Prevention of Venous Thromboembolism in 2020 and Beyond


Abstract
1. Introduction
1.1. Venous Thromboembolism Remains a Significant Public Health Concern
1.2. Venous Thromboembolism Exists in a Hierarchy of Clinical Importance
1.3. An Ounce of Prevention is Worth a Pound of Cure
1.4. Approaches to Prevent Venous Thromboembolism
1.5. Age Is One of The Most Important Risk Factors
1.6. Genetic Risk Factors
2. Prevention: Acquired Risk
2.1. Exogenous Hormonal Therapies
2.2. Pregnancy
2.3. Surgery
2.4. Medical Hospitalization
2.5. COVID-19 Infection
2.6. Cancer-Associated Thrombosis
3. Future Directions for Prevention of Venous Thromboembolism
3.1. A More Palatable Approach to Pharmacologic Prevention
3.2. Bleeding Complications Limit the Net Benefits of Thromboprophylaxis
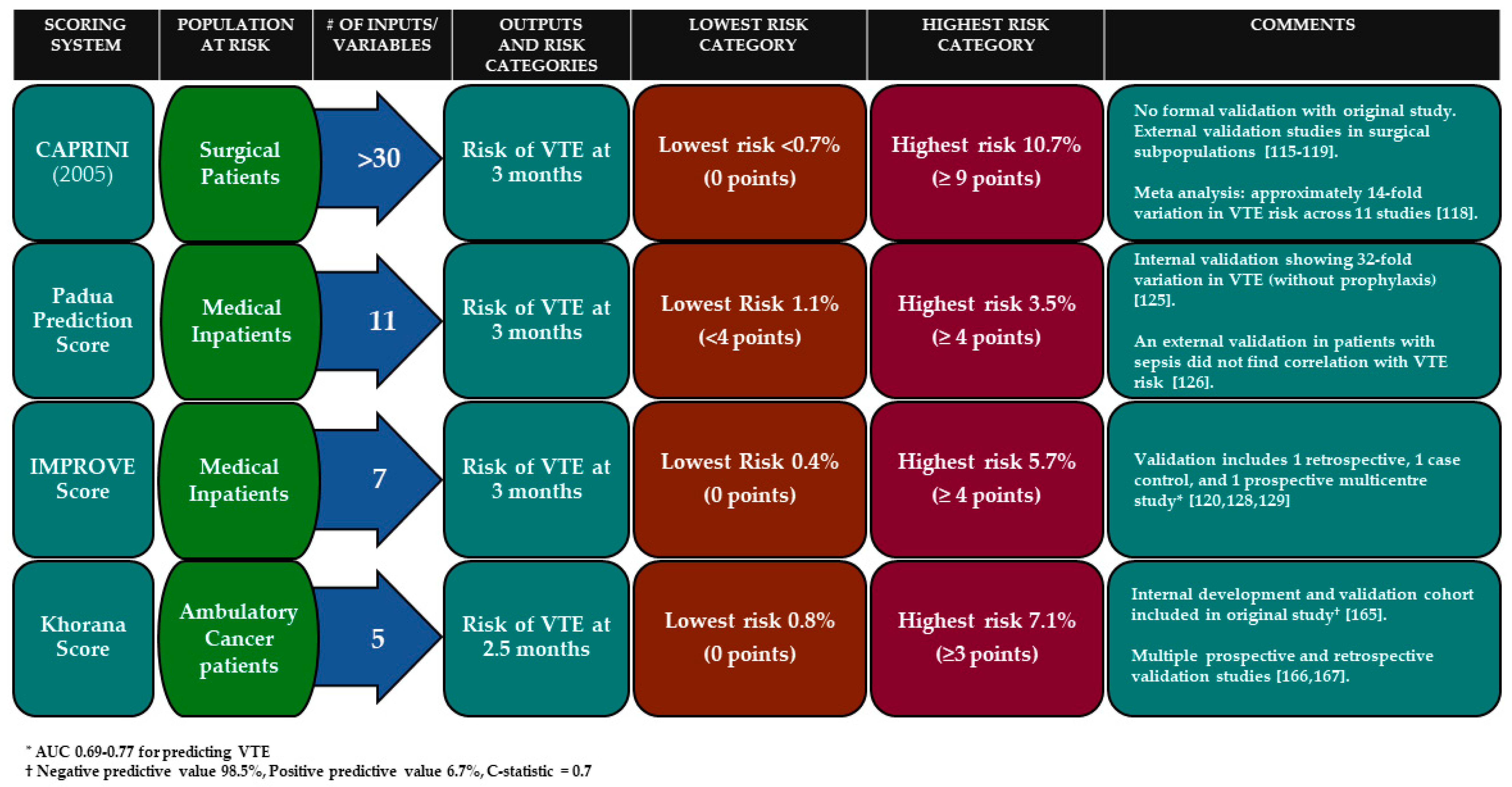
3.3. Implementing and Improving Scoring Systems
3.4. Better Prevention Through Technology
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wendelboe, A.M.; Raskob, G.E. Global Burden of Thrombosis: Epidemiologic Aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Anderson, F.A.; Wheeler, H.B.; Goldberg, R.J.; Hosmer, D.W.; Patwardhan, N.A.; Jovanovic, B.; Forcier, A.; Dalen, J.E. A Population-Based Perspective of the Hospital Incidence and Case-Fatality Rates of Deep Vein Thrombosis and Pulmonary Embolism: The Worcester DVT Study. Arch. Intern. Med. 1991, 151, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Oger, E. Incidence of venous thromboembolism: A community-based study in western France. Thromb. Haemost. 2000, 83, 657–660. [Google Scholar] [CrossRef] [PubMed]
- Riva, N. Cerebral and Splanchnic Vein Thrombosis: Advances, Challenges, and Unanswered Questions. J. Clin. Med. 2020, 9, 743. [Google Scholar] [CrossRef] [PubMed]
- Collins, R.; Scrimgeour, A.; Yusuf, S.; Peto, R. Reduction in fatal pulmonary embolism and venous thrombosis by perioperative administration of subcutaneous heparin. J. Cardiothorac. Anesth. 1988, 2, 853–854. [Google Scholar] [CrossRef] [PubMed]
- Lilly, C.M.; Liu, X.; Badawi, O.; Franey, C.S.; Zuckerman, I.H. Thrombosis prophylaxis and mortality risk among critically Ill adults. Chest 2014, 146, 51–57. [Google Scholar] [CrossRef]
- Millar, J.A. Effect of medical thromboprophylaxis on mortality from pulmonary embolus and major bleeding. Australas. Med. J. 2015, 8, 286–291. [Google Scholar] [CrossRef]
- Novo-Veleiro, I.; Alvela-Suárez, L.; Costa-Grille, A.; Suárez-Dono, J.; Ferrón-Vidan, F.; Pose-Reino, A. Compliance with current VTE prophylaxis guidelines and risk factors linked to complications of VTE prophylaxis in medical inpatients: A prospective cohort study in a Spanish internal medicine department. BMJ Open 2018, 8, 1–5. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Cushman, M.; Burnett, A.E.; Kahn, S.R.; Beyer-Westendorf, J.; Spencer, F.A.; Rezende, S.M.; Zakai, N.A.; Bauer, K.A.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2018, 2, 3198–3225. [Google Scholar] [CrossRef] [PubMed]
- Maynard, G. Preventing Hospital-Associated Venous Thromboembolism: A Guide for Effective Quality Improvement; AHRQ Publ. No. 16-0001-EF; Agency for Healthcare Research and Quality, US Department of Health and Human Services: Rockville, MD, USA, 2016.
- Siegal, D.M.; Eikelboom, J.W.; Lee, S.F.; Rangarajan, S.; Bosch, J.; Zhu, J.; Yusuf, S. Variations in incidence of venous thromboembolism in low-, middle-, and high-income countries. Cardiovasc. Res. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cushman, M.; Tsai, A.W.; White, R.H.; Heckbert, S.R.; Rosamond, W.D.; Enright, P.; Folsom, A.R. Deep vein thrombosis and pulmonary embolism in two cohorts: The longitudinal investigation of thromboembolism etiology. Am. J. Med. 2004, 117, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Hansson, P.O.; Welin, L.; Tibblin, G.; Eriksson, H. Deep vein thrombosis and pulmonary embolism in the general population. “The Study of Men Born in 1913”. Arch. Intern. Med. 1997, 157, 1665–1670. [Google Scholar] [CrossRef] [PubMed]
- Næss, I.A.; Christiansen, S.C.; Romundstad, P.; Cannegieter, S.C.; Rosendaal, F.R.; Hammerstrøm, J. Incidence and mortality of venous thrombosis: A population-based study. J. Thromb. Haemost. 2007, 5, 692–699. [Google Scholar] [CrossRef]
- Silverstein, M.D.; Heit, J.A.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J. Trends in the incidence of deep vein thrombosis and pulmonary embolism: A 25-year population-based study. Arch. Intern. Med. 1998, 158, 585–593. [Google Scholar] [CrossRef]
- Tagalakis, V.; Patenaude, V.; Kahn, S.R.; Suissa, S. Incidence of and mortality from venous thromboembolism in a real-world population: The Q-VTE study cohort. Am. J. Med. 2013, 126, 832.e13–832.e21. [Google Scholar] [CrossRef]
- Grosse, S.D.; Nelson, R.E.; Nyarko, K.A.; Richardson, L.C.; Raskob, G.E. The economic burden of incident venous thromboembolism in the United States: A review of estimated attributable healthcare costs. Thromb. Res. 2016, 137, 3–10. [Google Scholar] [CrossRef]
- Lee, L.H.; Gallus, A.; Jindal, R.; Wang, C.; Wu, C.C. Incidence of Venous Thromboembolism in Asian Populations: A Systematic Review. Thromb. Haemost. 2017, 117, 2243–2260. [Google Scholar] [CrossRef]
- Holst, A.G.; Jensen, G.; Prescott, E. Risk factors for venous thromboembolism: Results from the copenhagen city heart study. Circulation 2010, 121, 1896–1903. [Google Scholar] [CrossRef]
- White, R.; Zhou, H.; Murin, S.; Harvey, D. Effect of ethnicity and gender on the incidence of venous thromboembolism in a diverse population in California in 1996. Thromb. Haemost. 2005, 93, 298–305. [Google Scholar] [CrossRef]
- Goldstein, L.N.; Wu, M.T. A one year audit of patients with venous thromboembolism presenting to a tertiary hospital in Johannesburg, South Africa. Afr. J. Emerg. Med. 2018, 8, 12–15. [Google Scholar] [CrossRef]
- Rasmussen, L.D.; Dybdal, M.; Gerstoft, J.; Kronborg, G.; Larsen, C.; Pedersen, C.; Pedersen, G.; Jensen, J.; Pedersen, L.; Sørensen, H.; et al. HIV and risk of venous thromboembolism: A Danish nationwide population-based cohort study. HIV Med. 2011, 12, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Kline, J.A.; Richardson, D.M.; Than, M.P.; Penaloza, A.; Roy, P.M. Systematic review and meta-analysis of pregnant patients investigated for suspected pulmonary embolism in the emergency department. Acad. Emerg. Med. 2014, 21, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Kruip, M.J.H.A.; Slob, M.J.; Schijen, J.H.E.M.; Van Der Heul, C.; Büller, H.R. Use of a clinical decision rule in combination with D-dimer concentration in diagnostic workup of patients with suspected pulmonary embolism: A prospective management study. Arch. Intern. Med. 2002, 162, 1631–1635. [Google Scholar] [CrossRef] [PubMed]
- Van Der Pol, L.M.; Tromeur, C.; Bistervels, I.M.; Ni Ainle, F.; Van Bemmel, T.; Bertoletti, L.; Couturaud, F.; Van Dooren, Y.P.A.; Elias, A.; Faber, L.M.; et al. Pregnancy-adapted YEARS algorithm for diagnosis of suspected pulmonary embolism. N. Engl. J. Med. 2019, 380, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Bates, S.M.; Jaeschke, R.; Stevens, S.M.; Goodacre, S.; Wells, P.S.; Stevenson, M.D.; Kearon, C.; Schunemann, H.J.; Crowther, M.; Pauker, S.G.; et al. Diagnosis of DVT: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012, 141, e351S–e418S. [Google Scholar] [CrossRef]
- Walton, B.L.; Byrnes, J.R.; Wolberg, A.S. Fibrinogen, red blood cells, and factor XIII in venous thrombosis. J. Thromb. Haemost. 2015, 13, S208–S215. [Google Scholar] [CrossRef]
- Galanaud, J.P.; Quenet, S.; Rivron-Guillot, K.; Quere, I.; Sanchez Muñoz-Torrero, J.F.; Tolosa, C.; Monreal, M. Comparison of the clinical history of symptomatic isolated distal deep-vein thrombosis vs. proximal deep vein thrombosis in 11086 patients. J. Thromb. Haemost. 2009, 7, 2028–2034. [Google Scholar] [CrossRef]
- Kakkar, V.; Howe, C.; Flanc, C.; Clarke, M. Natural History Of Postoperative Deep-Vein Thrombosis. Lancet 1969, 294, 230–233. [Google Scholar] [CrossRef]
- Kearon, C. Natural history of venous thromboembolism. Circulation 2003, 107, 22–30. [Google Scholar] [CrossRef]
- Quinlan, D.J.; Eikelboom, J.W.; Dahl, O.E.; Eriksson, B.I.; Sidhu, P.S.; Hirsh, J. Association between asymptomatic deep vein thrombosis detected by venography and symptomatic venous thromboembolism in patients undergoing elective hip or knee surgery. J. Thromb. Haemost. 2007, 5, 1438–1443. [Google Scholar] [CrossRef]
- Chan, N.C.; Siegal, D.; Lauw, M.N.; Ginsberg, J.S.; Eikelboom, J.W.; Guyatt, G.H.; Hirsh, J. A systematic review of contemporary trials of anticoagulants in orthopaedic thromboprophylaxis: Suggestions for a radical reappraisal. J. Thromb. Thrombolysis 2015, 40, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Valerio, L.; Ambaglio, C.; Barone, M.; Ciola, M.; Konstantinides, S.; Mahmoudpour, S.; Picchi, C.; Pieresca, C.; Trinchero, A.; Barco, S. Recurrence Risk after First Symptomatic Distal versus Proximal Deep Vein Thrombosis According to Baseline Risk Factors. TH Open 2019, 3, e58–e63. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Akl, E.A.; Comerota, A.J.; Prandoni, P.; Bounameaux, H.; Goldhaber, S.Z.; Nelson, M.E.; Wells, P.S.; Gould, M.K.; Dentali, F.; et al. Antithrombotic therapy for VTE disease: Antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2012, 141, e419S–e496S. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Ageno, W.; Becattini, C.; Galli, L.; Gianni, M.; Riva, N.; Imberti, D.; Squizzato, A.; Venco, A.; Agnelli, G. Prevalence and Clinical History of Incidental, Asymptomatic Pulmonary Embolism: A Meta-Analysis. Thromb. Res. 2010, 125, 518–522. [Google Scholar] [CrossRef]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Yusuf, H.; Tsai, J.; Siddiqi, A.-E.-A.; Boulet, S.; Soucie, J.M. Emergency department visits by patients with venous thromboembolism, 1998–2009. J. Hosp. Adm. 2012, 1, 1. [Google Scholar] [CrossRef]
- Yoo, H.H.; Nunes-Nogueira, V.S.; Fortes Villas Boas, P.J. Anticoagulant treatment for subsegmental pulmonary embolism. Cochrane Database Syst. Rev. 2020, 2, CD010222. [Google Scholar] [CrossRef]
- Carrier, M. A Study to Evaluate the Safety of Withholding Anticoagulation in Patients With Subsegmental PE Who Have a Negative Serial Bilateral Lower Extremity Ultrasound (SSPE). U.S National Library of Medicine Clinical Trials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT01455818 (accessed on 24 May 2020).
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Francis, C.W.; et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J. Clin. Oncol. 2020, 38, 496–520. [Google Scholar] [CrossRef]
- Cohen, A.T.; Agnelli, G.; Anderson, F.A.; Arcelus, J.; Bergqvist, D.; Brecht, J.G.; Greer, I.A.; Heit, J.A.; Hutchinson, J.L.; Kakkar, A.K.; et al. Venous Thromboembolism (VTE) in Europe. Thromb. Haemost. 2007, 98, 756–764. [Google Scholar] [CrossRef]
- Heit, J.A.; Spencer, F.A.; White, R.H. The epidemiology of venous thromboembolism. J. Thromb. Thrombolysis 2016, 41, 3–14. [Google Scholar] [CrossRef]
- Heit, J.A.; Silverstein, M.D.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J. Predictors of survival after deep vein thrombosis and pulmonary embolism: A population-based, cohort study. Arch. Intern. Med. 1999, 159, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Ende-Verhaar, Y.M.; Tick, L.W.; Klok, F.A.; Huisman, M.V.; Rosendaal, F.R.; le Cessie, S.; Cannegieter, S.C. Post-thrombotic syndrome: Short and long-term incidence and risk factors. Thromb. Res. 2019, 177, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Kahn, S.R.; Kearon, C.; Julian, J.A.; Mackinnon, B.; Kovacs, M.J.; Wells, P.; Crowther, M.A.; Anderson, D.R.; Van Nguyen, P.; Demers, C.; et al. Predictors of the post-thrombotic syndrome during long-term treatment of proximal deep vein thrombosis. J. Thromb. Haemost. 2005, 3, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Ende-Verhaar, Y.M.; Cannegieter, S.C.; Noordegraaf, A.V.; Delcroix, M.; Pruszczyk, P.; Mairuhu, A.T.A.; Huisman, M.V.; Klok, F.A. Incidence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism: A contemporary view of the published literature. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef]
- Pengo, V.; Lensing, A.W.A.; Prins, M.H.; Marchiori, A.; Davidson, B.L.; Tiozzo, F.; Albanese, P.; Biasiolo, A.; Pegoraro, C.; Iliceto, S.; et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N. Engl. J. Med. 2004, 350, 2257–2264. [Google Scholar] [CrossRef]
- Boon, G.J.A.M.; van Rein, N.; Bogaard, H.J.; Ende-Verhaar, Y.M.; Huisman, M.V.; Kroft, L.J.M.; van der Meer, F.J.M.; Meijboom, L.J.; Symersky, P.; Noordegraaf, A.V.; et al. Quality of initial anticoagulant treatment and risk of CTEPH after acute pulmonary embolism. PLoS ONE 2020, 15, 1–11. [Google Scholar] [CrossRef]
- Ghanima, W.; Wik, H.S.; Tavoly, M.; Enden, T.; Jelsness-Jørgensen, L.P. Late consequences of venous thromboembolism: Measuring quality of life after deep vein thrombosis and pulmonary embolism. Thromb. Res. 2018, 164, 170–176. [Google Scholar] [CrossRef]
- Sista, A.K.; Klok, F.A. Late outcomes of pulmonary embolism: The post-PE syndrome. Thromb. Res. 2018, 164, 157–162. [Google Scholar] [CrossRef]
- Johnson, S.A.; Stevens, S.M.; Woller, S.C.; Lake, E.; Donadini, M.; Cheng, J.; Labarère, J.; Douketis, J.D. Risk of deep vein thrombosis following a single negative whole-leg compression ultrasound: A systematic review and meta-analysis. JAMA 2010, 303, 438–445. [Google Scholar] [CrossRef]
- Hirsh, J.; Ginsberg, J.S.; Chan, N.; Guyatt, G.; Eikelboom, J.W. Mandatory contrast-enhanced venography to detect deep-vein thrombosis (DVT) in studies of DVT prophylaxis: Upsides and downsides. Thromb. Haemost. 2013, 111, 10–13. [Google Scholar] [CrossRef]
- Choi, H.S.; Kim, H.J.; Kang, H.J.; Lee, J.W.; Shin, H.Y.; Park, H.J.; Park, B.K.; Lee, Y.H.; Lee, J.A.; Lim, Y.J.; et al. Thromboembolism in children with cancer: A retrospective multicenter study in Korea. J. Thromb. Thrombolysis 2019, 47, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Andrew, M.; David, M.; Adams, M.; Ali, K.; Anderson, R.; Barnard, D.; Bernstein, M.; Brisson, L.; Cairney, B.; DeSai, D.; et al. Venous thromboembolic complications (VTE) in children: First analyses of the Canadian registry of VTE. Blood 1994, 83, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Biss, T.T.; Brandão, L.R.; Kahr, W.H.; Chan, A.K.; Williams, S. Clinical features and outcome of pulmonary embolism in children. Br. J. Haematol. 2008, 142, 808–818. [Google Scholar] [CrossRef] [PubMed]
- Gouin, B.; Blondon, M.; Jiménez, D.; Fernández-Capitán, C.; Bounameaux, H.; Soler, S.; Duce, R.; Sahuquillo, J.C.; Ruiz-Giménez, N.; Monreal, M. Clinical Prognosis of Nonmassive Central and Noncentral Pulmonary Embolism: A Registry-Based Cohort Study. Chest 2017, 151, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Mari, D.; Ogliari, G.; Castaldi, D.; Vitale, G.; Bollini, E.M.; Lio, D. Hemostasis and ageing. Immun. Ageing 2008, 5, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Middeldorp, S.; Van Hylckama Vlieg, A. Does thrombophilia testing help in the clinical management of patients? Br. J. Haematol. 2008, 143, 321–335. [Google Scholar] [CrossRef]
- Gohil, R.; Peck, G.; Sharma, P. The genetics of venous thromboembolism: A meta-analysis involving ~120,000 cases and 180,000 controls. Thromb. Haemost. 2009, 102, 360–370. [Google Scholar] [CrossRef]
- Varga, E.A.; Kujovich, J.L. Management of inherited thrombophilia: Guide for genetics professionals. Clin. Genet. 2012, 81, 7–17. [Google Scholar] [CrossRef]
- Rees, D.C.; Cox, M.; Clegg, J.B. World distribution of factor V Leiden. Lancet 1995, 346, 1133–1134. [Google Scholar] [CrossRef]
- Dziadosz, M.; Baxi, L.V. Global prevalence of prothrombin gene mutation G20210A and implications in women’s health: A systematic review. Blood Coagul. Fibrinolysis 2016, 27, 481–489. [Google Scholar] [CrossRef]
- Dykes, A.C.; Walker, I.D.; Mcmahon, A.D.; Islam, S.I.A.M.; Tait, R.C. A study of Protein S antigen levels in 3788 healthy volunteers: Influence of age, sex and hormone use, and estimate for prevalence of deficiency state. Br. J. Haematol. 2001, 113, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Tait, R.C.; Walker, I.D.; Reitsma, P.H.; Islam, S.I.; McCall, F.; Poort, S.R.; Conkie, J.A.; Bertina, R.M. Prevalence of protein C deficiency in the healthy population. Thromb. Haemost. 1995, 73, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Croles, F.N.; Borjas-Howard, J.; Nasserinejad, K.; Leebeek, F.W.G.; Meijer, K. Risk of Venous Thrombosis in Antithrombin Deficiency: A Systematic Review and Bayesian Meta-analysis. Semin. Thromb. Hemost. 2018, 44, 315–326. [Google Scholar] [CrossRef] [PubMed]
- Samama, M.M. An epidemiologic study of risk factors for deep vein thrombosis in medical outpatients: The sirius study. Arch. Intern. Med. 2000, 160, 3415–3420. [Google Scholar] [CrossRef] [PubMed]
- Simone, B.; De Stefano, V.; Leoncini, E.; Zacho, J.; Martinelli, I.; Emmerich, J.; Rossi, E.; Folsom, A.R.; Almawi, W.Y.; Scarabin, P.Y.; et al. Risk of venous thromboembolism associated with single and combined effects of Factor V Leiden, Prothrombin 20210A and Methylenetethraydrofolate reductase C677T: A meta-analysis involving over 11,000 cases and 21,000 controls. Eur. J. Epidemiol. 2013, 28, 621–647. [Google Scholar] [CrossRef] [PubMed]
- Hirmerová, J. Homocysteine and venous thromboembolism-is there any link? Cor Vasa 2013, 55, 248–258. [Google Scholar] [CrossRef]
- Schambeck, C.M.; Hinney, K.; Haubitz, I.; Taleghani, B.M.; Wahler, D.; Keller, F. Familial clustering of high factor VIII levels in patients with venous thromboembolism. Arter. Thromb. Vasc. Biol. 2001, 21, 289–292. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ho, W.K.; Hankey, G.J.; Quinlan, D.J.; Eikelboom, J.W. Risk of recurrent venous thromboembolism in patients with common thrombophilia: A systematic review. Arch. Intern. Med. 2006, 166, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C. Antithrombotic Therapy for VTE Disease. Chest J. 2012, 141, e419S. [Google Scholar] [CrossRef]
- Federici, E.H.; Al-Mondhiry, H. High risk of thrombosis recurrence in patients with homozygous and compound heterozygous factor V R506Q (Factor V Leiden) and prothrombin G20210A. Thromb. Res. 2019, 182, 75–78. [Google Scholar] [CrossRef]
- Segal, J.B.; Brotman, D.J.; Necochea, A.J.; Emadi, A.; Samal, L.; Wilson, L.M.; Crim, M.T.; Bass, E.B. Predictive Value of Factor V Leiden and Prothrombin G20210A in Adults With Venous Thromboembolism and in Family Members of Those With a Mutation. JAMA 2009, 301, 2472. [Google Scholar] [CrossRef] [PubMed]
- Lijfering, W.M.; Middeldorp, S.; Veeger, N.J.G.M.; Hamulyák, K.; Prins, M.H.; Büller, H.R.; Van Der Meer, J. Risk of recurrent venous thrombosis in homozygous carriers and double heterozygous carriers of factor v leiden and prothrombin G20210A. Circulation 2010, 121, 1706–1712. [Google Scholar] [CrossRef] [PubMed]
- Van Hylckama Vlieg, A.; Helmerhorst, F.M.; Rosendaal, F.R. The risk of deep venous thrombosis associated with injectable depot-medroxyprogesterone acetate contraceptives or a levonorgestrel intrauterine device. Arter. Thromb. Vasc. Biol. 2010, 30, 2297–2300. [Google Scholar] [CrossRef] [PubMed]
- Vlieg, A.V.H.; Helmerhorst, F.M.; Vandenbroucke, J.P.; Doggen, C.J.M.; Rosendaal, F.R. The venous thrombotic risk of oral contraceptives, effects of oestrogen dose and progestogen type: Results of the MEGA case-control study. Br. Med. J. 2001, 339, h2921. [Google Scholar] [CrossRef] [PubMed]
- Oedingen, C.; Scholz, S.; Razum, O. Systematic review and meta-analysis of the association of combined oral contraceptives on the risk of venous thromboembolism: The role of the progestogen type and estrogen dose. Thromb. Res. 2018, 165, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Lidegaard, O.; Nielsen, L.H.; Skovlund, C.W.; Løkkegaard, E. Venous thrombosis in users of non-oral hormonal contraception: Follow-up study, Denmark 2001–10. BMJ 2012, 344, 1–9. [Google Scholar] [CrossRef]
- Lidegaard, Ø.; Edström, B.; Kreiner, S. Oral contraceptives and venous thromboembolism: A five-year national case-control study. Contraception 2002, 65, 187–196. [Google Scholar] [CrossRef]
- Jick, H.; Jick, S.S.; Myers, M.W.; Vasilakis, C.; Gurewich, V. Risk of idiopathic cardiovascular death and rionfatal venous thromboembolism in women using oral contraceptives with differing progestagen components. Lancet 1995, 346, 1589–1593. [Google Scholar] [CrossRef]
- Baratloo, A.; Safari, S.; Rouhipour, A.; Hashemi, B.; Rahmati, F.; Motamedi, M.; Forouzanfar, M.; Haroutunian, P. The Risk of Venous Thromboembolism with Different Generation of Oral Contraceptives; a Systematic Review and Meta-Analysis. Emergency 2014, 2, 1–11. [Google Scholar] [CrossRef]
- Canonico, M.; Plu-Bureau, G.; Lowe, G.D.O.; Scarabin, P.Y. Hormone replacement therapy and risk of venous thromboembolism in postmenopausal women: Systematic review and meta-analysis. BMJ 2008, 336, 1227–1231. [Google Scholar] [CrossRef]
- Vinogradova, Y.; Coupland, C.; Hippisley-Cox, J. Use of hormone replacement therapy and risk of venous thromboembolism: Nested case-control studies using the QResearch and CPRD databases. BMJ 2019, 364, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Silverstein, M.D.; Mohr, D.N.; Petterson, T.M.; O’Fallon, W.M.; Melton, L.J. Risk factors for deep vein thrombosis and pulmonary embolism: A population-based case-control study. Arch. Intern. Med. 2000, 160, 809–815. [Google Scholar] [CrossRef] [PubMed]
- Cannegieter, S.C.; Doggen, C.J.M.; Van Houwelingen, H.C.; Rosendaal, F.R. Travel-Related Venous Thrombosis: Results from a Large Population-Based Case Control Study (MEGA Study). PLoS Med. 2006, 3. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.F.; Zakai, N.A.; Maclehose, R.F.; Cowan, L.T.; Adam, T.J.; Alonso, A.; Lutsey, P.L. Association of Testosterone Therapy with Risk of Venous Thromboembolism among Men with and without Hypogonadism. JAMA Intern. Med. 2019, 55413, 1–8. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Perrin, K.; Aldington, S.; Weatherall, M.; Beasley, R. A case-control study of seated immobility at work as a risk factor for venous thromboembolism. J. R. Soc. Med. 2008, 101, 237–243. [Google Scholar] [CrossRef]
- Moigne, E.L.; Tromeur, C.; Delluc, A.; Gouillou, M.; Alavi, Z.; Lacut, K.; Mottier, D.; Gal, G. Le Risk of recurrent venous thromboembolism on progestin-only contraception: A cohort study. Haematologica 2016, 101, e12–e14. [Google Scholar] [CrossRef]
- Tepper, N.K.; Whiteman, M.K.; Marchbanks, P.A.; James, A.H.; Curtis, K.M. Progestin-only contraception and thromboembolism: A systematic review. Contraception 2016, 94, 678–700. [Google Scholar] [CrossRef]
- Abe, K.; Kuklina, E.V.; Hooper, W.C.; Callaghan, W.M. Venous thromboembolism as a cause of severe maternal morbidity and mortality in the United States. Semin. Perinatol. 2019, 43, 200–204. [Google Scholar] [CrossRef]
- Ray, J.G.; Chan, W.S. Deep vein thrombosis during pregnancy and the puerperium: A meta- analysis of the period of risk and the leg of presentation. Obs. Gynecol. Surv. 1999, 54, 265–271. [Google Scholar] [CrossRef]
- Greer, I.A.; Nelson-Piercy, C. Low-molecular-weight heparins for thromboprophylaxis and treatment of venous thromboembolism in pregnancy: A systematic review of safety and efficacy. Blood 2005, 106, 401–407. [Google Scholar] [CrossRef]
- Bates, S.M.; Rajasekhar, A.; Middeldorp, S.; McLintock, C.; Rodger, M.A.; James, A.H.; Vazquez, S.R.; Greer, I.A.; Riva, J.J.; Bhatt, M.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Venous thromboembolism in the context of pregnancy. Blood Adv. 2018, 2, 3317–3359. [Google Scholar] [CrossRef]
- Kourlaba, G.; Relakis, J.; Kontodimas, S.; Holm, M.V.; Maniadakis, N. A systematic review and meta-analysis of the epidemiology and burden of venous thromboembolism among pregnant women. Int. J. Gynecol. Obs. 2016, 132, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Abbattista, M.; Gianniello, F.; Novembrino, C.; Clerici, M.; Artoni, A.; Bucciarelli, P.; Capecchi, M.; Peyvandi, F.; Martinelli, I. Risk of pregnancy-related venous thromboembolism and obstetrical complications in women with inherited type I antithrombin deficiency: A retrospective, single-centre, cohort study. Lancet Haematol. 2020, 7, e320–e328. [Google Scholar] [CrossRef]
- Gerhardt, A.; Scharf, R.E.; Greer, I.A.; Zotz, R.B. Hereditary risk factors for thrombophilia and probability of venous thromboembolism during pregnancy and the puerperium. Blood 2016, 128, 2343–2349. [Google Scholar] [CrossRef] [PubMed]
- Kovac, M. Antithrombin deficiency in pregnancy—The unresolved issues. Lancet Haematol. 2020, 7, e276–e278. [Google Scholar] [CrossRef]
- Refaei, M.; Xing, L.; Lim, W.; Crowther, M.; Boonyawat, K. Management of Venous Thromboembolism in Patients with Hereditary Antithrombin Deficiency and Pregnancy: Case Report and Review of the Literature. Case Rep. Hematol. 2017, 2017, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chauleur, C.; Quenet, S.; Varlet, M.N.; Seffert, P.; Laporte, S.; Decousus, H.; Mismetti, P. Feasibility of an easy-to-use risk score in the prevention of venous thromboembolism and placental vascular complications in pregnant women: A prospective cohort of 2736 women. Thromb. Res. 2008, 122, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Dargaud, Y.; Rugeri, L.; Fleury, C.; Battie, C.; Gaucherand, P.; Huissoud, C.; Rudigoz, R.C.; Desmurs-Clavel, H.; Ninet, J.; Trzeciak, M.C. Personalized thromboprophylaxis using a risk score for the management of pregnancies with high risk of thrombosis: A prospective clinical study. J. Thromb. Haemost. 2017, 15, 897–906. [Google Scholar] [CrossRef]
- Sultan, A.A.; West, J.; Grainge, M.J.; Riley, R.D.; Tata, L.J.; Stephansson, O.; Fleming, K.M.; Nelson-Piercy, C.; Ludvigsson, J.F. Development and validation of risk prediction model for venous thromboembolism in postpartum women: Multinational cohort study. BMJ 2016, 355. [Google Scholar] [CrossRef]
- Testa, S.; Passamonti, S.M.; Paoletti, O.; Bucciarelli, P.; Ronca, E.; Riccardi, A.; Rigolli, A.; Zimmermann, A.; Martinelli, I. The “Pregnancy Health-care Program” for the prevention of venous thromboembolism in pregnancy. Intern. Emerg. Med. 2015, 10, 129–134. [Google Scholar] [CrossRef]
- Reducing the risk of thrombosis and embolism during pregnancy and the puerperium. Green-top Guideline No. 37a. J. Matern. Neonatal Med. 2018. [CrossRef]
- Sweetland, S.; Green, J.; Liu, B.; De González, A.B.; Canonico, M.; Reeves, G.; Beral, V. Duration and magnitude of the postoperative risk of venous thromboembolism in middle aged women: Prospective cohort study. BMJ 2009, 339, 32. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, A.B.; Ehrenstein, V.; Szépligeti, S.K.; Sørensen, H.T. Excess risk of venous thromboembolism in hip fracture patients and the prognostic impact of comorbidity. Osteoporos. Int. 2017, 28, 3421–3430. [Google Scholar] [CrossRef] [PubMed]
- Januel, J.-M.; Chen, G.; Ruffieux, C.; Quan, H.; Douketis, J.D.; Crowther, M.A.; Colin, C.; Ghali, W.A.; Burnand, B. IMECCHI Group, for the Symptomatic In-Hospital Deep Vein Thrombosis and Pulmonary Embolism Following Hip and Knee Arthroplasty Among Patients Receiving Recommended Prophylaxis. JAMA 2012, 307, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-I.; Kang, D.-G.; Khurana, S.S.; Lee, S.-H.; Cho, Y.-J.; Bae, D.-K. Thromboprophylaxis for Deep Vein Thrombosis and Pulmonary Embolism after Total Joint Arthroplasty in a Low Incidence Population. Knee Surg. Relat. Res. 2013, 25, 43–53. [Google Scholar] [CrossRef]
- Bouras, G.; Burns, E.M.; Howell, A.M.; Bottle, A.; Athanasiou, T.; Darzi, A. Risk of post-discharge venous thromboembolism and associated mortality in general surgery: A population-based cohort study using linked hospital and primary care data in England. PLoS ONE 2015, 10, 1–16. [Google Scholar] [CrossRef]
- Anderson, D.R.; Dunbar, M.; Murnaghan, J.; Kahn, S.R.; Gross, P.; Forsythe, M.; Pelet, S.; Fisher, W.; Belzile, E.; Dolan, S.; et al. Aspirin or rivaroxaban for VTE prophylaxis after hip or knee arthroplasty. N. Engl. J. Med. 2018, 378, 699–707. [Google Scholar] [CrossRef]
- Jorgensen, E.M.; Li, A.; Modest, A.M.; Leung, K.; Moore Simas, T.A.; Hur, H.-C. Incidence of Venous Thromboembolism After Different Modes of Gynecologic Surgery. Obs. Gynecol. 2018, 132, 1275–1284. [Google Scholar] [CrossRef]
- Anderson, D.R.; Morgano, G.P.; Bennett, C.; Dentali, F.; Francis, C.W.; Garcia, D.A.; Kahn, S.R.; Rahman, M.; Rajasekhar, A.; Rogers, F.B.; et al. American Society of Hematology 2019 guidelines for management of venous thromboembolism: Prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019, 3, 3898–3944. [Google Scholar] [CrossRef]
- Caprini, J.A.; Arcelus, J.I.; Hasty, J.H.; Tamhane, A.C.; Fabrega, F. Clinical assessment of venous thromboembolic risk in surgical patients. Semin. Thromb. Hemost. 1991, 17 (Suppl. 3), 304–312. [Google Scholar]
- Caprini, J.A. Thrombosis Risk Assessment as a Guide to Quality Patient Care. Disease-a-Month 2005, 51, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Obi, A.T.; Pannucci, C.J.; Nackashi, A.; Abdullah, N.; Alvarez, R.; Bahl, V.; Wakefield, T.W.; Henke, P.K. Validation of the caprini venous thromboembolism risk assessment model in critically ill surgical patients. Jama Surg. 2015, 150, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Pannucci, C.J.; Bailey, S.H.; Dreszer, G.; Fisher Wachtman, C.; Zumsteg, J.W.; Jaber, R.M.; Hamill, J.B.; Hume, K.M.; Rubin, J.P.; Neligan, P.C.; et al. Validation of the Caprini Risk Assessment Model in Plastic and Reconstructive Surgery Patients. J. Am. Coll. Surg. 2011, 212, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Pannucci, C.J.; Swistun, L.; MacDonald, J.K.; Henke, P.K.; Brooke, B.S. Individualized venous thromboembolism risk stratification using the 2005 caprini score to identify the benefits and harms of chemoprophylaxis in surgical patients: A meta-analysis. Ann. Surg. 2017, 265, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Saragas, N.P.; Ferrao, P.N.F.; Saragas, E.; Jacobson, B.F. The impact of risk assessment on the implementation of venous thromboembolism prophylaxis in foot and ankle surgery. Foot Ankle Surg. 2014, 20, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Amin, A.N.; Varker, H.; Princic, N.; Lin, J.; Thompson, S.; Johnston, S. Duration of venous thromboembolism risk across a continuum in medically ill hospitalized patients. J. Hosp. Med. 2012, 7, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Anderson, F.A.; FitzGerald, G.; Decousus, H.; Pini, M.; Chong, B.H.; Zotz, R.B.; Bergmann, J.F.; Tapson, V.; Froehlich, J.B.; et al. Predictive and associative models to identify hospitalized medical patients at risk for VTE. Chest 2011, 140, 706–714. [Google Scholar] [CrossRef]
- Darzi, A.J.; Karam, S.G.; Charide, R.; Etxeandia-Ikobaltzeta, I.; Cushman, M.; Gould, M.K.; Mbuagbaw, L.; Spencer, F.A.; Spyropoulos, A.C.; Streiff, M.B.; et al. Prognostic factors for VTE and Bleeding in Hospitalized Medical Patients: A systematic review and and meta-analysis. Blood 2020, 135, 1788–1810. [Google Scholar] [CrossRef]
- Chan, N.C.; Gross, P.L.; Weitz, J.I. Addressing the burden of hospital-related venous thromboembolism: The role of extended anticoagulant prophylaxis. J. Thromb. Haemost. 2018, 16, 413–417. [Google Scholar] [CrossRef]
- Leizorovicz, A.; Cohen, A.T.; Turpie, A.G.G.; Olsson, C.G.; Vaitkus, P.T.; Goldhaber, S.Z. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients. Circulation 2004, 110, 874–879. [Google Scholar] [CrossRef]
- Samama, M.M.; Cohen, A.T.; Darmon, J.Y.; Desjardins, L.; Eldor, A.; Janbon, C.; Leizorovicz, A.; Nguyen, H.; Olsson, C.G.; Turpie, A.G.; et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. N. Engl. J. Med. 1999, 341, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Barbar, S.; Noventa, F.; Rossetto, V.; Ferrari, A.; Brandolin, B.; Perlati, M.; De Bon, E.; Tormene, D.; Pagnan, A.; Prandoni, P. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: The Padua Prediction Score. J. Thromb. Haemost. 2010, 8, 2450–2457. [Google Scholar] [CrossRef] [PubMed]
- Vardi, M.; Ghanem-Zoubi, N.O.; Zidan, R.; Yurin, V.; Bitterman, H. Venous thromboembolism and the utility of the Padua Prediction Score in patients with sepsis admitted to internal medicine departments. J. Thromb. Haemost. 2013, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.; Spyropoulos, A.; Cohen, A.; Hull, R.; Goldhaber, S.; Yusen, R.; Hernandez, A.; Korjian, S.; Daaboul, Y.; Gold, A.; et al. The IMPROVEDD VTE Risk Score: Incorporation of D-Dimer into the IMPROVE Score to Improve Venous Thromboembolism Risk Stratification. TH Open 2017, 1, e56–e65. [Google Scholar] [CrossRef] [PubMed]
- Mahan, C.E.; Liu, Y.; Douketis, J.D.; Turpie, A.G.G.; Dairkee, U.; Spyropoulos, A.C. Venous Thromboembolism Validation Study of the IMPROVE Risk Assessment Models in the Medical Patient (VTE-VALOURR). Blood 2011, 118, 4218. [Google Scholar] [CrossRef]
- Rosenberg, D.; Eichorn, A.; Alarcon, M.; McCullagh, L.; McGinn, T.; Spyropoulos, A.C. External validation of the risk assessment model of the international medical prevention registry on venous thromboembolism (IMPROVE) for medical patients in a tertiary health system. J. Am. Heart Assoc. 2014, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Lipardi, C.; Xu, J.; Peluso, C.; Spiro, T.E.; De Sanctis, Y.; Barnathan, E.S.; Raskob, G.E. Modified IMPROVE VTE Risk Score and Elevated D-Dimer Identify a High Venous Thromboembolism Risk in Acutely Ill Medical Population for Extended Thromboprophylaxis. TH Open 2020, 4, e59–e65. [Google Scholar] [CrossRef] [PubMed]
- Haut, E.R.; Lau, B.D.; Kraenzlin, F.S.; Hobson, D.B.; Kraus, P.S.; Carolan, H.T.; Haider, A.H.; Holzmueller, C.G.; Efron, D.T.; Pronovost, P.J.; et al. Improved Prophylaxis and Decreased Rates of Preventable Harm With the Use of a Mandatory Computerized Clinical Decision Support Tool for Prophylaxis for Venous Thromboembolism in Trauma. Arch. Surg. 2012, 147, 901. [Google Scholar] [CrossRef] [PubMed]
- Turrentine, F.E.; Sohn, M.W.; Wilson, S.L.; Stanley, C.; Novicoff, W.; Sawyer, R.G.; Williams, M.D. Fewer thromboembolic events after implementation of a venous thromboembolism risk stratification tool. J. Surg. Res. 2018, 225, 148–156. [Google Scholar] [CrossRef]
- Henke, P.K.; Kahn, S.R.; Pannucci, C.J.; Secemksy, E.A.; Evans, N.S.; Khorana, A.A.; Creager, M.A.; Pradhan, A.D. Call to Action to Prevent Venous Thromboembolism in Hospitalized Patients: A Policy Statement From the American Heart Association. Circulation 2020, 141, e914–e931. [Google Scholar] [CrossRef]
- Cohen, A.T.; Spiro, T.E.; Büller, H.R.; Haskell, L.; Hu, D.; Hull, R.; Mebazaa, A.; Merli, G.; Schellong, S.; Spyropoulos, A.C.; et al. Rivaroxaban for thromboprophylaxis in acutely ill medical patients. N. Engl. J. Med. 2013, 368, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.T.; Harrington, R.A.; Goldhaber, S.Z.; Hull, R.D.; Wiens, B.L.; Gold, A.; Hernandez, A.F.; Gibson, C.M.; Bello, F.; Ferrari, A.E.; et al. Extended thromboprophylaxis with betrixaban in acutely ill medical patients. N. Engl. J. Med. 2016, 375, 534–544. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, K.; Spyropoulos, A.C. New Paradigms of Extended Thromboprophylaxis in Medically Ill Patients. J. Clin. Med. 2020, 9, 1002. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Keller, T.T.; Van Gorp, E.; Ten Cate, H. Infection and inflammation and the coagulation system. Cardiovasc. Res. 2003, 60, 26–39. [Google Scholar] [CrossRef]
- Minet, C.; Potton, L.; Bonadona, A.; Hamidfar-Roy, R.; Somohano, C.A.; Lugosi, M.; Cartier, J.C.; Ferretti, G.; Schwebel, C.; Timsit, J.F. Venous thromboembolism in the ICU: Main characteristics, diagnosis and thromboprophylaxis. Crit. Care 2015, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Wright, F.L.; Vogler, T.O.; Moore, E.E.; Moore, H.B.; Wohlauer, M.V.; Urban, S.; Nydam, T.L.; Moore, P.K.; McIntyre, R.C. Fibrinolysis Shutdown Correlation with Thromboembolic Events in Severe COVID-19 Infection. J. Am. Coll. Surg. 2020, 142, 114–128. [Google Scholar] [CrossRef]
- Panigada, M.; Bottino, N.; Tagliabue, P.; Grasselli, G.; Novembrino, C.; Chantarangkul, V.; Pesenti, A.; Peyvandi, F.; Tripodi, A. Hypercoagulability of COVID-19 patients in Intensive Care Unit. A Report of Thromboelastography Findings and other Parameters of Hemostasis. J. Thromb. Haemost. 2020, 1738–1742. [Google Scholar] [CrossRef]
- Maatman, T.K.; Jalali, F.; Feizpour, C.; Douglas, A.; McGuire, S.P.; Kinnaman, G.; Hartwell, J.L.; Maatman, B.T.; Kreutz, R.P.; Kapoor, R.; et al. Routine Venous Thromboembolism Prophylaxis May Be Inadequate in the Hypercoagulable State of Severe Coronavirus Disease 2019. Crit. Care Med. 2020, 1–8. [Google Scholar] [CrossRef]
- Klok, F.A.; Kruip, M.J.H.A.; van der Meer, N.J.M.; Arbous, M.S.; Gommers, D.; Kant, K.M.; Kaptein, F.H.J.; van Paassen, J.; Stals, M.A.M.; Huisman, M.V.; et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb. Res. 2020. [Google Scholar] [CrossRef]
- Fox, S.E.; Akmatbekov, A.; Harbert, J.L.; Li, G.; Quincy Brown, J.; Vander Heide, R.S. Pulmonary and cardiac pathology in African American patients with COVID-19: An autopsy series from New Orleans. Lancet Respir. Med. 2020, 8, 681–686. [Google Scholar] [CrossRef]
- Lodigiani, C.; Iapichino, G.; Carenzo, L.; Cecconi, M.; Ferrazzi, P.; Sebastian, T.; Kucher, N.; Studt, J.D.; Sacco, C.; Alexia, B.; et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb. Res. 2020, 191, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Demelo-Rodríguez, P.; Cervilla-Muñoz, E.; Ordieres-Ortega, L.; Parra-Virto, A.; Toledano-Macías, M.; Toledo-Samaniego, N.; García-García, A.; García-Fernández-Bravo, I.; Ji, Z.; de-Miguel-Diez, J.; et al. Incidence of asymptomatic deep vein thrombosis in patients with COVID-19 pneumonia and elevated D-dimer levels. Thromb. Res. 2020, 192, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tavazzi, G.; Civardi, L.; Caneva, L.; Mongodi, S.; Mojoli, F. Thrombotic events in SARS-CoV-2 patients: An urgent call for ultrasound screening. Intensive Care Med. 2020, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Poissy, J.; Goutay, J.; Caplan, M.; Parmentier, E.; Duburcq, T.; Lassalle, F.; Jeanpierre, E.; Rauch, A.; Labreuche, J.; Susen, S. Pulmonary Embolism in COVID-19 Patients: Awareness of an Increased Prevalence. Circulation 2020, 1–6. [Google Scholar] [CrossRef]
- Llitjos, J.-F.; Leclerc, M.; Chochois, C.; Monsallier, J.-M.; Ramakers, M.; Auvray, M.; Merouani, K. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef]
- Helms, J.; Tacquard, C.; Severac, F.; Leonard-Lorant, I.; Ohana, M.; Delabranche, X.; Merdji, H.; Clere-Jehl, R.; Schenck, M.; Fagot Gandet, F.; et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: A multicenter prospective cohort study. Intensive Care Med. 2020, 46, 1089–1098. [Google Scholar] [CrossRef]
- Middeldorp, S.; Coppens, M.; van Haaps, T.F.; Foppen, M.; Vlaar, A.P.; Müller, M.C.A.; Bouman, C.C.S.; Beenen, L.F.M.; Kootte, R.S.; Heijmans, J.; et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef]
- Zhang, L.; Feng, X.; Zhang, D.; Jiang, C.; Mei, H.; Wang, J.; Zhang, C.; Li, H.; Xia, X.; Kong, S.; et al. Deep Vein Thrombosis in Hospitalized Patients with Coronavirus Disease 2019 (COVID-19) in Wuhan, China: Prevalence, Risk Factors, and Outcome. Circulation 2020, 114–128. [Google Scholar] [CrossRef]
- Thomas, W.; Varley, J.; Johnston, A.; Symington, E.; Robinson, M.; Sheares, K.; Lavinio, A.; Besser, M. Thrombotic complications of patients admitted to intensive care with COVID-19 at a teaching hospital in the United Kingdom. Thromb. Res. 2020, 191, 76–77. [Google Scholar] [CrossRef] [PubMed]
- Paranjpe, I.; Fuster, V.; Lala, A.; Russak, A.J.; Glicksberg, B.S.; Levin, M.A.; Charney, A.W.; Narula, J.; Fayad, Z.A.; Bagiella, E.; et al. Association of Treatment Dose Anticoagulation With In-Hospital Survival Among Hospitalized Patients With COVID-19. J. Am. Coll. Cardiol. 2020, 76, 122–124. [Google Scholar] [CrossRef]
- Horsted, F.; West, J.; Grainge, M.J. Risk of venous thromboembolism in patients with cancer: A systematic review and meta-analysis. PLoS Med. 2012, 9, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Seng, S.; Liu, Z.; Chiu, S.K.; Proverbs-Singh, T.; Sonpavde, G.; Choueiri, T.K.; Tsao, C.K.; Yu, M.; Hahn, N.M.; Oh, W.K.; et al. Risk of venous thromboembolism in patients with cancer treated with cisplatin: A systematic review and meta-analysis. J. Clin. Oncol. 2012, 30, 4416–4426. [Google Scholar] [CrossRef]
- Rupa-Matysek, J.; Lembicz, M.; Rogowska, E.K.; Gil, L.; Komarnicki, M.; Batura-Gabryel, H. Evaluation of risk factors and assessment models for predicting venous thromboembolism in lung cancer patients. Med. Oncol. 2018, 35, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gade, I.L.; Brækkan, S.; Næss, I.A.; Hansen, J.B.; Rosendaal, F.; Cannegieter, S.; Overvad, K.; Jensvoll, H.; Hammerstrøm, J.; Gran, O.V.; et al. Epidemiology of venous thromboembolism in hematological cancers: The Scandinavian Thrombosis and Cancer (STAC) cohort. Thromb. Res. 2017, 158, 157–160. [Google Scholar] [CrossRef]
- Frere, C.; Bournet, B.; Gourgou, S.; Fraisse, J.; Canivet, C.; Connors, J.M.; Buscail, L.; Farge, D. Incidence of Venous Thromboembolism in Patients With Newly diagnosed pancreatic Ca and factors associated with outcomes. Gastroenterology 2020, 158, 1346–1358. [Google Scholar] [CrossRef]
- Godinho, J.; Casa-Nova, M.; Moreira-Pinto, J.; Simões, P.; Paralta Branco, F.; Leal-Costa, L.; Faria, A.; Lopes, F.; Teixeira, J.A.; Passos-Coelho, J.L. ONKOTEV Score as a Predictive Tool for Thromboembolic Events in Pancreatic Cancer—A Retrospective Analysis. Oncologist 2020, 25, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Ögren, M.; Bergqvist, D.; Wåhlander, K.; Eriksson, H.; Sternby, N.H. Trousseau’s syndrome—What is the evidence? A population-based autopsy study. Thromb. Haemost. 2006, 95, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef]
- Ay, C.; Dunkler, D.; Marosi, C.; Chiriac, A.-L.; Vormittag, R.; Simanek, R.; Quehenberger, P.; Zielinski, C.; Pabinger, I. Prediction of venous thromboembolism in cancer patients. Blood 2010, 116, 5377–5382. [Google Scholar] [CrossRef] [PubMed]
- Posch, F.; Riedl, J.; Reitter, E.M.; Kaider, A.; Zielinski, C.; Pabinger, I.; Ay, C. Hypercoagulabilty, venous thromboembolism, and death in patients with cancer: A multi-state model. Thromb. Haemost. 2016, 115, 817–826. [Google Scholar] [CrossRef] [PubMed]
- Parker, A.; Peterson, E.; Lee, A.Y.Y.; de Wit, C.; Carrier, M.; Polley, G.; Tien, J.; Wu, C. Risk stratification for the development of venous thromboembolism in hospitalized patients with cancer. J. Thromb. Haemost. 2018, 16, 1321–1326. [Google Scholar] [CrossRef] [PubMed]
- Patell, R.; Rybicki, L.; McCrae, K.R.; Khorana, A.A. Predicting risk of venous thromboembolism in hospitalized cancer patients: Utility of a risk assessment tool. Am. J. Hematol. 2017, 92, 501–507. [Google Scholar] [CrossRef]
- Wang, Y.; Attar, B.M.; Fuentes, H.E.; Yu, J.; Zhang, H.; Tafur, A.J. Performance of Khorana Risk Score for Prediction of Venous Thromboembolism in Patients With Hepatocellular Carcinoma. Clin. Appl. Thromb. 2018, 24, 471–476. [Google Scholar] [CrossRef]
- Mirza, A.S.; Yun, S.; Ali, N.A.; Shin, H.; O’Neil, J.L.; Elharake, M.; Schwartz, D.; Robinson, K.; Nowell, E.; Engle, G.; et al. Validation of the Khorana score in acute myeloid leukemia patients: A single-institution experience. Thromb. J. 2019, 17, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, A.S.; Tafur, A.J.; Wang, C.E.; Kourelis, T.V.; Wysokinska, E.M.; Yang, P. Predictors of active cancer thromboembolic outcomes: Validation of the Khorana score among patients with lung cancer. J. Thromb. Haemost. 2016, 14, 1773–1778. [Google Scholar] [CrossRef]
- Rupa-Matysek, J.; Gil, L.; Kaźmierczak, M.; Barańska, M.; Komarnicki, M. Prediction of venous thromboembolism in newly diagnosed patients treated for lymphoid malignancies: Validation of the Khorana Risk Score. Med. Oncol. 2018, 35, 1–8. [Google Scholar] [CrossRef]
- Carrier, M.; Abou-Nassar, K.; Mallick, R.; Tagalakis, V.; Shivakumar, S.; Schattner, A.; Kuruvilla, P.; Hill, D.; Spadafora, S.; Marquis, K.; et al. Apixaban to prevent venous thromboembolism in patients with cancer. N. Engl. J. Med. 2019, 380, 711–719. [Google Scholar] [CrossRef]
- Khorana, A.A.; Soff, G.A.; Kakkar, A.K.; Vadhan-Raj, S.; Riess, H.; Wun, T.; Streiff, M.B.; Garcia, D.A.; Liebman, H.A.; Belani, C.P.; et al. Rivaroxaban for thromboprophylaxis in high-risk ambulatory patients with cancer. N. Engl. J. Med. 2019, 380, 720–728. [Google Scholar] [CrossRef]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the treatment of venous thromboembolism associated with cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef] [PubMed]
- Raskob, G.E.; Van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N. Engl. J. Med. 2018, 378, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Young, A.M.; Marshall, A.; Thirlwall, J.; Chapman, O.; Lokare, A.; Hill, C.; Hale, D.; Dunn, J.A.; Lyman, G.H.; Hutchinson, C.; et al. Comparison of an oral factor xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: Results of a randomized trial (SELECT-D). J. Clin. Oncol. 2018, 36, 2017–2023. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Carlson, J.J.; Kuderer, N.M.; Schaefer, J.K.; Li, S.; Garcia, D.A.; Khorana, A.A.; Carrier, M.; Lyman, G.H. Cost-effectiveness analysis of low-dose direct oral anticoagulant (DOAC) for the prevention of cancer-associated thrombosis in the United States. Cancer 2020. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Tao, R.; Zhao, H.; Jiang, J.; Yang, J. Prevention of venous thromboembolism in patients with cancer with direct oral anticoagulants: A systematic review and meta-analysis. Medicine 2020, 99, e19000. [Google Scholar] [CrossRef] [PubMed]
- Pabinger, I.; van Es, N.; Heinze, G.; Posch, F.; Riedl, J.; Reitter, E.M.; Di Nisio, M.; Cesarman-Maus, G.; Kraaijpoel, N.; Zielinski, C.C.; et al. A clinical prediction model for cancer-associated venous thromboembolism: A development and validation study in two independent prospective cohorts. Lancet Haematol. 2018, 5, e289–e298. [Google Scholar] [CrossRef]
- Haltout, J.; Awada, A.; Paesmans, M.; Moreau, M.; Klastersky, J.; Machiels, G.; Ignatiadis, M.; Kotecki, N. Predictive factors for cancer-associated thrombosis in a large retrospective single-center study. Support. Care Cancer 2019, 27, 1163–1170. [Google Scholar] [CrossRef]
- McBane, R.; Wysokinski, W.E.; Le-Rademacher, J.G.; Zemla, T.; Ashrani, A.; Tafur, A.; Perepu, U.; Anderson, D.; Gundabolu, K.; Kuzma, C.; et al. Apixaban and Dalteparin in Active Malignancy Associated Venous Thromboembolism: The ADAM VTE Trial. J. Thromb. Haemost. 2019, 18, 411–421. [Google Scholar] [CrossRef]
- Büller, H.R.; Bethune, C.; Bhanot, S.; Gailani, D.; Monia, B.P.; Raskob, G.E.; Segers, A.; Verhamme, P.; Weitz, J.I. Factor XI antisense oligonucleotide for prevention of venous thrombosis. N. Engl. J. Med. 2015, 372, 232–240. [Google Scholar] [CrossRef]
- Bradley, M.; Shi, A.; Khatri, V.; Schobel, S.; Silvius, E.; Kirk, A.; Buchman, T.; Oh, J.; Elster, E. Prediction of venous thromboembolism using clinical and serum biomarker data from a military cohort of trauma patients. BMJ Mil. Heal. 2020. [Google Scholar] [CrossRef]
- Posch, F.; Thaler, J.; Zlabinger, G.J.; Königsbrügge, O.; Koder, S.; Zielinski, C.; Pabinger, I.; Ay, C. Soluble vascular endothelial growth factor (sVEGF) and the risk of venous thromboembolism in patients with cancer: Results from the Vienna cancer and Thrombosis Study (CATS). Clin. Cancer Res. 2016, 22, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Mauracher, L.-M.; Posch, F.; Martinod, K.; Grilz, E.; Däullary, T.; Hell, L.; Brostjan, C.; Zielinski, C.; Ay, C.; Wagner, D.D.; et al. Citrullinated histone H3, a biomarker of neutrophil extracellular trap formation, predicts the risk of venous thromboembolism in cancer patients. J. Thromb. Haemost. 2018, 16, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Albertsen, I.E.; Nielsen, P.B.; Søgaard, M.; Goldhaber, S.Z.; Overvad, T.F.; Rasmussen, L.H.; Larsen, T.B. Risk of Recurrent Venous Thromboembolism: A Danish Nationwide Cohort Study. Am. J. Med. 2018, 131, 1067–1074.e4. [Google Scholar] [CrossRef] [PubMed]
- Cowley, L.E.; Farewell, D.M.; Maguire, S.; Kemp, A.M. Methodological standards for the development and evaluation of clinical prediction rules: A review of the literature. Diagn. Progn. Res. 2019, 3, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Taha, H.; Govindraj, E.; Jaber, F.; Shehadeh, G.; Kelly, B.; Krishnan, S.; Hamed, W.K. Improving venous thromboembolism prophylaxis through critical thinking and health informatics. BMJ Open Qual. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Depietri, L.; Marietta, M.; Scarlini, S.; Marcacci, M.; Corradini, E.; Pietrangelo, A.; Ventura, P. Clinical impact of application of risk assessment models (Padua Prediction Score and Improve Bleeding Score) on venous thromboembolism, major hemorrhage and health expenditure associated with pharmacologic VTE prophylaxis: A “real life” prospective and re. Intern. Emerg. Med. 2018, 13, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Nafee, T.; Gibson, C.M.; Travis, R.; Yee, M.K.; Kerneis, M.; Chi, G.; AlKhalfan, F.; Hernandez, A.F.; Hull, R.D.; Cohen, A.T.; et al. Machine learning to predict venous thrombosis in acutely ill medical patients. Res. Pr. Thromb. Haemost. 2020, 4, 230–237. [Google Scholar] [CrossRef]


{kind=link}
| Intrinsic Risk Factors | Odds Ratio (or) for VTE |
|---|---|
| Elevated BMI > 30 | 2.3 |
| Heterozygous Prothrombin gene mutation | 2.8 |
| Heterozygous Factor V Leiden gene mutation | 4.2 |
| Homozygous Prothrombin gene mutation | 6.7 |
| Homozygous Factor V Leiden gene mutation | 11.5 |
| Antithrombin deficiency | 14.0 |
| Acquired Risk Factors | Odds Ratio (or) for VTE |
|---|---|
| Seated immobility at work * | 1.8 |
| Long-Haul Travel † | 2.1 |
| Testosterone supplementation | 2.3 |
| Low risk COC (Levonorgestrel) | 3.6 |
| Pregnancy or Postpartum | 4.2 |
| Trauma/Fracture | 4.6 |
| Medical Hospitalization | 5.1 |
| Neurologic Disease with Leg Paresis | 6.1 |
| High risk COC (Desogestrel) | 6.8 |
| Active Cancer | 14.6 |
| Surgery | 21.7 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicholson, M.; Chan, N.; Bhagirath, V.; Ginsberg, J. Prevention of Venous Thromboembolism in 2020 and Beyond. J. Clin. Med. 2020, 9, 2467. https://doi.org/10.3390/jcm9082467
Nicholson M, Chan N, Bhagirath V, Ginsberg J. Prevention of Venous Thromboembolism in 2020 and Beyond. Journal of Clinical Medicine. 2020; 9(8):2467. https://doi.org/10.3390/jcm9082467
Chicago/Turabian StyleNicholson, Matthew, Noel Chan, Vinai Bhagirath, and Jeffrey Ginsberg. 2020. "Prevention of Venous Thromboembolism in 2020 and Beyond" Journal of Clinical Medicine 9, no. 8: 2467. https://doi.org/10.3390/jcm9082467
APA StyleNicholson, M., Chan, N., Bhagirath, V., & Ginsberg, J. (2020). Prevention of Venous Thromboembolism in 2020 and Beyond. Journal of Clinical Medicine, 9(8), 2467. https://doi.org/10.3390/jcm9082467