Both HCV Infection and Elevated Liver Stiffness Significantly Impacts on Several Parameters of T-Cells Homeostasis in HIV-Infected Patients


 , and
, and
Abstract
1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Cell Samples
2.3. Immunophenotypic Analysis
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Patients Included in the Study
3.2. HCV Co-Infection Significantly Impacts on T-Cells Homeostasis
3.3. The Degree of Liver Stiffness Significantly Impacts on T-Cells Homeostasis
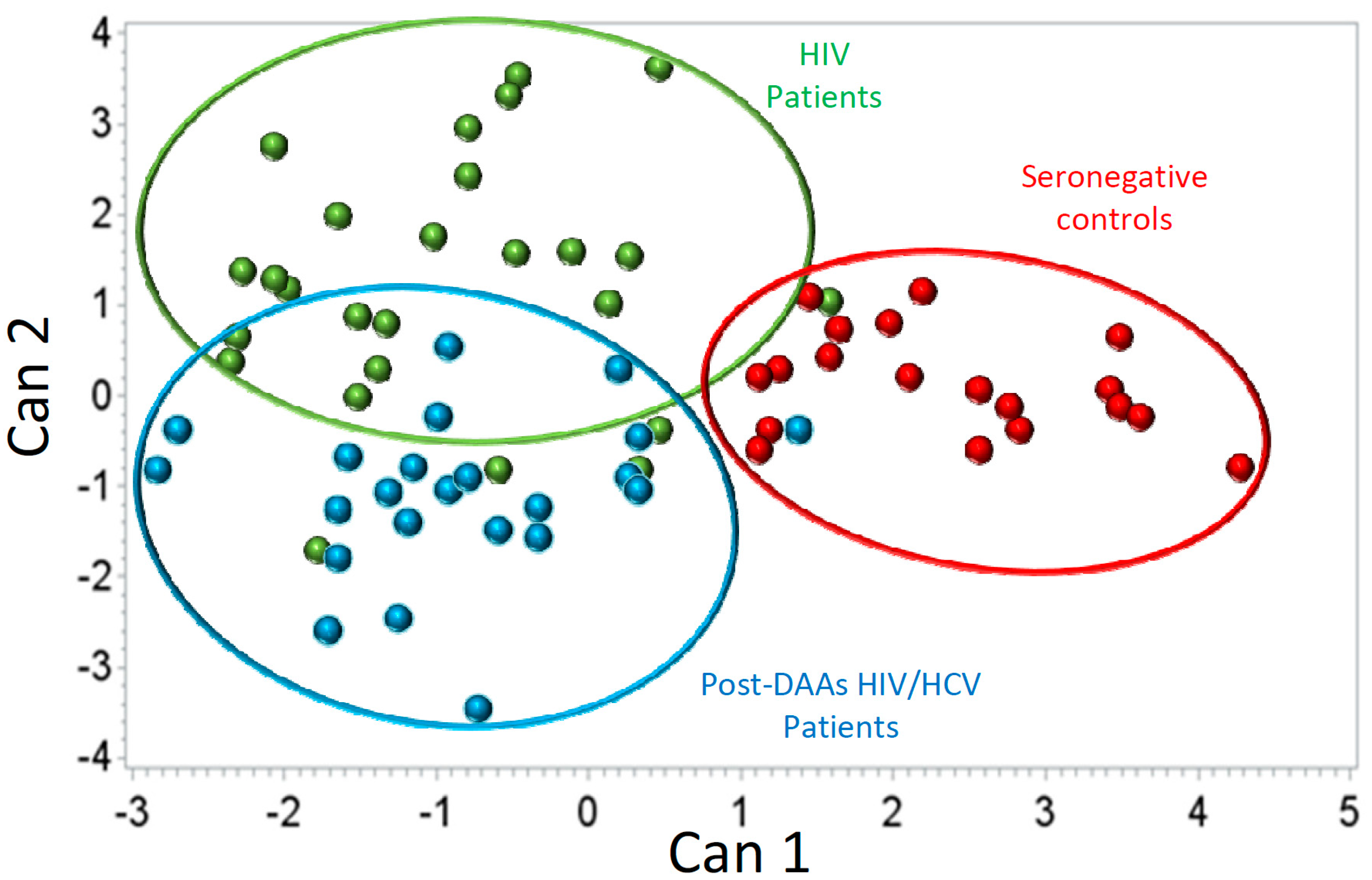
3.4. HCV Eradication with DAAs Does Not Completely Revert T-Cells Homeostasis Disturbances
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Unaids.org. UNAIDS DATA 2019. Available online: https://www.unaids.org/en/resources/documents/2019/2019-UNAIDS-data (accessed on 15 February 2020).
- WHO. Global Hepatitis Report 2017. Available online: https://www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ (accessed on 15 February 2020).
- Hernandez, M.D.; Sherman, K. HIV/hepatitis C coinfection natural history and disease progression. Curr. Opin. HIV AIDS 2011, 6, 478–482. [Google Scholar] [CrossRef]
- Matthews, G.; Dore, G. HIV and hepatitis C coinfection. J. Gastroenterol. Hepatol. 2008, 23, 1000–1008. [Google Scholar] [CrossRef] [PubMed]
- Ingiliz, P.; Rockstroh, J. Natural history of liver disease and effect of hepatitis C virus on HIV disease progression. Curr. Opin. HIV AIDS 2015, 10, 303–308. [Google Scholar] [CrossRef]
- Sherman, K.E.; O’Brien, J.; Gutierrez, A.G.; Harrison, S.; Urdea, M.; Neuwald, P.; Wilber, J. Quantitative Evaluation of Hepatitis C Virus RNA in Patients with Concurrent Human Immunodeficiency Virus Infections. J. Clin. Microbiol. 1993, 31, 2679–2682. [Google Scholar] [CrossRef]
- Telfer, P.; Sabin, C.; Devereux, H.; Scott, F.; Dusheiko, G.; Lee, C. The progression of HCV-associated liver disease in a cohort of haemophilic patients. Br. J. Haematol. 1994, 87, 555–561. [Google Scholar] [CrossRef]
- Benhamou, Y.; Bochet, M.; Di Martino, V.; Charlotte, F.; Azria, F.; Coutellier, A.; Vidaud, M.; Bricaire, F.; Opolon, P.; Katlama, C.; et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. Hepatology 1999, 30, 1054–1058. [Google Scholar] [CrossRef]
- Bräu, N.; Fox, R.; Xiao, P.; Marks, K.; Naqvi, Z.; Taylor, L.E.; Trikha, A.; Sherman, M.; Sulkowski, M.S.; Dieterich, D.T.; et al. North American Liver Cancer in HIV Study Group. Presentation and outcome of hepatocellular carcinoma in HIV-infected patients: A U.S.–Canadian multicenter study. J. Hepatol. 2007, 47, 527–537. [Google Scholar] [CrossRef]
- Qurishi, N.; Kreuzberg, C.; Lüchters, G.; Effenberger, W.; Kupfer, B.; Sauerbruch, T.; Rockstroh, J.K.; Spengler, U. Effect of antiretroviral therapy on liver-related mortality in patients with HIV and hepatitis C virus coinfection. Lancet 2003, 362, 1708–1713. [Google Scholar] [CrossRef]
- Thein, H.; Yi, Q.; Dore, G.; Krahn, M. Natural history of hepatitis C virus infection in HIV-infected individuals and the impact of HIV in the era of highly active antiretroviral therapy: A meta-analysis. AIDS 2008, 22, 1979–1991. [Google Scholar] [CrossRef]
- Sulkowski, M.S.; Moore, R.D.; Mehta, S.H.; Chaisson, R.E.; Thomas, D.L. Hepatitis C and progression of HIV disease. JAMA 2002, 288, 199–206. [Google Scholar] [CrossRef]
- Rockstroh, J.K.; Mocroft, A.; Soriano, V.; Tural, C.; Losso, M.H.; Horban, A.; Kirk, O.; Phillips, A.; Ledergerber, B.; Lundgren, J. EuroSIDA Study Group. Influence of hepatitis C virus infection on HIV-1 disease progression and response to highly active antiretroviral therapy. J. Infect. Dis. 2005, 192, 992–1002. [Google Scholar] [CrossRef]
- D’ Arminio Monforte, A.; Cozzi-Lepri, A.; Castagna, A.; Antinori, A.; De Luca, A.; Mussini, C.; Caputo, S.L.; Arlotti, M.; Magnani, G.; Pellizzer, G.; et al. Icona Foundation Study Group. Risk of developing specific AIDS-defining illnesses in patients coinfected with HIV and hepatitis C virus with or without liver cirrhosis. Clin. Infect. Dis. 2009, 49, 612–622. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Van der Helm, J.; Geskus, R.; Sabin, C.; Meyer, L.; Del Amo, J.; Chêne, G.; Dorrucci, M.; Muga, R.; Porter, K.; Prins, M. CASCADE Collaboration in EuroCoord. Effect of HCV infection on cause-specific mortality after HIV seroconversion, before and after 1997. Gastroenterology 2013, 144, 751–760. [Google Scholar] [CrossRef]
- Kovacs, A.; Karim, R.; Mack, W.J.; Xu, J.; Chen, Z.; Operskalski, E.; Frederick, T.; Landay, A.; Voris, J.; Spencer, L.S.; et al. Activation of CD8 T cells predicts progression of HIV infection in women coinfected with hepatitis C virus. J. Infect. Dis. 2010, 201, 823–834. [Google Scholar] [CrossRef]
- Gonzalez, V.D.; Falconer, K.; Blom, K.G.; Reichard, O.; Mørn, B.; Laursen, A.L.; Weis, N.; Alaeus, A.; Sandberg, J.K. High levels of chronic immune activation in the T-cell compartments of patients coinfected with hepatitis C virus and human immunodeficiency virus type 1 and on highly active antiretroviral therapy are reverted by alpha interferon and ribavirin treatment. J. Virol. 2009, 83, 11407–11411. [Google Scholar] [CrossRef]
- Feuth, T.; Arends, J.E.; Fransen, J.H.; Nanlohy, N.M.; van Erpecum, K.J.; Siersema, P.D.; Hoepelman, A.I.; van Baarle, D. Complementary role of HCV and HIV in T-cell activation and exhaustion in HIV/HCV coinfection. PLoS ONE 2013, 8, e59302. [Google Scholar] [CrossRef]
- Korner, C.; Kramer, B.; Schulte, D.; Coenen, M.; Mauss, S.; Fätkenheuer, G.; Oldenburg, J.; Nattermann, J.; Rockstroh, J.K.; Spengler, U. Effects of HCV coinfection on apoptosis of CD4+ T-cells in HIV-positive patients. Clin. Sci. (Lond.) 2009, 116, 861–870. [Google Scholar] [CrossRef]
- Nuñez, M.; Soriano, V.; López, M.; Ballesteros, C.; Cascajero, A.; González-Lahoz, J.; Benito, J.M. Coinfection with Hepatitis C Virus Increases Lymphocyte Apoptosis in HIV-Infected Patients. Clin. Infect. Dis. 2006, 43, 1209–1212. [Google Scholar] [CrossRef][Green Version]
- Laskus, T.; Kibler, K.V.; Chmielewski, M.; Wilkinson, J.; Adair, D.; Horban, A.; Stańczak, G.; Radkowski, M. Effect of hepatitis C virus on HIV-induced apoptosis. PLoS ONE 2013, 8, e75921. [Google Scholar] [CrossRef]
- Schmagel, K.V.; Saidakova, E.V.; Korolevskaya, L.B.; Shmagel, N.G.; Chereshnev, V.A.; Anthony, D.D.; Lederman, M.M. Influence of hepatitis C virus coinfection on CD4+ T cells of HIV-infected patients receiving HAART. AIDS 2014, 28, 2381–2388. [Google Scholar] [CrossRef]
- Korolevskaya, L.; Shmagel, K.; Saidakova, E.; Shmagel, N.; Slobodchikova, S.; Chereshnev, V. Effect of Hepatitis C Virus Coinfection on the Content of CD4+ and CD8+ T Cell Subpopulations in HIV-Infected Patients Receiving Antiretroviral Therapy. Bull. Exp. Biol. Med. 2016, 161, 281–283. [Google Scholar] [CrossRef] [PubMed]
- Saha, B.; Choudhary, M.; Sarin, S. Expression of inhibitory markers is increased on effector memory T cells during hepatitis C virus/HIV coinfection as compared to hepatitis C virus or HIV monoinfection. AIDS 2013, 27, 2191–2200. [Google Scholar] [CrossRef] [PubMed]
- Grady, B.; Nanlohy, N.; van Baarle, D. HCV monoinfection and HIV/HCV coinfection enhance T-cell immune senescence in injecting drug users early during infection. Immun. Ageing 2016, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Rallón, N.; García, M.; García-Samaniego, J.; Rodríguez, N.; Cabello, A.; Restrepo, C.; Álvarez, B.; García, R.; Górgolas, M.; Benito, J.M. HCV coinfection contributes to HIV pathogenesis by increasing immune exhaustion in CD8 T-cells. PLoS ONE 2017, 12, e0173943. [Google Scholar] [CrossRef]
- Massanella, M.; Tural, C.; Papagno, L.; Garcia, E.; Jou, A.; Bofill, M.; Autran, B.; Clotet, B.; Blanco, J. Changes in T-cell subsets in HIV–HCV-coinfected patients during pegylated interferon-α2a plus ribavirin treatment. Antivir. Therapy 2010, 15, 333–342. [Google Scholar] [CrossRef]
- Marchetti, G.; Nasta, P.; Bai, F.; Gatti, F.; Bellistrì, G.M.; Tincati, C.; Borghi, F.; Carosi, G.; Puoti, M.; Monforte, A.D. Circulating sCD14 is associated with virological response to pegylated-interferon-alpha/ribavirin treatment in HIV/HCV co-infected patients. PLoS ONE 2012, 7, e32018. [Google Scholar] [CrossRef]
- Thomas, H.; Foster, G.; Platis, D. Mechanisms of action of interferon and nucleoside analogues. J. Hepatol. 2003, 39, S93–S98. [Google Scholar] [CrossRef]
- Sikavi, C.; Chen, P.; Lee, A.; Saab, E.; Choi, G.; Saab, S. Hepatitis C and Human Immunodeficiency Virus Co-Infection in the Era of Direct-Acting Antiviral Agents: No Longer A Difficult to Treat Population. Hepatology 2018, 67, 847–857. [Google Scholar] [CrossRef]
- Castéra, L.; Vergniol, J.; Foucher, J.; Le Bail, B.; Chanteloup, E.; Haaser, M.; Darriet, M.; Couzigou, P.; De Lédinghen, V. Prospective comparison of transient elastography, Fibrotest, APRI, and liver biopsy for the assessment of fibrosis in chronic hepatitis C. Gastroenterology 2005, 128, 343–350. [Google Scholar] [CrossRef]
- Wilson, E.M.P.; Sereti, I. Immune restoration after antiretroviral therapy: The pitfalls of hasty or incomplete repairs. Immunol. Rev. 2013, 254, 343–354. [Google Scholar] [CrossRef]
- d’Ettorre, G.; Ceccarelli, G.; Serafino, S.; Giustini, N.; Cavallari, E.N.; Bianchi, L.; Pavone, P.; Bellelli, V.; Turriziani, O.; Antonelli, G.; et al. Dominant enrichment of phenotypically activated CD38(+) HLA-DR(+) CD8(+) T cells, rather than CD38(+) HLA-DR(+) CD4(+) T cells, in HIV/HCV coinfected patients on antiretroviral therapy. J. Med. Virol. 2016, 88, 1347–1356. [Google Scholar] [CrossRef]
- Kuniholm, M.H.; Xie, X.; Anastos, K.; Kaplan, R.C.; Xue, X.; Kovacs, A.; Peters, M.G.; Seaberg, E.C.; French, A.L.; Young, M.A.; et al. Association of Chronic Hepatitis C Infection with T-Cell Phenotypes in HIV-Negative and HIV-Positive Women. J. Acquir. Immune Defic. Syndr. 2014, 67, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Medrano, L.M.; Garcia-Broncano, P.; Berenguer, J.; González-García, J.; Jiménez-Sousa, M.Á.; Guardiola, J.M.; Crespo, M.; Quereda, C.; Sanz, J.; Canorea, I.; et al. GESIDA 3603b Study Group. Elevated liver stiffness is linked to increased biomarkers of inflammation and immune activation in HIV/hepatitis C virus-coinfected patients. AIDS 2018, 32, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Alba, J.C.; Abrego-Peredo, A.; Gallardo-Hernández, C.; Pérez-Lara, J.; Santiago-Cruz, W.; Jiang, W.; Espinosa, E. HIV Disease Progression: Overexpression of the Ectoenzyme CD38 as a Contributory Factor? Bioessays 2019, 41, e1800128. [Google Scholar] [CrossRef]
- Cockerham, L.R.; Jain, V.; Sinclair, E.; Glidden, D.V.; Hartogenesis, W.; Hatano, H.; Hunt, P.W.; Martin, J.N.; Pilcher, C.D.; Sekaly, R.; et al. Programmed death-1 expression on CD4+ and CD8+ T cells in treated and untreated HIV disease. AIDS 2014, 28, 1749–1758. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.; Pantazis, N.; Martin, G.E.; Hickling, S.; Hurst, J.; Meyerowitz, J.; Willberg, C.B.; Robinson, N.; Brown, H.; Fisher, M.; et al. SPARTAC and CHERUB Investigators. Exhaustion of activated CD8 T cells predicts disease progression in primary HIV-1 infection. PLoS Pathog. 2016, 12, e1005661. [Google Scholar] [CrossRef]
- Rallón, N.; García, M.; García-Samaniego, J.; Cabello, A.; Álvarez, B.; Restrepo, C.; Nistal, S.; Górgolas, M.; Benito, J.M. Expression of PD-1 and Tim-3 markers of T-cell exhaustion is associated with CD4 dynamics during the course of untreated and treated HIV infection. PLoS ONE 2018, 13, e0193829. [Google Scholar] [CrossRef]
- Khaitan, A.; Unutmaz, D. Revisiting immune exhaustion during HIV infection. Curr. HIV/AIDS Rep. 2011, 8, 4–11. [Google Scholar] [CrossRef]
- Callendret, B.; Walker, C. Immune boost for viral hepatitis. Nat. Med. 2011, 17, 252–253. [Google Scholar] [CrossRef]
- López-Cortés, L.F.; Trujillo-Rodríguez, M.; Báez-Palomo, A.; Benmarzouk-Hidalgo, O.J.; Dominguez-Molina, B.; Milanés-Guisado, Y.; Espinosa, N.; Viciana, P.; Gutiérrez-Valencia, A. Eradication of Hepatitis C Virus (HCV) Reduces Immune Activation, Microbial Translocation, and the HIV DNA Level in HIV/HCV-Coinfected Patients. J. Infect. Dis. 2018, 218, 624–632. [Google Scholar] [CrossRef]
- Lin, W.; Weinberg, E.M.; Chung, R.T. Pathogenesis of accelerated fibrosis in HIV/HCV co-infection. J. Infect. Dis. 2013, 207, S13–S18. [Google Scholar] [CrossRef]
- Mastroianni, C.M.; Lichtner, M.; Mascia, C.; Zuccalà, P.; Vullo, V. Molecular mechanisms of liver fibrosis in HIV/HCV coinfection. Int. J. Mol. Sci. 2014, 15, 9184–9208. [Google Scholar] [CrossRef] [PubMed]
- Perazzo, H.; Veloso, V.G.; Grinsztejn, B.; Hyde, C.; Castro, R. Factors That Could Impact on Liver Fibrosis Staging by Transient Elastography. Int. J. Hepatol. 2015, 2015, 624596. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhu, M.; Cao, L.; Yao, M.; Lu, Y.; Wen, X. Liver Stiffness Measurement Can Reflect the Active Liver Necroinflammation in Population with Chronic Liver Disease: A Real-world Evidence Study. J. Clin. Transl. Hepatol. 2019, 7, 313–321. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | HIV Group (n = 25) | HIV/HCV Group (n = 25) | p-Value |
|---|---|---|---|
| Age (years) | 48 (42–55) | 44 (39–48) | 0.11 |
| Gender (% of males) | 88% | 100% | 0.24 |
| Time since HIV diagnosis (years) | 9 (6–14) | 7 (2–10) | 0.07 |
| Time since HCV diagnosis (years) | NA | 2 (1.5–5) | NA |
| Time on ART (years) | 5 (3.5–7.5) | 4 (2–9) | 0.63 |
| CD4 count (cells/μL) | 816 (605–992) | 735 (577–902) | 0.31 |
| Ratio CD4/CD8 | 0.84 (0.56–1.34) | 0.75 (0.60–1.09) | 0.49 |
| ALT level (IU/L) | 32 (24–37) | 74 (49–162) | <0.0001 |
| AST level (IU/L) | 27 (22–31) | 58 (37–122) | <0.0001 |
| GGT level (IU/L) | 36 (22–54) | 55 (25–119) | 0.06 |
| Total cholesterol level (mg/dL) | 194 (162–227) | 157 (125–177) | <0.0001 |
| HDL level (mg/dL) | 42 (37–50) | 46 (33–50) | 0.815 |
| LDL level (mg/dL) | 119 (93–146) | 85 (71–104) | 0.001 |
| HCV-RNA (log copies/mL) | NA | 6.1 (5.8–6.4) | NA |
| HIV transmission route (%) | 1 | ||
| Sexual | 100% | 96% | |
| Parenteral | 0% | 4% | |
| HCV genotype (%) | NA | ||
| 1a | NA | 60% | |
| 1b | NA | 12% | |
| 4 | NA | 28% | |
| Liver stiffness (measured by elastography) (%) | NA | ||
| <7.1 KPa | NA | 60% | |
| ≥7.1 KPa | NA | 40% | |
| DAA regimen | |||
| GZR/EBR | NA | 64% | |
| SOF/LDV | NA | 32% | |
| OBV/PTV/r/DSV | NA | 4% |
| T-Cell Subsets | Level of T-Cell Subsets Median [IQR] | p-Value * | |
|---|---|---|---|
| pre-DAAs HIV/HCV Coinfected Patients | HIV Monoinfected Patients | ||
| CD4+CD45RA+CCR7-PD1-TIM3+ | 0.91 (0.45–1.57) | 0.46 (0.27–0.74) | 0.076 |
| CD4+CD45RA+CCR7-CD38+HLADR- | 5.59 (3.84–8.83) | 3.29 (2.19–0.47) | 0.004 |
| CD8+CD45RA+CCR7-PD1+TIM3+ | 0.59 (0.31–1.25) | 0.29 (0.18–0.44) | 0.006 |
| CD8+CD45RA+CCR7-CD38+HLADR- | 1.41 (1.01–3.66) | 0.67 (0.39–0.91) | <0.0001 |
| T-Cell Subsets | Level of T-Cell Subsets Median [IQR] | p-Value * | |
|---|---|---|---|
| post-DAAs HIV/HCV Coinfected Patients | HIV Monoinfected Patients | ||
| CD8+CD45RA+CCR7-PD1+TIM3+ | 0.51 (0.23–0.99) | 0.29 (0.18–0.44) | 0.051 |
| CD8+CD45RA+CCR7-CD38+HLADR- | 1.20 (0.77–2.51) | 0.67 (0.39–1.58) | 0.003 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Restrepo, C.; Álvarez, B.; Valencia, J.L.; García, M.; Navarrete-Muñoz, M.A.; Ligos, J.M.; Cabello, A.; Prieto, L.; Nistal, S.; Montoya, M.; et al. Both HCV Infection and Elevated Liver Stiffness Significantly Impacts on Several Parameters of T-Cells Homeostasis in HIV-Infected Patients. J. Clin. Med. 2020, 9, 2978. https://doi.org/10.3390/jcm9092978
Restrepo C, Álvarez B, Valencia JL, García M, Navarrete-Muñoz MA, Ligos JM, Cabello A, Prieto L, Nistal S, Montoya M, et al. Both HCV Infection and Elevated Liver Stiffness Significantly Impacts on Several Parameters of T-Cells Homeostasis in HIV-Infected Patients. Journal of Clinical Medicine. 2020; 9(9):2978. https://doi.org/10.3390/jcm9092978
Chicago/Turabian StyleRestrepo, Clara, Beatriz Álvarez, José L Valencia, Marcial García, María A Navarrete-Muñoz, José M Ligos, Alfonso Cabello, Laura Prieto, Sara Nistal, María Montoya, and et al. 2020. "Both HCV Infection and Elevated Liver Stiffness Significantly Impacts on Several Parameters of T-Cells Homeostasis in HIV-Infected Patients" Journal of Clinical Medicine 9, no. 9: 2978. https://doi.org/10.3390/jcm9092978
APA StyleRestrepo, C., Álvarez, B., Valencia, J. L., García, M., Navarrete-Muñoz, M. A., Ligos, J. M., Cabello, A., Prieto, L., Nistal, S., Montoya, M., Górgolas, M., Rallón, N., & Benito, J. M. (2020). Both HCV Infection and Elevated Liver Stiffness Significantly Impacts on Several Parameters of T-Cells Homeostasis in HIV-Infected Patients. Journal of Clinical Medicine, 9(9), 2978. https://doi.org/10.3390/jcm9092978