Comparative Analysis of Blood and Bone Marrow for the Detection of Circulating and Disseminated Tumor Cells and Their Prognostic and Predictive Value in Esophageal Cancer Patients

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Patient Cohort
2.2. Liquid Biopsy Collection
2.3. Nested RT-PCR and Analysis
2.4. Statistical Analysis
3. Results
3.1. Characterization of the Analyzed Patient Cohort
3.2. Detection Rates of CK20 mRNA by RT-PCR
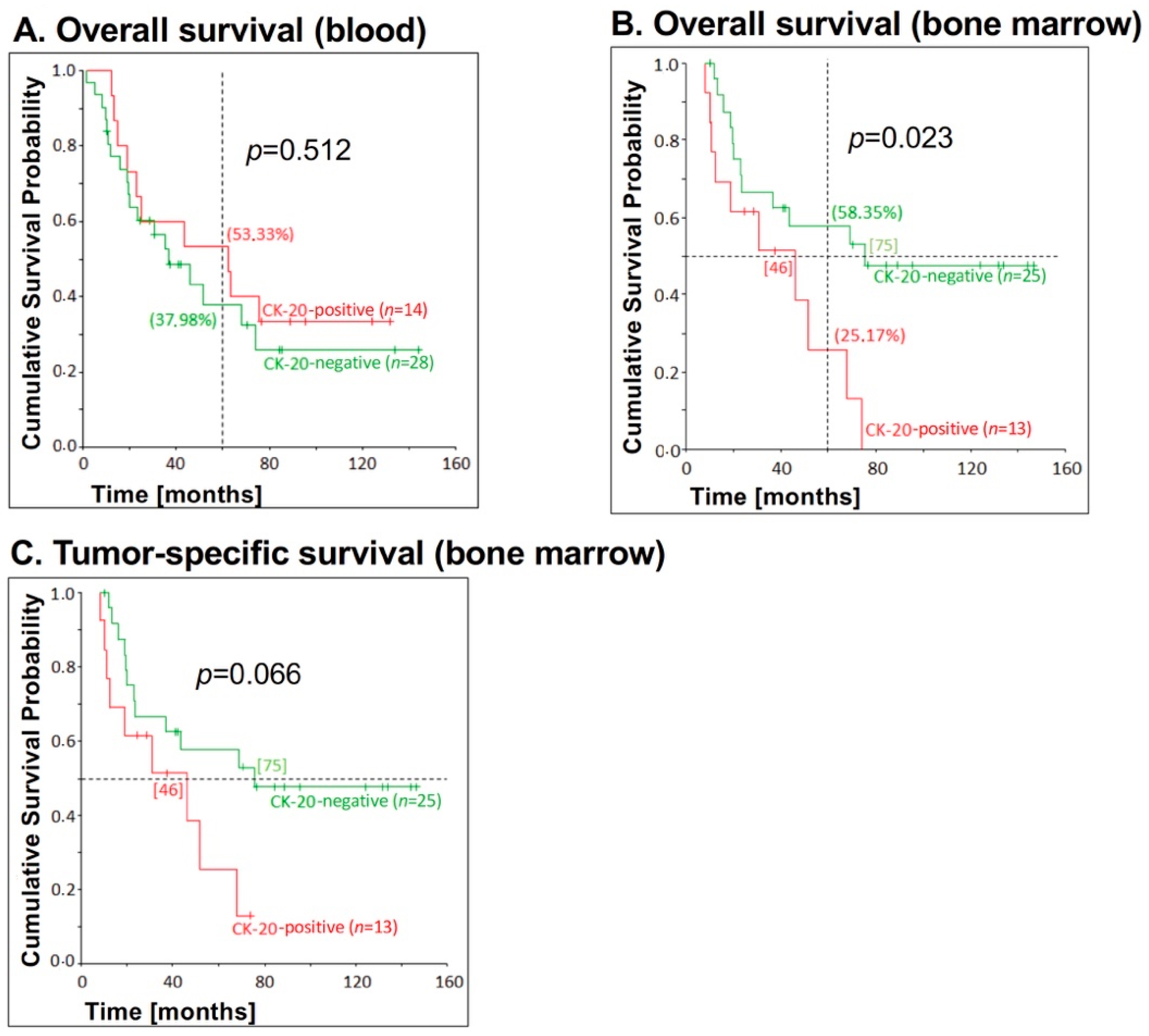
3.3. Correlation of CK20 mRNA Detection Levels in Blood and Bone Marrow and Patient’s Survival
3.4. Correlation between CK20 mRNA Detection in Blood and Bone Marrow and Survival of EC Patients in Dependence on UICC Stage
3.5. Correlation between CK20 mRNA Detection in Blood and Bone Marrow and Survival in EC Patients without Neo-Adjuvant Chemotherapy
3.6. Detection Rates of CK20 mRNA in Liquid Biopsies of EC Patients Associated with Clinical Parameters
3.7. Results of the Multivariate Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Pennathur, A.; Gibson, M.K.; Jobe, B.A.; Luketich, J.D. Oesophageal carcinoma. Lancet 2013, 381, 400–412. [Google Scholar] [CrossRef]
- Gupta, B.; Kumar, N. Worldwide incidence, mortality and time trends for cancer of the oesophagus. Eur. J. Cancer Prev. 2017, 26, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Kaatsch, P. Krebs in Deutschland für 2013/2014, 11th ed.; Robert-Koch-Institut and The Society of the Epidemiological Cancer Registries in Germany: Berlin, Germany, 2017. [Google Scholar]
- Kamangar, F.; Dores, G.M.; Anderson, W.F. Patterns of cancer incidence, mortality, and prevalence across five continents: Defining priorities to reduce cancer disparities in different geographic regions of the world. J. Clin. Oncol. 2006, 24, 2137–2150. [Google Scholar] [CrossRef] [PubMed]
- Pech, O.; May, A.; Gunter, E.; Gossner, L.; Ell, C. The impact of endoscopic ultrasound and computed tomography on the TNM staging of early cancer in Barrett’s esophagus. Am. J. Gastroenterol. 2006, 101, 2223–2229. [Google Scholar] [CrossRef] [PubMed]
- Vilgrain, V.; Mompoint, D.; Palazzo, L.; Menu, Y.; Gayet, B.; Ollier, P.; Nahum, H.; Fekete, F. Staging of esophageal carcinoma: Comparison of results with endoscopic sonography and CT. Am. J. Roentgenol. 1990, 155, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Omloo, J.M.; Lagarde, S.M.; Hulscher, J.B.; Reitsma, J.B.; Fockens, P.; van Dekken, H.; Ten Kate, F.J.; Obertop, H.; Tilanus, H.W.; van Lanschot, J.J. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the mid/distal esophagus: Five-year survival of a randomized clinical trial. Ann. Surg. 2007, 246, 992–1000. [Google Scholar] [CrossRef] [PubMed]
- Burmeister, B.H.; Smithers, B.M.; Gebski, V.; Fitzgerald, L.; Simes, R.J.; Devitt, P.; Ackland, S.; Gotley, D.C.; Joseph, D.; Millar, J.; et al. Surgery alone versus chemoradiotherapy followed by surgery for resectable cancer of the oesophagus: A randomised controlled phase III trial. Lancet Oncol. 2005, 6, 659–668. [Google Scholar] [CrossRef]
- Haverkamp, L.; Seesing, M.F.; Ruurda, J.P.; Boone, J.; Van Hillegersberg, R. Worldwide trends in surgical techniques in the treatment of esophageal and gastroesophageal junction cancer. Dis. Esophagus 2017, 30, 1–7. [Google Scholar] [CrossRef]
- Hulscher, J.B.; van Sandick, J.W.; de Boer, A.G.; Wijnhoven, B.P.; Tijssen, J.G.; Fockens, P.; Stalmeier, P.F.; ten Kate, F.J.; van Dekken, H.; Obertop, H.; et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N. Engl. J. Med. 2002, 347, 1662–1669. [Google Scholar] [CrossRef]
- Mariette, C.; Balon, J.M.; Piessen, G.; Fabre, S.; Van Seuningen, I.; Triboulet, J.P. Pattern of recurrence following complete resection of esophageal carcinoma and factors predictive of recurrent disease. Cancer 2003, 97, 1616–1623. [Google Scholar] [CrossRef]
- Izbicki, J.R.; Hosch, S.B.; Pichlmeier, U.; Rehders, A.; Busch, C.; Niendorf, A.; Passlick, B.; Broelsch, C.E.; Pantel, K. Prognostic value of immunohistochemically identifiable tumor cells in lymph nodes of patients with completely resected esophageal cancer. N. Engl. J. Med. 1997, 337, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Vashist, Y.K.; Effenberger, K.E.; Vettorazzi, E.; Riethdorf, S.; Yekebas, E.F.; Izbicki, J.R.; Pantel, K. Disseminated tumor cells in bone marrow and the natural course of resected esophageal cancer. Ann. Surg. 2012, 255, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Kalluri, R.; Weinberg, R.A. The basics of epithelial-mesenchymal transition. J. Clin. Investig. 2009, 119, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Shinde, A.; Hardy, S.D.; Kim, D.; Akhand, S.S.; Jolly, M.K.; Wang, W.H.; Anderson, J.C.; Khodadadi, R.B.; Brown, W.S.; George, J.T.; et al. Spleen Tyrosine Kinase-Mediated Autophagy Is Required for Epithelial-Mesenchymal Plasticity and Metastasis in Breast Cancer. Cancer Res. 2019, 79, 1831–1843. [Google Scholar] [CrossRef] [PubMed]
- Shinde, A.; Paez, J.S.; Libring, S.; Hopkins, K.; Solorio, L.; Wendt, M.K. Transglutaminase-2 facilitates extracellular vesicle-mediated establishment of the metastatic niche. Oncogenesis 2020, 9, 16. [Google Scholar] [CrossRef]
- Hoeppner, J.; Kulemann, B. Circulating Tumor Cells in Esophageal Cancer. Oncol. Res. Treat. 2017, 40, 417–422. [Google Scholar] [CrossRef]
- Sun, Y.F.; Yang, X.R.; Zhou, J.; Qiu, S.J.; Fan, J.; Xu, Y. Circulating tumor cells: Advances in detection methods, biological issues, and clinical relevance. J. Cancer Res. Clin. Oncol. 2011, 137, 1151–1173. [Google Scholar] [CrossRef]
- Li, X.Y.; Dong, M.; Zang, X.Y.; Li, M.Y.; Zhou, J.Y.; Ma, J.J.; Wang, G.Y. The emerging role of circulating tumor cells in cancer management. Am. J. Transl. Res. 2020, 12, 332–342. [Google Scholar]
- Masuda, T.; Hayashi, N.; Iguchi, T.; Ito, S.; Eguchi, H.; Mimori, K. Clinical and biological significance of circulating tumor cells in cancer. Mol. Oncol. 2016, 10, 408–417. [Google Scholar] [CrossRef]
- Bardelli, A.; Pantel, K. Liquid Biopsies, What We Do Not Know (Yet). Cancer Cell 2017, 31, 172–179. [Google Scholar] [CrossRef]
- Alix-Panabieres, C.; Pantel, K. Circulating tumor cells: Liquid biopsy of cancer. Clin. Chem. 2013, 59, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Su, P.J.; Wu, M.H.; Wang, H.M.; Lee, C.L.; Huang, W.K.; Wu, C.E.; Chang, H.K.; Chao, Y.K.; Tseng, C.K.; Chiu, T.K.; et al. Circulating Tumour Cells as an Independent Prognostic Factor in Patients with Advanced Oesophageal Squamous Cell Carcinoma Undergoing Chemoradiotherapy. Sci. Rep. 2016, 6, 31423. [Google Scholar] [CrossRef]
- Zhao, Y.; Han, L.; Zhang, W.; Shan, L.; Wang, Y.; Song, P.; Peng, C.; Zhao, X. Preoperative chemotherapy compared with postoperative adjuvant chemotherapy for squamous cell carcinoma of the thoracic oesophagus with the detection of circulating tumour cells randomized controlled trial. Int. J. Surg. 2020, 73, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Pantel, K.; Alix-Panabieres, C. Bone marrow as a reservoir for disseminated tumor cells: A special source for liquid biopsy in cancer patients. Bonekey Rep. 2014, 3, 584. [Google Scholar] [CrossRef] [PubMed]
- Hinz, S.; Hendricks, A.; Wittig, A.; Schafmayer, C.; Tepel, J.; Kalthoff, H.; Becker, T.; Röder, C. Detection of circulating tumor cells with CK20 RT-PCR is an independent negative prognostic marker in colon cancer patients-a prospective study. BMC Cancer 2017, 17, 53. [Google Scholar] [CrossRef]
- Andergassen, U.; Kolbl, A.C.; Mahner, S.; Jeschke, U. Real-time RT-PCR systems for CTC detection from blood samples of breast cancer and gynaecological tumour patients (Review). Oncol. Rep. 2016, 35, 1905–1915. [Google Scholar] [CrossRef]
- Gorges, T.M.; Tinhofer, I.; Drosch, M.; Röse, L.; Zollner, T.M.; Krahn, T.; von Ahsen, O. Circulating tumour cells escape from EpCAM-based detection due to epithelial-to-mesenchymal transition. BMC Cancer 2012, 12, 178. [Google Scholar] [CrossRef]
- Jung, R.; Petersen, K.; Kruger, W.; Wolf, M.; Wagener, C.; Zander, A.; Neumaier, M. Detection of micrometastasis by cytokeratin 20 RT-PCR is limited due to stable background transcription in granulocytes. Br. J. Cancer 1999, 81, 870–873. [Google Scholar] [CrossRef]
- Brakenhoff, R.H.; Stroomer, J.G.; ten Brink, C.; de Bree, R.; Weima, S.M.; Snow, G.B.; van Dongen, G.A. Sensitive detection of squamous cells in bone marrow and blood of head and neck cancer patients by E48 reverse transcriptase-polymerase chain reaction. Clin. Cancer Res. 1999, 5, 725–732. [Google Scholar]
- Soeth, E.; Röder, C.; Juhl, H.; Krüger, U.; Kremer, B.; Kalthoff, H. The detection of disseminated tumor cells in bone marrow from colorectal-cancer patients by a cytokeratin-20-specific nested reverse-transcriptase-polymerase-chain reaction is related to the stage of disease. Int. J. Cancer 1996, 69, 278–282. [Google Scholar] [CrossRef]
- Soeth, E.; Vogel, I.; Röder, C.; Juhl, H.; Marxsen, J.; Krüger, U.; Henne-Bruns, D.; Kremer, B.; Kalthoff, H. Comparative analysis of bone marrow and venous blood isolates from gastrointestinal cancer patients for the detection of disseminated tumor cells using reverse transcription PCR. Cancer Res. 1997, 57, 3106–3110. [Google Scholar] [PubMed]
- Kutyavin, I.V.; Afonina, I.A.; Mills, A.; Gorn, V.V.; Lukhtanov, E.A.; Belousov, E.S.; Singer, M.J.; Walburger, D.K.; Lokhov, S.G.; Gall, A.A.; et al. 3′-minor groove binder-DNA probes increase sequence specificity at PCR extension temperatures. Nucleic Acids Res. 2000, 28, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Siewert, J.R.; Stein, H.J. Classification of adenocarcinoma of the oesophagogastric junction. Br. J. Surg. 1998, 85, 1457–1459. [Google Scholar] [CrossRef] [PubMed]
- Ponce, M.R.; Micol, J.L. PCR amplification of long DNA fragments. Nucleic Acids Res. 1992, 20, 623. [Google Scholar] [CrossRef]
- Hinz, S.; Bockhorst, J.; Röder, C.; Egberts, J.H.; Schafmayer, C.; Küchler, T.; Becker, T.; Kalthoff, H. Disseminated tumor cells in the bone marrow negatively influence survival after resection of colorectal liver metastases. Ann. Surg. Oncol. 2012, 19, 2539–2546. [Google Scholar] [CrossRef]
- Hinz, S.; Röder, C.; Tepel, J.; Hendricks, A.; Schafmayer, C.; Becker, T.; Kalthoff, H. Cytokeratin 20 positive circulating tumor cells are a marker for response after neoadjuvant chemoradiation but not for prognosis in patients with rectal cancer. BMC Cancer 2015, 15, 953. [Google Scholar] [CrossRef]
- Konczalla, L.; Ghadban, T.; Effenberger, K.E.; Wöstemeier, A.; Riethdorf, S.; Uzunoglu, F.G.; Izbicki, J.R.; Pantel, K.; Bockhorn, M.; Reeh, M. Prospective Comparison of the Prognostic Relevance of Circulating Tumor Cells in Blood and Disseminated Tumor Cells in Bone Marrow of a Single Patient’s Cohort With Esophageal Cancer. Ann. Surg. 2019, in press. [Google Scholar] [CrossRef]
- Li, H.; Song, P.; Zou, B.; Liu, M.; Cui, K.; Zhou, P.; Li, S.; Zhang, B. Circulating Tumor Cell Analyses in Patients With Esophageal Squamous Cell Carcinoma Using Epithelial Marker-Dependent and -Independent Approaches. Medicine 2015, 94, e1565. [Google Scholar] [CrossRef]
- Reeh, M.; Effenberger, K.E.; Koenig, A.M.; Riethdorf, S.; Eichstadt, D.; Vettorazzi, E.; Uzunoglu, F.G.; Vashist, Y.K.; Izbicki, J.R.; Pantel, K.; et al. Circulating Tumor Cells as a Biomarker for Preoperative Prognostic Staging in Patients With Esophageal Cancer. Ann. Surg. 2015, 261, 1124–1130. [Google Scholar] [CrossRef]
- Woestemeier, A.; Harms-Effenberger, K.; Karstens, K.F.; Konczalla, L.; Ghadban, T.; Uzunoglu, F.G.; Izbicki, J.R.; Bockhorn, M.; Pantel, K.; Reeh, M. Clinical Relevance of Circulating Tumor Cells in Esophageal Cancer Detected by a Combined MACS Enrichment Method. Cancers 2020, 12, 718. [Google Scholar] [CrossRef]
- Gradilone, A.; Iacovelli, R.; Cortesi, E.; Raimondi, C.; Gianni, W.; Nicolazzo, C.; Petracca, A.; Palazzo, A.; Longo, F.; Frati, L.; et al. Circulating tumor cells and “suspicious objects” evaluated through CellSearch® in metastatic renal cell carcinoma. Anticancer Res. 2011, 31, 4219–4221. [Google Scholar] [PubMed]
- Raimondi, C.; Gradilone, A.; Naso, G.; Vincenzi, B.; Petracca, A.; Nicolazzo, C.; Palazzo, A.; Saltarelli, R.; Spremberg, F.; Cortesi, E.; et al. Epithelial-mesenchymal transition and stemness features in circulating tumor cells from breast cancer patients. Breast Cancer Res. Treat. 2011, 130, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, C.; Gradilone, A.; Naso, G.; Cortesi, E.; Gazzaniga, P. Clinical utility of circulating tumor cell counting through CellSearch®: The dilemma of a concept suspended in Limbo. Onco Targets Ther. 2014, 7, 619–625. [Google Scholar] [CrossRef]
- Marth, C.; Kisic, J.; Kaern, J.; Trope, C.; Fodstad, O. Circulating tumor cells in the peripheral blood and bone marrow of patients with ovarian carcinoma do not predict prognosis. Cancer 2002, 94, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Kaganoi, J.; Shimada, Y.; Kano, M.; Okumura, T.; Watanabe, G.; Imamura, M. Detection of circulating oesophageal squamous cancer cells in peripheral blood and its impact on prognosis. Br. J. Surg. 2004, 91, 1055–1060. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, S.; Natsugoe, S.; Matsumoto, M.; Miyazono, F.; Nakajo, A.; Uchikura, K.; Tokuda, K.; Ishigami, S.; Baba, M.; Takao, S.; et al. Clinical significance of circulating tumor cells in blood by molecular detection and tumor markers in esophageal cancer. Surgery 2003, 133, 162–169. [Google Scholar] [CrossRef]
- Setoyama, T.; Natsugoe, S.; Okumura, H.; Matsumoto, M.; Uchikado, Y.; Ishigami, S.; Owaki, T.; Takao, S.; Aikou, T. Carcinoembryonic antigen messenger RNA expression in blood predicts recurrence in esophageal cancer. Clin. Cancer Res. 2006, 12, 5972–5977. [Google Scholar] [CrossRef]
- Wang, S.; Du, H.; Li, G. Significant prognostic value of circulating tumor cells in esophageal cancer patients: A meta-analysis. Oncotarget 2017, 8, 15815–15826. [Google Scholar] [CrossRef]
- Xu, H.T.; Miao, J.; Liu, J.W.; Zhang, L.G.; Zhang, Q.G. Prognostic value of circulating tumor cells in esophageal cancer. World J. Gastroenterol. 2017, 23, 1310–1318. [Google Scholar] [CrossRef]
- Ryan, P.; McCarthy, S.; Kelly, J.; Collins, J.K.; Dunne, C.; Grogan, L.; Breathnach, O.; Shanahan, F.; Carey, P.D.; Walsh, T.N.; et al. Prevalence of bone marrow micrometastases in esophagogastric cancer patients with and without neoadjuvant chemoradiotherapy. J. Surg. Res. 2004, 117, 121–126. [Google Scholar] [CrossRef]
- Noguchi, T.; Shibata, T.; Fumoto, S.; Sato, T.; Uchida, Y.; Daa, T.; Yokoyama, S.; Gabbert, H.E.; Mueller, W.; Takeno, S. Detection of disseminated cancer cells in rib marrow of patients with esophageal cancer. Oncol. Rep. 2003, 10, 623–627. [Google Scholar] [PubMed]
- Chen, S.B.; Su, X.D.; Ma, G.W.; Lin, P.; Wen, J.; Wang, F.X.; Zhang, H.; Fu, J.H.; Zhang, X. Prognostic value of bone marrow micrometastasis in patients with operable esophageal squamous cell carcinoma: A long-term follow-up study. J. Thorac. Oncol. 2014, 9, 1207–1213. [Google Scholar] [CrossRef] [PubMed][Green Version]
- D′Oronzo, S.; Brown, J.; Coleman, R. The role of biomarkers in the management of bone-homing malignancies. J. Bone Oncol. 2017, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.; Furlong, H.; Murphy, C.G.; O’Sullivan, F.; Walsh, T.N.; Shanahan, F.; O’Sullivan, G.C. Prognostic significance of prospectively detected bone marrow micrometastases in esophagogastric cancer: 10-year follow-up confirms prognostic significance. Cancer Med. 2015, 4, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Steinert, G.; Scholch, S.; Koch, M.; Weitz, J. Biology and significance of circulating and disseminated tumour cells in colorectal cancer. Langenbecks Arch. Surg. 2012, 397, 535–542. [Google Scholar] [CrossRef]
- Bidard, F.C.; Vincent-Salomon, A.; Sigal-Zafrani, B.; Dieras, V.; Mathiot, C.; Mignot, L.; Thiery, J.P.; Sastre-Garau, X.; Pierga, J.Y. Prognosis of women with stage IV breast cancer depends on detection of circulating tumor cells rather than disseminated tumor cells. Ann. Oncol. 2008, 19, 496–500. [Google Scholar] [CrossRef]
- Zhang, J.Q.; Hooker, C.M.; Brock, M.V.; Shin, J.; Lee, S.; How, R.; Franco, N.; Prevas, H.; Hulbert, A.; Yang, S.C. Neoadjuvant chemoradiation therapy is beneficial for clinical stage T2 N0 esophageal cancer patients due to inaccurate preoperative staging. Ann. Thorac. Surg. 2012, 93, 429–435. [Google Scholar] [CrossRef]
- Stiles, B.M.; Mirza, F.; Coppolino, A.; Port, J.L.; Lee, P.C.; Paul, S.; Altorki, N.K. Clinical T2-T3N0M0 esophageal cancer: The risk of node positive disease. Ann. Thorac. Surg. 2011, 92, 491–496. [Google Scholar] [CrossRef]
- Van Hagen, P.; Hulshof, M.C.; van Lanschot, J.J.; Steyerberg, E.W.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; Richel, D.J.; Nieuwenhuijzen, G.A.; Hospers, G.A.; Bonenkamp, J.J.; et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N. Engl. J. Med. 2012, 366, 2074–2084. [Google Scholar] [CrossRef]
- Braun, S.; Kentenich, C.; Janni, W.; Hepp, F.; de Waal, J.; Willgeroth, F.; Sommer, H.; Pantel, K. Lack of effect of adjuvant chemotherapy on the elimination of single dormant tumor cells in bone marrow of high-risk breast cancer patients. J. Clin. Oncol. 2000, 18, 80–86. [Google Scholar] [CrossRef]
- Engel, H.; Kleespies, C.; Friedrich, J.; Breidenbach, M.; Kallenborn, A.; Schöndorf, T.; Kolhagen, H.; Mallmann, P. Detection of circulating tumour cells in patients with breast or ovarian cancer by molecular cytogenetics. Br. J. Cancer 1999, 81, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.; Ma, F.; Li, C.; Wu, S.; Hu, S.; Huang, J.; Sun, X.; Wang, J.; Luo, Y.; Cai, R.; et al. The prognostic and therapeutic implications of circulating tumor cell phenotype detection based on epithelial-mesenchymal transition markers in the first-line chemotherapy of HER2-negative metastatic breast cancer. Cancer Commun. 2019, 39, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Miyata, H.; Yamasaki, M.; Makino, T.; Tatsumi, M.; Miyazaki, Y.; Takahashi, T.; Kurokawa, Y.; Takiguchi, S.; Mori, M.; Doki, Y. Impact of number of [18F]fluorodeoxyglucose-PET-positive lymph nodes on survival of patients receiving neoadjuvant chemotherapy and surgery for oesophageal cancer. Br. J. Surg. 2016, 103, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Hardy, S.D.; Shinde, A.; Wang, W.H.; Wendt, M.K.; Geahlen, R.L. Regulation of epithelial-mesenchymal transition and metastasis by TGF-beta, P-bodies, and autophagy. Oncotarget 2017, 8, 103302–103314. [Google Scholar] [CrossRef]
- Shinde, A.; Libring, S.; Alpsoy, A.; Abdullah, A.; Schaber, J.A.; Solorio, L.; Wendt, M.K. Autocrine Fibronectin Inhibits Breast Cancer Metastasis. Mol. Cancer Res. 2018, 16, 1579–1589. [Google Scholar] [CrossRef]
- Sicklick, J.K.; Kato, S.; Okamura, R.; Schwaederle, M.; Hahn, M.E.; Williams, C.B.; De, P.; Krie, A.; Piccioni, D.E.; Miller, V.A.; et al. Molecular profiling of cancer patients enables personalized combination therapy: The I-PREDICT study. Nat. Med. 2019, 25, 744–750. [Google Scholar] [CrossRef]
- Janmaat, V.T.; Steyerberg, E.W.; van der Gaast, A.; Mathijssen, R.H.; Bruno, M.J.; Peppelenbosch, M.P.; Kuipers, E.J.; Spaander, M.C. Palliative chemotherapy and targeted therapies for esophageal and gastroesophageal junction cancer. Cochrane Database Syst. Rev. 2017, 11, CD004063. [Google Scholar] [CrossRef]
- Barsouk, A.; Rawla, P.; Hadjinicolaou, A.V.; Aluru, J.S.; Barsouk, A. Targeted Therapies and Immunotherapies in the Treatment of Esophageal Cancers. Med. Sci. 2019, 7, 100. [Google Scholar] [CrossRef]
- Fatehi Hassanabad, A.; Chehade, R.; Breadner, D.; Raphael, J. Esophageal carcinoma: Towards targeted therapies. Cell Oncol. 2020, 43, 195–209. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cycle | Denaturation | Primer Hybridization 1 | Elongation | Cycles |
|---|---|---|---|---|
| Touch-down-cycles | ||||
| 1 | 40 s/94 °C | 2 min/70 °C | 1 | |
| 2 | 40 s/94 °C | 1 min 55 s/69 °C | 1 | |
| 3 | 40 s/94 °C | 1 min 50 s/68 °C (66 °C) | 1 | |
| 4 | 40 s/94 °C | 1 min 45 s/67 °C (65 °C) | 1 | |
| 5 | 40 s/94 °C | 1 min 40 s/66 °C (64 °C) | 1 | |
| 6 | 40 s/94 °C | 1 min 35 s/65 °C (63 °C) | 1 | |
| 7 | 40 s/94 °C | 1 min 30 s/64 °C (62 °C) | 1 | |
| 8 | 40 s/94 °C | 1 min 25 s/63 °C (61 °C) | 1 | |
| 9 | 40 s/94 °C | 1 min 20 s/62 °C (60 °C) | 1 | |
| External and internal PCR | ||||
| 10–30 31 | 40 s/94 °C | 1 min/61 °C (59 °C) | 1 min 30 s/72 °C 15 min/72 °C | 21 1 |
| n (%) | |
|---|---|
| All Sex | 77 (100) |
| male | 64 (83.1) |
| female | 13 (16.9) |
| Tumor site | |
| Squamous cell carcinoma | 37 (48.1) |
| adenocarcinoma | 39 (50.6) |
| Neuroendocrine tumor | 1 (1.3) |
| Neo-adjuvant treatment | |
| yes | 32 (41.6) |
| no | 45 (58.4) |
| Adjuvant treatment | |
| yes | 2 (2.5) |
| no | 53 (68.8) |
| unknown | 22 (28.6) |
| Variable | Detection of CK20 mRNA in Blood (n = 74) | Correlation χ2-Test (p-Value) | |||
|---|---|---|---|---|---|
| Total | Positive (%) | Negative (%) | |||
| Gender | Female | 13 | 7 (53.85%) | 6 (46.15%) | 0.152 |
| Male | 61 | 20 (32.79%) | 41 (67.21%) | ||
| UICC-stage (n = 70) | I | 16 | 5 (31.25%) | 11 (68.75%) | 0.447 |
| II | 26 | 9 (34.62%) | 17 (65.38%) | ||
| III | 18 | 6 (33.33%) | 12 (66.67%) | ||
| IV | 10 | 6 (60%) | 4 (40%) | ||
| T-category (n = 71) | I | 18 | 5 (27.78%) | 13 (72.22%) | 0.439 |
| II | 22 | 7 (31.82%) | 15 (68.18%) | ||
| III | 30 | 14 (46.67%) | 16 (53.33%) | ||
| IV | 1 | 0 | 1 (100%) | ||
| N-category (n = 74) | 0 | 33 | 13 (39.39%) | 20 (60.61%) | 0.641 |
| I | 41 | 14 (34.15%) | 27 (65.85%) | ||
| M-category (n = 73) | 0 | 63 | 21 (33.33%) | 42 (66.67%) | 0.105 |
| I | 10 | 6 (60%) | 4 (40%) | ||
| Neo-adjuvant therapy | Yes | 31 | 12 (38.71%) | 19 (61.29%) | 0.736 |
| No | 43 | 15 (34.88%) | 28 (65.12%) | ||
| Relapse | Yes | 34 | 15 (44.12%) | 19 (55.88%) | 0.209 |
| No | 40 | 12 (30%) | 28 (70%) | ||
| Tumor type (histological) (n = 73) | Adenocarcinoma SCC | 38 | 10 (26.32%) | 28 (73.68%) | 0.084 |
| 35 | 16 (45.71%) | 19 (54.29%) | |||
| Variable | Detection of CK20 mRNA in Bone Marrow (n = 61) | Correlation χ2-Test (p-Value) | |||
|---|---|---|---|---|---|
| Total | Positive (%) | Negative (%) | |||
| Gender | Female | 9 | 2 (22.22%) | 7 (77.78%) | 0.53 |
| Male | 52 | 17 (32.69%) | 35 (67.31%) | ||
| UICC-stage (n = 70) | I | 12 | 3 (25%) | 9 (75%) | 0.49 |
| II | 24 | 10 (41.67%) | 14 (58.33%) | ||
| III | 15 | 3 (20%) | 12 (80%) | ||
| IV | 8 | 3 (37.5%) | 5 (62.5%) | ||
| T-category (n = 71) | I | 14 | 5 (35.71%) | 9 (64.29%) | 0.82 |
| II | 19 | 7 (36.84%) | 12 (63.16%) | ||
| III | 25 | 7 (28%) | 18 (72%) | ||
| IV | 1 | 0 | 1 (100%) | ||
| N-category (n = 61) | 0 | 27 | 8 (29.63%) | 19 (70.37%) | 0.82 |
| I | 34 | 11 (32.35%) | 23 (67.65%) | ||
| M-category (n = 73) | 0 | 53 | 16 (30.19%) | 37 (69.81%) | 0.68 |
| I | 8 | 3 (37.5%) | 5 (62.5%) | ||
| Neo-adjuvant therapy | Yes | 25 | 7 (28%) | 18 (72%) | 0.66 |
| No | 36 | 12 (33.33%) | 24 (66.67%) | ||
| Relapse | Yes | 28 | 8 (28.57%) | 20 (71.43%) | 0.69 |
| No | 33 | 11 (33.33%) | 22 (66.67%) | ||
| Tumor type (histological) (n = 73) | Adenocarcinoma SCC | 29 | 7 (24.14%) | 22 (75.86%) | 0.34 |
| 31 | 11 (35.48%) | 20 (64.52%) | |||
| Variable | Detection of CK20 mRNA in Blood and/or Bone Marrow (n = 77) | Correlation χ2-Test (p-Value) | |||
|---|---|---|---|---|---|
| Total | Positive (%) | Negative (%) | |||
| Gender | Female | 13 | 8 (61.54%) | 5 (38.46%) | 0.448 |
| Male | 64 | 32 (50%) | 32 (50%) | ||
| UICC-stage (n = 70) | I | 16 | 7 (43.75%) | 9 (56.25%) | 0.038 |
| II | 28 | 18 (64.29%) | 10 (35.71%) | ||
| III | 19 | 6 (31.58%) | 13 (68.52%) | ||
| IV | 10 | 8 (80%) | 2 (20%) | ||
| T-category (n = 71) | I | 18 | 9 (50%) | 9 (50%) | 0.598 |
| II | 23 | 14 (60.87%) | 9 (39.13%) | ||
| III | 32 | 16 (50%) | 16 (50%) | ||
| IV | 1 | 0 | 1 (100%) | ||
| N-category (n = 77) | 0 | 34 | 19 (55.88%) | 15 (44.12%) | 0.539 |
| I | 43 | 21 (48.84%) | 22 (51.16%) | ||
| M-category (n = 73) | 0 | 66 | 32 (48.48%) | 34 (51.52%) | 0.063 |
| I | 10 | 8 (80%) | 2 (20%) | ||
| Neo-adjuvant therapy | Yes | 32 | 17 (53.13%) | 15 (46.87%) | 0.862 |
| No | 45 | 23 (51.11%) | 22 (48.89%) | ||
| Relapse | Yes | 36 | 19 (52.78%) | 17 (47.22%) | 0.891 |
| No | 41 | 21 (51.22%) | 20 (48.78%) | ||
| Tumor type (histological) (n = 73) | Adenocarcinoma SCC | 39 | 16 (41%) | 23 (59%) | 0.065 |
| 37 | 23 (62.16%) | 14 (37.84%) | |||
| Variables | p-Value (Univariate) | p-Value (Multivariate) | Hazard Quotient |
|---|---|---|---|
| Overall survival | |||
| CK20 detection in BM | 0.029 | 0.006 | 2.529 |
| N-category | <0.001 | 0.357 | 1.53 |
| UICC stage-group | <0.001 | <0.001 | 3.128 |
| Tumor-specific survival | |||
| CK20 detection in BM | 0.048 | 0.013 | 2.37 |
| N-category | <0.001 | 0.548 | 1.31 |
| UICC stage-group | <0.001 | 0.002 | 2.873 |
| Relapse free survival | |||
| N-category | <0.001 | 0.258 | 1.646 |
| UICC stage-group | <0.001 | 0.001 | 2.913 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Richter, F.; Baratay, A.; Röder, C.; Egberts, J.-H.; Kalthoff, H.; Becker, T.; Sebens, S. Comparative Analysis of Blood and Bone Marrow for the Detection of Circulating and Disseminated Tumor Cells and Their Prognostic and Predictive Value in Esophageal Cancer Patients. J. Clin. Med. 2020, 9, 2674. https://doi.org/10.3390/jcm9082674
Richter F, Baratay A, Röder C, Egberts J-H, Kalthoff H, Becker T, Sebens S. Comparative Analysis of Blood and Bone Marrow for the Detection of Circulating and Disseminated Tumor Cells and Their Prognostic and Predictive Value in Esophageal Cancer Patients. Journal of Clinical Medicine. 2020; 9(8):2674. https://doi.org/10.3390/jcm9082674
Chicago/Turabian StyleRichter, Florian, Annette Baratay, Christian Röder, Jan-Hendrik Egberts, Holger Kalthoff, Thomas Becker, and Susanne Sebens. 2020. "Comparative Analysis of Blood and Bone Marrow for the Detection of Circulating and Disseminated Tumor Cells and Their Prognostic and Predictive Value in Esophageal Cancer Patients" Journal of Clinical Medicine 9, no. 8: 2674. https://doi.org/10.3390/jcm9082674
APA StyleRichter, F., Baratay, A., Röder, C., Egberts, J.-H., Kalthoff, H., Becker, T., & Sebens, S. (2020). Comparative Analysis of Blood and Bone Marrow for the Detection of Circulating and Disseminated Tumor Cells and Their Prognostic and Predictive Value in Esophageal Cancer Patients. Journal of Clinical Medicine, 9(8), 2674. https://doi.org/10.3390/jcm9082674