Effect of CYP3A5 on the Once-Daily Tacrolimus Conversion in Stable Liver Transplant Patients

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
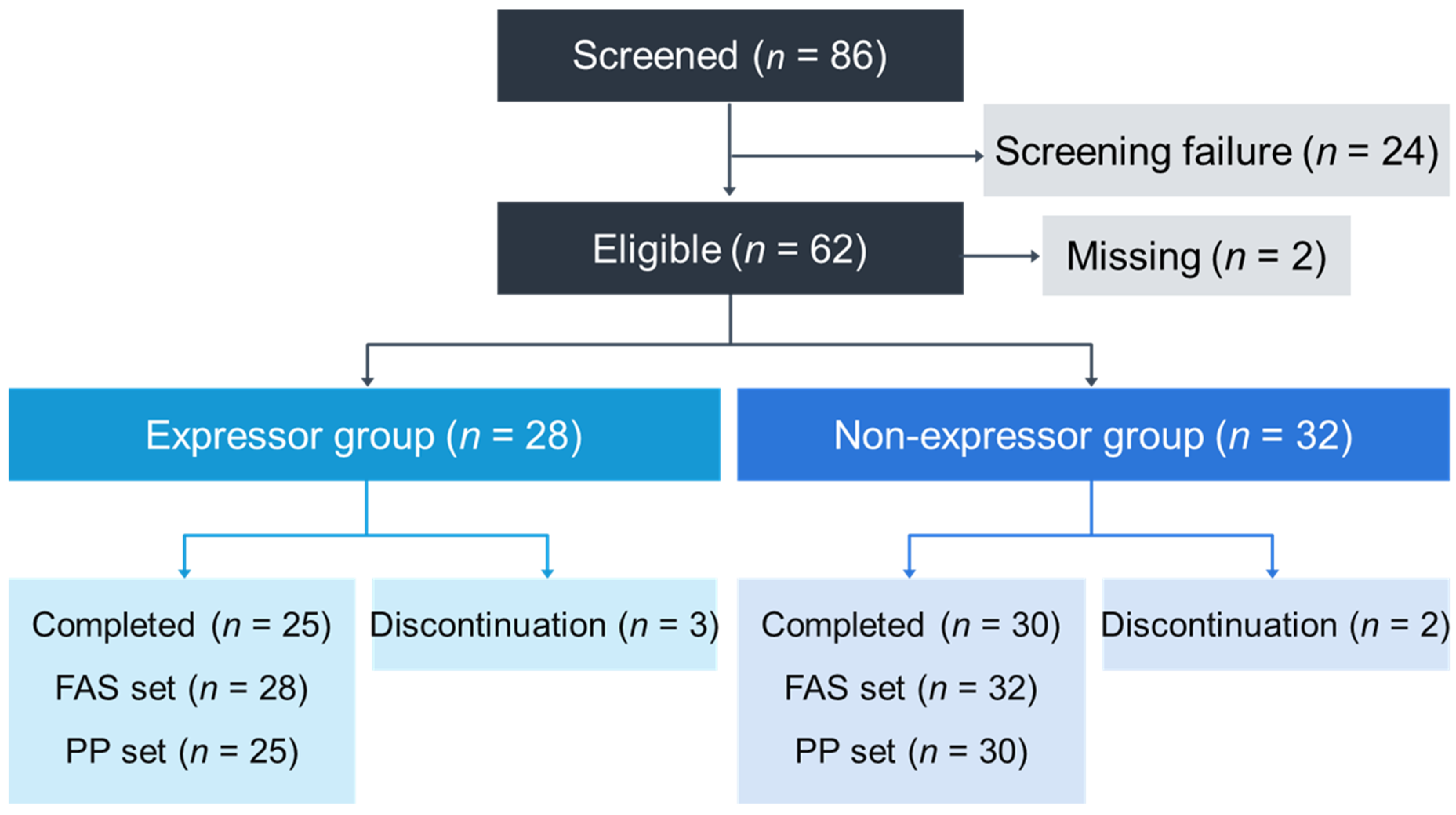
2.1. Study Design
2.2. Patients
2.3. Tacrolimus Concentrations
2.4. Genotyping of Cytochrome P450 3A5
2.5. Immunosuppression
2.6. Endpoints
2.7. Pharmacokinetic Analysis
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Efficacy
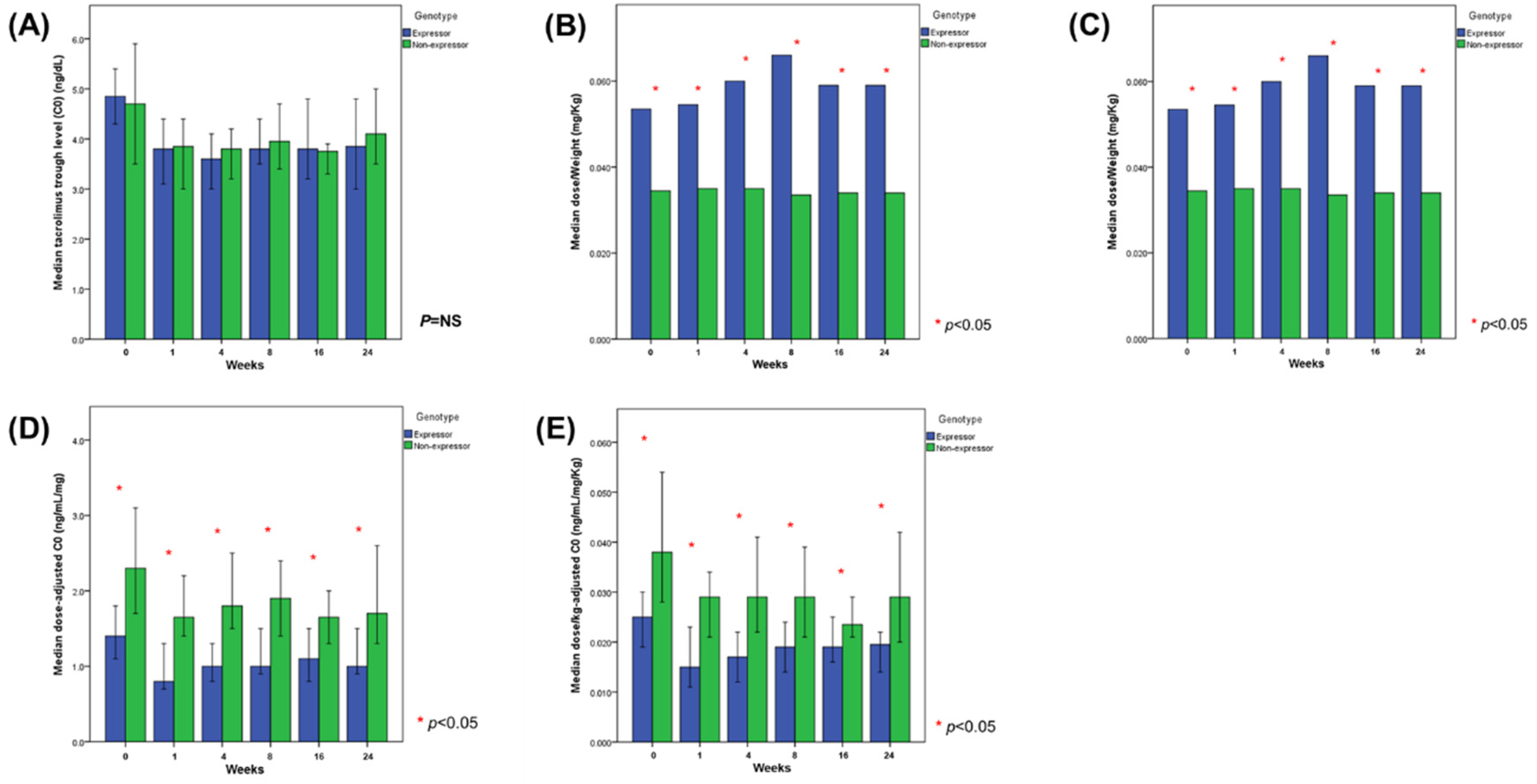
3.3. Tacrolimus Dose Adjustments after the Conversion
3.4. Tacrolimus Exposure before and after the Conversion
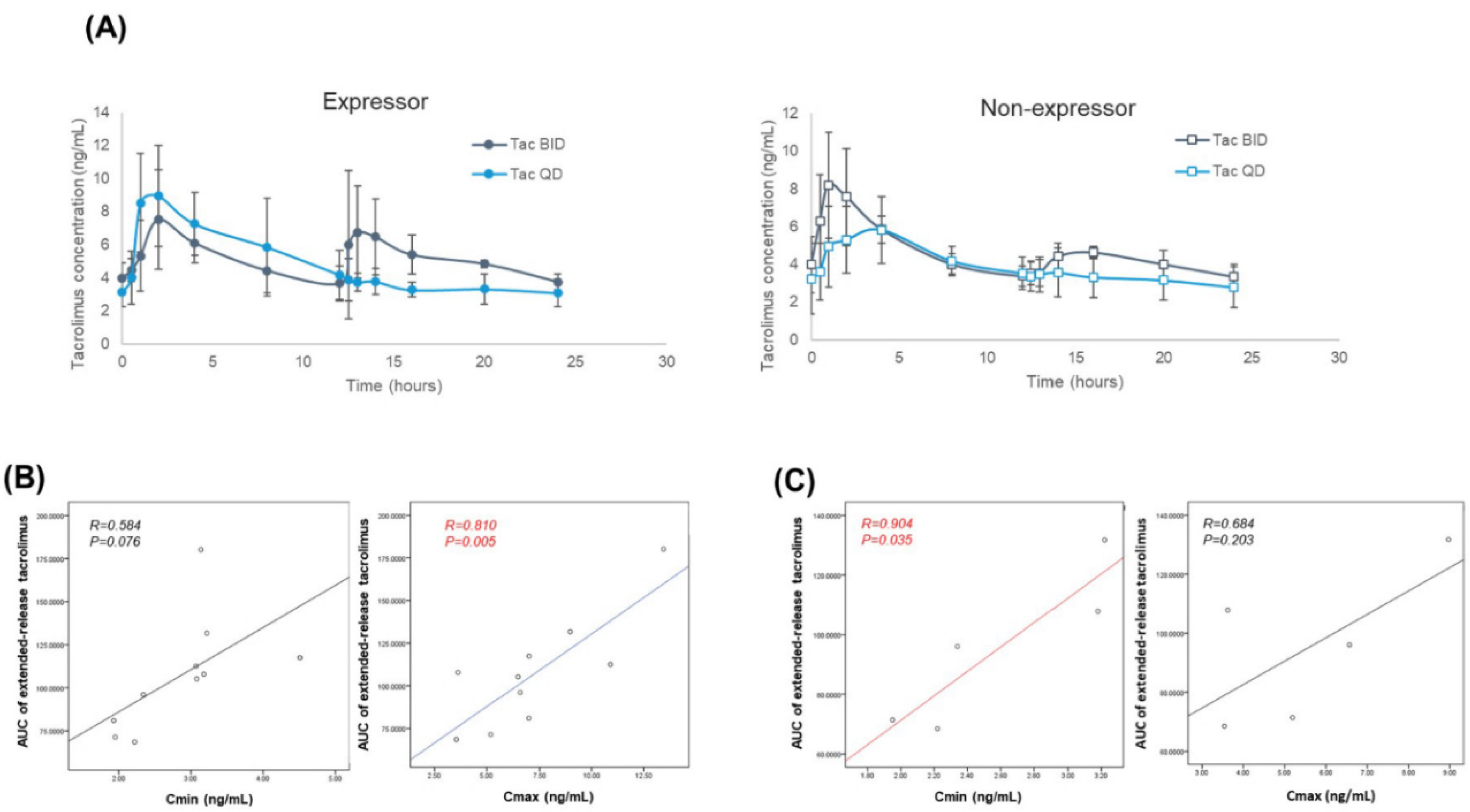
3.5. Pharmacokinetics before and after the Conversion
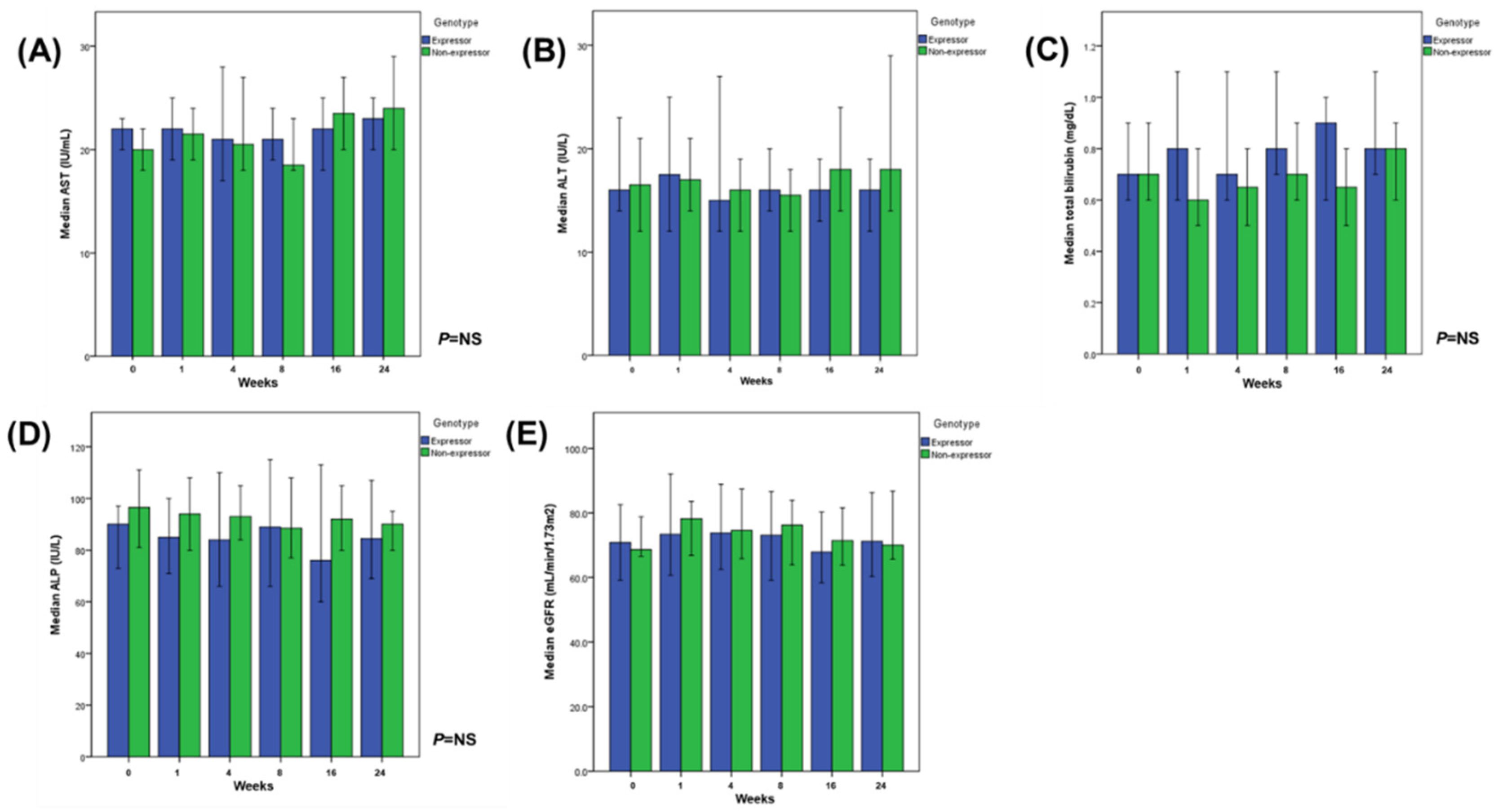
3.6. Safety
4. Discussion
5. Conclusions
6. Patents
Author Contributions
Funding
Conflicts of Interest
References
- U.S. Multicenter FK506 Liver Study Group. A comparison of tacrolimus (FK 506) and cyclosporine for immunosuppression in liver transplantation. N. Engl. J. Med. 1994, 331, 1110–1115. [Google Scholar] [CrossRef] [PubMed]
- Kuypers, D.R.J. Intra-Patient Variability of tacrolimus exposure in solid organ transplantation: A novel marker for clinical outcome. Clin. Pharmacol. Ther. 2019, 107, 347–358. [Google Scholar] [CrossRef] [PubMed]
- Brunet, M.; van Gelder, T.; Asberg, A.; Haufroid, V.; Hesselink, D.A.; Langman, L.; Lemaitre, F.; Marquet, P.; Seger, C.; Shipkova, M.; et al. Therapeutic Drug Monitoring of Tacrolimus-Personalized Therapy: Second Consensus Report. Ther. Drug Monit. 2019, 41, 261–307. [Google Scholar] [CrossRef] [PubMed]
- Schutte-Nutgen, K.; Tholking, G.; Suwelack, B.; Reuter, S. Tacrolimus—Pharmacokinetic Considerations for Clinicians. Curr. Drug Metab. 2018, 19, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Hendijani, F.; Azarpira, N.; Kaviani, M. Effect of CYP3A5*1 expression on tacrolimus required dose after liver transplantation: A systematic review and meta-analysis. Clin. Transplant. 2018, 32, e13306. [Google Scholar] [CrossRef]
- Loh, P.T.; Lou, H.X.; Zhao, Y.; Chin, Y.M.; Vathsala, A. Significant impact of gene polymorphisms on tacrolimus but not cyclosporine dosing in Asian renal transplant recipients. Transplant. Proc. 2008, 40, 1690–1695. [Google Scholar] [CrossRef]
- Ji, E.; Kim, M.G.; Oh, J.M. CYP3A5 genotype-based model to predict tacrolimus dosage in the early postoperative period after living donor liver transplantation. Ther. Clin. Risk Manag. 2018, 14, 2119–2126. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Prasad, G.V.R. CYP3A5 polymorphisms in renal transplant recipients: Influence on tacrolimus treatment. Pharmgenom. Pers. Med. 2018, 11, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Min, S.I.; Kim, S.Y.; Ahn, S.H.; Min, S.K.; Kim, S.H.; Kim, Y.S.; Moon, K.C.; Oh, J.M.; Kim, S.J.; Ha, J. CYP3A5 *1 allele: Impacts on early acute rejection and graft function in tacrolimus-based renal transplant recipients. Transplantation 2010, 90, 1394–1400. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, S.D.; Kim, Y.K.; Park, S.J. Conversion of twice-daily to once-daily tacrolimus is safe in stable adult living donor liver transplant recipients. Hepatobiliary Pancreat. Dis. Int. 2015, 14, 374–379. [Google Scholar] [CrossRef]
- Kim, J.M.; Kwon, C.H.; Joh, J.W.; Sinn, D.H.; Lee, S.; Choi, G.S.; Lee, S.K. Conversion of once-daily extended-release tacrolimus is safe in stable liver transplant recipients: A randomized prospective study. Liver Transpl. 2016, 22, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suh, S.W.; Lee, K.W.; Jeong, J.; Kim, H.; Yi, N.J.; Suh, K.S. Risk Factors for the Adverse Events after Conversion from Twice-Daily to Once-Daily Tacrolimus in Stable Liver Transplantation Patients. J. Korean Med. Sci. 2016, 31, 1711–1716. [Google Scholar] [CrossRef] [PubMed]
- Kwo, P.Y.; Cohen, S.M.; Lim, J.K. ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries. Am. J. Gastroenterol. 2017, 112, 18–35. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.G.; Kim, J.H. Central limit theorem: The cornerstone of modern statistics. Korean J. Anesthesiol. 2017, 70, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Demetris, A.J.; Bellamy, C.; Hubscher, S.G.; O’Leary, J.; Randhawa, P.S.; Feng, S.; Neil, D.; Colvin, R.B.; McCaughan, G.; Fung, J.J.; et al. 2016 Comprehensive Update of the Banff Working Group on Liver Allograft Pathology: Introduction of Antibody-Mediated Rejection. Am. J. Transplant. 2016, 16, 2816–2835. [Google Scholar] [CrossRef] [PubMed]
- Demetris, A.; Adams, D.; Bellamy, C.; Blakolmer, K.; Clouston, A.; Dhillon, A.P.; Fung, J.; Gouw, A.; Gustafsson, B.; Haga, H.; et al. Update of the International Banff Schema for Liver Allograft Rejection: Working recommendations for the histopathologic staging and reporting of chronic rejection. An International Panel. Hepatology 2000, 31, 792–799. [Google Scholar]
- Iwasaki, M.; Yano, I.; Fukatsu, S.; Hashi, S.; Yamamoto, Y.; Sugimoto, M.; Fukudo, M.; Masuda, S.; Nakagawa, S.; Yonezawa, A.; et al. Pharmacokinetics and Pharmacodynamics of Once-Daily Tacrolimus Compared With Twice-Daily Tacrolimus in the Early Stage After Living Donor Liver Transplantation. Ther. Drug Monit. 2018, 40, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Fischer, L.; Trunecka, P.; Gridelli, B.; Roy, A.; Vitale, A.; Valdivieso, A.; Varo, E.; Seehofer, D.; Lynch, S.; Samuel, D.; et al. Pharmacokinetics for once-daily versus twice-daily tacrolimus formulations in de novo liver transplantation: A randomized, open-label trial. Liver Transpl. 2011, 17, 167–177. [Google Scholar] [CrossRef]
- Beckebaum, S.; Iacob, S.; Sweid, D.; Sotiropoulos, G.C.; Saner, F.; Kaiser, G.; Radtke, A.; Klein, C.G.; Erim, Y.; de Geest, S.; et al. Efficacy, safety, and immunosuppressant adherence in stable liver transplant patients converted from a twice-daily tacrolimus-based regimen to once-daily tacrolimus extended-release formulation. Transpl. Int. 2011, 24, 666–675. [Google Scholar] [CrossRef]
- Kuypers, D.R.; Naesens, M.; de Jonge, H.; Lerut, E.; Verbeke, K.; Vanrenterghem, Y. Tacrolimus dose requirements and CYP3A5 genotype and the development of calcineurin inhibitor-associated nephrotoxicity in renal allograft recipients. Ther. Drug Monit. 2010, 32, 394–404. [Google Scholar] [CrossRef]
- Genvigir, F.D.; Salgado, P.C.; Felipe, C.R.; Luo, E.Y.; Alves, C.; Cerda, A.; Tedesco-Silva, H., Jr.; Medina-Pestana, J.O.; Oliveira, N.; Rodrigues, A.C.; et al. Influence of the CYP3A4/5 genetic score and ABCB1 polymorphisms on tacrolimus exposure and renal function in Brazilian kidney transplant patients. Pharmacogenet. Genom. 2016, 26, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, S.; Nigro, V.; Weinberg, J.; Woodle, E.S.; Alloway, R.R. A Steady-State Head-to-Head Pharmacokinetic Comparison of All FK-506 (Tacrolimus) Formulations (ASTCOFF): An Open-Label, Prospective, Randomized, Two-Arm, Three-Period Crossover Study. Am. J. Transplant. 2017, 17, 432–442. [Google Scholar] [CrossRef]
- Barry, A.; Levine, M. A systematic review of the effect of CYP3A5 genotype on the apparent oral clearance of tacrolimus in renal transplant recipients. Ther. Drug Monit. 2010, 32, 708–714. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Hamada, T.; Nakatani, K.; Kishiwada, M.; Usui, M.; Sakurai, H.; Tabata, M.; Sakamoto, Y.; Nishioka, J.; Muraki, Y.; et al. Monitoring peripheral blood CD4+ adenosine triphosphate activity after living donor liver transplantation: Impact of combination assays of immune function and CYP3A5 genotype. J. Hepatobiliary Pancreat. Sci. 2011, 18, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Woillard, J.B.; de Winter, B.C.; Kamar, N.; Marquet, P.; Rostaing, L.; Rousseau, A. Population pharmacokinetic model and Bayesian estimator for two tacrolimus formulations--twice daily Prograf and once daily Advagraf. Br. J. Clin. Pharmacol. 2011, 71, 391–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews, L.M.; Li, Y.; De Winter, B.C.M.; Shi, Y.Y.; Baan, C.C.; Van Gelder, T.; Hesselink, D.A. Pharmacokinetic considerations related to therapeutic drug monitoring of tacrolimus in kidney transplant patients. Expert Opin. Drug Metab. Toxicol. 2017, 13, 1225–1236. [Google Scholar] [CrossRef]
- Caillard, S.; Moulin, B.; Buron, F.; Mariat, C.; Audard, V.; Grimbert, P.; Marquet, P. Advagraf ((R)), a once-daily prolonged release tacrolimus formulation, in kidney transplantation: Literature review and guidelines from a panel of experts. Transpl. Int. 2016, 29, 860–869. [Google Scholar] [CrossRef] [Green Version]
- Shuker, N.; Cadogan, M.; van Gelder, T.; Roodnat, J.I.; Kho, M.M.; Weimar, W.; Hesselink, D.A. Conversion from twice-daily to once-daily tacrolimus does not reduce intrapatient variability in tacrolimus exposure. Ther. Drug Monit. 2015, 37, 262–269. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Expressor Group (n = 28) | Non-Expressor Group (n = 32) | p-Value | |
|---|---|---|---|
| Donor | |||
| Sex (Male) | 12 (42.9%) | 24 (77.4%) | 0.008 |
| Age (years) | 34 (18–68) | 33 (20–78) | 0.641 |
| Recipient | |||
| Sex (Male) | 18 (64.3%) | 25 (78.1%) | 0.264 |
| Age (years) | 57 (35–74) | 54 (43–71) | 0.870 |
| Indications for LT | 0.396 | ||
| Alcoholic | 4 | 9 | |
| HBV | 5 | 3 | |
| HCV | 2 | 3 | |
| HCC | 12 | 12 | |
| AIH | 1 | 1 | |
| Biliary cirrhosis | 0 | 1 | |
| Budd–Chiari syndrome | 0 | 1 | |
| NBNC | 2 | 0 | |
| PBC | 0 | 1 | |
| PSC | 0 | 1 | |
| Wilson’s disease | 2 | 0 | |
| Retransplantation | 0 (0%) | 1 (3.1%) | 1.000 |
| Type of LT (LDLT) | 20 (71.4%) | 20 (62.5%) | 0.585 |
| MELD | 15 (6–40) | 14 (6–40) | 0.406 |
| Time from LT to study enrollment (mo.) | 16.7 (6.9–35.5) | 16.6 (6.2–43.5) | 0.711 |
| Efficacy | |||
| Biopsy-proven acute rejection | 0 (0%) | 0 (0%) | - |
| Graft failure | 0 (0%) | 0 (0%) | - |
| Death | 0 (0%) | 0 0%) | - |
| Before | After | p-Value | |
|---|---|---|---|
| Expressor group (n = 28) | |||
| Tacrolimus trough level (Cmin) (ng/mL) | 5.0 (2.6–7.9) | 3.8 (0.6–5.0) | <0.001 |
| Dose-adjusted Cmin (ng/mL/mg) | 1.4 (0.7–3.2) | 0.8 (0.4–2.8) | <0.001 |
| Dose/kg-adjusted Cmin (ng/mL/mg/kg) | 0.025 (0.008–0.067) | 0.015 (0.005–0.048) | <0.001 |
| Non-expressor group (n = 32) | |||
| Tacrolimus trough level (Cmin) (ng/mL) | 4.7 (2.7–7.8) | 3.9 (1.8–7.1) | <0.001 |
| Dose-adjusted Cmin (ng/mL/mg) | 2.3 (1.0–6.2) | 1.7 (0.7–4.7) | <0.001 |
| Dose/kg-adjusted Cmin (ng/mL/mg/kg) | 0.038 (0.016–0.115) | 0.029 (0.011–0.078) | <0.001 |
| Expressor Group (n = 5) | Non-Expressor Group (n = 5) | p-Value | |
|---|---|---|---|
| Dose (mg) | 4 (3–5) | 2 (1–3) | 0.016 |
| Weight (kg) | 54 (51.3–78.0) | 65 (43–82) | 0.690 |
| Dose/Weight (mg/kg) | 0.077 (0.045–0.097) | 0.037 (0.016–0.047) | 0.032 |
| AUC in Tac BID (ng·h/mL) | 126.3 (98.2–146.9) | 107.0 (102.4–126.7) | 0.310 |
| AUC in Tac QD (ng·h/mL) | 112.5 (81.0–168.6) | 96.1 (68.5–131.7) | 0.310 |
| Cmin in Tac BID (mg/mL) | 3.77 (3.05–4.20) | 3.07 (2.76–4.47) | 0.421 |
| Cmin in Tac QD (mg/mL) | 3.04 (1.85–4.21) | 2.59 (1.81–4.47) | 0.690 |
| Cmax in Tac BID (mg/mL) | 8.20 (4.94–11.54) | 9.93 (5.08–10.48) | 0.690 |
| Cmax in Tac QD (mg/mL) | 9.52 (6.81–11.90) | 7.85 (3.54–10.86) | 0.151 |
| Dose-adjusted Cmin in Tac BID (ng/mL/mg) | 0.918 (0.754–1.050) | 1.535 (0920–3.400) | 0.056 |
| Dose-adjusted Cmin in Tac QD (ng/mL/mg) | 0.680 (0.608–1.053) | 1.295 (0.603–2.235) | 0.151 |
| Dose-adjusted Cmax in Tac BID (ng/mL/mg) | 1.65 (1.58–2.40) | 3.79 (3.31–5.16) | 0.008 |
| Dose-adjusted Cmax in Tac QD (ng/mL/mg) | 2.73 (1.36–3.10) | 3.54 (1.85–5.43) | 0.310 |
| Dose-adjusted AUC in Tac BID (ng·h/mL/mg) | 29.4 (25.3–33.0) | 53.5 (35.2–102.4) | 0.008 |
| Dose-adjusted AUC in Tac QD (ng·h/mL/mg) | 27.0 (21.0–42.2) | 48.0 (24.2–68.5) | 0.095 |
| Dose/kg-adjusted Cmin Tac BID (ng/mL/mg/kg) | 0.015 (0.013–0.018) | 0.021 (0.012–0.053) | 0.548 |
| Dose/kg-adjusted Cmin Tac QD (ng/mL/mg/kg) | 0.013 (0.009–0.014) | 0.017 (0.009–0.052) | 0.222 |
| Dose/kg-adjusted Cmax Tac BID (ng/mL/mg/kg) | 0.032 (0.020–0.046) | 0.069 (0.040–0.088) | 0.032 |
| Dose/kg-adjusted Cmax Tac QD (ng/mL/mg/kg) | 0.038 (0.025–0.052) | 0.053 (0.029–0.126) | 0.421 |
| Dose/kg-adjusted AUC Tac BID (ng·h/mL/mg/kg) | 0.492 (0.423–0.553) | 0.716 (0.455–1.600) | 0.151 |
| Dose/kg-adjusted AUC Tac QD (ng·h/mL/mg/kg) | 0.458 (0.390–0.541) | 0.643 (0.379–1.532) | 0.421 |
| Expressor (n = 28) | Non-Expressor (n = 32) | p-Value | |
|---|---|---|---|
| Patients with adverse events | 17 (60.7%) | 18 (56.3%) | 0.796 |
| Adverse events | 41 | 30 | |
| Severity | 0.070 | ||
| Mild | 34 (82.9%) | 19 (63.3%) | |
| Moderate | 6 (14.6%) | 10 (33.3%) | |
| Severe | 1 (2.4%) | 1 (3.3%) | |
| Related to the study drug | 0.023 | ||
| Certain | 0 (0%) | 0 (0%) | |
| Probable/likely | 5 (12.2%) | 0 (0%) | |
| Possible | 5 (12.2%) | 0 (0%) | |
| Unlikely | 30 (73.2%) | 30 (100%) | |
| Conditional, unclassified | 1 (2.4%) | 0 (0%) | |
| Unassessable/unclassifiable | 0 (0%) | 0 (0%) | |
| Subjects with adverse events leading to drug discontinuation | 3 (10.7%) | 0 (0%) | 0.096 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.M.; Ryu, J.H.; Lee, K.-W.; Hong, S.K.; Yang, K.; Choi, G.-S.; Kim, Y.-A.; Lee, J.-Y.; Yi, N.-J.; Kwon, C.H.D.; et al. Effect of CYP3A5 on the Once-Daily Tacrolimus Conversion in Stable Liver Transplant Patients. J. Clin. Med. 2020, 9, 2897. https://doi.org/10.3390/jcm9092897
Kim JM, Ryu JH, Lee K-W, Hong SK, Yang K, Choi G-S, Kim Y-A, Lee J-Y, Yi N-J, Kwon CHD, et al. Effect of CYP3A5 on the Once-Daily Tacrolimus Conversion in Stable Liver Transplant Patients. Journal of Clinical Medicine. 2020; 9(9):2897. https://doi.org/10.3390/jcm9092897
Chicago/Turabian StyleKim, Jong Man, Je Ho Ryu, Kwang-Woong Lee, Suk Kyun Hong, Kwangho Yang, Gyu-Seong Choi, Young-Ae Kim, Ju-Yeun Lee, Nam-Joon Yi, Choon Hyuck David Kwon, and et al. 2020. "Effect of CYP3A5 on the Once-Daily Tacrolimus Conversion in Stable Liver Transplant Patients" Journal of Clinical Medicine 9, no. 9: 2897. https://doi.org/10.3390/jcm9092897
APA StyleKim, J. M., Ryu, J. H., Lee, K.-W., Hong, S. K., Yang, K., Choi, G.-S., Kim, Y.-A., Lee, J.-Y., Yi, N.-J., Kwon, C. H. D., Chu, C. W., Suh, K.-S., & Joh, J.-W. (2020). Effect of CYP3A5 on the Once-Daily Tacrolimus Conversion in Stable Liver Transplant Patients. Journal of Clinical Medicine, 9(9), 2897. https://doi.org/10.3390/jcm9092897