Journal of Clinical Medicine 9, no. 9: 3014. https://doi.org/10.3390/jcm9093014
APA StyleBaicry, F., Le Borgne, P., Fabacher, T., Behr, M., Lemaitre, E. L., Gayol, P.-A., Harscoat, S., Issur, N., Garnier-Kepka, S., Ohana, M., Bilbault, P., & Oberlin, M. (2020). Patients with Initial Negative RT-PCR and Typical Imaging of COVID-19: Clinical Implications. Journal of Clinical Medicine, 9(9), 3014. https://doi.org/10.3390/jcm9093014