The Effects of Adding Transcutaneous Spinal Cord Stimulation (tSCS) to Sit-To-Stand Training in People with Spinal Cord Injury: A Pilot Study

 ,
,
Abstract
:1. Introduction
2. Experimental Section
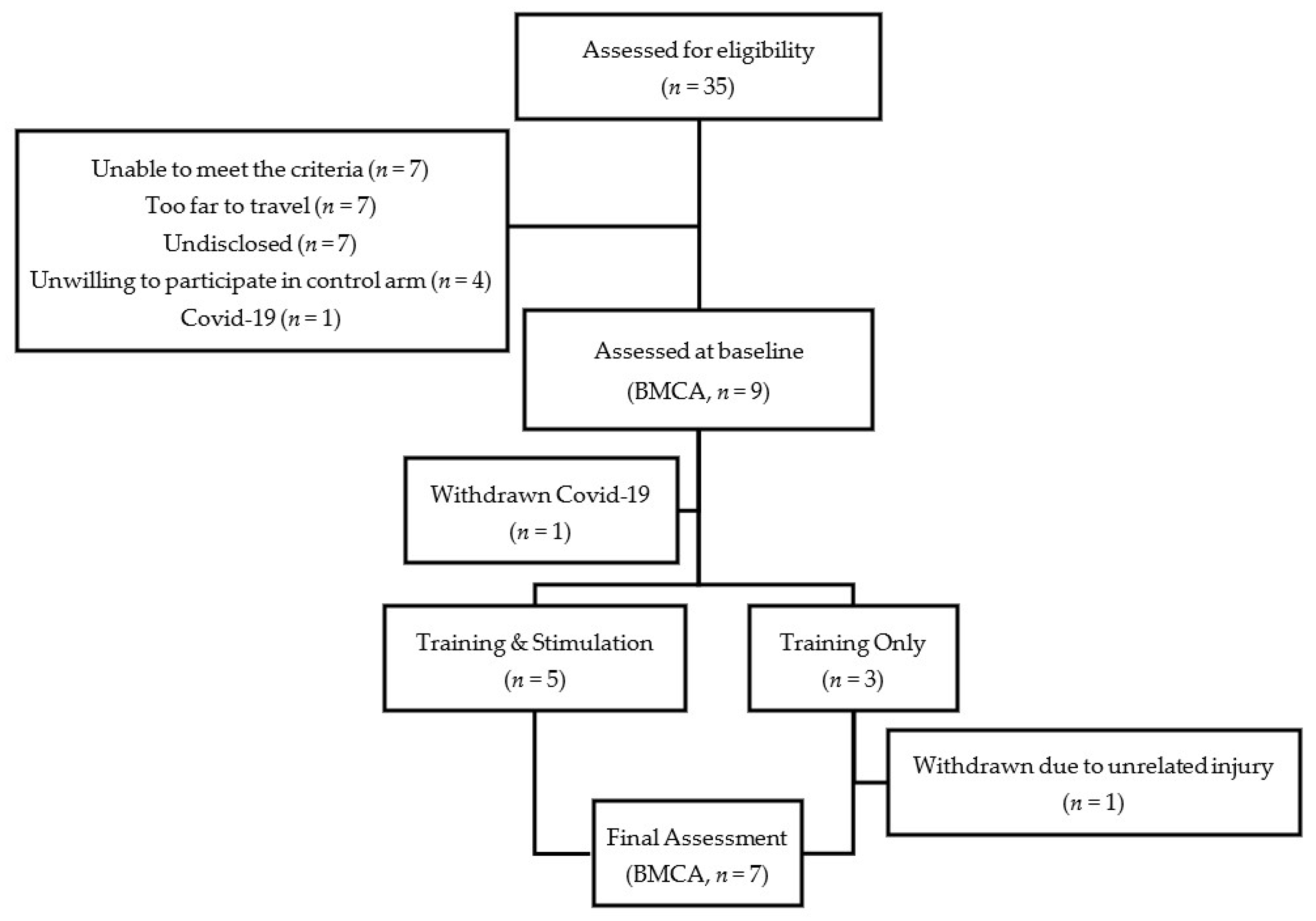
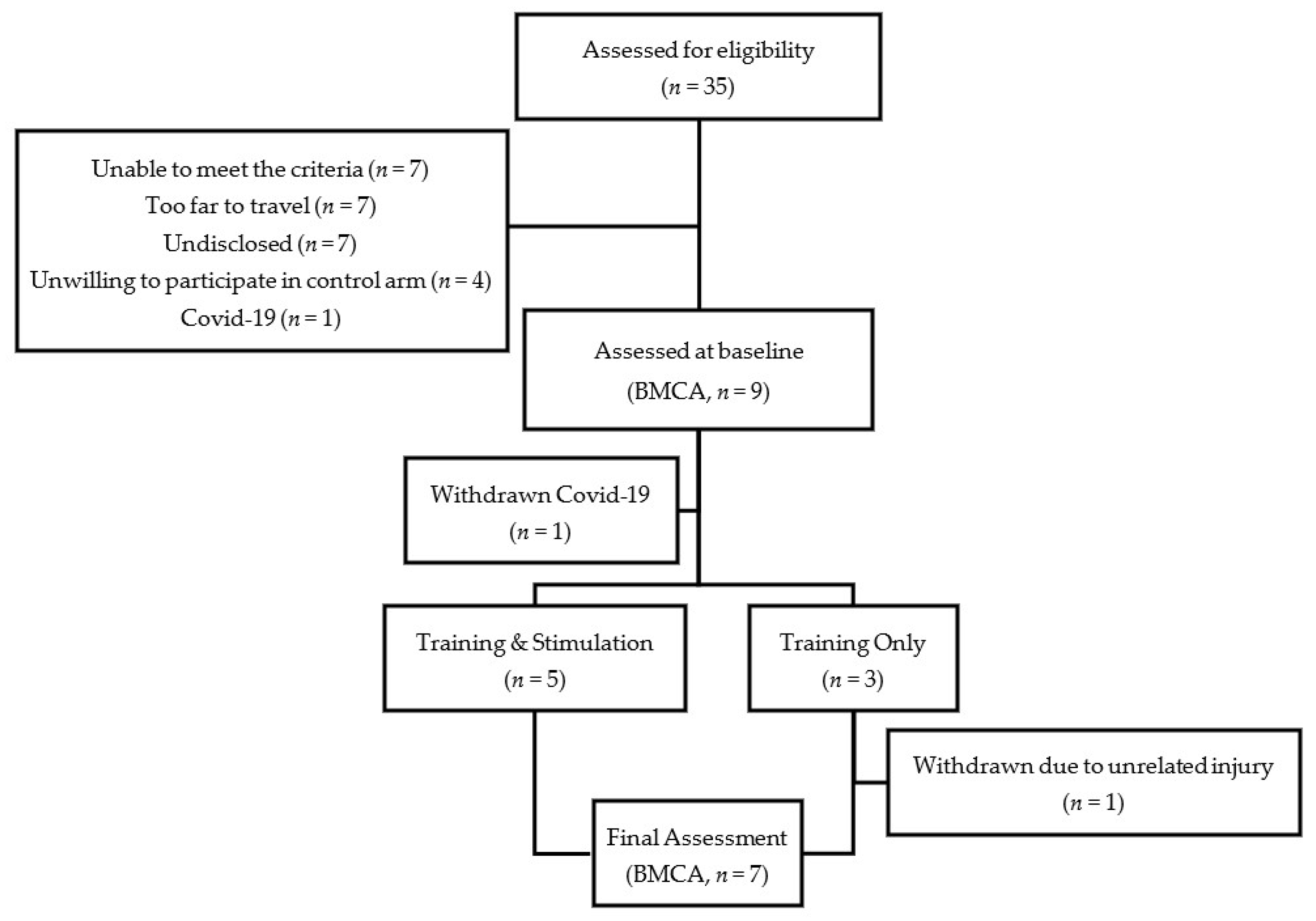
2.1. Participants
2.2. Study Design
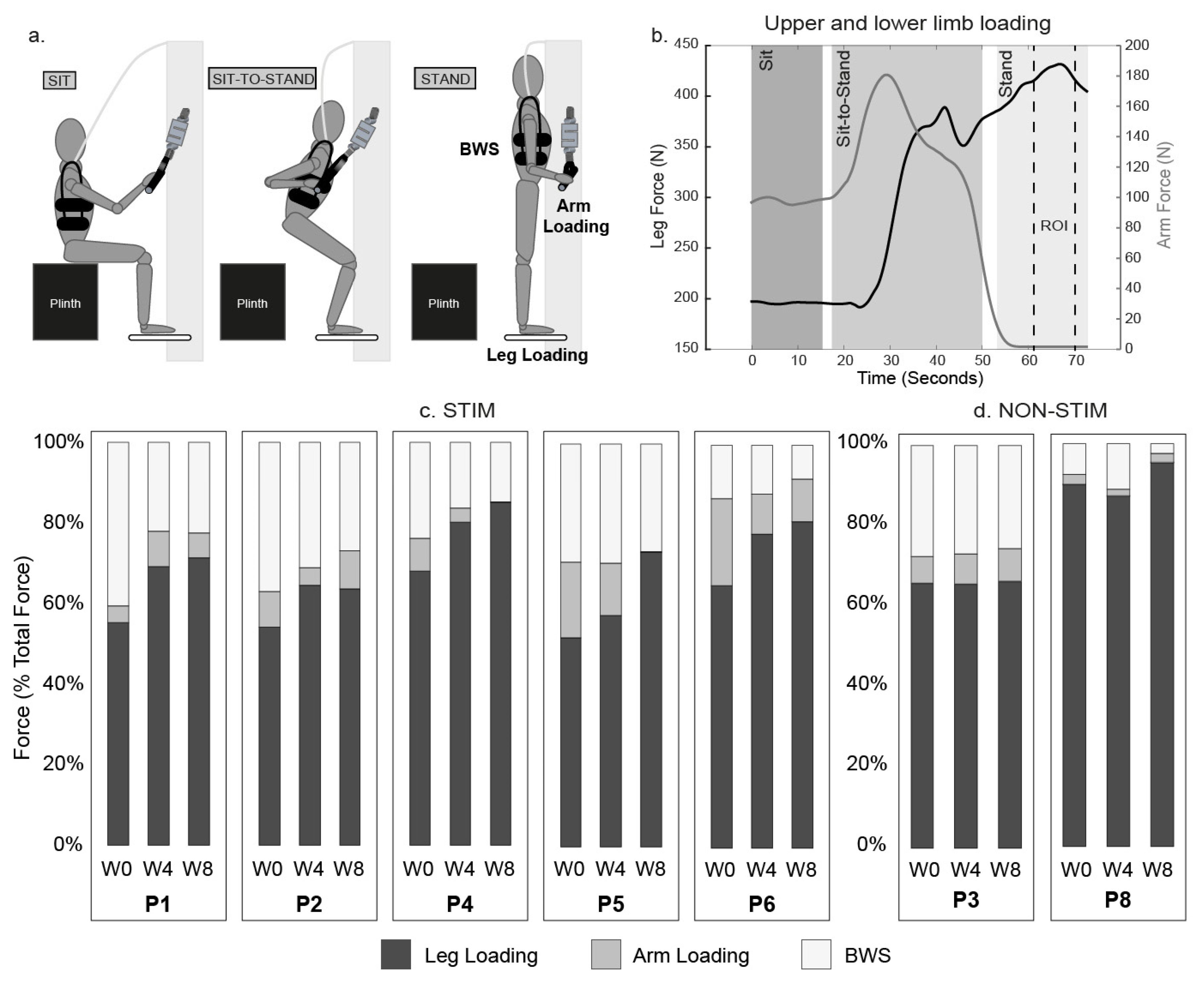
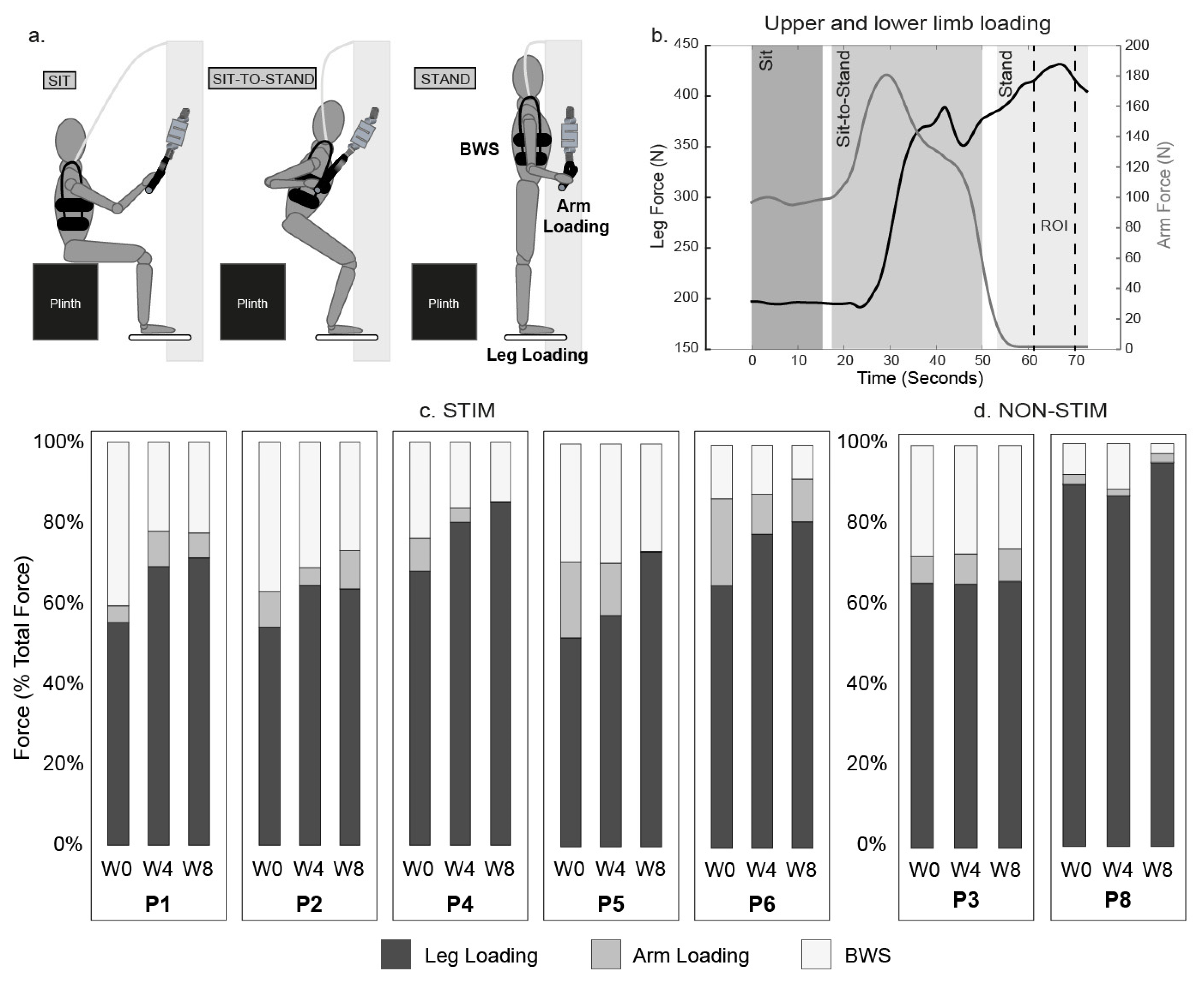
2.3. Intervention
2.4. Stimulation Parameters
2.5. Outcome Measures
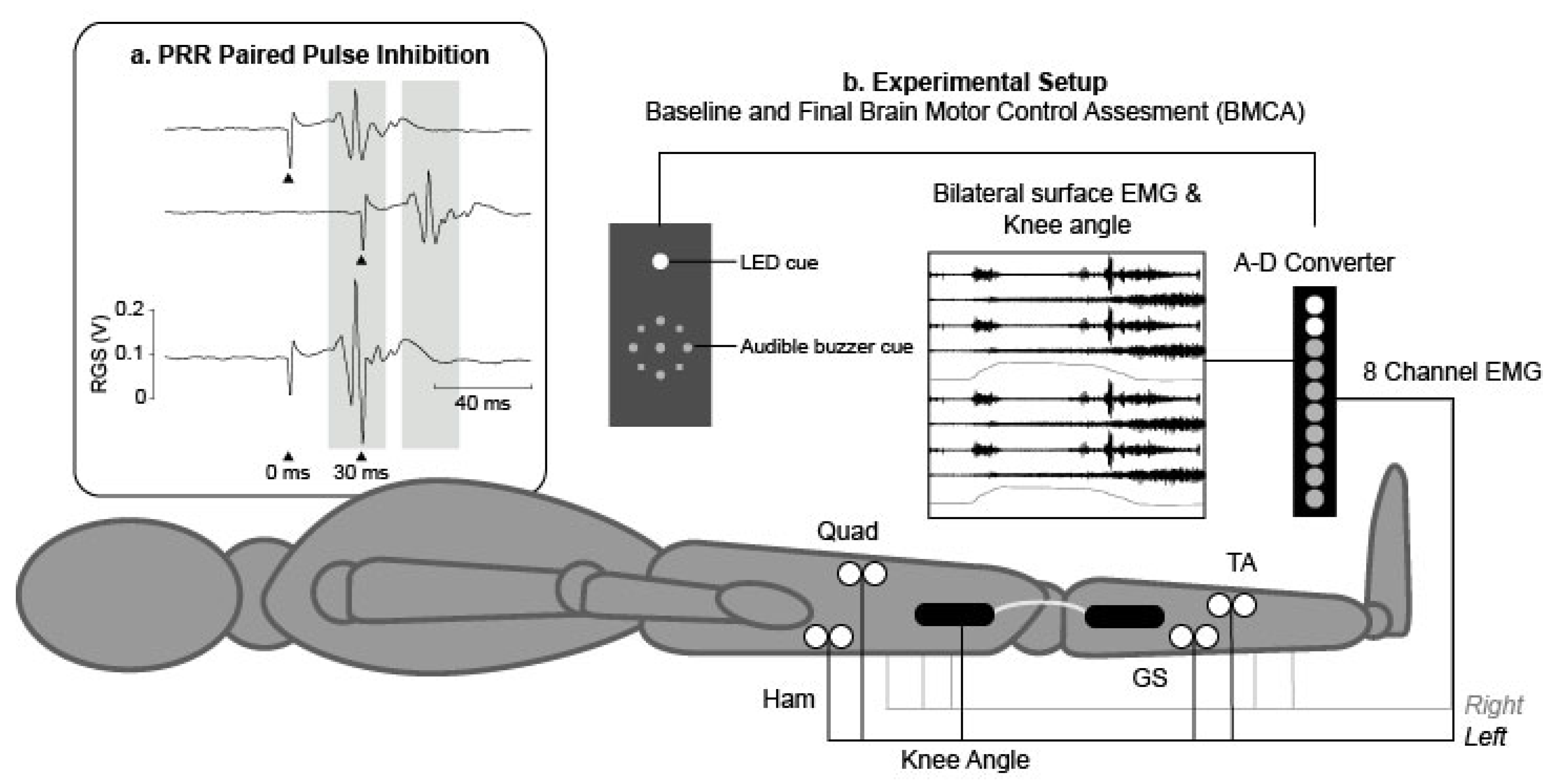
2.5.1. Baseline and Follow-Up Measures
2.5.2. Weekly Measures
2.6. Data Analysis
3. Results
3.1. Intervention
3.2. ISNCSCI Motor Scores
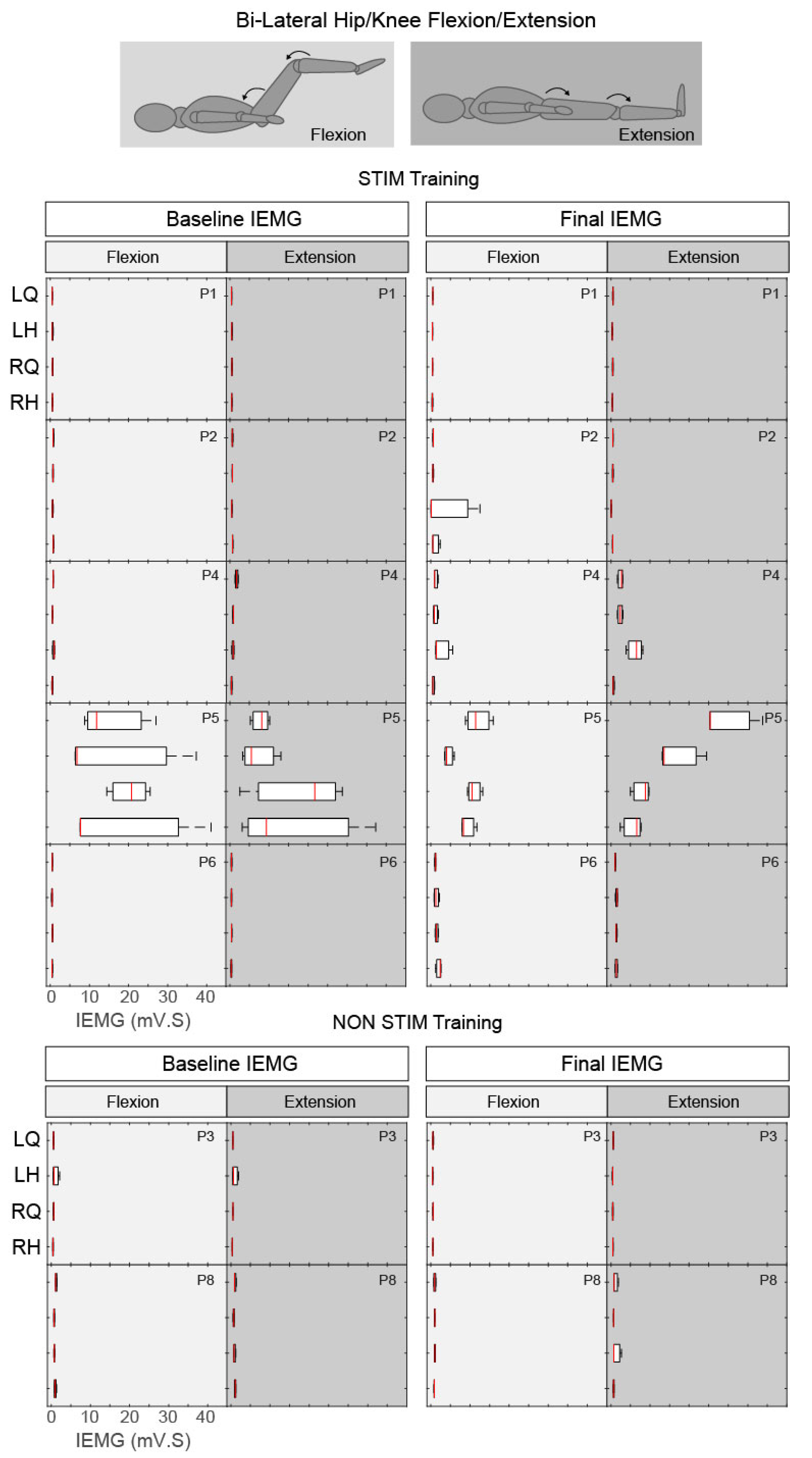
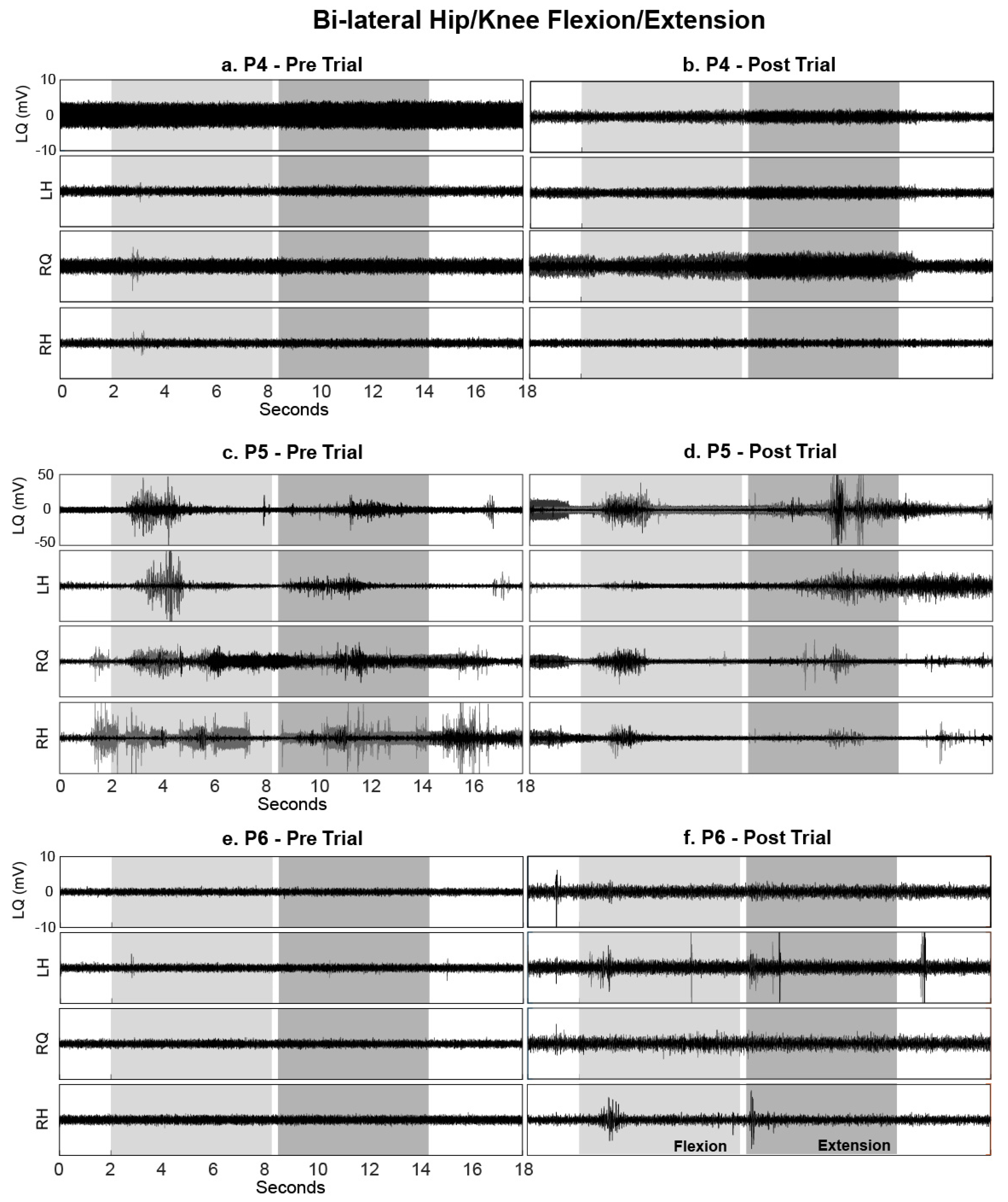
3.3. Brain Motor Control Assessment (BMCA)
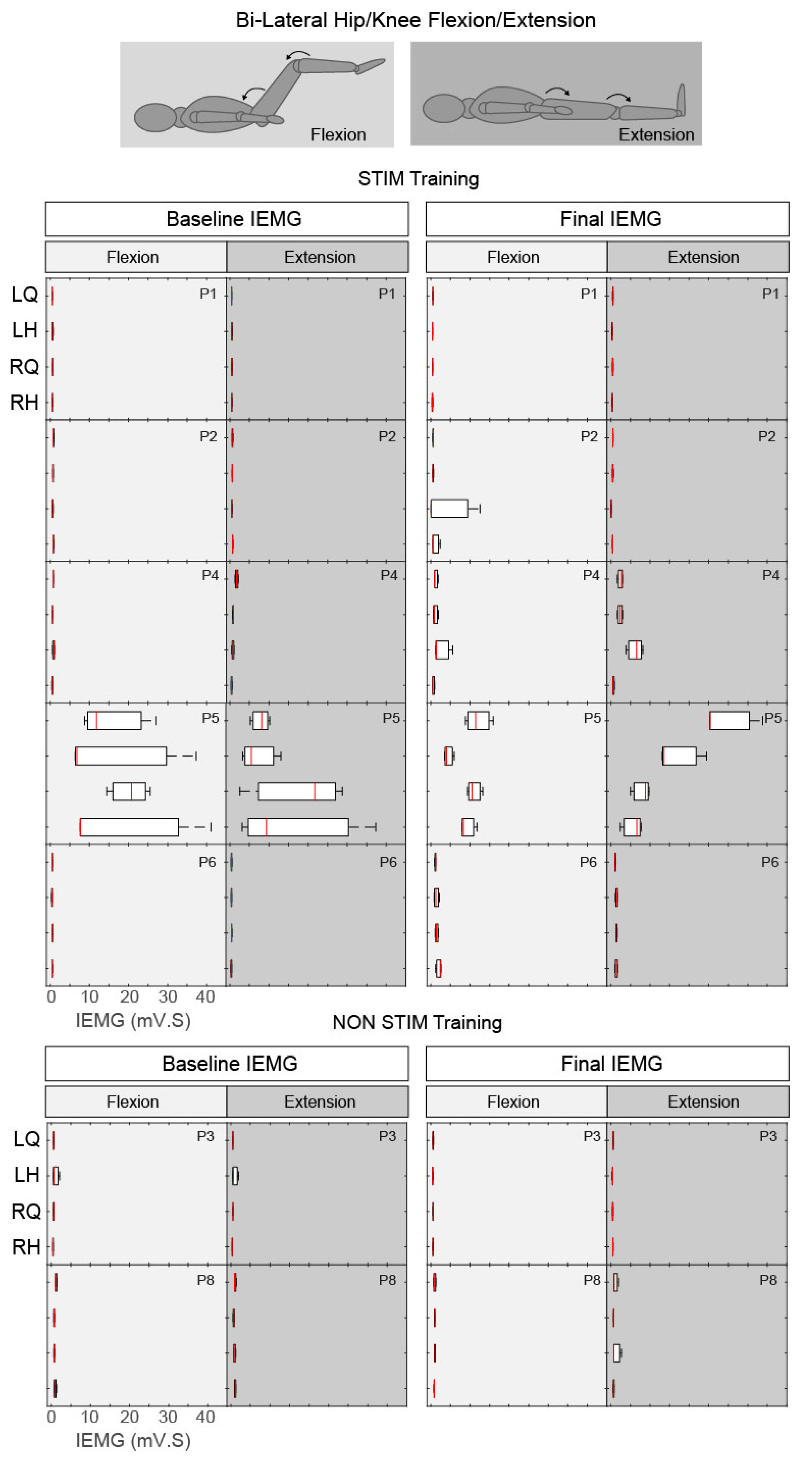
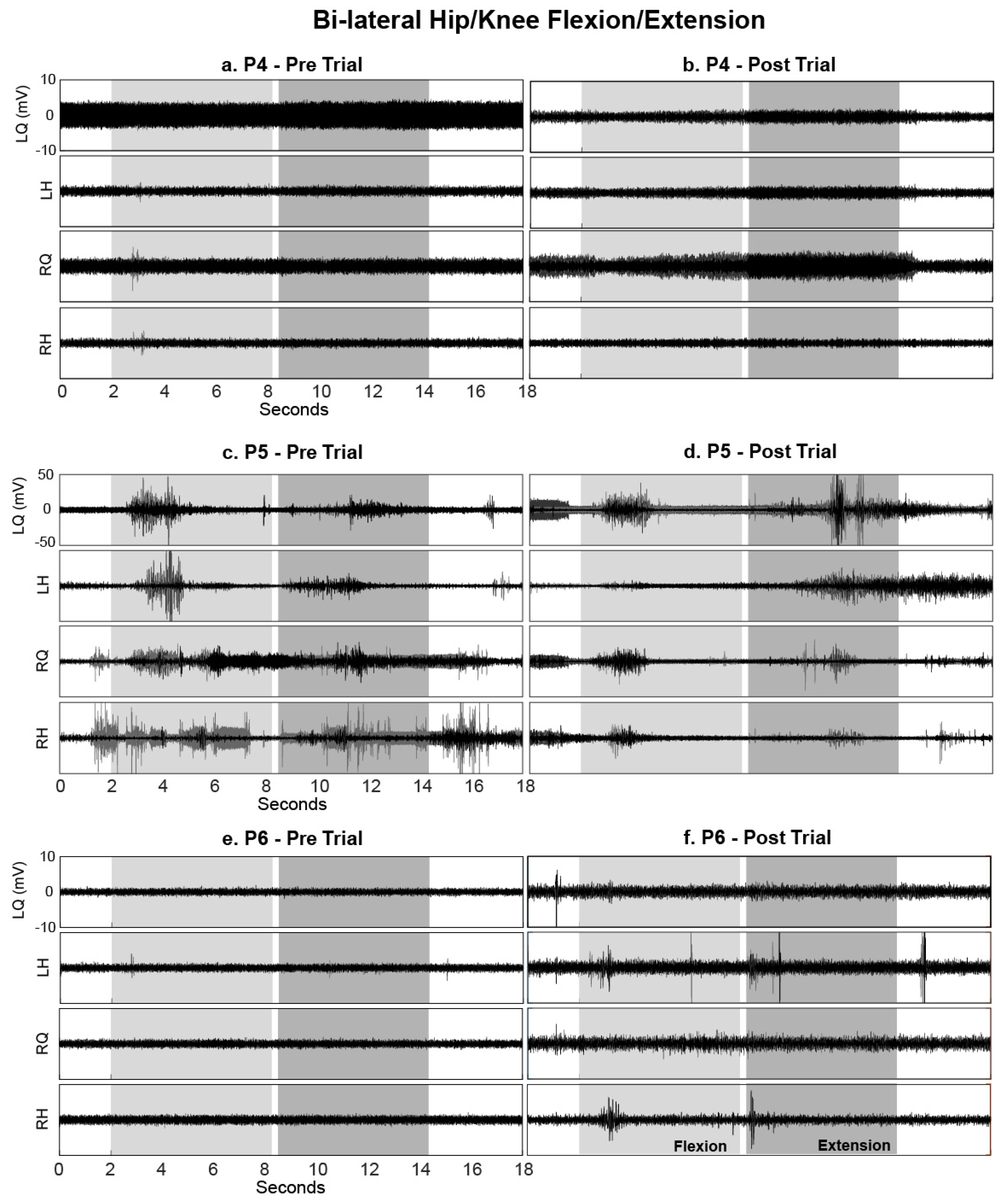
3.3.1. Hip/Knee Flexion and Extension
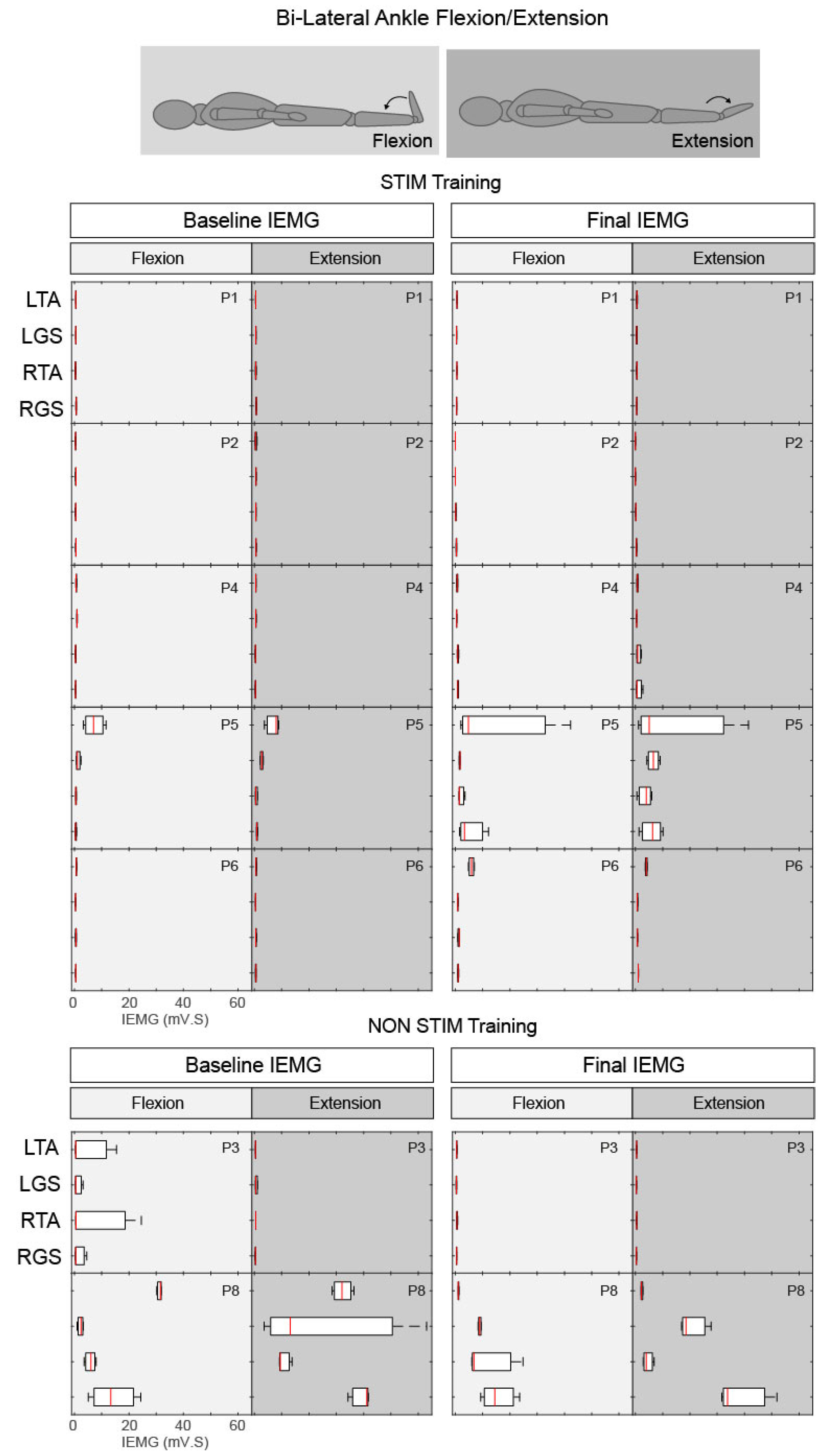
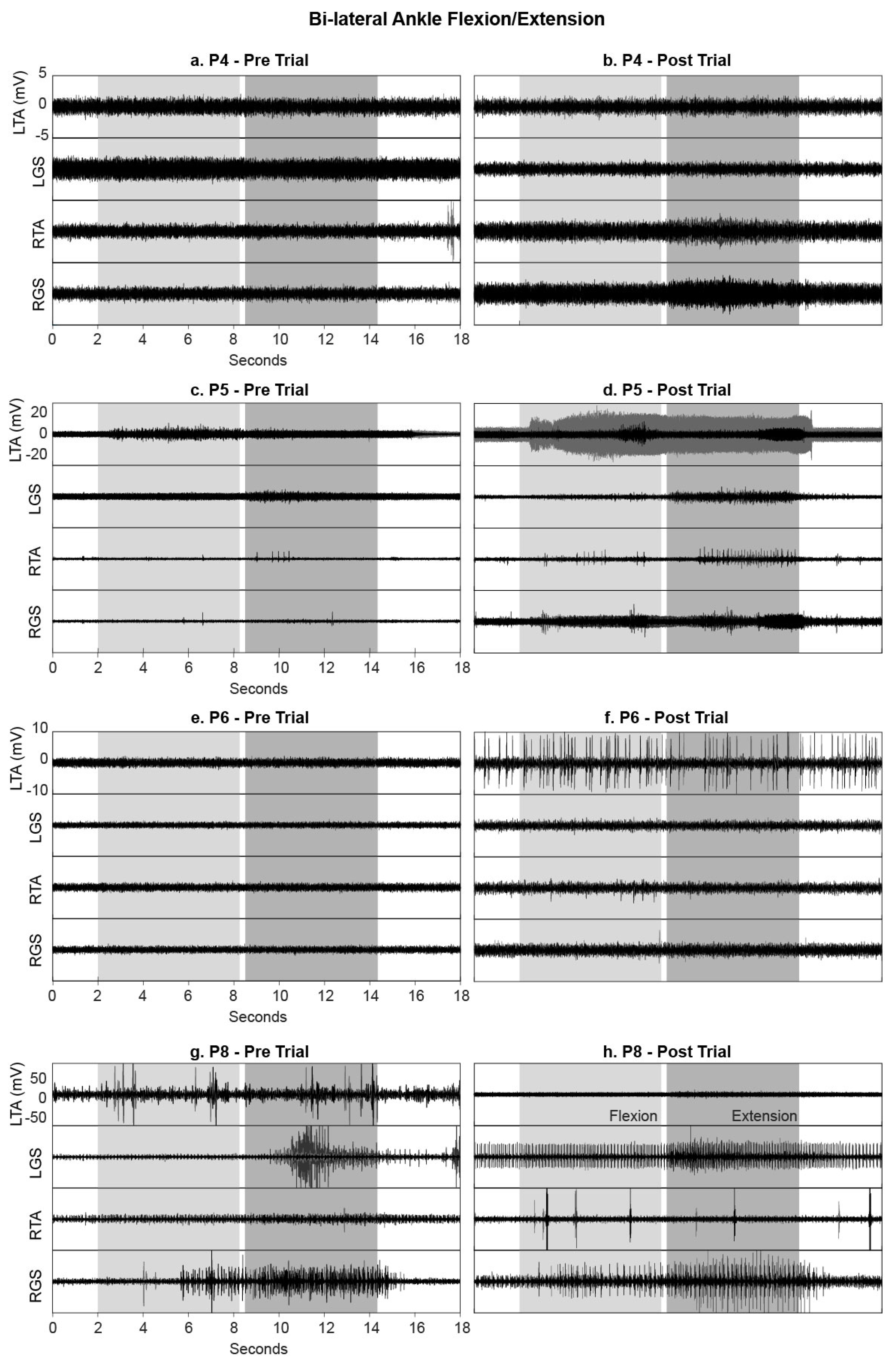
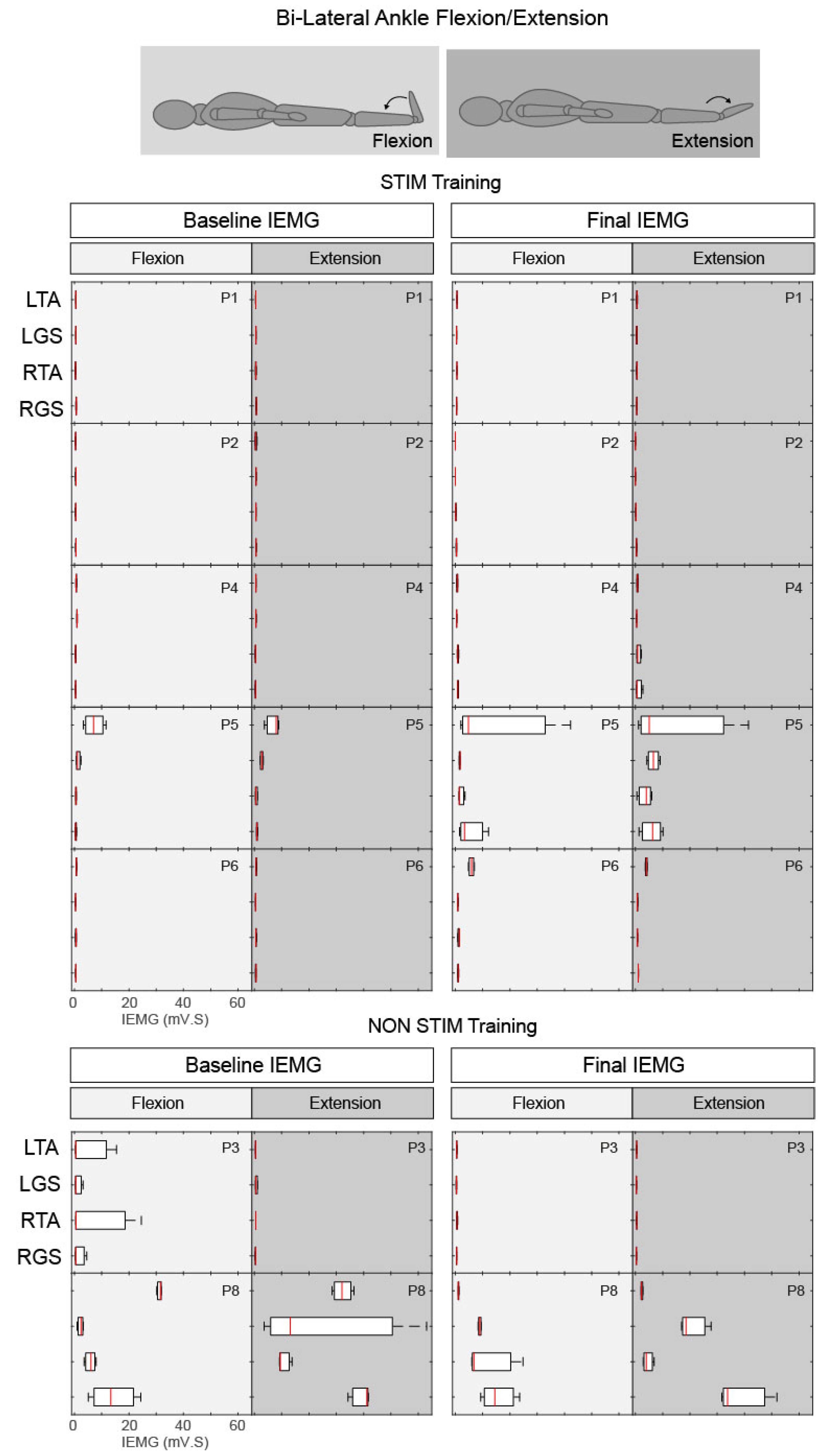
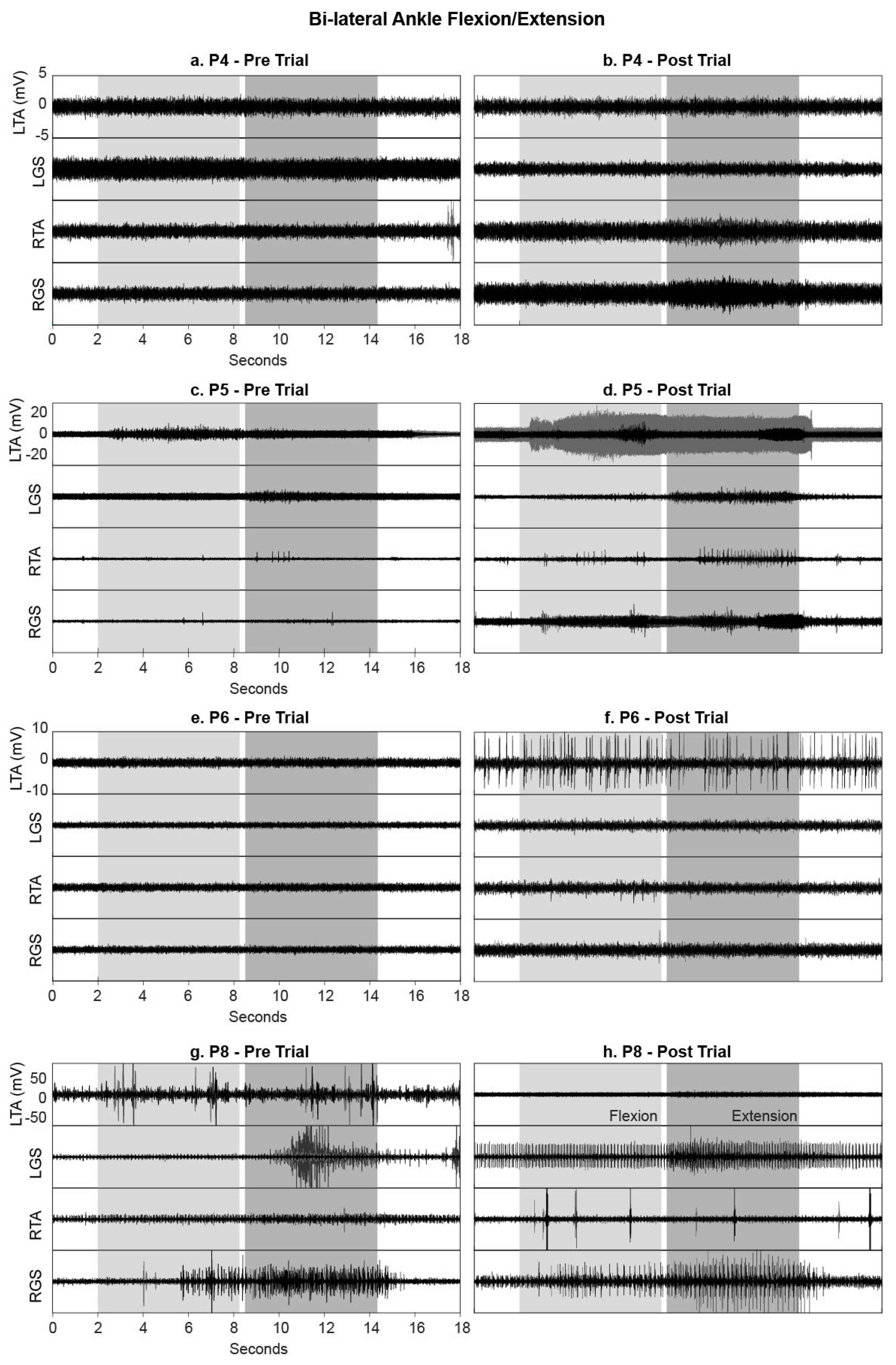
3.3.2. Ankle Flexion and Extension
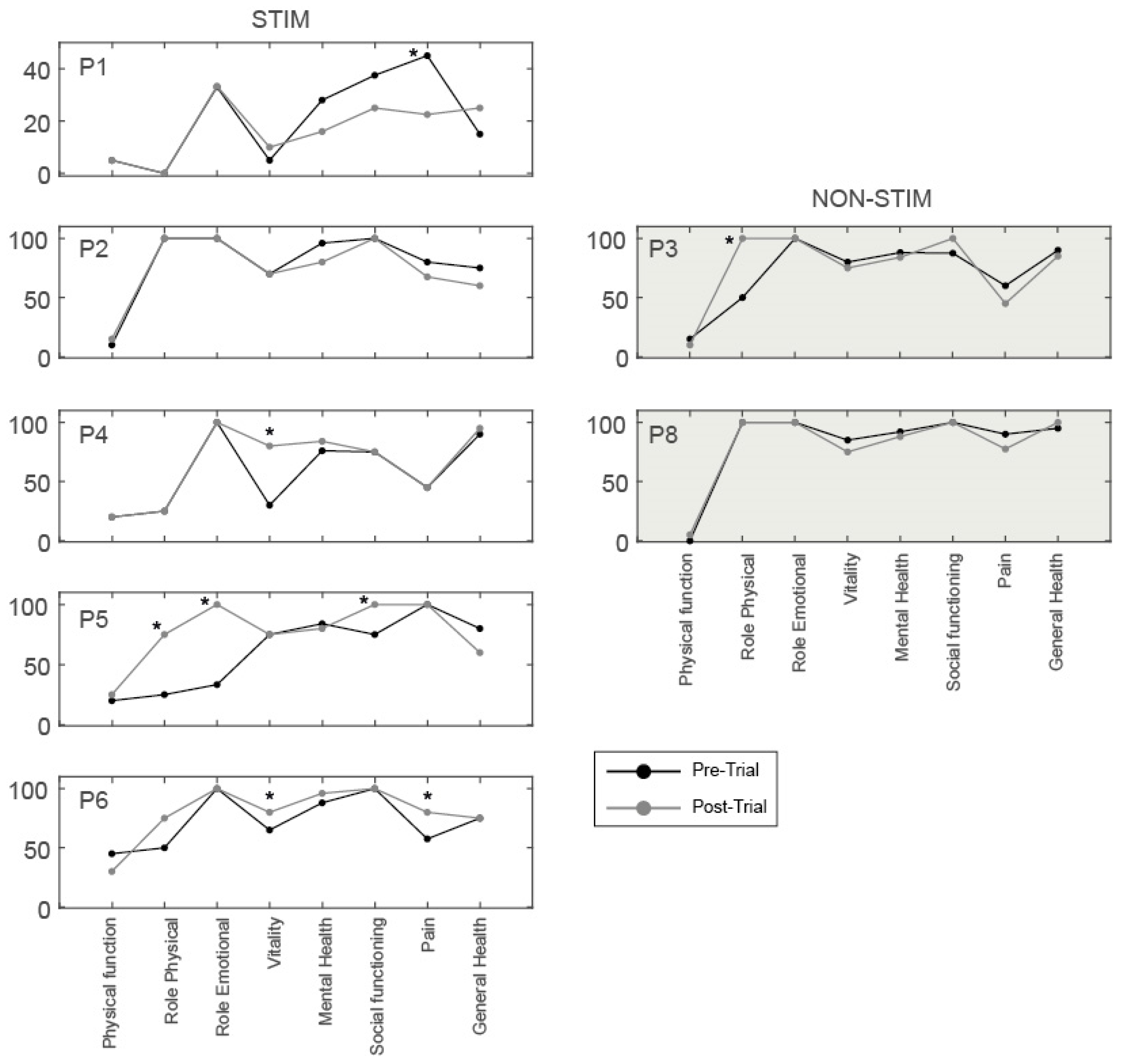
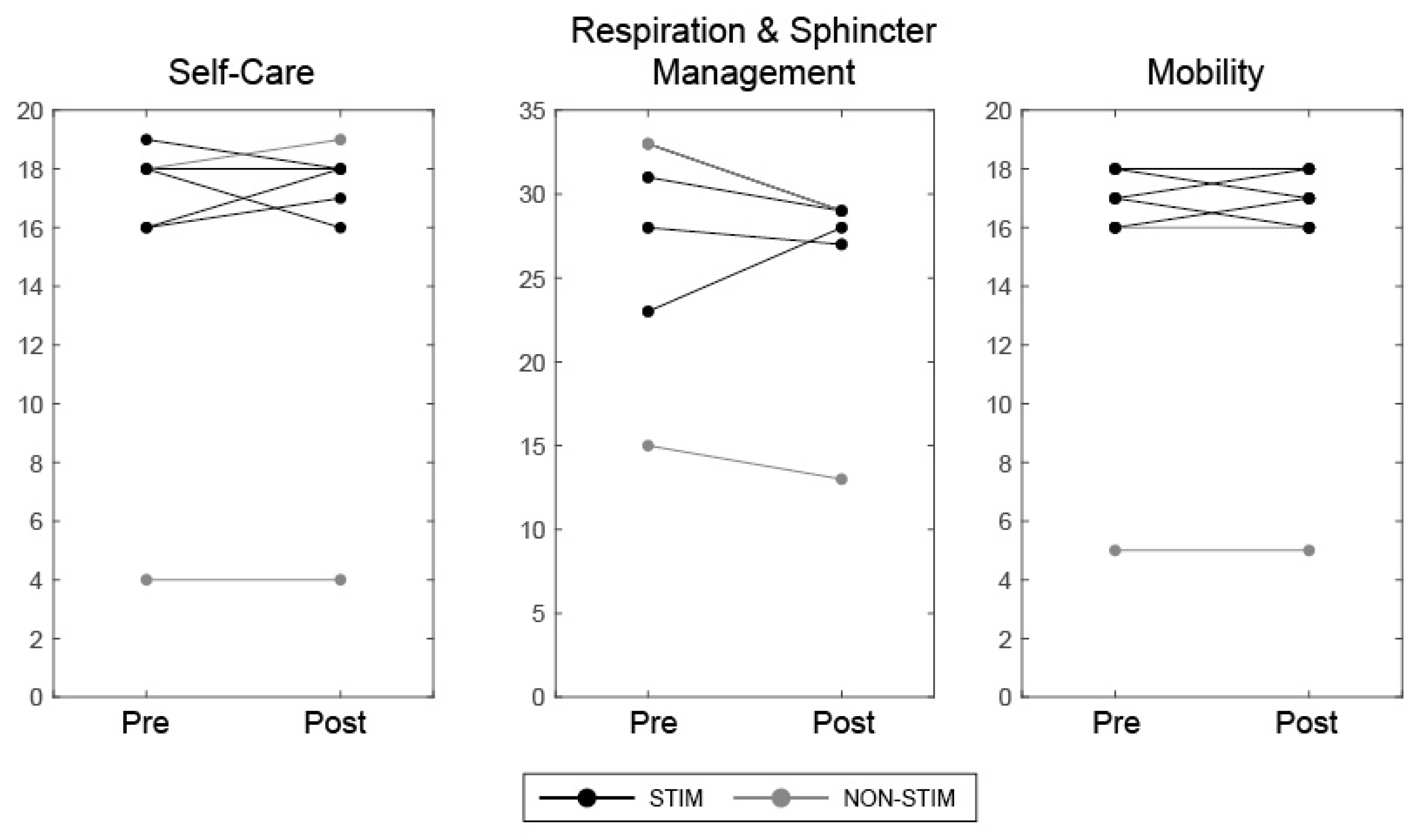
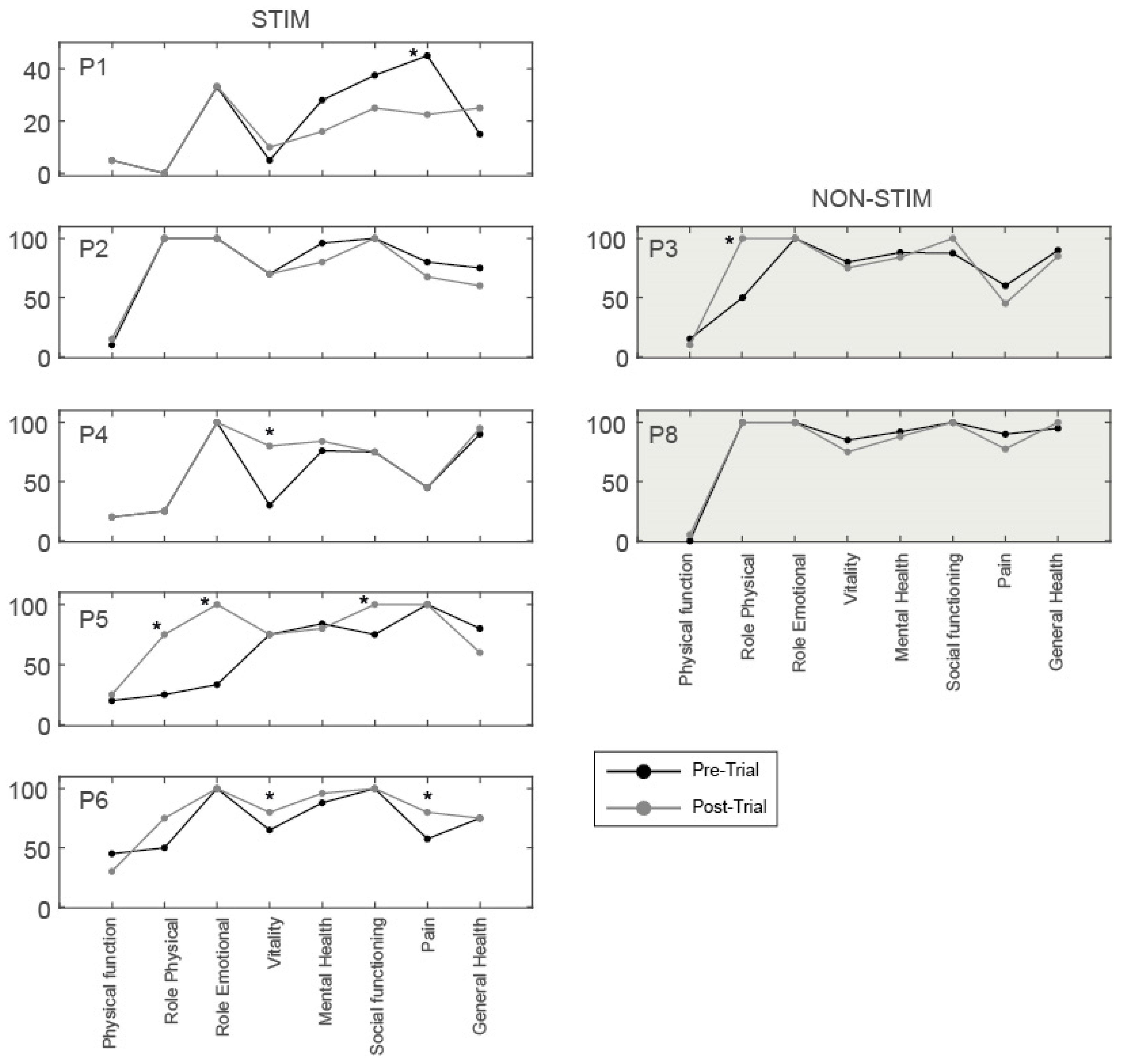
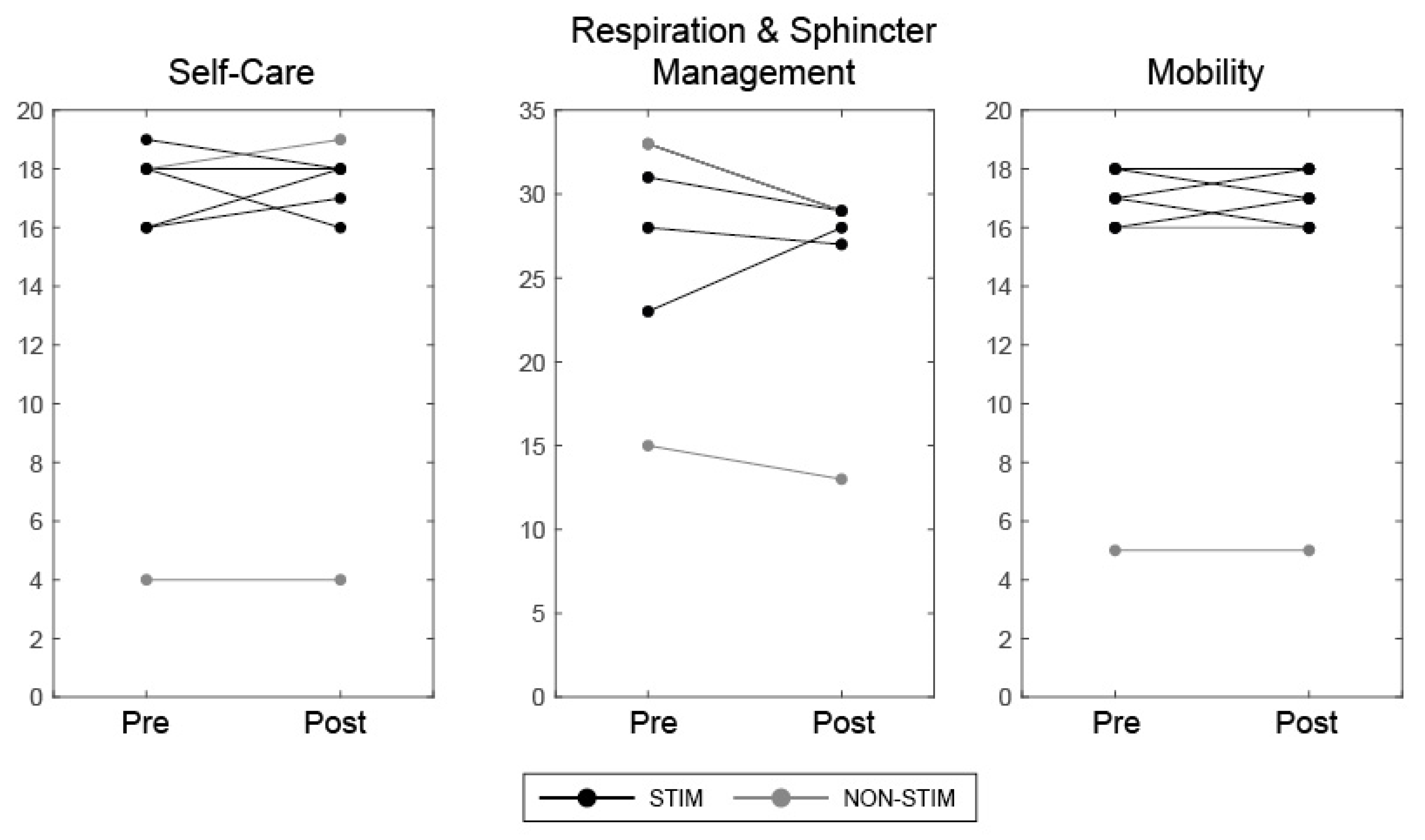
3.4. Health-Related Quality of Life Questionnaires
4. Discussion
4.1. Feasibility of Study Design
4.2. Recovery of Motor Control in the Presence of tSCS in the STIM Group
4.3. Recovery of Volitional Motor Control (in the Absence of tSCS)
4.4. Stimulation Parameters
4.5. Health-Related Quality of Life and Functional Independence
4.6. Limitations
4.7. Clinical Implications and Future Work
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spinal Cord Injury Centre Physiotherapy Lead Clinicians United Kingdom and Ireland. Clinical Guideline for Standing Adults Following Spinal Cord Injury; MASCIP: Aylesbury, UK, 2013. [Google Scholar]
- Hofer, A.S.; Schwab, M.E. Enhancing rehabilitation and functional recovery after brain and spinal cord trauma with electrical neuromodulation. Curr. Opin. Neurol. 2019, 32, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Ichiyama, R.M.; Gerasimenko, Y.P.; Zhong, H.; Roy, R.R.; Edgerton, V.R. Hindlimb stepping movements in complete spinal rats induced by epidural spinal cord stimulation. Neurosci. Lett. 2005, 383, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Lavrov, I.; Dy, C.J.; Fong, A.J.; Gerasimenko, Y.; Courtine, G.; Zhong, H.; Roy, R.R.; Edgerton, V.R. Epidural stimulation induced modulation of spinal locomotor networks in adult spinal rats. J. Neurosci. Off. J. Soc. Neurosci. 2008, 28, 6022–6029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitrijevic, M.R.; Gerasimenko, Y.; Pinter, M.M. Evidence for a spinal central pattern generator in humans. Ann. N. Y. Acad. Sci. 1998, 860, 360–376. [Google Scholar] [CrossRef] [PubMed]
- Minassian, K.; Jilge, B.; Rattay, F.; Pinter, M.M.; Binder, H.; Gerstenbrand, F.; Dimitrijevic, M.R. Stepping-like movements in humans with complete spinal cord injury induced by epidural stimulation of the lumbar cord: Electromyographic study of compound muscle action potentials. Spinal Cord 2004, 42, 401–416. [Google Scholar] [CrossRef] [Green Version]
- Jilge, B.; Minassian, K.; Rattay, F.; Pinter, M.M.; Gerstenbrand, F.; Binder, H.; Dimitrijevic, M.R. Initiating extension of the lower limbs in subjects with complete spinal cord injury by epidural lumbar cord stimulation. Exp. Brain Res. 2004, 154, 308–326. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Binder, H.; Minassian, K. Common neural structures activated by epidural and transcutaneous lumbar spinal cord stimulation: Elicitation of posterior root-muscle reflexes. PLoS ONE 2018, 13, e0192013. [Google Scholar] [CrossRef] [Green Version]
- Ladenbauer, J.; Minassian, K.; Hofstoetter, U.S.; Dimitrijevic, M.R.; Rattay, F. Stimulation of the human lumbar spinal cord with implanted and surface electrodes: A computer simulation study. IEEE Trans. Neural Syst. Rehabil. Eng. A Publ. IEEE Eng. Med. Biol. Soc. 2010, 18, 637–645. [Google Scholar] [CrossRef]
- Knikou, M. Neurophysiological characterization of transpinal evoked potentials in human leg muscles. Bioelectromagnetics 2013, 34, 630–640. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Freundl, B.; Binder, H.; Minassian, K. Recovery cycles of posterior root-muscle reflexes evoked by transcutaneous spinal cord stimulation and of the H reflex in individuals with intact and injured spinal cord. PLoS ONE 2019, 14, e0227057. [Google Scholar] [CrossRef] [Green Version]
- Minassian, K.; Persy, I.; Rattay, F.; Dimitrijevic, M.R.; Hofer, C.; Kern, H. Posterior root-muscle reflexes elicited by transcutaneous stimulation of the human lumbosacral cord. Muscle Nerve 2007, 35, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Minassian, K.; Persy, I.; Rattay, F.; Pinter, M.M.; Kern, H.; Dimitrijevic, M.R. Human lumbar cord circuitries can be activated by extrinsic tonic input to generate locomotor-like activity. Hum. Mov. Sci. 2007, 26, 275–295. [Google Scholar] [CrossRef] [PubMed]
- Sayenko, D.G.; Rath, M.; Ferguson, A.R.; Burdick, J.W.; Havton, L.A.; Edgerton, V.R.; Gerasimenko, Y.P. Self-Assisted Standing Enabled by Non-Invasive Spinal Stimulation after Spinal Cord Injury. J. Neurotrauma 2019, 36, 1435–1450. [Google Scholar] [CrossRef] [PubMed]
- Danner, S.M.; Krenn, M.; Hofstoetter, U.S.; Toth, A.; Mayr, W.; Minassian, K. Body Position Influences Which Neural Structures Are Recruited by Lumbar Transcutaneous Spinal Cord Stimulation. PLoS ONE 2016, 11, e0147479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angeli, C.A.; Edgerton, V.R.; Gerasimenko, Y.P.; Harkema, S.J. Altering spinal cord excitability enables voluntary movements after chronic complete paralysis in humans. Brain J. Neurol. 2014, 137, 1394–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harkema, S.; Gerasimenko, Y.; Hodes, J.; Burdick, J.; Angeli, C.; Chen, Y.; Ferreira, C.; Willhite, A.; Rejc, E.; Grossman, R.G.; et al. Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: A case study. Lancet 2011, 377, 1938–1947. [Google Scholar] [CrossRef] [Green Version]
- Darrow, D.; Balser, D.; Netoff, T.I.; Krassioukov, A.; Phillips, A.; Parr, A.; Samadani, U. Epidural Spinal Cord Stimulation Facilitates Immediate Restoration of Dormant Motor and Autonomic Supraspinal Pathways after Chronic Neurologically Complete Spinal Cord Injury. J. Neurotrauma 2019, 36, 2325–2336. [Google Scholar] [CrossRef] [Green Version]
- Angeli, C.A.; Boakye, M.; Morton, R.A.; Vogt, J.; Benton, K.; Chen, Y.; Ferreira, C.K.; Harkema, S.J. Recovery of Over-Ground Walking after Chronic Motor Complete Spinal Cord Injury. N. Engl. J. Med. 2018, 379, 1244–1250. [Google Scholar] [CrossRef]
- Grahn, P.J.; Lavrov, I.A.; Sayenko, D.G.; Van Straaten, M.G.; Gill, M.L.; Strommen, J.A.; Calvert, J.S.; Drubach, D.I.; Beck, L.A.; Linde, M.B.; et al. Enabling Task-Specific Volitional Motor Functions via Spinal Cord Neuromodulation in a Human With Paraplegia. Mayo Clin. Proc. 2017, 92, 544–554. [Google Scholar] [CrossRef]
- Huang, H.; He, J.; Herman, R.; Carhart, M.R. Modulation effects of epidural spinal cord stimulation on muscle activities during walking. IEEE Trans. Neural Syst. Rehabil. Eng. A Publ. IEEE Eng. Med. Biol. Soc. 2006, 14, 14–23. [Google Scholar] [CrossRef]
- Dimitrijevic, M.R.; Dimitrijevic, M.M.; Faganel, J.; Sherwood, A.M. Suprasegmentally induced motor unit activity in paralyzed muscles of patients with established spinal cord injury. Ann. Neurol. 1984, 16, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Hofstoetter, U.S.; Hofer, C.; Kern, H.; Danner, S.M.; Mayr, W.; Dimitrijevic, M.R.; Minassian, K. Effects of transcutaneous spinal cord stimulation on voluntary locomotor activity in an incomplete spinal cord injured individual. Biomed. Tech. Biomed. Eng. 2013. [Google Scholar] [CrossRef] [PubMed]
- Hofstoetter, U.S.; Krenn, M.; Danner, S.M.; Hofer, C.; Kern, H.; McKay, W.B.; Mayr, W.; Minassian, K. Augmentation of Voluntary Locomotor Activity by Transcutaneous Spinal Cord Stimulation in Motor-Incomplete Spinal Cord-Injured Individuals. Artif. Organs 2015, 39, E176–E186. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; McKay, W.B.; Tansey, K.E.; Mayr, W.; Kern, H.; Minassian, K. Modification of spasticity by transcutaneous spinal cord stimulation in individuals with incomplete spinal cord injury. J. Spinal Cord Med. 2014, 37, 202–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofstoetter, U.S.; Freundl, B.; Danner, S.M.; Krenn, M.J.; Mayr, W.; Binder, H.; Minassian, K. Transcutaneous Spinal Cord Stimulation Induces Temporary Attenuation of Spasticity in Individuals with Spinal Cord Injury. J. Neurotrauma 2019. [Google Scholar] [CrossRef] [PubMed]
- Estes, S.P.; Iddings, J.A.; Field-Fote, E.C. Priming Neural Circuits to Modulate Spinal Reflex Excitability. Front. Neurol. 2017, 8, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtine, G.; Gerasimenko, Y.; van den Brand, R.; Yew, A.; Musienko, P.; Zhong, H.; Song, B.; Ao, Y.; Ichiyama, R.M.; Lavrov, I.; et al. Transformation of nonfunctional spinal circuits into functional states after the loss of brain input. Nat. Neurosci. 2009, 12, 1333–1342. [Google Scholar] [CrossRef]
- Ichiyama, R.M.; Courtine, G.; Gerasimenko, Y.P.; Yang, G.J.; van den Brand, R.; Lavrov, I.A.; Zhong, H.; Roy, R.R.; Edgerton, V.R. Step training reinforces specific spinal locomotor circuitry in adult spinal rats. J. Neurosci. 2008, 28, 7370–7375. [Google Scholar] [CrossRef] [Green Version]
- Van den Brand, R.; Heutschi, J.; Barraud, Q.; DiGiovanna, J.; Bartholdi, K.; Huerlimann, M.; Friedli, L.; Vollenweider, I.; Moraud, E.M.; Duis, S.; et al. Restoring voluntary control of locomotion after paralyzing spinal cord injury. Science 2012, 336, 1182–1185. [Google Scholar] [CrossRef] [Green Version]
- Carhart, M.R.; He, J.; Herman, R.; D‘Luzansky, S.; Willis, W.T. Epidural spinal-cord stimulation facilitates recovery of functional walking following incomplete spinal-cord injury. IEEE Trans. Neural Syst. Rehabil. Eng. A Publ. IEEE Eng. Med. Biol. Soc. 2004, 12, 32–42. [Google Scholar] [CrossRef]
- Gill, M.L.; Grahn, P.J.; Calvert, J.S.; Linde, M.B.; Lavrov, I.A.; Strommen, J.A.; Beck, L.A.; Sayenko, D.G.; Van Straaten, M.G.; Drubach, D.I.; et al. Neuromodulation of lumbosacral spinal networks enables independent stepping after complete paraplegia. Nat. Med. 2018, 24, 1677–1682. [Google Scholar] [CrossRef] [PubMed]
- Wagner, F.B.; Mignardot, J.B.; Le Goff-Mignardot, C.G.; Demesmaeker, R.; Komi, S.; Capogrosso, M.; Rowald, A.; Seanez, I.; Caban, M.; Pirondini, E.; et al. Targeted neurotechnology restores walking in humans with spinal cord injury. Nature 2018, 563, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Peña Pino, I.; Hoover, C.; Venkatesh, S.; Ahmadi, A.; Sturtevant, D.; Patrick, N.; Freeman, D.; Parr, A.; Samadani, U.; Balser, D.; et al. Long-Term Spinal Cord Stimulation After Chronic Complete Spinal Cord Injury Enables Volitional Movement in the Absence of Stimulation. Front. Syst. Neurosci. 2020, 14. [Google Scholar] [CrossRef]
- Gerasimenko, Y.P.; Lu, D.C.; Modaber, M.; Zdunowski, S.; Gad, P.; Sayenko, D.G.; Morikawa, E.; Haakana, P.; Ferguson, A.R.; Roy, R.R.; et al. Noninvasive Reactivation of Motor Descending Control after Paralysis. J. Neurotrauma 2015, 32, 1968–1980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerasimenko, Y.; Gorodnichev, R.; Puhov, A.; Moshonkina, T.; Savochin, A.; Selionov, V.; Roy, R.R.; Lu, D.C.; Edgerton, V.R. Initiation and modulation of locomotor circuitry output with multisite transcutaneous electrical stimulation of the spinal cord in noninjured humans. J. Neurophysiol. 2015, 113, 834–842. [Google Scholar] [CrossRef]
- Andrews, J.C.; Stein, R.B.; Roy, F.D. Post-activation depression in the human soleus muscle using peripheral nerve and transcutaneous spinal stimulation. Neurosci. Lett. 2015, 589, 144–149. [Google Scholar] [CrossRef]
- McKay, W.B.; Sherwood, A.M.; Tang, S.F. Appendix 1. A Manual for the Neurophysiological Assessment of Motor Control: The Brain Motor Control Assessment (BMCA) Protoco. In Restorative Neurology of the Injured Spinal Cord; Dimitrijevic, M.R., Kakulas, B., McKay, W.B., Vrbova, G., Eds.; Oxford University Press: New York, NY, USA, 2011; pp. 262–283. [Google Scholar]
- Ware, J.E., Jr. SF-36 Health Survey. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment, 2nd ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1999; pp. 1227–1246. [Google Scholar]
- Haran, M.J.; Lee, B.B.; King, M.T.; Marial, O.; Stockler, M.R. Health status rated with the Medical Outcomes Study 36-Item Short-Form Health Survey after spinal cord injury. Arch. Phys. Med. Rehabil. 2005, 86, 2290–2295. [Google Scholar] [CrossRef]
- Catz, A.; Itzkovich, M.; Agranov, E.; Ring, H.; Tamir, A. SCIM—Spinal cord independence measure: A new disability scale for patients with spinal cord lesions. Spinal Cord 1997, 35, 850–856. [Google Scholar] [CrossRef]
- Catz, A.; Itzkovich, M.; Agranov, E.; Ring, H.; Tamir, A. The spinal cord independence measure (SCIM): Sensitivity to functional changes in subgroups of spinal cord lesion patients. Spinal Cord 2001, 39, 97–100. [Google Scholar] [CrossRef]
- Lin, M.R.; Hwang, H.F.; Chen, C.Y.; Chiu, W.T. Comparisons of the brief form of the World Health Organization Quality of Life and Short Form-36 for persons with spinal cord injuries. Am. J. Phys. Med. Rehabil. Assoc. Acad. Physiatr. 2007, 86, 104–113. [Google Scholar] [CrossRef]
- Scivoletto, G.; Tamburella, F.; Laurenza, L.; Molinari, M. The spinal cord independence measure: How much change is clinically significant for spinal cord injury subjects. Disabil. Rehabil. 2013, 35, 1808–1813. [Google Scholar] [CrossRef]
- McKay, W.B.; Lim, H.K.; Priebe, M.M.; Stokic, D.S.; Sherwood, A.M. Clinical neurophysiological assessment of residual motor control in post-spinal cord injury paralysis. Neurorehabilit. Neural Repair 2004, 18, 144–153. [Google Scholar] [CrossRef]
- McKay, W.B.; Ovechkin, A.V.; Vitaz, T.W.; Terson de Paleville, D.G.; Harkema, S.J. Neurophysiological characterization of motor recovery in acute spinal cord injury. Spinal Cord 2011, 49, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Lavrov, I.; Gerasimenko, Y.; Burdick, J.; Zhong, H.; Roy, R.R.; Edgerton, V.R. Integrating multiple sensory systems to modulate neural networks controlling posture. J. Neurophysiol. 2015, 114, 3306–3314. [Google Scholar] [CrossRef] [Green Version]
- Sherwood, A.M.; Dimitrijevic, M.R.; McKay, W.B. Evidence of subclinical brain influence in clinically complete spinal cord injury: Discomplete SCI. J. Neurol. Sci. 1992, 110, 90–98. [Google Scholar] [CrossRef]
- Fawcett, J.W.; Curt, A.; Steeves, J.D.; Coleman, W.P.; Tuszynski, M.H.; Lammertse, D.; Bartlett, P.F.; Blight, A.R.; Dietz, V.; Ditunno, J.; et al. Guidelines for the conduct of clinical trials for spinal cord injury as developed by the ICCP panel: Spontaneous recovery after spinal cord injury and statistical power needed for therapeutic clinical trials. Spinal Cord 2007, 45, 190–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dietz, V.; Fouad, K. Restoration of sensorimotor functions after spinal cord injury. Brain 2014, 137, 654–667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minassian, K.; Hofstoetter, U.S. Spinal Cord Stimulation and Augmentative Control Strategies for Leg Movement after Spinal Paralysis in Humans. CNS Neurosci. Ther. 2016, 22, 262–270. [Google Scholar] [CrossRef]
- Calvert, J.S.; Grahn, P.J.; Zhao, K.D.; Lee, K.H. Emergence of Epidural Electrical Stimulation to Facilitate Sensorimotor Network Functionality After Spinal Cord Injury. Neuromodul. J. Int. Neuromodul. Soc. 2019, 22, 244–252. [Google Scholar] [CrossRef]
- Minassian, K.; McKay, W.B.; Binder, H.; Hofstoetter, U.S. Targeting Lumbar Spinal Neural Circuitry by Epidural Stimulation to Restore Motor Function After Spinal Cord Injury. Neurotherapeutics 2016, 13, 284–294. [Google Scholar] [CrossRef] [Green Version]
- Edgerton, V.R.; Courtine, G.; Gerasimenko, Y.P.; Lavrov, I.; Ichiyama, R.M.; Fong, A.J.; Cai, L.L.; Otoshi, C.K.; Tillakaratne, N.J.; Burdick, J.W.; et al. Training locomotor networks. Brain Res. Rev. 2008, 57, 241–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinter, M.M.; Gerstenbrand, F.; Dimitrijevic, M.R. Epidural electrical stimulation of posterior structures of the human lumbosacral cord: 3. Control Of spasticity. Spinal Cord 2000, 38, 524–531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sangari, S.; Lundell, H.; Kirshblum, S.; Perez, M.A. Residual descending motor pathways influence spasticity after spinal cord injury. Ann. Neurol. 2019, 86, 28–41. [Google Scholar] [CrossRef] [PubMed]
- Knikou, M.; Murray, L.M. Repeated transspinal stimulation decreases soleus H-reflex excitability and restores spinal inhibition in human spinal cord injury. PLoS ONE 2019, 14, e0223135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barolat, G.; Singh-Sahni, K.; Staas, W.E., Jr.; Shatin, D.; Ketcik, B.; Allen, K. Epidural spinal cord stimulation in the management of spasms in spinal cord injury: A prospective study. Stereotact. Funct. Neurosurg. 1995, 64, 153–164. [Google Scholar] [CrossRef]
- Dimitrijevic, M.M.; Dimitrijevic, M.R.; Illis, L.S.; Nakajima, K.; Sharkey, P.C.; Sherwood, A.M. Spinal cord stimulation for the control of spasticity in patients with chronic spinal cord injury: I. Clinical observations. Cent. Nerv. Syst. Trauma J. Am. Paralys. Assoc. 1986, 3, 129–144. [Google Scholar] [CrossRef]
- Rejc, E.; Angeli, C.; Harkema, S. Effects of Lumbosacral Spinal Cord Epidural Stimulation for Standing after Chronic Complete Paralysis in Humans. PLoS ONE 2015, 10, e0133998. [Google Scholar] [CrossRef] [Green Version]
- Gerasimenko, Y.; Roy, R.R.; Edgerton, V.R. Epidural stimulation: Comparison of the spinal circuits that generate and control locomotion in rats, cats and humans. Exp. Neurol. 2008, 209, 417–425. [Google Scholar] [CrossRef] [Green Version]
- Sayenko, D.G.; Angeli, C.; Harkema, S.J.; Edgerton, V.R.; Gerasimenko, Y.P. Neuromodulation of evoked muscle potentials induced by epidural spinal-cord stimulation in paralyzed individuals. J. Neurophysiol. 2014, 111, 1088–1099. [Google Scholar] [CrossRef]
- Hofstoetter, U.S.; Minassian, K.; Hofer, C.; Mayr, W.; Rattay, F.; Dimitrijevic, M.R. Modification of reflex responses to lumbar posterior root stimulation by motor tasks in healthy subjects. Artif. Organs 2008, 32, 644–648. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Height (Meters) | Weight (Kg) | Sex (M/F) | Injury Level | Cause of Injury | AIS Grade | Time Since Injury | Group | ||
|---|---|---|---|---|---|---|---|---|---|---|
| P1 | 37 | 1.83 | 100 | M | T3 | Traumatic | Motor vehicle | A | 1yr 6m | STIM |
| P2 | 38 | 1.92 | 83 | M | T5 | Traumatic | Motor vehicle | A | 2 yr 2 m | STIM |
| P3 | 38 | 1.72 | 59 | F | T6 | Traumatic | Motor vehicle | A | 8 yr 4 m | NON-STIM |
| P4 | 41 | 1.71 | 58 | F | T5 | Non-Traumatic | Spinal tumor | C | 1 yr 5 m | STIM |
| P5 | 28 | 1.98 | 80 | M | C6/7 | Traumatic | Sports injury | D | 1 yr 1 m | STIM |
| P6 | 40 | 1.59 | 61 | F | T10 | Traumatic | Fall | A * | 9 yr 0 m | STIM |
| P7 W | 49 | 1.98 | 121 | M | T10 | Non-Traumatic | Vascular | B | 2 yr 11 m | NON-STIM |
| P8 | 31 | 1.81 | 80 | M | C5 | Traumatic | Fall | C | 7 yr 11 m | NON-STIM |
| P9 W | 69 | 1.75 | 70 | M | T6 | Non- Traumatic | Vascular | A | 1 yr 4 m | NON-STIM |
| PRR Threshold (mA) | Average Weekly Stimulation Thresholds during Training (mA) | Paraesthesia during Training (Y/N) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BL | W1 | W2 | W3 | W4 | W5 | W6 | W7 | W8 | ||
| P1 | 50 | 68.8 | 75.2 | 66.3 | 68.3 | 65.7 | 59.1 | 67.5 | 75.4 | Y |
| P2 | 150 | 70.8 | 64.9 | 63.7 | 61.1 | 69.6 | 60.0 | 71.7 | 71.8 | Y |
| P3 | 120 | - | - | - | - | - | - | - | - | - |
| P4 | 145 | 74.9 | 73.0 | 95.6 | 94.5 | 105.8 | 64.3 | 51.1 | 68.7 | Y |
| P5 | 53 | 78.2 | 86.3 | 102.5 | 105.6 | 97.4 | 95.4 | 75.7 | 80.0 | Y |
| P6 | 52 | 21.7 | 20.0 | 19.5 | 19.6 | 22.3 | 40.6 | 41.3 | 49.4 | Y |
| P8 | 90 | - | - | - | - | - | - | - | - | - |
| Group | Injury Level | AIS Grade | Upper Motor Max = 50 | Lower Motor Max = 50 | |||||
|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Diff | Pre | Post | Diff | ||||
| P1 | S | T3 | A | 50 | 50 | 0 | 0 | 1 | +1 |
| P2 | S | T5 | A | 50 | 50 | 0 | 0 | 0 | 0 |
| P3 | NS | T6 | A | 50 | 50 | 0 | 0 | 0 | 0 |
| P4 | S | T5 | C | 50 | 50 | 0 | 1 | 6 | +5 |
| P5 | S | C6/7 | D | 49 | 49 | 0 | 24 | 31 | +7 |
| P6 | S | T10 | A | 50 | 50 | 0 | 1 | 1 | 0 |
| P8 | NS | C5 | C | 20 | 19 | −1 | 0 | 0 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al’joboori, Y.; Massey, S.J.; Knight, S.L.; Donaldson, N.d.N.; Duffell, L.D. The Effects of Adding Transcutaneous Spinal Cord Stimulation (tSCS) to Sit-To-Stand Training in People with Spinal Cord Injury: A Pilot Study. J. Clin. Med. 2020, 9, 2765. https://doi.org/10.3390/jcm9092765
Al’joboori Y, Massey SJ, Knight SL, Donaldson NdN, Duffell LD. The Effects of Adding Transcutaneous Spinal Cord Stimulation (tSCS) to Sit-To-Stand Training in People with Spinal Cord Injury: A Pilot Study. Journal of Clinical Medicine. 2020; 9(9):2765. https://doi.org/10.3390/jcm9092765
Chicago/Turabian StyleAl’joboori, Yazi, Sarah J. Massey, Sarah L. Knight, Nick de N. Donaldson, and Lynsey D. Duffell. 2020. "The Effects of Adding Transcutaneous Spinal Cord Stimulation (tSCS) to Sit-To-Stand Training in People with Spinal Cord Injury: A Pilot Study" Journal of Clinical Medicine 9, no. 9: 2765. https://doi.org/10.3390/jcm9092765
APA StyleAl’joboori, Y., Massey, S. J., Knight, S. L., Donaldson, N. d. N., & Duffell, L. D. (2020). The Effects of Adding Transcutaneous Spinal Cord Stimulation (tSCS) to Sit-To-Stand Training in People with Spinal Cord Injury: A Pilot Study. Journal of Clinical Medicine, 9(9), 2765. https://doi.org/10.3390/jcm9092765