Mobile-Based Lifestyle Intervention in Women with Glucose Intolerance after Gestational Diabetes Mellitus (MELINDA), A Multicenter Randomized Controlled Trial: Methodology and Design

 ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Objectives of the Melinda Study
- To evaluate whether a telephone- and mobile-based lifestyle coaching program leads to a higher frequency of weight goal achievement (≥5% weight loss if pre-pregnancy Body Mass Index (BMI) ≥ 25 Kg/m2 or return to pre-gravid weight if BMI < 25 Kg/m2).
- To evaluate whether a telephone- and mobile-based lifestyle coaching intervention can reduce the incidence of metabolic syndrome, leading to an improved beta-cell function and lower insulin resistance in women with glucose intolerance after a recent history of GDM.
- To investigate the prevalence of glucose intolerance and T2DM after a recent diagnosis of GDM based on the 2013 World Health Organization (WHO) criteria and to evaluate the risk factors of developing glucose intolerance postpartum.
- To investigate factors related to success or failure in diabetes prevention and to develop materials and expertise to assist in the development of diabetes prevention programs in primary care.
3. Materials and Methods
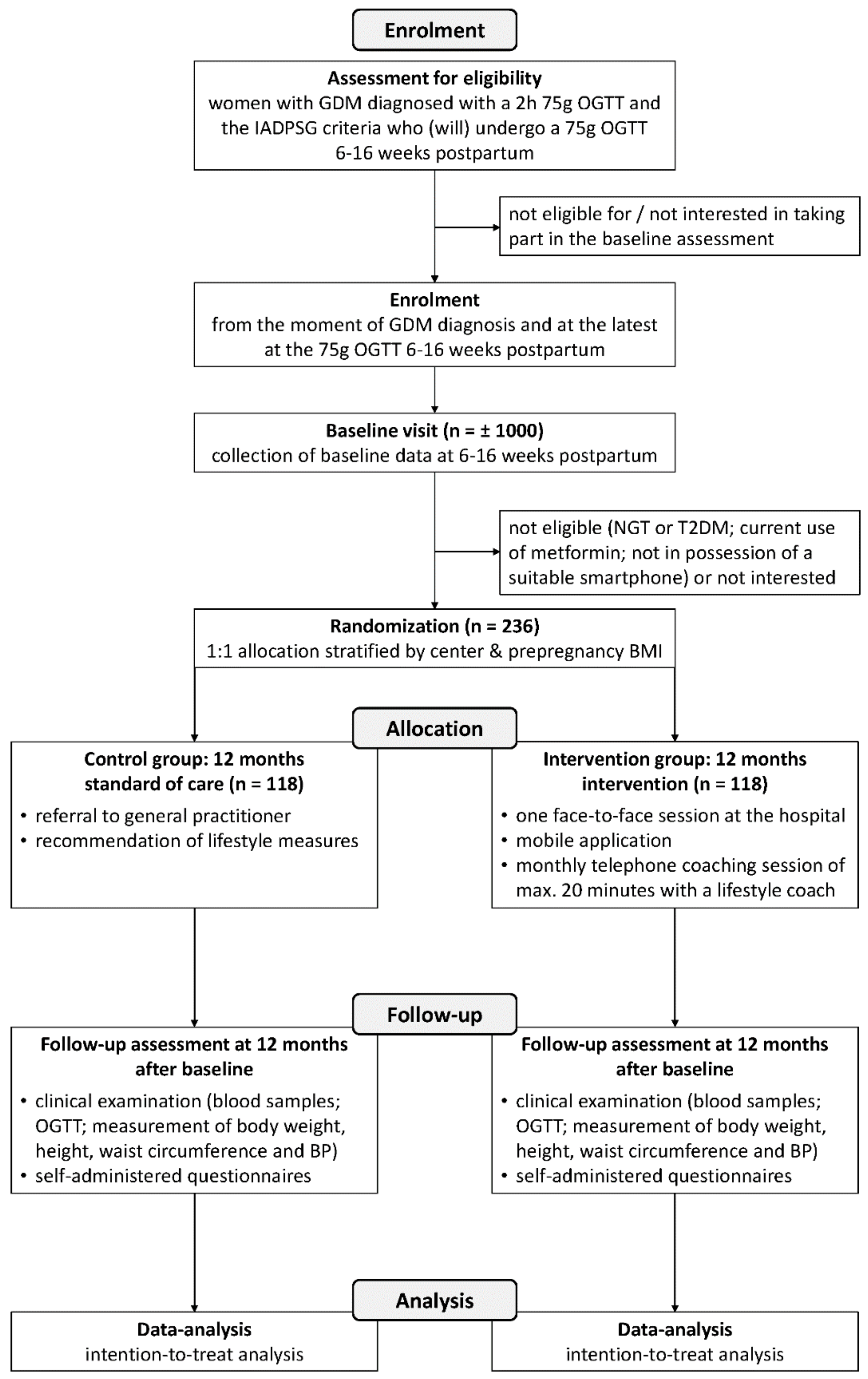
3.1. Study Design and Setting
3.2. Recruitment and Eligibility
- -
- current use of medication that can affect glucose values (such as glucocorticoids) or receiving treatment for glucose intolerance (such as metformin)
- -
- women who do not undergo the 75 g OGTT 6–16 weeks at the hospital
- -
- women who are not diagnosed with GDM based on the 2013 WHO criteria
- -
- insufficient Dutch, English or French language skills
- -
- diabetes (FPG ≥126 mg/dL and/or 2-h glucose value ≥ 200 mg/dL)
- -
- normal glucose tolerance
- -
- current use of metformin
- -
- health limitations or treatments (as assessed by the local investigator according to a standardized protocol) which would restrict participation in the intervention trial
- -
- not in possession of a suitable smartphone (iOS or Android)
3.3. Study Visits
3.3.1. Baseline Measurements during the 75 g OGTT 6–16 Weeks After Delivery
3.3.2. Enrolment in the Intervention RCT
3.3.3. Intervention Group
3.3.4. Control Group
3.4. Key Aspects of the Blended Lifestyle Intervention
3.5. Data Collection
3.5.1. Blood Collection
3.5.2. Clinical Examinations
3.5.3. Self-Administered Questionnaires
3.5.4. Melinda App
3.6. Outcomes of the Study
3.6.1. Primary Outcome
3.6.2. Secondary Outcomes
- -
- frequency of T2DM based on the ADA criteria after one year [37] and risk factors for the development of T2DM after one year
- -
- frequency of glucose intolerance and the risk factors of glucose intolerance in early postpartum
- -
- frequency of the metabolic syndrome based on the WHO criteria [38]
- -
- insulin resistance and beta-cell function. The insulin sensitivity will be measured using the Matsuda index and the reciprocal of the homeostasis model assessment of insulin resistance (1/HOMA-IR) [39,40]. Beta-cell function will be assessed by HOMA-B, the insulinogenic index divided by HOMA-IR, and by the insulin secretion sensitivity index [41,42]. All these measures have been validated for use in women with GDM [26].
- -
- mean weight loss
- -
- duration of breastfeeding and rate of exclusive breastfeeding
- -
- quality of life, symptoms of depression and anxiety
- -
- motivation for behavior change and perceived risk of developing diabetes
- -
- dietary quality
- -
- intensity and duration of physical activity
- -
- process outcome: the percentage of women adhering to the protocol of intervention, by monitoring the use of the MELINDA app and the number of telephone coaching sessions.
3.6.3. Pregnancy and Delivery Outcome Data (Collected from the Electronical Medical Record)
3.7. Power Calculation and Statistical Analysis
3.7.1. Sample Size
3.7.2. Data Analysis
3.8. Quality Control Procedures
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association. Standards of Medical Care in Diabetes-2017. Diabetes Care 2017, 40 (Suppl. 1), S11–S24. [Google Scholar]
- Crowther, C.A.; Hiller, J.E.; Moss, J.R.; Mcphee, A.J.; Jeffries, W.S.; Robinson, J.S. Effect of Treatment of Gestational Diabetes Mellitus on Pregnancy Outcomes. N. Engl. J. Med. 2005, 352, 2477–2486. [Google Scholar] [CrossRef] [PubMed]
- Landon, M.B.; Spong, C.Y.; Thom, E.; Carpenter, M.W.; Ramin, S.M.; Casey, B.; Wapner, R.J.; Varner, M.W.; Rouse, D.J.; Thorp, J.M., Jr.; et al. A multicenter, randomized trial of treatment for mild gestational diabetes. N. Engl. J. Med. 2009, 361, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, T.A. Pancreatic B-Cell Defects in Gestational Diabetes: Implications for the Pathogenesis and Prevention of Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2001, 86, 989–993. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, L.; Casas, J.-P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [Google Scholar] [CrossRef]
- Benhalima, K.; Lens, K.; Bosteels, J.; Chantal, M. The Risk for Glucose Intolerance after Gestational Diabetes Mellitus since the Introduction of the IADPSG Criteria: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1431. [Google Scholar] [CrossRef]
- Ratner, R.E.; Christophi, C.A.; Metzger, B.E.; Dabelea, D.; Bennett, P.H.; Pi-Sunyer, X.; Fowler, S.; Kahn, S.E. The Diabetes Prevention Program Research Group. Prevention of Diabetes in Women with a History of Gestational Diabetes: Effects of Metformin and Lifestyle Interventions. J. Clin. Endocrinol. Metab. 2008, 93, 4774–4779. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Santaguida, P.; Raina, P.; Morrison, K.M.; Balion, C.; Hunt, D.; Yazdi, H.; Booker, L. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: A systematic overview and meta-analysis of prospective studies. Diabetes Res. Clin. Pract. 2007, 78, 305–312. [Google Scholar] [CrossRef]
- Tuomilehto, J.; Lindstrom, J.; Eriksson, J.G.; Valle, T.T. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Aroda, V.R.; Christophi, C.A.; Edelstein, S.L.; Zhang, P.; Herman, W.H.; Barrett-Connor, E.; Delahanty, L.M.; Montez, M.G.; Ackermann, R.T.; Zhuo, X.; et al. The effect of lifestyle intervention and metformin on preventing or delaying diabetes among women with and without gestational diabetes: The Diabetes Prevention Program outcomes study 10-year follow-up. J. Clin. Endocrinol. Metab. 2015, 100, 1646–1653. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.W.; Smith, B.J.; Henriksen, H.; Tapsell, L.C.; McLean, M.; Bauman, A. A group-based healthy lifestyle program for women with previous gestational diabetes. Diabetes Res. Clin. Pract. 2007, 77, 333–334. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Draska, M.; Hess, M.L.; Wilson, E.J.; Richardson, C.R. A web-based pedometer programme in women with a recent history of gestational diabetes. Diabet. Med. 2012, 29, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, A.; Hedderson, M.; Albright, C.; Ehrlich, S.; Quesenberry, C.; Peng, T.; Feng, J.; Ching, J.; Crites, Y. A pregnancy and postpartum lifestyle intervention in women with gestational diabetes mellitus reduces diabetes risk factors: A feasibility randomized control trial. Diabetes Care 2011, 34, 1519–1525. [Google Scholar] [CrossRef]
- Goveia, P.; Cañon-Montañez, W.; De Paula Santos, D.; Lopes, G.W.; Ma, R.C.W.; Duncan, B.B.; Ziegelman, P.K.; Schmidt, M.I. Lifestyle intervention for the prevention of diabetes in women with previous gestational diabetes mellitus: A systematic review and meta-analysis. Front. Endocrinol. 2018, 9, 583. [Google Scholar] [CrossRef]
- Lim, S.; Dunbar, J.A.; Versace, V.L.; Janus, E.; Wildey, C.; Skinner, T.; O’Reilly, S. Comparing a telephone- and a group-delivered diabetes prevention program: Characteristics of engaged and non-engaged postpartum mothers with a history of gestational diabetes. Diabetes Res. Clin. Pract. 2017, 126, 254–262. [Google Scholar] [CrossRef]
- Lim, S.; Tan, A.; Madden, S.; Hill, B. Health professionals’ and postpartum women’s perspectives on digital health interventions for lifestyle management in the postpartum period: A systematic review of qualitative studies. Front. Endocrinol. 2019, 10, 767. [Google Scholar] [CrossRef]
- Nicklas, J.M.; Zera, C.A.; England, L.J.; Rosner, B.A.; Horton, E.; Levkoff, S.E.; Seely, E.W. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: A randomized controlled trial. Obs. Gynecol. 2014, 124, 563–570. [Google Scholar] [CrossRef]
- Appel, L.J.; Clark, J.M.; Yeh, H.-C.; Wang, N.-Y.; Coughlin, J.W.; Daumit, G.; Miller, E.R., III; Dalcin, A.; Jerome, G.J.; Geller, S.; et al. Comparative effectiveness of weight-loss interventions in clinical practice. N. Engl. J. Med. 2011, 365, 1959–1968. [Google Scholar] [CrossRef]
- Hurkmans, E.; Matthys, C.; Bogaerts, A.; Scheys, L.; Devloo, K.; Seghers, J. Face-to-Face Versus Mobile Versus Blended Weight Loss Program: Randomized Clinical Trial. JMIR mHealth uHealth 2018, 6, e14. [Google Scholar] [CrossRef]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Boedt, T.; Dancet, E.; Lie Fong, S.; Peeraer, K.; De Neubourg, D.; Pelckmans, S.; van de Vijver, A.; Seghers, J.; Van der Gucht, K.; Van Calster, B.; et al. Effectiveness of a mobile preconception lifestyle programme in couples undergoing in vitro fertilisation (IVF): The protocol for the PreLiFe randomised controlled trial (PreLiFe-RCT). BMJ Open 2019, 9, e029665. [Google Scholar] [CrossRef] [PubMed]
- Bogaerts, A.; Bijlholt, M.; Mertens, L.; Braeken, M.; Jacobs, B.; Vandenberghe, B.; Ameye, L.; Devlieger, R. Development and Field Evaluation of the INTER-ACT App, a Pregnancy and Interpregnancy Coaching App to Reduce Maternal Overweight and Obesity: Mixed Methods Design. JMIR Form. Res. 2020, 4, e16090. [Google Scholar] [CrossRef] [PubMed]
- Vidgen, H.A.; Gallegos, D. Defining food literacy and its components. Appetite 2014, 76, 50–59. [Google Scholar] [CrossRef]
- Benhalima, K.; Van Crombrugge, P.; Verhaeghe, J.; Vandeginste, S.; Verlaenen, H.; Vercammen, C.; Dufraimont, E.; De Block, C.; Jacquemyn, Y.; Mekahli, F.; et al. The Belgian Diabetes in Pregnancy Study (BEDIP-N), a multi-centric prospective cohort study on screening for diabetes in pregnancy and gestational diabetes: Methodology and design. BMC Pregnancy Childbirth 2014, 14, 226. [Google Scholar] [CrossRef] [PubMed]
- Matthys, C.; Meulemans, A. Development and validation of general FFQ for use in clinical practice. Nutr. Metab. 2015, 67, 239. [Google Scholar]
- Harrison, C.; Thompson, R.; Teede, H.; Lombard, C. Measuring physical activity during pregnancy. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 19. [Google Scholar] [CrossRef]
- Dalfrà, M.G.; Nicolucci, A.; Bisson, T.; Bonsembiante, B.; Lapolla, A. Quality of life in pregnancy and post-partum: A study in diabetic patients. Qual. Life Res. 2012, 21, 291–298. [Google Scholar] [CrossRef]
- Petrou, S.; Morrell, J.; Spiby, H. Assessing the empirical validity of alternative multi-attribute utility measures in the maternity context. Health Qual. Life Outcomes 2009, 7, 40–52. [Google Scholar] [CrossRef]
- Kim, C.; Mcewen, L.N.; Piette, J.D.; Goewey, J.; Ferrara, A.; Walker, E.A. Risk Perception for Diabetes among Women with Histories of Gestational Diabetes Mellitus. Diabetes Care 2007, 30, 2281–2286. [Google Scholar] [CrossRef]
- Shigaki, C.; Kruse, R.L.; Mehr, D.; Sheldon, K.M.; Bin, G.; Moore, C.; Lemaster, J. Motivation and diabetes self-management. Chronic Illn. 2010, 6, 202–214. [Google Scholar] [CrossRef] [PubMed]
- Levesque, C.S.; Williams, G.C.; Elliot, D.; Pickering, M.A.; Bodenhamer, B.; Finley, P.J. Validating the theoretical structure of the Treatment Self-Regulation Questionnaire (TSRQ) across three different health behaviors. Health Educ. Res. 2007, 22, 691–702. [Google Scholar] [CrossRef] [PubMed]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Van der Bij, A.K.; de Weerd, S.; Cikot, R.J.L.M.; Steegers, E.A.P.; Braspenning, J.C.C. Validation of the Dutch Short Form of the State Scale of the Spielberger State-Trait Anxiety Inventory: Considerations for Usage in Screening Outcomes. Community Genet. 2003, 6, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Lindström, B. Antonovsky’s sense of coherence scale and its relation with quality of life: A systematic review. J. Epidemiol. Community Health. 2007, 61, 938–944. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care 2016, 39, S13–S22. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B.; Cleeman, J.I.; Smith, S.C.; Lenfant, C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Kahn, S.E. The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of Type 2 diabetes. Diabetologia 2003, 46, 3–19. [Google Scholar] [CrossRef]
- Retnakaran, R.; Qi, Y.; Goran, M.I.; Hamilton, J.K. Evaluation of proposed oral disposition index measures in relation to the actual disposition index. Diabet. Med. 2009, 26, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Devlieger, H.; Martens, G.; Bekaert, A.; Eeckels, R. Standaarden van geboortegewicht-voor-zwangerschapsduur voor de vlaamse boreling. Tijdschr Geneeskd 2000, 56, 1–14. [Google Scholar] [CrossRef]
- Benhalima, K.; Jegers, K.; Devlieger, R.; Verhaeghe, J.; Mathieu, C. Glucose intolerance after a recent history of gestational diabetes based on the 2013 WHO criteria. PLoS ONE 2016, 10, e0157272. [Google Scholar] [CrossRef] [PubMed]
- Ciwit B.V. Castor Electronic Data Capture; Ciwit B.V.: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Saaristo, T.; Moilanen, L.; Korpi-Hyövälti, E.; Vanhala, M.; Saltevo, J.; Niskanen, L.; Jokelainen, J.; Peltonen, M.; Oksa, H.; Tuomilheto, J.; et al. Lifestyle intervention for prevention of type 2 diabetes in primary health care: One-year follow-up of the finnish national diabetes prevention program (FIN-D2D). Diabetes Care 2010, 33, 2146–2151. [Google Scholar] [CrossRef]


{kind=link}
| Outcomes | Assessments | Timing of Assessments | ||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | 1 Month * | Monthly * (Month 2 to 11) | 3 Months * | 6 Months * | 9 Months * | 12 Months ** | ||
| Outcomes Collected from Medical Records | ||||||||
| Demographic data | Age; date of birth | x | ||||||
| Medical and obstetric history | Pre-pregnancy weight and BMI; weight at delivery; parity; previous pregnancy outcomes | x | ||||||
| Patient-Reported Outcomes | ||||||||
| General lifestyle behaviour and socio-economic factors | Self-constructed questionnaire | x | ||||||
| Medication use | Questioned by study nurse | x | x | x | x | x | x | x |
| Diet | Food Frequency Questionnaire (FFQ) | x | x | x | x | x | ||
| Physical activity | International Physical Activity Questionnaire Long Form (IPAQ-LF) | x | x | |||||
| Mental health and well-being | Center for Epidemiologic Studies -Depression (CES-D) questionnaire and Spielberger State-Trait Anxiety Inventory (STAI-6) questionnaire | x | x | |||||
| Quality of life | 36-Item Short Form Health Survey (SF-36) | x | x | |||||
| Diabetes risk perception | Risk Perception Survey for Developing Diabetes (RPS-DD) | x | x | |||||
| Motivation for lifestyle change | Treatment Self-Regulation Questionnaire (TSRQ) | x (v2) | x (v3) | |||||
| Breastfeeding and anticonception | Self-constructed questionnaire | x | x | |||||
| Sense of coherence | Sense of Coherence (SOC) questionnaire | x | x | |||||
| Acceptability and subjective quality of the lifestyle intervention | Self-constructed questionnaire | x | ||||||
| Clinical and Biochemical Outcomes | ||||||||
| Anthropometry | Height (only baseline), weight, waist circumference, blood pressure, BMI | x | x | |||||
| Glucose and insulin | Fasting 75 g OGTT (0, 30, 60 and 120 min) | x | x | |||||
| HbA1c | Fasting | x | x | |||||
| Lipid profile | Total cholesterol, triglycerides, HDL, LDL (fasting) | x | x | |||||
| Outcomes Collected from the MELINDA App | ||||||||
| Weight | Self-reported weight in the MELINDA app | x | ||||||
| Motivational status | Self-reported motivational status in the MELINDA app | x | ||||||
| Waist circumference | Self-reported waist circumference in the MELINDA app | x | x | x | ||||
| Physical activity | Steps collected from pedometer connected to Melinda app | x | ||||||
| Use of the MELINDA app | App-based tracking to evaluate the use of the MELINDA app | x | x | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minschart, C.; Maes, T.; De Block, C.; Van Pottelbergh, I.; Myngheer, N.; Abrams, P.; Vinck, W.; Leuridan, L.; Mathieu, C.; Billen, J.; et al. Mobile-Based Lifestyle Intervention in Women with Glucose Intolerance after Gestational Diabetes Mellitus (MELINDA), A Multicenter Randomized Controlled Trial: Methodology and Design. J. Clin. Med. 2020, 9, 2635. https://doi.org/10.3390/jcm9082635
Minschart C, Maes T, De Block C, Van Pottelbergh I, Myngheer N, Abrams P, Vinck W, Leuridan L, Mathieu C, Billen J, et al. Mobile-Based Lifestyle Intervention in Women with Glucose Intolerance after Gestational Diabetes Mellitus (MELINDA), A Multicenter Randomized Controlled Trial: Methodology and Design. Journal of Clinical Medicine. 2020; 9(8):2635. https://doi.org/10.3390/jcm9082635
Chicago/Turabian StyleMinschart, Caro, Toon Maes, Christophe De Block, Inge Van Pottelbergh, Nele Myngheer, Pascale Abrams, Wouter Vinck, Liesbeth Leuridan, Chantal Mathieu, Jaak Billen, and et al. 2020. "Mobile-Based Lifestyle Intervention in Women with Glucose Intolerance after Gestational Diabetes Mellitus (MELINDA), A Multicenter Randomized Controlled Trial: Methodology and Design" Journal of Clinical Medicine 9, no. 8: 2635. https://doi.org/10.3390/jcm9082635
APA StyleMinschart, C., Maes, T., De Block, C., Van Pottelbergh, I., Myngheer, N., Abrams, P., Vinck, W., Leuridan, L., Mathieu, C., Billen, J., Matthys, C., Weyn, B., Laenen, A., Bogaerts, A., & Benhalima, K. (2020). Mobile-Based Lifestyle Intervention in Women with Glucose Intolerance after Gestational Diabetes Mellitus (MELINDA), A Multicenter Randomized Controlled Trial: Methodology and Design. Journal of Clinical Medicine, 9(8), 2635. https://doi.org/10.3390/jcm9082635