Portal Thrombosis in Cirrhosis: Role of Thrombophilic Disorders


 ,
,
Abstract
1. Introduction
2. Experimental Section
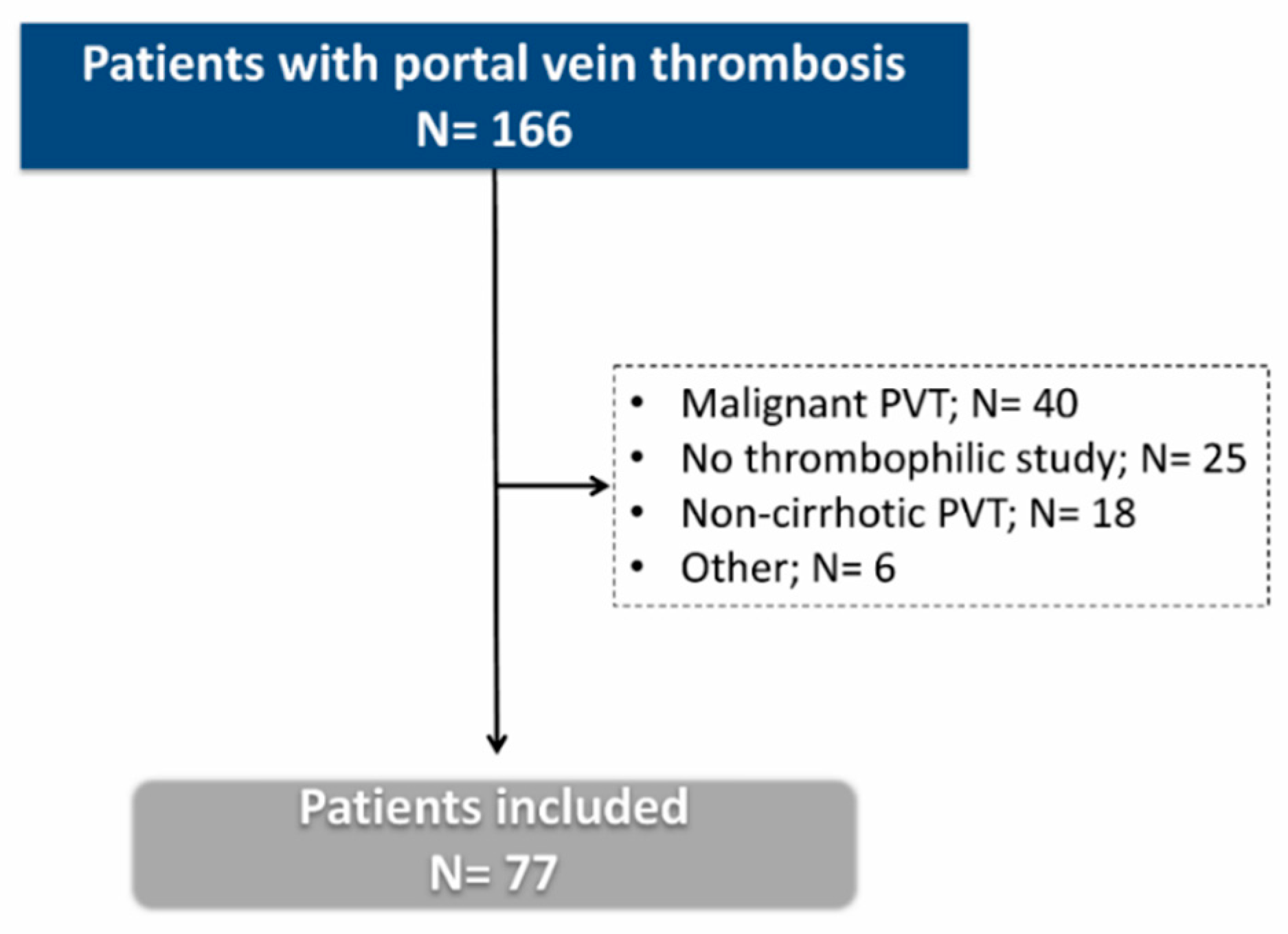
2.1. Patients
2.2. Definitions
2.2.1. Thrombosis
2.2.2. Recanalization
2.2.3. Thrombosis Progression
2.3. Anticoagulation Therapy
2.4. Follow Up
2.5. Thrombophilic Study
2.6. Statistical Analysis
3. Results
3.1. Prevalence of Thrombophilia
3.2. Characteristics of Patients with and without Thrombophilia
3.3. Extension and Clinical Characteristics of Thrombosis at Diagnosis
3.4. Treatment and Factors Associated with the Outcome of Portal Vein Thrombosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ACA | Anti-cardiolipin antibodies |
| ALT | Alanine aminotransferase |
| AP | Alkaline phosphatase |
| APS | Antiphospholipid syndrome |
| AT-III | Antithrombin III |
| BCLC | Barcelona Clinic Liver Cancer |
| CT | Computed tomography |
| EV | Esophageal varices |
| FV | factor V Leiden mutation |
| FVL | Factor V Leiden |
| HCC | Hepatocellular carcinoma |
| HE | Hepatic encephalopathy |
| HIV | Human immunodeficiency virus |
| INR | International normalized ratio |
| JAK2 | Janus Kinase 2 mutation |
| LA | Lupus anticoagulant |
| LMWH | Molecular-weight heparin |
| LT | Liver transplantation |
| MELD | Model for End-Stage Disease |
| MRI | Magnetic resonance imaging |
| MTHFR | Methylenetetrahydrofolate reductase TT677 genotype |
| PAI-1 | Plasminogen activator inhibitor type 1 |
| PNH | Paroxysmal nocturnal hemoglobinuria |
| PTHR | Prothrombin G20210A mutation |
| PV | Polycythemia vera |
| PVT | Portal vein thrombosis |
| RCT | Randomized control trial |
| SBP | Spontaneous bacterial peritonitis |
| SMV | Superior mesenteric vei |
| SV | Splenic vein |
| TIPS | Transjugular intrahepatic portosystemic shunt |
| UK | United Kingdom |
| US | Ultrasound |
| VB | Variceal bleeding |
References
- EASL Clinical Practice Guidelines: Vascular diseases of the liver. J. Hepatol. 2016, 64, 179–202. [CrossRef]
- Zanetto, A.; Rodriguez-Kastro, K.I.; Germani, G.; Ferrarese, A.; Cillo, U.; Burra, P.; Senzolo, M. Mortality in liver transplant recipients with portal vein thrombosis—An updated meta-analysis. Transpl. Int. 2018, 31, 1318–1329. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Caldwell, S.H.; Tripodi, A. Diagnosis, Development, and Treatment of Portal Vein Thrombosis in Patients with and Without Cirrhosis. Gastroenterology 2019, 156, 1582–1599. [Google Scholar] [CrossRef]
- Intagliata, N.M.; Argo, C.K.; Stine, J.G.; Lisman, T.; Caldwell, S.H.; Violi, F. Concepts and Controversies in Haemostasis and Thrombosis Associated with Liver Disease: Proceedings of the 7th International Coagulation in Liver Disease Conference. Thromb. Haemost. 2018, 118, 1491–1506. [Google Scholar] [CrossRef]
- O’Leary, J.G.; Greenberg, C.S.; Patton, H.M.; Caldwell, S.H. AGA Clinical Practice Update: Coagulation in Cirrhosis. Gastroenterology 2019, 157, 34–43. [Google Scholar] [CrossRef]
- Zanetto, A.; Garcia-Tsao, G. Some Answers and More Questions About Portal Vein Thrombosis in Patients with Decompensated Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 30485–30487. [Google Scholar] [CrossRef]
- DeLeve, L.D.; Valla, D.C.; Garcia-Tsao, G. Vascular disorders of the liver. Hepatology 2009, 49, 1729–1764. [Google Scholar] [CrossRef] [PubMed]
- Martín-Llahí, M.; Albillos, A.; Bañares, R.; Berzigotti, A.; García-Criado, M.; Genescà, J.; Hernández-Gea, V.; Llop-Herrera, E.; Masnou-Ridaura, H.; Mateo, J.; et al. Vascular diseases of the liver. Clinical Guidelines from the Catalan Society of Digestology and the Spanish Association for the Study of the Liver. Gastroenterol. Hepatology 2017, 40, 538–580. [Google Scholar] [CrossRef]
- Zocco, M.A.; Di Stasio, E.; De Cristofaro, R.; Novi, M.; Ainora, M.E.; Ponziani, F.; Riccardi, L.; Lancellotti, S.; Santoliquido, A.; Flore, R.; et al. Thrombotic risk factors in patients with liver cirrhosis: Correlation with MELD scoring system and portal vein thrombosis development. J. Hepatol. 2009, 51, 682–689. [Google Scholar] [CrossRef]
- Stine, J.G.; Wang, J.; Shah, P.M.; Argo, C.K.; Intagliata, N.; Uflacker, A.; Caldwell, S.H.; Northup, P.G. Decreased portal vein velocity is predictive of the development of portal vein thrombosis: A matched case-control study. Liver. Int. 2018, 38, 94–101. [Google Scholar] [CrossRef]
- Mahmoud, A.E.; Elias, E.; Beauchamp, N.; Wilde, J.T. Prevalence of the factor V Leiden mutation in hepatic and portal vein thrombosis. Gut 1997, 40, 798–800. [Google Scholar] [CrossRef] [PubMed]
- Amitrano, L.; Brancaccio, V.; Guardascione, M.A.; Margaglione, M.; Iannaccone, L.; D’Andrea, G.; Marmo, R.; Ames, P.R.; Balzano, A. Inherited coagulation disorders in cirrhotic patients with portal vein thrombosis. Hepatology 2000, 31, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Amitrano, L.; Guardascione, M.A.; Brancaccio, V.; Margaglione, M.; Manguso, F.; Iannaccone, L.; Grandone, E.; Balzano, A. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J. Hepatol. 2004, 40, 736–741. [Google Scholar] [CrossRef]
- Amitrano, L.; Guardascione, M.A.; Ames, P.R.; Margaglione, M.; Iannaccone, L.; Brancaccio, V.; Balzano, A. Increased plasma prothrombin concentration in cirrhotic patients with portal vein thrombosis and prothrombin G20210A mutation. Thromb. Haemost. 2006, 95, 221–223. [Google Scholar] [CrossRef]
- Amitrano, L.; Ames, P.R.; Guardascione, M.A.; Lopez, L.R.; Menchise, A.; Brancaccio, V.; Iannaccone, L.; Balzano, A. Antiphospholipid antibodies and antiphospholipid syndrome: Role in portal vein thrombosis in patients with and without liver cirrhosis. Clin. Appl. Thromb. Hemost. 2011, 17, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Mangia, A.; Villani, M.R.; Cappucci, G.; Santoro, R.; Ricciardi, R.; Facciorusso, D.; Leandro, G.; Caruso, N.; Andriulli, A. Causes of portal venous thrombosis in cirrhotic patients: The role of genetic and acquired factors. Eur. J. Gastroenterol. Hepatol. 2005, 17, 745–751. [Google Scholar] [CrossRef]
- Pasta, L.; Marrone, C.; D’Amico, M.; Virdone, R.; D’Amico, G.; Sammarco, P.; Fabiano, C.; Pagliaro, L. MTHFR C677T mutations in liver cirrhosis with and without portal vein thrombosis. Liver. Int. 2006, 26, 269–270. [Google Scholar] [CrossRef] [PubMed]
- Pasta, L.; Pasta, F.; D’Amico, M. PAI-1 4G-4G, MTHFR 677TT, V Leiden 506Q, and Prothrombin 20210A in Splanchnic Vein Thrombosis: Analysis of Individual Patient Data from Three Prospective Studies. J. Clin. Exp. Hepatol. 2016, 6, 10–14. [Google Scholar] [CrossRef]
- Colaizzo, D.; Amitrano, L.; Guardascione, M.A.; Balzano, A.; Margaglione, M. Janus kinase-2 mutation, cirrhosis and splanchnic vein thrombosis. Eur. J. Gastroenterol. Hepatol. 2008, 20, 245–246. [Google Scholar] [CrossRef]
- Gabr, M.A.; Bessa, S.S.; El-Zamarani, E.A. Portal vein thrombosis in Egyptian patients with liver cirrhosis: Role of methylenetetrahydrofolate reductase C677T gene mutation. Hepatol. Res. 2010, 40, 486–493. [Google Scholar] [CrossRef]
- Ayala, R.; Grande, S.; Bustelos, R.; Ribera, C.; García-Sesma, A.; Jimenez, C.; Moreno, E.; Martínez-López, J. Obesity is an independent risk factor for pre-transplant portal vein thrombosis in liver recipients. BMC Gastroenterol. 2012, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; Zhang, C.; Han, G.; Zhang, W.; He, C.; Yin, Z.; Liu, Z.; Bai, W.; Li, R.; Bai, M.; et al. Prevalence of the JAK2V617F mutation in Chinese patients with Budd-Chiari syndrome and portal vein thrombosis: A prospective study. J. Gastroenterol. Hepatol. 2012, 27, 1036–1043. [Google Scholar] [CrossRef]
- Senzolo, M.; Sartori, T.M.; Rossetto, V.; Burra, P.; Cillo, U.; Boccagni, P.; Gasparini, D.; Miotto, D.; Simioni, P.; Tsochatzis, E.; et al. Prospective evaluation of anticoagulation and transjugular intrahepatic portosystemic shunt for the management of portal vein thrombosis in cirrhosis. Liver. Int. 2012, 32, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Werner, K.T.; Sando, S.; Carey, E.J.; Vargas, H.E.; Byrne, T.J.; Douglas, D.D.; Harrison, M.E.; Rakela, J.; Aqel, B.A. Portal vein thrombosis in patients with end stage liver disease awaiting liver transplantation: Outcome of anticoagulation. Dig. Dis. Sci. 2013, 58, 1776–1780. [Google Scholar] [CrossRef]
- Nery, F.; Chevret, S.; Condat, B.; de Raucourt, E.; Boudaoud, L.; Rautou, P.-E.; Plessier, A.; Roulot, D.; Chaffaut, C.; Bourcier, V.; et al. Causes and consequences of portal vein thrombosis in 1,243 patients with cirrhosis: Results of a longitudinal study. Hepatology 2015, 61, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Karaköse, S.; Oruç, N.; Zengin, M.; Akarca, U.S.; Ersöz, G. Diagnostic value of the JAK2 V617F mutation for latent chronic myeloproliferative disorders in patients with Budd-Chiari syndrome and/or portal vein thrombosis. Turk. J. Gastroenterol. 2015, 26, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Lee, M.; Feichtinger, S.; Hapfelmeier, A.; Schmid, R.M.; Siveke, J.T. Thrombophilic factor analysis in cirrhotic patients with portal vein thrombosis. J. Thromb. Thrombol. 2015, 40, 54–60. [Google Scholar] [CrossRef]
- Lancellotti, S.; Basso, M.; Veca, V.; Sacco, M.; Riccardi, L.; Pompili, M.; De Cristofaro, R. Presence of portal vein thrombosis in liver cirrhosis is strongly associated with low levels of ADAMTS-13: A pilot study. Intern. Emerg. Med. 2016, 11, 959–967. [Google Scholar] [CrossRef]
- Ventura, P.; Venturelli, G.; Marcacci, M.; Fiorini, M.; Marchini, S.; Cuoghi, C.; Pietrangelo, A. Hyperhomocysteinemia and MTHFR C677T polymorphism in patients with portal vein thrombosis complicating liver cirrhosis. Thromb. Res. 2016, 141, 189–195. [Google Scholar] [CrossRef]
- Artaza, T.; Lopes, M.; Romero, M.; Gómez, A.Z.; de la Cruz, G.; Sánchez, J.J.; González, C.; Gómez, R. Efficacy and safety of anticoagulation in non-malignant portal vein thrombosis in patients with liver cirrhosis. Gastroenterol. Hepatol. 2018, 41, 611–617. [Google Scholar] [CrossRef]
- Senzolo, M.; Riva, N.; Dentali, F.; Rodriguez-Castro, K.; Sartori, M.T.; Bang, S.M.; Martinelli, I.; Schulman, S.; Alatri, A.; Beyer-Westendorf, J.; et al. Long-Term Outcome of Splanchnic Vein Thrombosis in Cirrhosis. Clin. Transl. Gastroenterol. 2018, 9, 176. [Google Scholar] [CrossRef] [PubMed]
- Cagin, Y.F.; Bilgic, Y.; Berber, İ.; Yildirim, O.; Erdogan, M.A.; Firat, F.; Arslan, A.K.; Colak, C.; Seckin, Y.; Harputluoglu, M. The risk factors of portal vein thrombosis in patients with liver cirrhosis. Exp. Ther. Med. 2019, 17, 3189–3194. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, D.; Naymagon, L.; Troy, K.; Cromwell, C.; Edwards, C.; Schiano, T.; Kremyanskaya, M.; Mascarenhas, J. The utility of thrombophilia testing in patients with newly diagnosed portal vein thrombosis. Blood Coagul. Fibrinolysis 2020, 31, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Galli, M.; Gianni, M.; Ageno, W. Inherited thrombophilic abnormalities and risk of portal vein thrombosis. a meta-analysis. Thromb. Haemost. 2008, 99, 675–682. [Google Scholar] [CrossRef]
- Qi, X.; Ren, W.; De Stefano, V.; Fan, D. Associations of coagulation factor V Leiden and prothrombin G20210A mutations with Budd-Chiari syndrome and portal vein thrombosis: A systematic review and meta-analysis. Clin. Gastroenterol. Hepatol. 2014, 12, 1801–1812. [Google Scholar] [CrossRef]
- Ma, S.D.; Wang, J.; Bezinover, D.; Kadry, Z.; Northup, P.G.; Stine, J.G. Inherited thrombophilia and portal vein thrombosis in cirrhosis: A systematic review and meta-analysis. Res. Pract. Thromb. Haemost. 2019, 3, 658–667. [Google Scholar] [CrossRef]
- Qi, X.; Chen, H.; Han, G. Effect of antithrombin, protein C and protein S on portal vein thrombosis in liver cirrhosis: A meta-analysis. Am. J. Med. Sci. 2013, 346, 38–44. [Google Scholar] [CrossRef]
- Colucci, G.; Tsakiris, D.A. Thrombophilia screening revisited: An issue of personalized medicine. J. Thromb. Thrombol. 2020, 49, 618–629. [Google Scholar] [CrossRef]
- Delgado, M.G.; Seijo, S.; Yepes, I.; Achécar, L.; Catalina, M.V.; García-Criado, A.; Abraldes, J.G.; de la Peña, J.; Bañares, R.; Albillos, A.; et al. Efficacy and safety of anticoagulation on patients with cirrhosis and portal vein thrombosis. Clin. Gastroenterol. Hepatol. 2012, 10, 776–783. [Google Scholar] [CrossRef]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.W.M.; De Groot, P.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef] [PubMed]
- Qi, X.; De Stefano, V.; Su, C.; Bai, M.; Guo, X.; Fan, D. Associations of antiphospholipid antibodies with splanchnic vein thrombosis: A systematic review with meta-analysis. Medicine 2015, 94. [Google Scholar] [CrossRef] [PubMed]
- Connors, J.M. Thrombophilia Testing and Venous Thrombosis. N. Engl. J. Med. 2017, 377, 1177–1187. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, L.; Pastori, D.; Farcomeni, A.; Violi, F. Effects of Anticoagulants in Patients with Cirrhosis and Portal Vein Thrombosis: A Systematic Review and Meta-analysis. Gastroenterology 2017, 153, 480–487. [Google Scholar] [CrossRef]
- Magaz, M.; Alvarez-Larrán, A.; Colomer, D.; López-Guerra, M.; García-Criado, M.Á.; Mezzano, G.; Belmonte, E.; Olivas, P.; Soy, G.; Cervantes, F.; et al. Next generation sequencing in the diagnosis of non-cirrhotic splanchnic vein thrombosis. J. Hepatol. 2020. [Google Scholar] [CrossRef]


{kind=link}
| Variable * | Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 |
|---|---|---|---|---|---|---|
| Type of thrombophilia | APS | APS | APS | APS | PV + FVL (heterozygous) | PTHR (heterozygous) |
| Age (years) | 51 | 77 | 57 | 56 | 72 | 69 |
| Gender | Female | Male | Male | Male | Male | Male |
| Race | Caucasian | Caucasian | Caucasian | Caucasian | Caucasian | Caucasian |
| Comorbidity | Diabetes | Diabetes | No | Hypertension | Diabetes | Diabetes |
| Etiology of liver disease | Hepatitis C | Alcohol | Alcohol | Alcohol | Alcohol | Alcohol |
| Child-Pugh | B (7 points) | B (7 points) | A (6 points) | B (9 points) | B (7 points) | A (6 points) |
| MELD (points) | 11 | 9 | 8 | 27 | 13 | 10 |
| Previous decompensation | VB + HE + ascites | Ascites | VB + ascites | Ascites | No | VB + HE + ascites |
| EV without bleeding | High risk | Low risk | High risk | |||
| Non-selective betablockers | Yes | Yes | Yes | Yes | No | Yes |
| Hepatocellular carcinoma (HCC) (No/BCLC stage) | No | No | No | No | No | A |
| Previous thrombotic events | No | No | No | No | No | No |
| Imaging for PVT diagnosis | CT | US | CT | CT | US | CT |
| Localization and extension | Main PV/Complete | Main PV/Partial | Main PV (complete), SV and SMV (partial) | PV, both branches and SMV/Partial | PV and branches/Complete | Right PV/Complete |
| Portal cavernoma | Yes | No | No | No | No | No |
| Local predisposing factor | No | No | No | No | No | No |
| Decompensation at diagnosis | Ascites | VB and ascites | No | SBP and HE | Ascites | No |
| Other symptoms | No | No | No | No | No | No |
| Analytical parameters at diagnosis | ||||||
| Leucocytes (×103 μL) | 3.4 | 5.1 | 3.0 | 12.0 | 2.3 | 5.0 |
| Platelets (×103 μL) | 60 | 140 | 35 | 94 | 65 | 162 |
| Hemoglobin (gr/dL) | 9.8 | 11.6 | 14.8 | 13.8 | 11 | 13.9 |
| Creatinine (mg/dL) | 0.96 | 0.97 | 0.80 | 2.81 | 0.88 | 0.85 |
| Sodium (mEq/L) | 138 | 134 | 137 | 129 | 138 | 137 |
| ALT (U/L) | 56 | 44 | 20 | 21 | 62 | 26 |
| AP (U/L) | 119 | 235 | 46 | 100 | 47 | 123 |
| Bilirubin (mg/dL) | 0.9 | 1.2 | 0.6 | 3 | 2.1 | 1.4 |
| Albumin (gr/dL) | 2.9 | 3.2 | 4.4 | 3.4 | 4.2 | 3.8 |
| INR | 1.45 | 1.14 | 1.2 | 1.77 | 1.34 | 1.27 |
| Treatment | Acenocoumarol | Acenocoumarol | Acenocoumarol | Acenocoumarol | LMWH | No |
| PVT evolution | Progression | Partial resolution | No | Total resolution | Total resolution | Stability |
| Duration anticoagulation (months) | Indefinite (157.2) | Finite (8.1) | Indefinite (101.1) | Indefinite (38.6) | (Finite) 22.2 | |
| Re-thrombosis | Yes | Yes | ||||
| Exitus/LT | LT | Death | Death | No | Death | LT |
| Time of follow-up (months) | 21.3 | 16.9 | 102.5 | 38.6 | 85.0 | 24.0 |
| Variable * | Population (N = 77) | Non-Thrombophilia (N = 71) | Thrombophilia (N = 6) | p |
|---|---|---|---|---|
| Age (years) | 61.9 (55.0–67.6) | 61.9 (54.9–67.2) | 63 (54.6–73.6) | 0.464 |
| Gender (male) | 67 (87) | 62 (87.3) | 5 (75.0) | 0.579 |
| Race (Caucasian) | 76 (98.7) | 70 (98.6) | 6 (100) | 1 |
| Diabetes Mellitus | 24 (31.2) | 20 (28.2) | 4 (66.7) | 0.072 |
| Dyslipidemia | 12 (15.6) | 12 (16.9) | 0 (0) | 0.582 |
| Arterial hypertension | 22 (28.6) | 21 (29.6) | 1 (16.7) | 0.668 |
| Chronic kidney injury | 5 (6.5) | 5 (7.0) | 0 (0) | 0.929 |
| HIV | 4 (5.2) | 4 (5.6) | 0 (0) | 1 |
| Etiology of liver disease | 0.969 | |||
| Alcohol | 49 (63.6) | 44 (62.0) | 5 (83.3) | |
| Hepatitis C | 8 (10.4) | 7 (9.9) | 1 (16.7) | |
| Other | 20 (26.0) | 20 (28.2) | 0 (0) | |
| Child-Pugh (points) | 7 (6–9) | 7 (6–9) | 7 (5.8–7.5) | 0.379 |
| Child A/B/C (%) | 35/50/15 | 36/49/15 | 33/67/0 | 0.519 |
| MELD (points) | 12 (10–14) | 13 (10–14) | 11 (9.0–15.8) | 0.814 |
| Previous TIPS | 4 (5.2) | 4 (5.6) | 0 (0) | 1 |
| Liver allograft cirrhosis | 3 (3.9) | 3 (4.2) | 0 (0) | 1 |
| Esophageal varices (Low/High risk) | 14 (32)/22 (50) | 13 (31.7)/20 (48.8) | 1 (33.3)/2 (66.7) | 0.682 |
| Previous variceal bleeding | 33 (42.9) | 30 (42.3) | 3 (50) | 1 |
| Non-selective betablockers | 51 (66.2) | 46 (64.8) | 5 (83.3) | 0.657 |
| Previous ascites (No/Yes/Refractory) (%) | 27/65/8 | 28/63/9 | 17/83/0 | 0.818 |
| Previous SBP | 6 (7.8) | 6 (8.5) | 0 (0) | 1 |
| Previous HE (No/Episodic/Recurrent) (%) | 75/24/1 | 76/23/1 | 67/33/0 | 0.808 |
| Any previous decompensation | 62 (80.5) | 57 (80.3) | 5 (83.3) | 1 |
| HCC (No/BCLC stage A/B) (%) | 87/12/1 | 88/11/1 | 83/17/0 | 0.890 |
| Previous arterial/venous thrombotic events | 3 (3.9) | 3 (4.2) | 0 (0) | 1 |
| Variable * | Population (N = 77) | Non-Thrombophilia (N = 71) | Thrombophilia (N = 6) | p |
|---|---|---|---|---|
| CT or MRI portal vein thrombosis (PVT) diagnosis | 67 (87.0) | 63 (88.7) | 4 (66.7) | 0.172 |
| Localization and extension | ||||
| Right PV (Partial/total) (%) | 27 (35.1)/8 (10.4) | 26 (36.6)/6 (8.5) | 1 (16.7)/2 (33.3) | 0.139 |
| Left PV (Partial/total) (%) | 18 (23.4)/5 (6.5) | 16 (22.5)/5 (7.0) | 2 (33.3)/0 (0) | 0.701 |
| Main PV (Partial/total) (%) | 49 (63.6)/8 (10.4) | 47 (66.2)/5 (7.0) | 2 (33.3)/3 (50) | 0.004 |
| Splenic vein (SV) (Partial/total) (%) | 5 (6.5)/2 (2.6) | 4 (5.6)/2 (2.8) | 1 (16.7)/0 (0) | 0.536 |
| Superior mesenteric vein (SMV) (Partial/total) (%) | 21 (27.3)/3 (3.9) | 19 (26.8)/3 (4.2) | 2 (33.3)/0 (0) | 0.841 |
| Portal cavernoma | 9 (11.7) | 8 (11.3) | 1 (16.7) | 0.538 |
| Local predisposing factor | 4 (5.2) | 4 (5.6) | 0 (0) | 1 |
| Symptoms at diagnosis | 33 (42.9) | 31 (43.7) | 2 (33.3) | 0.695 |
| Acute mesenteric ischemia | 1 (1.3) | 1 (1.4) | 0 (0) | 1 |
| Abdominal pain | 7 (9.1) | 7 (9.9) | 0 (0) | 1 |
| Fever | 2 (2.6) | 2 (2.8) | 0 (0) | 1 |
| Variceal bleeding | 14 (18.2) | 13 (18.3) | 1 (16.7) | 1 |
| Ascites (total/de novo) | 38 (49.4)/5 (6.5) | 34 (47.9)/4 (5.6) | 4 (66.7)/1 (16.7) | 0.431 |
| SBP | 6 (7.8) | 5 (7.0) | 1 (16.7) | 0.396 |
| HE | 10 (13.0) | 9 (12.7) | 1 (16.7) | 0.579 |
| Analytical parameters at diagnosis | ||||
| Leucocytes (×103 μL) | 5.0 (3.3–6.0) | 5.0 (3.4–6.0) | 4.2 (2.8–6.8) | 0.791 |
| Platelets (×103 μL) | 79 (62–110) | 79 (63–109) | 80 (54–146) | 0.882 |
| Hemoglobin (gr/dL) | 12.8 (10.4–14.4) | 12.8 (10.3–14.4) | 12.7 (10.7–14.1) | 0.905 |
| Creatinine (mg/dL) | 0.8 (0.7–1.0) | 0.8 (0.7–1.0) | 0.9 (0.8–1.4) | 0.309 |
| Sodium (mEq/L) | 139 (137–141) | 139 (137–141) | 137 (132–138) | 0.124 |
| ALT (U/L) | 34 (23–46) | 34 (24–45) | 35 (21–58) | 0.768 |
| Alkaline phosphatase (U/L) | 114 (78–154) | 114 (79–155) | 110 (47–151) | 0.576 |
| Bilirubin | 1.6 (1.1–2.5) | 1.6 (1.2–2.6) | 1.3 (0.8–2.3) | 0.389 |
| Albumin (gr/dL) | 3.4 (3.0–3.8) | 3.4 (3.0–3.8) | 3.6 (3.1–4.3) | 0.296 |
| INR | 1.34 (1.23–1.52) | 1.34 (1.23–1.52) | 1.31 (1.19–1.53) | 0.691 |
| Variable * | Population (N = 72) | Non-Thrombophilia (N = 66) | Thrombophilia (N = 6) | p |
|---|---|---|---|---|
| Anticoagulation | 58 (80.6) | 53 (80.3) | 5 (83.3) | 1 |
| Acenocoumarol | 45 (77.6) | 41 (77.4) | 4 (80.0) | 0.951 |
| LMWH | 12 (20.7) | 11 (20.8) | 1 (20.0) | |
| Apixaban | 1 (1.7) | 1 (1.9) | 0 (0) | |
| Duration (months) | 12.6 (6.2–27.0) | 11.6 (5.8–20.3) | 38.6 (15.1–129.1) | 0.174 |
| Transjugular intrahepatic portosystemic shunt (TIPS) | 4 (5.6) | 4 (6.1) | 0 (0) | 1 |
| PVT evolution in non-treated patients | 10 (3.9) | 9 (13.6) | 1 (16.7) | 0.923 |
| Stability | 7 (70.0) | 6 (66.7) | 1 (100) | |
| Progression | 2 (20.0) | 2 (22.2) | 0 (0) | |
| Partial resolution | 1 (0.0) | 1 (11.1) | 0 (0) | |
| Total resolution | 0 (0) | 0 (0) | 0 (0) | |
| PVT evolution in treated patients (anticoagulation or TIPS) | 62 (86.1) | 57 (86.4) | 5 (83.3) | 0.954 |
| Stability | 14 (22.6) | 13 (22.8) | 1 (20.0) | |
| Progression | 7 (11.3) | 6 (10.5) | 1 (20.0) | |
| Partial resolution | 12 (19.4) | 11 (19.3) | 1 (20.0) | |
| Total resolution | 29 (46.8) | 27 (47.4) | 2 (40.0) | |
| Re-thrombosis after ceasing anticoagulation | 10 (32.3) | 8 (27.6) | 2 (100) | 0.097 |
| Exitus | 36 (50.0) | 33 (50) | 3 (50) | 1 |
| Liver transplantation | 17 (23.6) | 15 (22.7) | 2 (33.3) | 0.621 |
| Time of follow-up (months) | 27.0 (10.9–55.5) | 27.0 (10.8–55.0) | 22.7 (18.0–69.7) | 0.339 |
| Author and Year | N † | Study Period And Type | Population | PTHR ‡ | FVL ‡ | APS ‡ | JAK2 ‡ | MTHFR ‡ | PAI ‡ | Comments |
|---|---|---|---|---|---|---|---|---|---|---|
| Mahmoud et al.; 1997 [11] | 32 | NS Retrospective | UK | 1/32 (3.1%) | Authors concluded Factor V Leiden (FVL) was not a major contributor of portal vein thrombosis (PVT). Not all 32 patients had liver cirrhosis. | |||||
| Amitrano et al.; 2000 [12] | 23 | 1998–1999 Case-control | Italy | 8/23 (34.8%) | 3/13 (13%) | NS | 10/23 (43.5%) | Prothrombin G20210A (PTHR) and MTHFR were strongly associated with PVT. ACA in 4% and LA in 0%. No further test to confirm ACA positivity. | ||
| Amitrano et al.; 2004 [13] | 79 | 1998–2002 Case-control | Italy | 15/70 (21.4%) | 8/70 (11.4%) | NS | 15/70 (21.4%) | ACA IgG and ACA IgM at low levels in PVT and in one above 40 UI/L. PTHR increased more than fivefold the risk of PVT. | ||
| Mangia et al.; 2005 [16] | 43 | 1997–1999 Case-control | Italy | 2/43 (4.7%) | 1/43 (2.3%) | 9/43 (20.9%) | PTHR, FVL and MTHFR were evenly distributed among patients with and without PVT. | |||
| Amitrano et al.; 2006 [14] | 78 | 1998–2002 Case-control | Italy | 17/78 (21.4%) | PTHR was associated with PVT, and factor II levels were higher in patients with PTHR and PVT. | |||||
| Pasta et al.; 2006 [17] | 78 | 2000–2005 Case-control | Italy | 19/78 (24.4%) | MTHFR was associated with PVT development. | |||||
| Colaizzo et al.; 2008 [19] | 91 | NS Retrospective | Italy | 5/91 (5.5%) | Authors suggested to search for JAK2 in the setting of severe PVT, previous thrombosis and no thrombopenia. | |||||
| Gabr et al.; 2010 [20] | 21 | NS Case-control | Egypt | 7/21 (33%) | Authors concluded that MTHFR was associated with an increased risk of PVT. | |||||
| Amitrano et al.; 2011 [15] | 50 | NS Case-control | Italy | 0/50 (0%) | Antiphospholipid antibodies played no role in PVT associated with liver cirrhosis. | |||||
| Ayala et al.; 2012 [21] | 50 | 2001–2006 Case-control | Spain | 1/49 (2%) | 1/49 (2%) | 0/50 (0%) | 7/48 (14.6%) | No association was observed between pre-transplant PVT and presence of genetic thrombophilia. | ||
| Delgado et al.; 2012 [39] | 43 | 2003–2010 Retrospective | Spain | 3/43 (7%) | 1/43 (2.3%) | 1/43 (2.3%) | Multicenter study. Thrombophilia in 16% of patients and it was not associated with response to anticoagulation. | |||
| Qi et al.; 2012 [22] | 71 | 2009–2011 Prospective | China | 1/71 (1.4%) | Prevalence very close to that of a Chinese hospital population of patients without PVT. | |||||
| Senzolo et al.; 2012 [23] | 56 | 2007–2008 Prospective | UK, Italy | 4/56 (7%) | 2/56 (3.6%) | 0/56 (0%) | - | - | - | Bicenter study. One patient had combined thrombophilia (FVL + PTHR). |
| Werner et al.; 2013 [24] | 69 | 2005–2011 Retrospective | USA | 0/22 (0%) | 0/22 (0%) | 0/22 (0%) | One patient had antithrombin deficiency. | |||
| Karakose et al.; 2015 [26] | 38 | 2005–2009 Prospective | Turkey | 4/38 (10.5%) | 5/38 (13.1%) | 1/38 (2.6%) | 5/38 (13.2%) | Unicenter study. | ||
| Nery et al.; 2015 [25] | 67 | 2000–2006 RCT | France | NS | NS | Multicenter RCT. PTHR and FVL were studied in 283 patients, (PVT in 67). Their presence was not associated with PVT. | ||||
| Saugel et al.; 2015 [27] | 21 | 2009–2011 Case-control | Germany | 0/21 (0%) | 1/21 (4.8%) | 2/21 (9.5%) | There was a trend for higher frequency of JAK2 mutation in cirrhotic patients with PVT than those without PVT. | |||
| Lancelloti et al.; 2016 [28] | 24 | 2013 Case-control | Italy | 1/24 (4.2%) | 0/24 (0%) | NS | PTHR and FVL were infrequent and not associated with PVT development. | |||
| Pasta et al.; 2016 [18] | 350 | 2000–2014 Prospective | Italy | 18/350 (5%) | 29/350 (8%) | 88/350 (25%) | 111/350 (31%) | Data from 3 prospective studies. ≥1 genetic thrombophilia in 54% of patients. MTHFR/PAI were associated with PVT. | ||
| Ventura et al.; 2016 [29] | 38 | 2009–2013 Case-control | Italy | 11/38 (10.5%) | 4/38 (10.5%) | 2/38 (7.9%) | 13/38 (34.2) | PTHR and hyperhomocysteinemia were associated with PVT development. | ||
| Artaza et al.; 2018 [30] | 32 | 2009–2015 Retrospective | Spain | 0/24 (0%) | 2/24 (8.3%) | 1/24 (4.2%) | Thrombophilia in 4 patients (16%). No association between thrombophilia and evolution of PVT. | |||
| Senzolo et al.; 2018 [31] | 149 | 2008–2012 Prospective | International | 7/64 (10.9%) | 7/71 (9.9%) | 1/32 (3.1%) | Thrombophilia testing <50% of the patients. Authors did not search for an association between PVT and thrombophilia. | |||
| Cagin et al.; 2019 [32] | 98 | 2009–2015 Case-control | Turkey | 15/98 (15.3%) | 12/98 (12.2%) | 16/98 (16.3%) | FVL mutation was the only type of thrombophilia associated with PVT. | |||
| Tremblay et al., 2020 [33] | 73 | 2000–2019 Retrospective | USA | 4/63 (6.3%) | 4/65 (6.1%) | 2/66 (3%) | 1/45 (2.2%) | 1/27 (3.7%) | 20/34 (58.8%) | Thrombophilia testing was not complete in most patients and infrequently led to change in management. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fortea, J.I.; Carrera, I.G.; Puente, Á.; Cuadrado, A.; Huelin, P.; Tato, C.Á.; Fernández, P.Á.; Montes, M.d.R.P.; Céspedes, J.N.; López, A.B.; et al. Portal Thrombosis in Cirrhosis: Role of Thrombophilic Disorders. J. Clin. Med. 2020, 9, 2822. https://doi.org/10.3390/jcm9092822
Fortea JI, Carrera IG, Puente Á, Cuadrado A, Huelin P, Tato CÁ, Fernández PÁ, Montes MdRP, Céspedes JN, López AB, et al. Portal Thrombosis in Cirrhosis: Role of Thrombophilic Disorders. Journal of Clinical Medicine. 2020; 9(9):2822. https://doi.org/10.3390/jcm9092822
Chicago/Turabian StyleFortea, José Ignacio, Inés García Carrera, Ángela Puente, Antonio Cuadrado, Patricia Huelin, Carmen Álvarez Tato, Paloma Álvarez Fernández, María del Rocío Pérez Montes, Javier Nuñez Céspedes, Ana Batlle López, and et al. 2020. "Portal Thrombosis in Cirrhosis: Role of Thrombophilic Disorders" Journal of Clinical Medicine 9, no. 9: 2822. https://doi.org/10.3390/jcm9092822
APA StyleFortea, J. I., Carrera, I. G., Puente, Á., Cuadrado, A., Huelin, P., Tato, C. Á., Fernández, P. Á., Montes, M. d. R. P., Céspedes, J. N., López, A. B., Sanchez, F. J. G., Hoyos, M. L., Crespo, J., & Fábrega, E. (2020). Portal Thrombosis in Cirrhosis: Role of Thrombophilic Disorders. Journal of Clinical Medicine, 9(9), 2822. https://doi.org/10.3390/jcm9092822