The Use of 3D Titanium Miniplates in Surgical Treatment of Patients with Condylar Fractures




Abstract
:1. Introduction
2. Aim of the Study
3. Materials and Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Kozakiewicz, M. Classification proposal for fractures of the processus condylaris mandibulae. Clin. Oral Investig. 2018, 23, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neff, A.; Cornelius, C.-P.; Rasse, M.; Torre, D.D.; Audigé, L. The Comprehensive AOCMF Classification System: Condylar Process Fractures—Level 3 Tutorial. Craniomaxillofacial Trauma Reconstr. 2014, 7, 44–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loukota, R.; Eckelt, U.; De Bont, L.; Rasse, M. Subclassification of fractures of the condylar process of the mandible. Br. J. Oral Maxillofac. Surg. 2005, 43, 72–73. [Google Scholar] [CrossRef] [PubMed]
- Xiao-Dong, L.; Qiu-Xu, W.; Wei-Xian, L. Epidemiological pattern of maxillofacial fractures in northern China. Medicine 2020, 99, e19299. [Google Scholar] [CrossRef]
- Bhutia, D.P.; Singh, G.; Mohammed, S.; Ram, H.; Gamit, J.; Howlader, D. Prevalence and Etiology of Pediatric Maxillofacial Injuries: A Unicenter-based Retrospective Study. Int. J. Clin. Pediatr. Dent. 2019, 12, 528–531. [Google Scholar] [CrossRef]
- Sikora, M.; Olszowski, T.; Chlubek, D. Current views on the treatment of condylar fractures. Pomeranian J. Life Sci. 2018, 64, 14–23. [Google Scholar]
- Sikora, M.; Sielski, M.; Stąpor, A.; Chlubek, D. Use of the Delta plate for surgical treatment of patients with condylar fractures. J. Cranio-Maxillofac. Surg. 2016, 44, 770–774. [Google Scholar] [CrossRef]
- Sikora, M.; Olszowski, T.; Sielski, M.; Stąpor, A.; Janiszewska-Olszowska, J.; Chlubek, D. The use of the transparotid approach for surgical treatment of condylar fractures—Own experience. J. Craniomaxillofac. Surg. 2015, 43, 1961–1965. [Google Scholar] [CrossRef]
- Moin, A.; Shetty, A.D.; Archana, T.; Kale, S.G. Facial Nerve Injury in Temporomandibular Joint Approaches. Ann. Maxillofac. Surg. 2018, 8, 51–55. [Google Scholar] [CrossRef]
- Nussbaum, M.L.; Laskin, D.M.; Best, A.M. Closed Versus Open Reduction of Mandibular Condylar Fractures in Adults: A Meta-Analysis. J. Oral Maxillofac. Surg. 2008, 66, 1087–1092. [Google Scholar] [CrossRef]
- Shakya, S.; Zhang, X.; Liu, L. Key points in surgical management of mandibular condylar fractures. Chin. J. Traumatol. 2020, 23, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M.; Zieliński, R.; Konieczny, B.; Krasowski, M.; Okulski, J. Open Rigid Internal Fixation of Low-Neck Condylar Fractures of the Mandible: Mechanical Comparison of 16 Plate Designs. Materials 2020, 13, 1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zieliński, R.; Kozakiewicz, M.; Konieczny, B.; Krasowski, M.; Okulski, J. Mechanical Evaluation of Titanium Plates for Osteoesynthesis High Neck Condylar Fracture of Mandible. Materials 2020, 13, 592. [Google Scholar] [CrossRef] [Green Version]
- Pappachan, B.; Agrawal, R. Comparison of two L shaped Plate on Plate Versus Single Conventional L Miniplate in Fixation of Subcondylar Mandibular Fractures. J. Maxillofac. Oral Surg. 2018, 18, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, S.; Galinde, J.; Asnani, U.; Mistry, Y.A. Comparative Evaluation of Clinical Outcomes Using Delta Plates and Conventional Miniplates for Internal Fixation of Mandibular Condylar Fractures in Adults. J. Oral Maxillofac. Surg. 2018, 76, 1255–1266. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M.; Zieliński, R.; Krasowski, M.; Okulski, J. Forces Causing One-Millimeter Displacement of Bone Fragments of Condylar Base Fractures of the Mandible after Fixation by All Available Plate Designs. Materials 2019, 12, 3122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albogha, M.H.; Mori, Y.; Takahashi, I. Three-dimensional titanium miniplates for fixation of subcondylar mandibular fractures: Comparison of five designs using patient-specific finite element analysis. J. Cranio-Maxillofac. Surg. 2018, 46, 391–397. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Swiniarski, J. “A” shape plate for open rigid internal fixation of mandible condyle neck fracture. J. Cranio-Maxillofac. Surg. 2014, 42, 730–737. [Google Scholar] [CrossRef]
- Zieliński, R.; Kozakiewicz, M.; Swiniarski, J. Comparison of Titanium and Bioresorbable Plates in “A” Shape Plate Properties-Finite Element Analysis. Materials 2019, 12, 1110. [Google Scholar] [CrossRef] [Green Version]
- McLeod, N.; Van Gijn, D. Use of ultrasound-activated resorbable sheets and pins in the management of fractures of the condylar neck of the mandible: A case series. Br. J. Oral Maxillofac. Surg. 2018, 56, 182–185. [Google Scholar] [CrossRef]
- Sikora, M.; Baranowska-Bosiacka, I.; Goschorska, M.; Chlubek, D. In vitro effect of three-dimensional (3D) titanium mini-plate systems used for surgical treatment of condylar fractures on interleukin 1 (IL-1) and interleukin 6 (IL-6) concentration in THP-1 macrophages. Tissue Cell 2020, 67, 101404. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Baranowska-Bosiacka, I.; Lukomska, A.; Goschorska, M.; Chlubek, D. Expression of metalloproteinase 2 (MMP-2) and metalloproteinase 9 (MMP-9) in THP-1 macrophages cultured with three-dimensional titanium mini-plate systems used for surgical treatment of condylar fractures. Acta Biochim. Pol. 2019, 66, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Goschorska, M.; Baranowska-Bosiacka, I.; Chlubek, D. In Vitro Effect of 3D Plates Used for Surgical Treatment of Condylar Fractures on Prostaglandin E2 (PGE2) and Thromboxane B2 (TXB2) Concentration in THP-1 Macrophages. Int. J. Mol. Sci. 2017, 18, 2638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aquilina, P.; Parr, W.C.H.; Chamoli, U.; Wroe, S. Finite Element Analysis of Patient-Specific Condyle Fracture Plates: A Preliminary Study. Craniomaxillofacial Trauma Reconstr. 2015, 8, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilde, F.; Cornelius, C.-P.; Schramm, A. Computer-Assisted Mandibular Reconstruction using a Patient-Specific Reconstruction Plate Fabricated with Computer-Aided Design and Manufacturing Techniques. Craniomaxillofacial Trauma Reconstr. 2014, 7, 158–166. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Li, Z.; Ren, J.; He, M.; Huang, Y.; Tian, W.; Tang, W. Digital diagnosis and treatment of mandibular condylar fractures based on Extensible Neuro imaging Archive Toolkit (XNAT). PLoS ONE 2018, 13, e0192831. [Google Scholar] [CrossRef]
- Krzewski, S.; Baranowski, M.; Zubrzycki, R.; Stachurski, M.; Borowicz, J. Correlation between temporomandibular joint dysfunction and Eichner classification. J. Educ. Heal. Sport 2020, 10, 155. [Google Scholar] [CrossRef]
- Song, I.; Vong, J.; Yen, N.Y.; Diederich, J.; Yellowlees, P. Profiling Bell’s Palsy based on House-Brackmann Score. J. Artif. Intell. Soft Comput. Res. 2013, 3, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Yang, H.; Han, L. Open versus closed treatment for unilateral mandibular extra-capsular condylar fractures: A meta-analysis. J. Cranio-Maxillofac. Surg. 2019, 47, 1110–1119. [Google Scholar] [CrossRef]
- Schneider, M.; Erasmus, F.; Gerlach, K.L.; Kuhlisch, E.; Loukota, R.; Rasse, M.; Schubert, J.; Terheyden, H.; Eckelt, U. Open Reduction and Internal Fixation Versus Closed Treatment and Mandibulomaxillary Fixation of Fractures of the Mandibular Condylar Process: A Randomized, Prospective, Multicenter Study With Special Evaluation of Fracture Level. J. Oral Maxillofac. Surg. 2008, 66, 2537–2544. [Google Scholar] [CrossRef]
- Louvrier, A.; Barrabé, A.; Weber, E.; Chatelain, B.; Sigaux, N.; Meyer, C.; Aurélien, L.; Aude, B.; Elise, W.; Brice, C.; et al. The high sub-mandibular approach: Our experience about 496 procedures. J. Stomatol. Oral Maxillofac. Surg. 2020, 20, 2468–7855. [Google Scholar] [CrossRef] [PubMed]
- Smolka, W.; Liokatis, P.; Cornelius, C.-P. Open Reduction and Internal Fixation of Unilateral Mandibular Condylar Base and Neck Fractures Using a Lambda Plate: Selection Criteria for Application. J. Oral Maxillofac. Surg. 2020, 78, 979–985. [Google Scholar] [CrossRef]
- Lechler, C.; Probst, F.; Cornelius, C.-P.; Smolka, W. Open Reduction and Internal Fixation of Mandibular Condylar Base and Neck Fractures Using Strut Plates. J. Oral Maxillofac. Surg. 2018, 76, 1494–1503. [Google Scholar] [CrossRef] [PubMed]
- Asim, M.A.; Ibrahim, M.W.; Javed, M.U.; Zahra, R.; Qayyum, M.U. Functional Outcomes of Open Versus Closed Treatment Of Unilateral Mandibular Condylar Fractures. J. Ayub Med. Coll. Abbottabad: JAMC 2019, 31, 67–71. [Google Scholar] [PubMed]
- Anehosur, V.; Kulkarni, K.; Shetty, S.; Kumar, N.; Shetty, S. Clinical outcomes of endoscopic vs retromandibular approach for the treatment of condylar fractures—A randomized clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 479–484. [Google Scholar] [CrossRef]
- Yang, L.; Patil, P.M. The retromandibular transparotid approach to mandibular subcondylar fractures. Int. J. Oral Maxillofac. Surg. 2012, 41, 494–499. [Google Scholar] [CrossRef]
- Haim, D.; Müller, A.; Leonhardt, H.; Nowak, A.; Richter, G.; Lauer, G. Biomechanical Study of the Delta Plate and the TriLock Delta Condyle Trauma Plate. J. Oral Maxillofac. Surg. 2011, 69, 2619–2625. [Google Scholar] [CrossRef]
- Rai, A. Comparison of single vs double noncompression miniplates in the management of subcondylar fracture of the mandible. Ann. Maxillofac. Surg. 2012, 2, 141–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauer, G.; Pradel, W.; Schneider, M.; Eckelt, U. A New 3-Dimensional Plate for Transoral Endoscopic-Assisted Osteosynthesis of Condylar Neck Fractures. J. Oral Maxillofac. Surg. 2007, 65, 964–971. [Google Scholar] [CrossRef]
- Zrounba, H.; Lutz, J.-C.; Zink, S.; Wilk, A. Epidemiology and treatment outcome of surgically treated mandibular condyle fractures. A five years retrospective study. J. Cranio-Maxillofac. Surg. 2014, 42, 879–884. [Google Scholar] [CrossRef]
- Yang, W.-G.; Chen, C.-T.; Tsay, P.-K.; Chen, Y.-R. Functional Results of Unilateral Mandibular Condylar Process Fractures after Open and Closed Treatment. J. Trauma: Inj. Infect. Crit. Care 2002, 52, 498–503. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Qualification Criteria |
|---|
| (1) Fracture in the anatomical region of the base and/or neck of the condyle of the mandible according to the AOCMF Classification System [2] (2) At least one of the following criteria: (a) presence of occlusal disorders (b) reduction of the vertical dimension of the mandible ramus by at least 4 mm due to displacement and overlapping of fragments (c) comminuted fracture (d) dislocation of the condyle in the temporomandibular joint (e) no contact between bone fragments (3) Age greater than or equal to 18 years |
| General Exclusion Criteria |
|---|
| (1) Lack of patient’s consent to open treatment (2) Contraindications for treatment under general anesthesia expressed in categories IV–VI on the ASA Physical Status Classification System scale |
| Local Exclusion Criteria |
| Mandibular head fracture according to the AOCMF Classification System [2]—the course of any fragment of the fracture line above the reference line of the head of the mandible |
| Patient Number | |
|---|---|
| Medical Interview | |
| Sex | Male/Female |
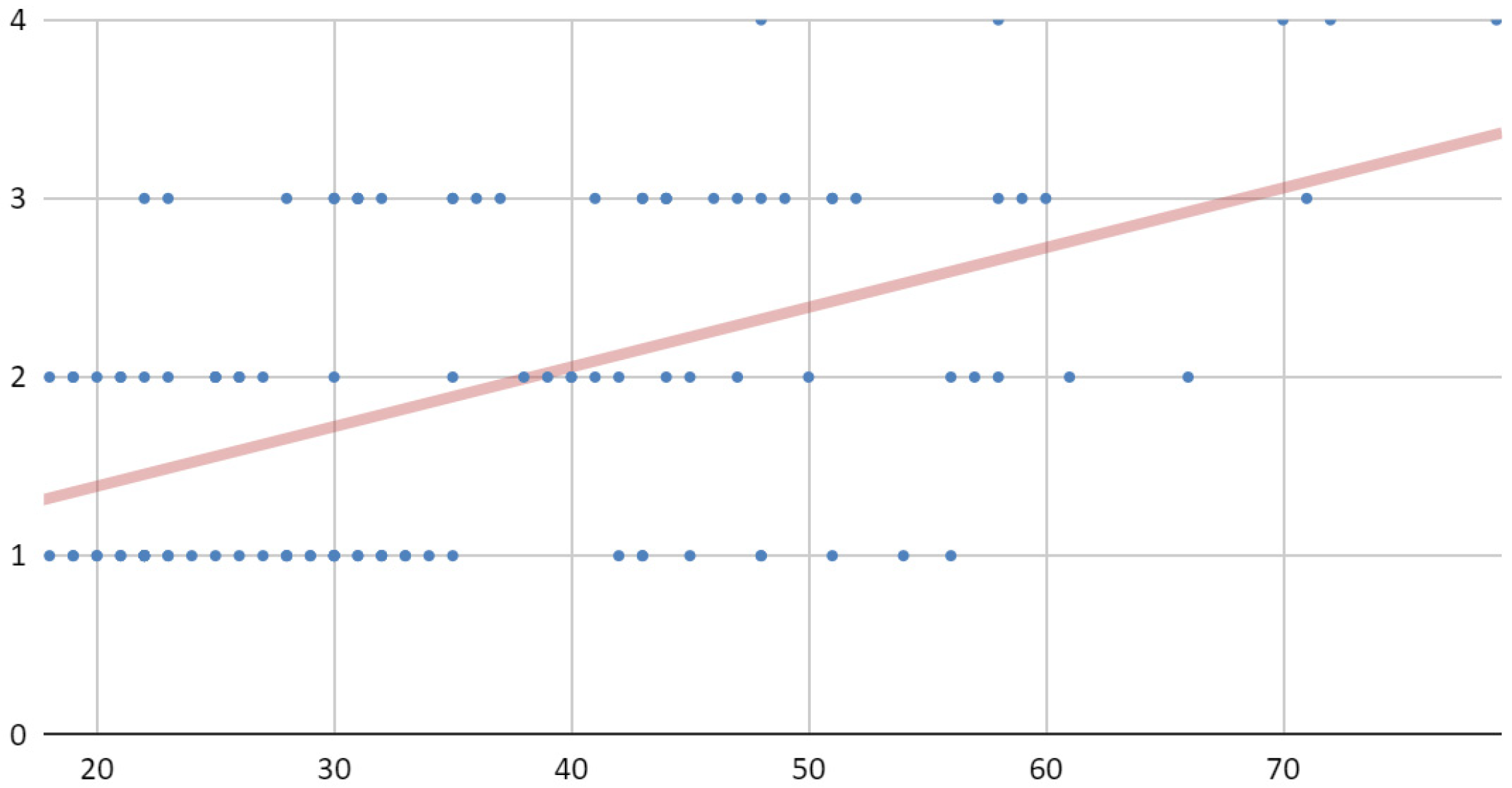
| Age | ... |
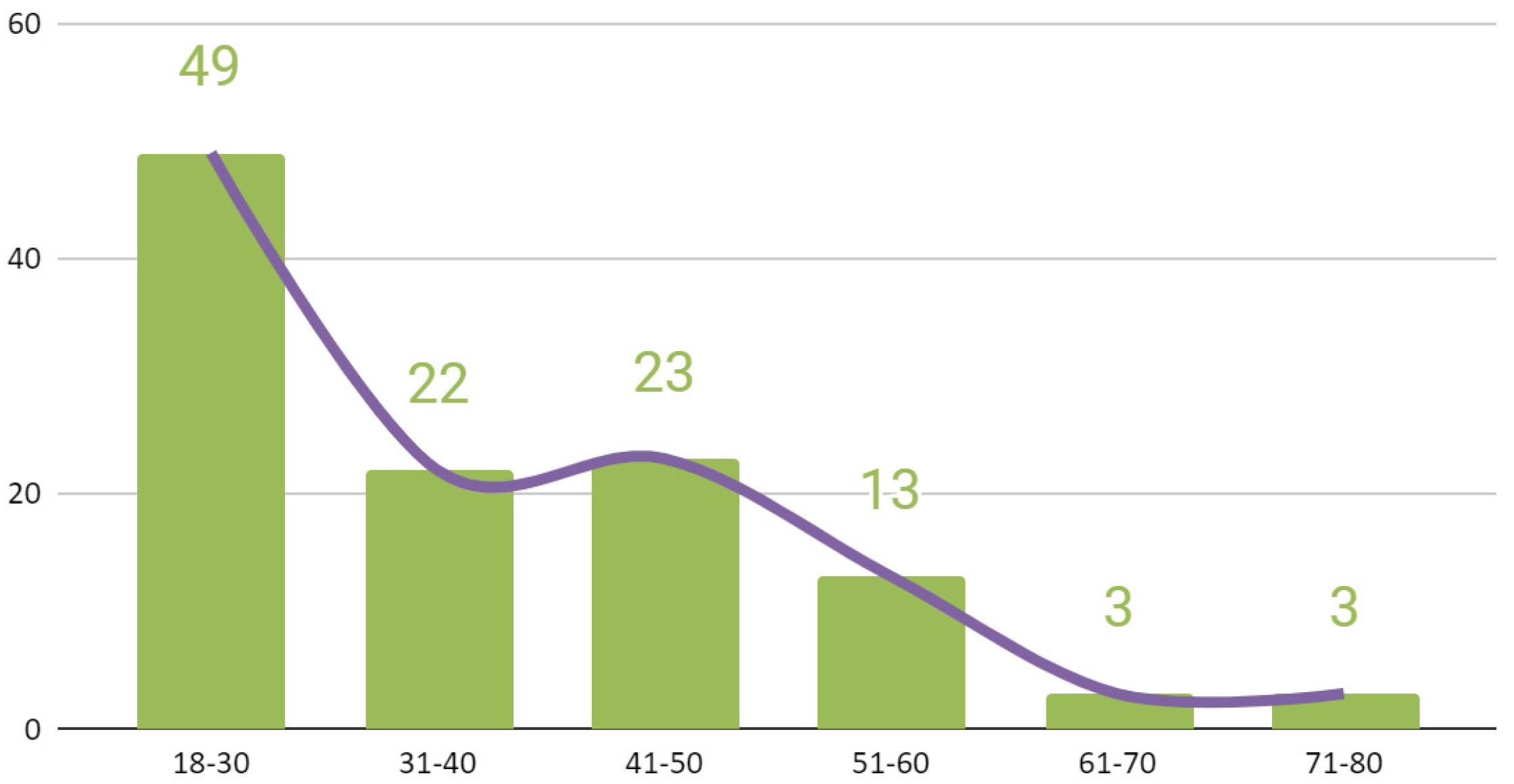
| Age range | 18–30/31–40/41–50/51–60/61–70/71–80 |
| Residence | Village and town below 20 k/Medium town from 20 k to 100 k/Big city over 100 k |
| Tobacco use | Not applicable/Up to 10 cigarettes a day/11–20 cigarettes a day/More than 20 cigarettes a day |
| Alcohol consumption | Not applicable/Occasionally (less than once a week)/Frequently (1–3 times a week)/Alcohol dependence (more than 3 times a week) |
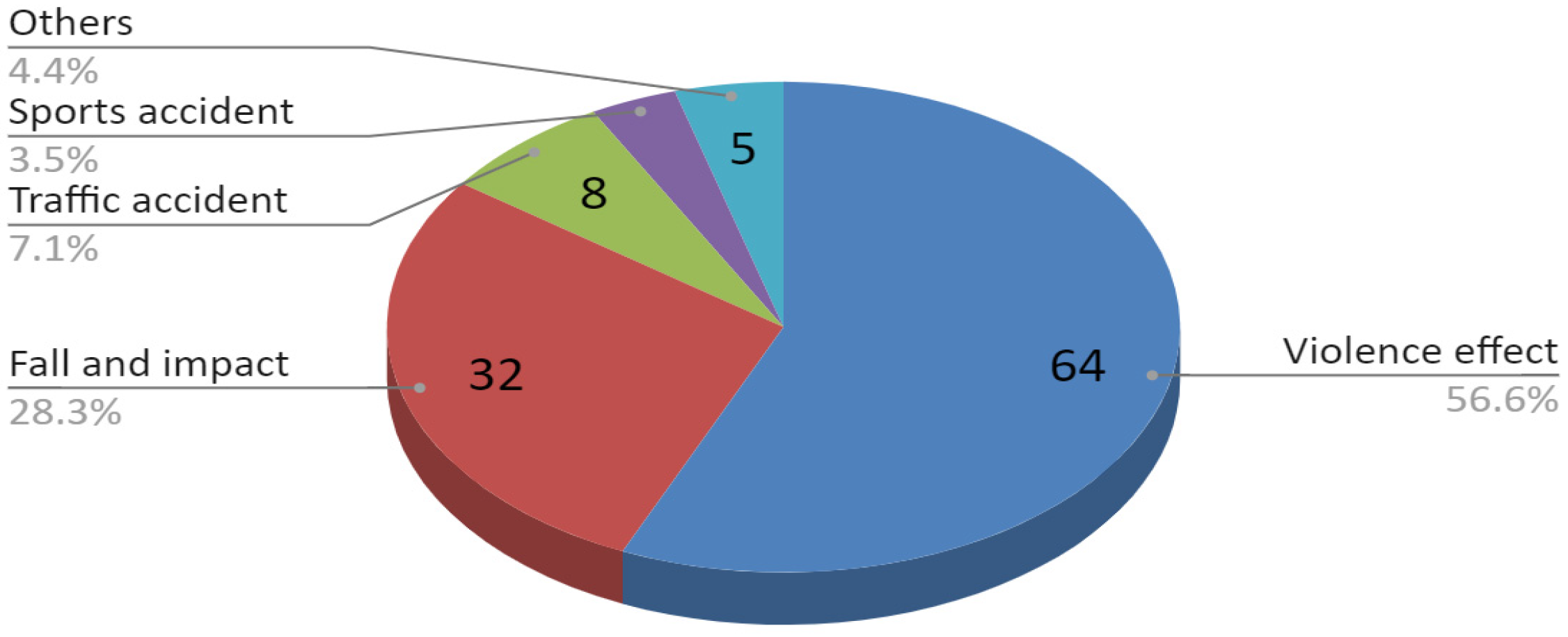
| Cause of injury | Violence effect/Fall and impact/Traffic accident/Sports accident/Others |
| Time from trauma to surgery, days | ... |
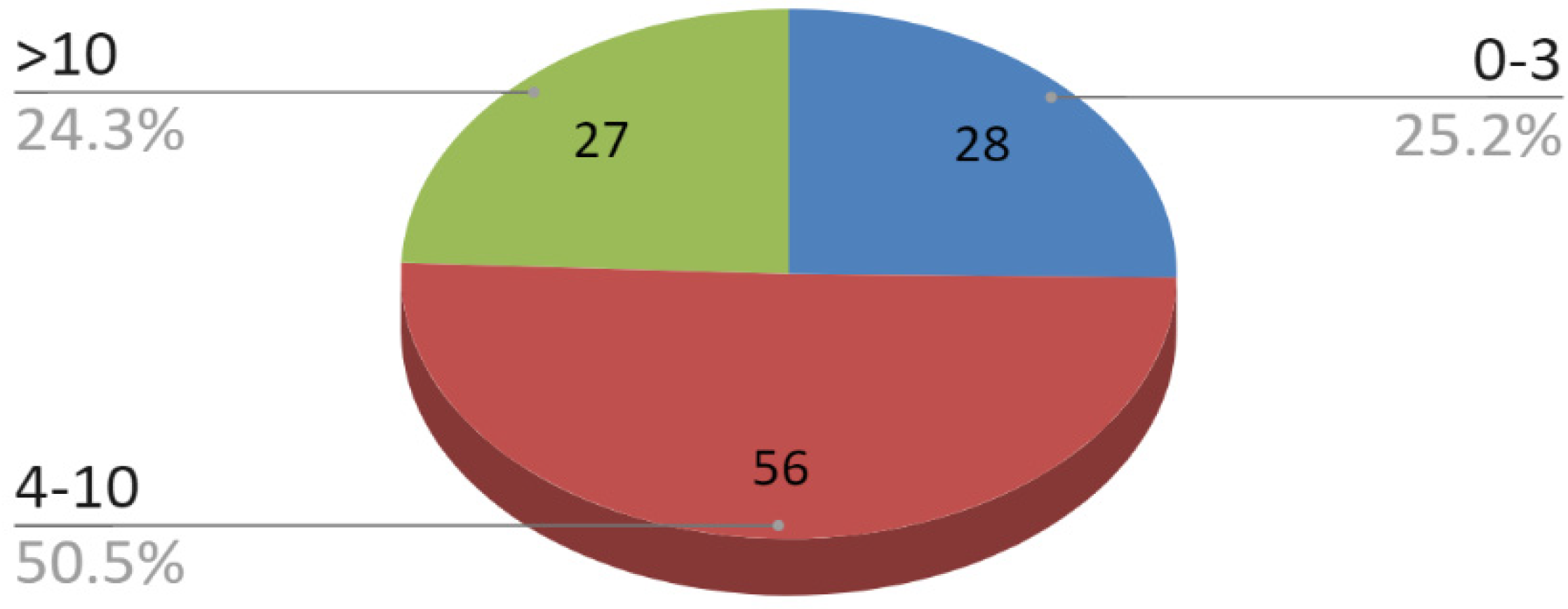
| Time range from trauma to surgery | Up to 3 days/4–10 days/More than 10 days |
| Clinical Examination | |
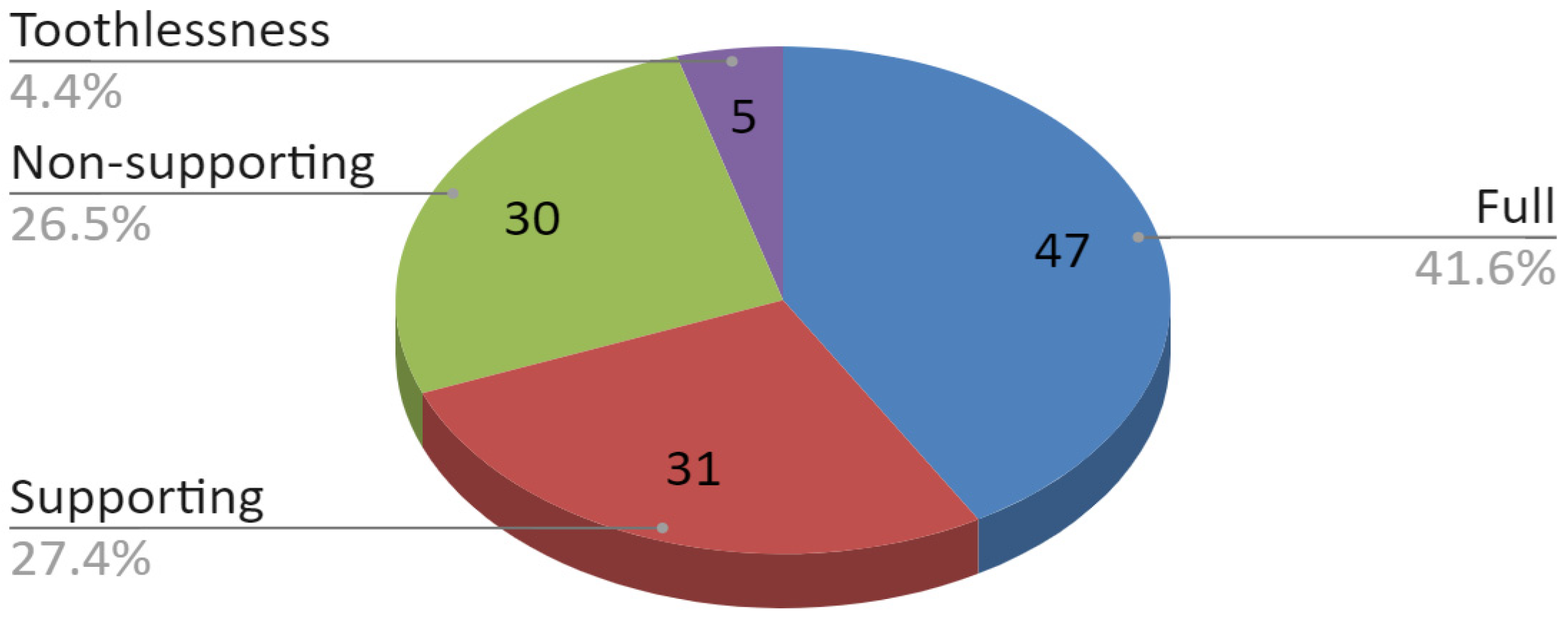
| Classification of missing teeth according to Eichner [27] | Full dental arches (A1)/Supporting zones preserved (A2, A3)/Missing supporting zones (B1, B2, B3, B4, C1, C2)/Toothlessness (C3) |
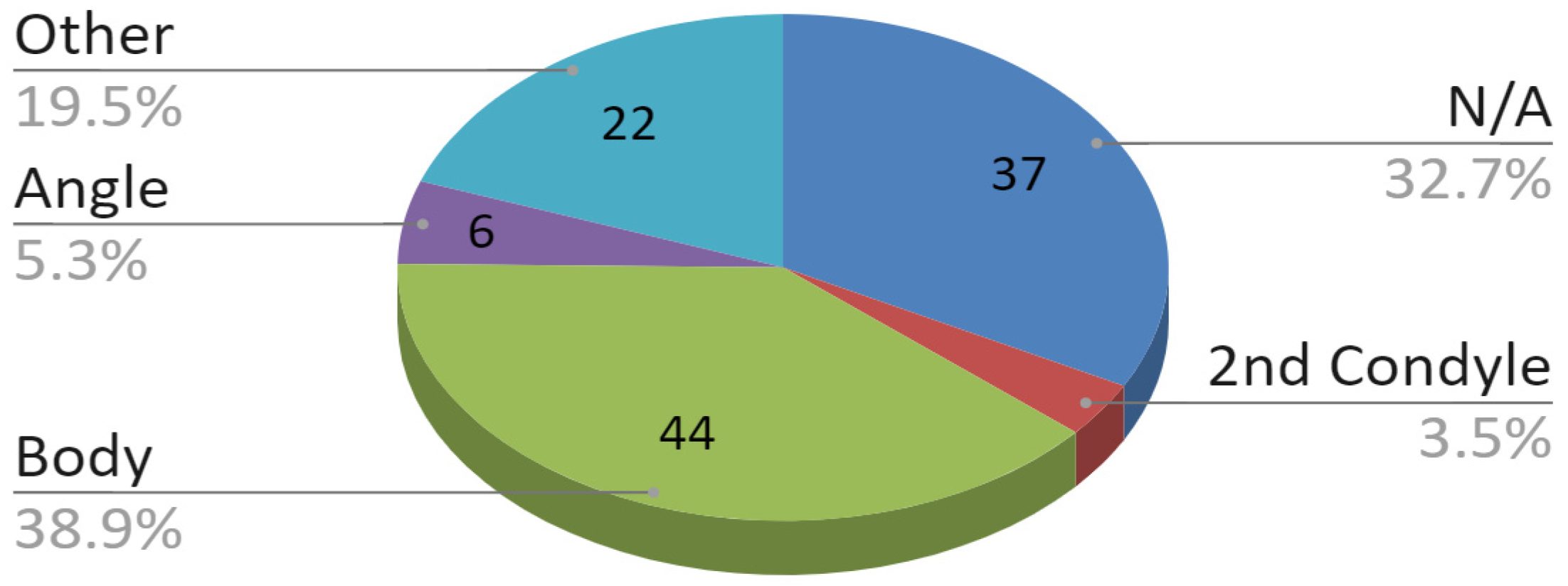
| Coexisting mandibular fracture | Not applicable/Opposite condylar process/Mandibular angle/Mandibular body/Other mandibular fracture |
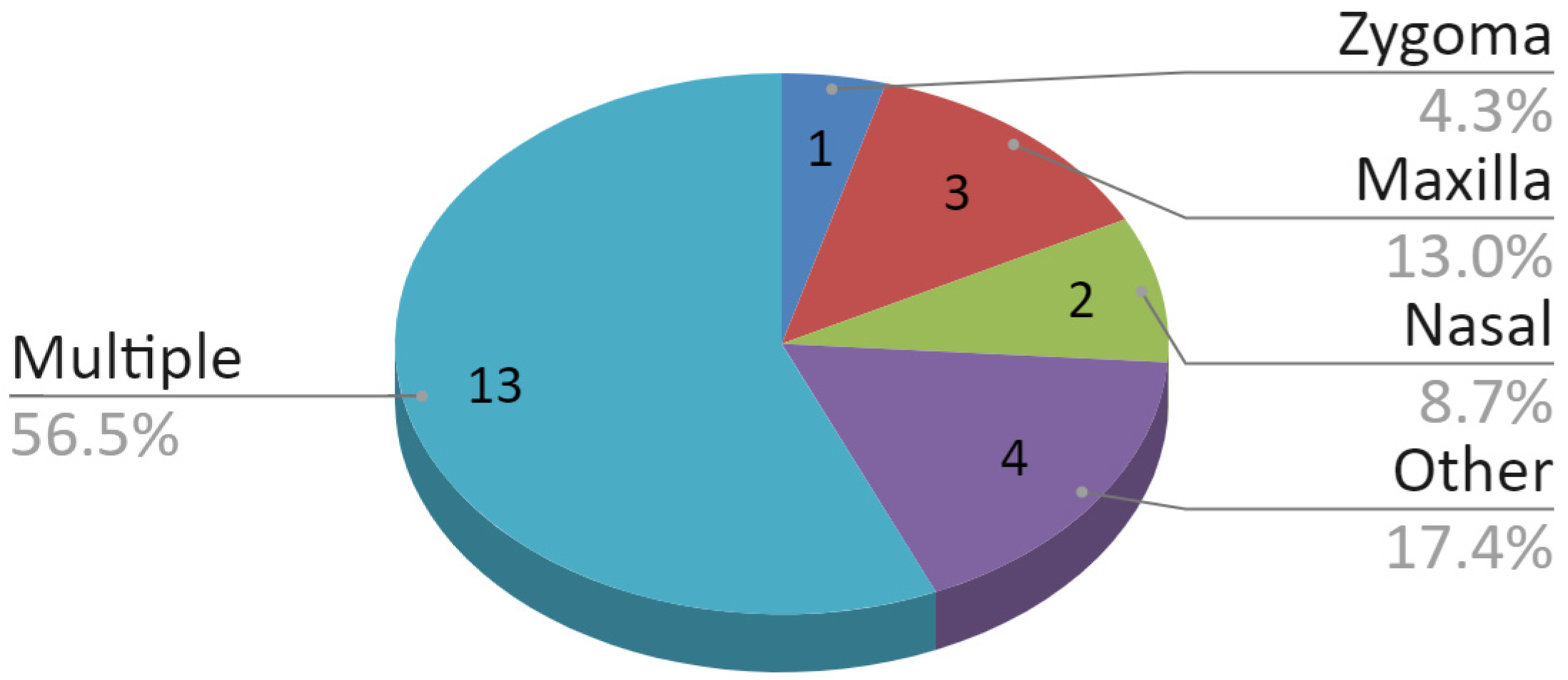
| Coexisting fracture of other facial bones | Not applicable/Zygomatic bone/Maxilla/Nasal skeleton/Other location/Fractures of multiple bones |
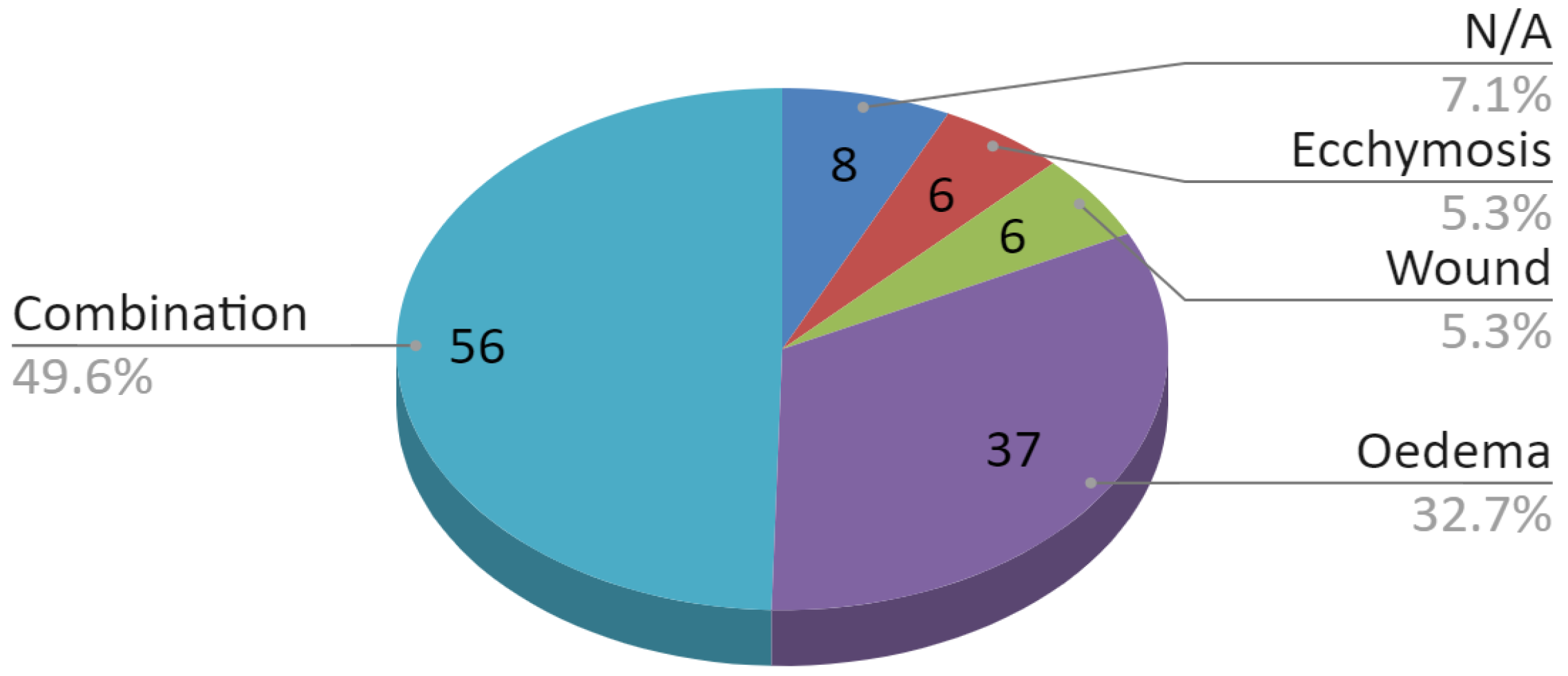
| Coexisting soft tissue injuries | Not applicable/Ecchymosis/Wound/Oedema/Combination of the above |
| Type of condylar fracture | Simple/Comminuted |
| Localization of the condylar fracture | Condylar base/Lower portion of the condylar neck |
| Displacement of bone fragments | No/Yes |
| Dislocation in the temporomandibular joint | No/Yes |
| 4-DCCP | 4-TCP | 9-TCP |
|---|---|---|
| 4-hole Delta Condyle Compression Plate | 4-hole Trapezoid Condyle Plate | 9-hole Trapezoid Condyle Plate |
| Medartis Modus 2.0 M-4894 | Medartis Modus 2.0 M-4852 or M-4854 | Medartis Modus 2.0 M-4858 or M-4860 |
 |  |  |
| Material: Titanium ASTM F67 Elasticity: Semi-rigid Plate thickness: 1.0 mm | ||
| Hospitalization | |
|---|---|
| Surgical approach | Intraoral/Retromandibular transparotid/Submandibular |
| 3D plate used | 4-DCCP/4-TCP/9-TCP/more than one plate |
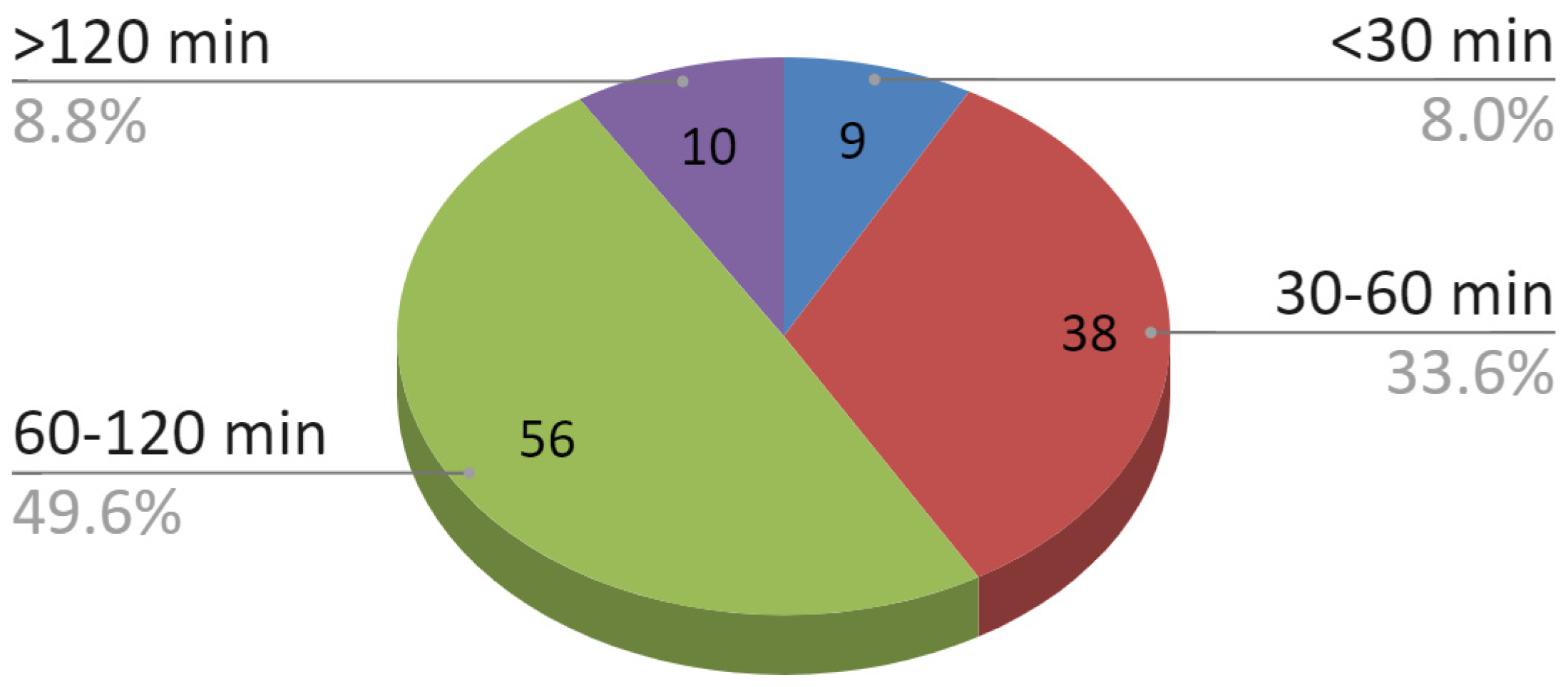
| Duration range of the operation | Less than 30 min/30–60 min/60–120 min/More than 120 min |
| Hospitalization time range | 1–3 days/4–10 days/More than 10 days |
| Outpatient Control After 6 Months | |
| Assessment of facial nerve dysfunction according to House and Brackmann scale [28] | Normal function (I)/Mild dysfunction (II)/Moderate dysfunction (III)/Moderately severe dysfunction (IV)/Severe dysfunction (V)/Total paralysis (VI) |
| Interincisal mouth opening, mm | ... |
| Plate breakage | Yes/No |
| Screw loosening | Yes/No |
| Malocclusion | Yes/No |
| Temporomandibular joints disorders (i.e., clicking) | Not applicable/Transient (up to 6 months)/Persistent (over 6 months) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikora, M.; Chęciński, M.; Sielski, M.; Chlubek, D. The Use of 3D Titanium Miniplates in Surgical Treatment of Patients with Condylar Fractures. J. Clin. Med. 2020, 9, 2923. https://doi.org/10.3390/jcm9092923
Sikora M, Chęciński M, Sielski M, Chlubek D. The Use of 3D Titanium Miniplates in Surgical Treatment of Patients with Condylar Fractures. Journal of Clinical Medicine. 2020; 9(9):2923. https://doi.org/10.3390/jcm9092923
Chicago/Turabian StyleSikora, Maciej, Maciej Chęciński, Marcin Sielski, and Dariusz Chlubek. 2020. "The Use of 3D Titanium Miniplates in Surgical Treatment of Patients with Condylar Fractures" Journal of Clinical Medicine 9, no. 9: 2923. https://doi.org/10.3390/jcm9092923
APA StyleSikora, M., Chęciński, M., Sielski, M., & Chlubek, D. (2020). The Use of 3D Titanium Miniplates in Surgical Treatment of Patients with Condylar Fractures. Journal of Clinical Medicine, 9(9), 2923. https://doi.org/10.3390/jcm9092923