Correlation between Three-Dimensional Volume and Malignant Potential of Gastrointestinal Stromal Tumors (GISTs)

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Source
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Patients with GISTs
3.2. Clinical Characteristics of Patients with Recurrent GISTs
3.3. Multivariate Analysis of the Malignant Potential of GISTs
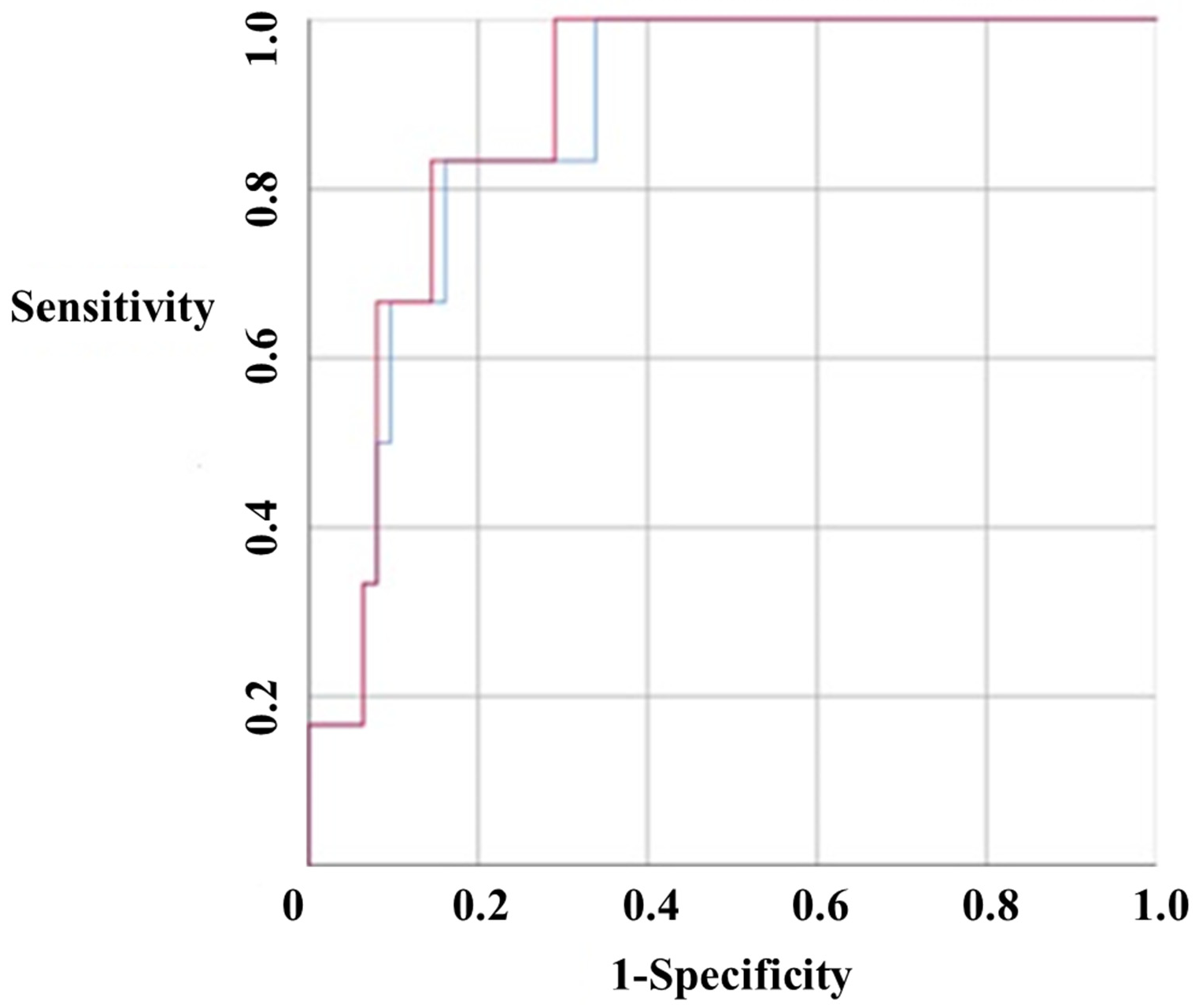
3.4. Receiver Operating Characteristic (ROC) Curve of the Malignant Potential of GISTs
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Patil, D.T.; Rubin, B.P. Gastrointestinal stromal tumor: Advances in diagnosis and management. Arch. Pathol. Lab. Med. 2011, 135, 1298–1310. [Google Scholar] [CrossRef] [Green Version]
- Jumniensuk, C.; Charoenpitakchai, M. Gastrointestinal stromal tumor: Clinicopathological characteristics and pathologic prognostic analysis. World J. Surg. Oncol. 2018, 16, 231. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.D.; Berman, J.J.; Corless, C.; Gorstein, F.; Lasota, J.; Longley, B.J.; Miettinen, M.; O′Leary, T.J.; Remotti, H.; Rubin, B.P.; et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum. Pathol. 2002, 33, 459–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joensuu, H. Risk stratification of patients diagnosed with gastrointestinal stromal tumor. Hum. Pathol. 2008, 39, 1411–1419. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Qiu, H.; Zhang, P.; Feng, X.; Chen, T.; Li, Y.; Tao, K.; Li, G.; Sun, X.; Zhou, Z. Prognostic role of tumor necrosis in patients undergoing curative resection for gastric gastrointestinal stromal tumor: A multicenter analysis of 740 cases in China. Cancer Med. 2017, 6, 2796–2803. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Xia, L.; Zhou, Y.; Wu, X.; Zhuang, W.; Chen, Y.; Zhao, R.; Wan, Q.; Du, L.; Zhou, Y. Prognostic value of tumor necrosis in gastrointestinal stromal tumor: A meta-analysis. Medicine (Baltimore) 2019, 98, e15338. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.M.; Chen, H.C.; Leung, T.K.; Chen, Y.Y. Gastrointestinal stromal tumor: Computed tomographic features. World J. Gastroenterol. 2004, 10, 2417–2418. [Google Scholar] [CrossRef] [PubMed]
- Poveda, A.; Garcia Del Muro, X.; Lopez-Guerrero, J.A.; Cubedo, R.; Martinez, V.; Romero, I.; Serrano, C.; Valverde, C.; Martin-Broto, J. GEIS guidelines for gastrointestinal sarcomas (GIST). Cancer Treat. Rev. 2017, 55, 107–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lino-Silva, L.S.; Segales-Rojas, P.; Aguilar-Cruz, E.; Salcedo-Hernandez, R.A.; Zepeda-Najar, C. Gastrointestinal Stromal Tumors Risk of Recurrence Stratification by Tumor Volume is a Best Predictor Compared with Risk Based on Mitosis and Tumor Size. J. Gastrointest. Cancer 2018. [Google Scholar] [CrossRef] [PubMed]
- Tirumani, S.H.; Shinagare, A.B.; O′Neill, A.C.; Nishino, M.; Rosenthal, M.H.; Ramaiya, N.H. Accuracy and feasibility of estimated tumour volumetry in primary gastric gastrointestinal stromal tumours: Validation using semiautomated technique in 127 patients. Eur. Radiol. 2016, 26, 286–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schramm, N.; Englhart, E.; Schlemmer, M.; Hittinger, M.; Ubleis, C.; Becker, C.R.; Reiser, M.F.; Berger, F. Tumor response and clinical outcome in metastatic gastrointestinal stromal tumors under sunitinib therapy: Comparison of RECIST, Choi and volumetric criteria. Eur. J. Radiol. 2013, 82, 951–958. [Google Scholar] [CrossRef] [PubMed]
- Yankelevitz, D.F.; Reeves, A.P.; Kostis, W.J.; Zhao, B.; Henschke, C.I. Small pulmonary nodules: Volumetrically determined growth rates based on CT evaluation. Radiology 2000, 217, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Dematteo, R.P.; Gold, J.S.; Saran, L.; Gonen, M.; Liau, K.H.; Maki, R.G.; Singer, S.; Besmer, P.; Brennan, M.F.; Antonescu, C.R. Tumor mitotic rate, size, and location independently predict recurrence after resection of primary gastrointestinal stromal tumor (GIST). Cancer 2008, 112, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Schiavon, G.; Ruggiero, A.; Schoffski, P.; van der Holt, B.; Bekers, D.J.; Eechoute, K.; Vandecaveye, V.; Krestin, G.P.; Verweij, J.; Sleijfer, S.; et al. Tumor volume as an alternative response measurement for imatinib treated GIST patients. PLoS ONE 2012, 7, e48372. [Google Scholar]


{kind=link}
| Benign GIST (n = 64) | Malignant GIST (n = 6) | p | |
|---|---|---|---|
| Age | 57.77 ± 11.79 | 60.83 ± 20.57 | 0.032 |
| Sex | |||
| Men | 30 (46.9%) | 4 (66.7%) | 0.354 |
| Women | 34 (53.1%) | 2 (33.3%) | |
| Location | |||
| Stomach | 51 (80.0%) | 2 (33.3%) | 0.011 |
| Non-stomach | 13 (20.0%) | 4 (66.7%) | |
| Mitoses | |||
| Less than 5 | 52 (81.3%) | 4 (66.7%) | 0.393 |
| 5 or more | 12 (18.7%) | 2 (33.3%) | |
| Long axis (mm) | 35.40 ± 22.38 | 73.33 ± 38.04 | 0.073 |
| Volume (cm3) | 53.07 ± 142.84 | 270.67 ± 410.80 | 0.001 |
| Necrosis | 9 (14.1%) | 4 (66.7%) | 0.001 |
| No Recurrence (n = 44) | Recurrence (n = 4) | p | |
|---|---|---|---|
| Age | 58.41 ± 10.81 | 61.00 ± 19.65 | 0.045 |
| Sex | |||
| Men | 20 (45.5%) | 3 (75.0%) | 0.257 |
| Women | 24 (54.5%) | 1 (25.0%) | |
| Follow-up period (year) | 3.84 ± 2.73 | 3.75 ± 1.26 | 0.950 |
| Location | |||
| Stomach | 36 (81.8%) | 0 (0.0%) | 0.000 |
| Non-stomach | 8 (18.2%) | 4 (100.0%) | |
| Mitoses | |||
| Less than 5 | 33 (75.0%) | 3 (75.0%) | 1.000 |
| 5 or more | 11 (25.0%) | 1 (25.0%) | |
| Long axis (mm) | 33.67 ± 25.08 | 72.49 ± 22.01 | 0.005 |
| Volume (cm3) | 56.25 ± 188.37 | 240.96 ± 242.38 | 0.072 |
| Variable | Odd Ratio (95% CI) | p |
|---|---|---|
| Age | 1.020 (0.953–1.092) | 0.567 |
| Location | ||
| Stomach | Reference | 0.025 |
| Non-stomach | 7.846 (1.293–47.624) | |
| Long axis | 1.037 (1.011–1.065) | 0.006 |
| Volume | 1.003 (1.000–1.006) | 0.029 |
| Long axis | ||
| Less than 5cm | Reference | 0.009 |
| Above 5cm | 11.778 (1.873–74.05) | |
| Necrosis | 12.222 (1.945–76.794) | 0.008 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.H.; Kang, B.-k.; Lee, H.L.; Yoon, J.H.; Lee, K.N.; Jun, D.W.; Lee, O.Y.; Han, D.S.; Yoon, B.C.; Choi, H.S. Correlation between Three-Dimensional Volume and Malignant Potential of Gastrointestinal Stromal Tumors (GISTs). J. Clin. Med. 2020, 9, 2763. https://doi.org/10.3390/jcm9092763
Park JH, Kang B-k, Lee HL, Yoon JH, Lee KN, Jun DW, Lee OY, Han DS, Yoon BC, Choi HS. Correlation between Three-Dimensional Volume and Malignant Potential of Gastrointestinal Stromal Tumors (GISTs). Journal of Clinical Medicine. 2020; 9(9):2763. https://doi.org/10.3390/jcm9092763
Chicago/Turabian StylePark, Jin Hwa, Bo-kyeong Kang, Hang Lak Lee, Jai Hoon Yoon, Kang Nyeong Lee, Dae Won Jun, Oh Young Lee, Dong Soo Han, Byung Chul Yoon, and Ho Soon Choi. 2020. "Correlation between Three-Dimensional Volume and Malignant Potential of Gastrointestinal Stromal Tumors (GISTs)" Journal of Clinical Medicine 9, no. 9: 2763. https://doi.org/10.3390/jcm9092763
APA StylePark, J. H., Kang, B.-k., Lee, H. L., Yoon, J. H., Lee, K. N., Jun, D. W., Lee, O. Y., Han, D. S., Yoon, B. C., & Choi, H. S. (2020). Correlation between Three-Dimensional Volume and Malignant Potential of Gastrointestinal Stromal Tumors (GISTs). Journal of Clinical Medicine, 9(9), 2763. https://doi.org/10.3390/jcm9092763